
Proposed Cut-Off Score for the Japanese Version of the Fear of Coronavirus Disease 2019 Scale (FCV-19S): Evidence from a Large-Scale National Survey in Japan

 , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Measures
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. WHO Coronavirus (COVID-19) Dashboard. 2022. Available online: https://covid19.who.int/ (accessed on 1 April 2022).
- Ministry of Health, Labour and Welfare. COVID-19 Situation Report: Current Situation in Japan. 2022. Available online: https://www.mhlw.go.jp/stf/covid-19/kokunainohasseijoukyou_00006.html (accessed on 1 April 2022).
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tanaka, T.; Okamoto, S. Increase in suicide following an initial decline during the COVID-19 pandemic in Japan. Nat. Hum. Behav. 2021, 5, 229–238. [Google Scholar] [CrossRef] [PubMed]
- Organisation for Economic Co-operation and Development. Tackling the Mental Health Impact of the COVID-19 Crisis: An Integrated, Whole-of-Society Response. 2021. Available online: https://read.oecd-ilibrary.org/view/?ref=1094_1094455-bukuf1f0cm (accessed on 1 April 2022).
- Xiong, J.; Lipsitz, O.; Nasri, F.; Lui, L.M.W.; Gill, H.; Phan, L.; Chen-Li, D.; Iacobucci, M.; Ho, R.; Majeed, A.; et al. Impact of COVID-19 pandemic on mental health in the general population: A systematic review. J. Affect. Disord. 2020, 277, 55–64. [Google Scholar] [CrossRef] [PubMed]
- Yoshioka, T.; Okubo, R.; Tabuchi, T.; Odani, S.; Shinozaki, T.; Tsugawa, Y. Factors associated with serious psychological distress during the COVID-19 pandemic in Japan: A nationwide cross-sectional internet-based study. BMJ Open 2021, 11, e051115. [Google Scholar] [CrossRef]
- Harper, C.A.; Satchell, L.P.; Fido, D.; Latzman, R.D. Functional fear predicts public health compliance in the COVID-19 pandemic. Int. J. Ment. Health Addict. 2021, 19, 1875–1888. [Google Scholar] [CrossRef]
- Ahorsu, D.K.; Lin, C.Y.; Imani, V.; Saffari, M.; Griffiths, M.D.; Pakpour, A.H. The fear of COVID-19 scale: Development and initial validation. Int. J. Ment. Health Addict. 2022, 20, 1537–1545. [Google Scholar] [CrossRef] [Green Version]
- Lee, S.A. Coronavirus Anxiety Scale: A brief mental health screener for COVID-19 related anxiety. Death Stud. 2020, 44, 393–401. [Google Scholar] [CrossRef] [Green Version]
- Taylor, S.; Landry, C.A.; Paluszek, M.M.; Fergus, T.A.; McKay, D.; Asmundson, G.J.G. Development and initial validation of the COVID Stress Scales. J. Anxiety Disord. 2020, 72, 32408047. [Google Scholar] [CrossRef]
- Masuyama, A.; Shinkawa, H.; Kubo, T. Validation and psychometric properties of the Japanese version of the fear of COVID-19 scale among adolescents. Int. J. Ment. Health Addict. 2022, 20, 387–397. [Google Scholar] [CrossRef]
- Wakashima, K.; Asai, K.; Kobayashi, D.; Koiwa, K.; Kamoshida, S.; Sakuraba, M. The Japanese version of the Fear of COVID-19 scale: Reliability, validity, and relation to coping behavior. PLoS ONE 2020, 15, e0241958. [Google Scholar] [CrossRef]
- Midorikawa, H.; Aiba, M.; Lebowitz, A.; Taguchi, T.; Shiratori, Y.; Ogawa, T.; Takahashi, A.; Takahashi, S.; Nemoto, K.; Arai, T.; et al. Confirming validity of the Fear of COVID-19 Scale in Japanese with a nationwide large-scale sample. PLoS ONE 2021, 16, e0246840. [Google Scholar] [CrossRef]
- Chi, X.; Chen, S.; Chen, Y.; Chen, D.; Yu, Q.; Guo, T.; Cao, Q.; Zheng, X.; Huang, S.; Hossain, M.M.; et al. Psychometric Evaluation of the Fear of COVID-19 Scale among Chinese Population. Int. J. Ment. Health Addict. 2022, 20, 1273–1288. [Google Scholar] [CrossRef] [PubMed]
- Sakib, N.; Bhuiyan, A.K.M.I.; Hossain, S.; Al Mamun, F.; Hosen, I.; Abdullah, A.H.; Sarker, M.A.; Mohiuddin, M.S.; Rayhan, I.; Hossain, M.; et al. Psychometric validation of the Bangla fear of COVID-19 scale: Confirmatory factor analysis and Rasch analysis. Int. J. Ment. Health Addict. 2022, 20, 2623–2634. [Google Scholar] [CrossRef] [PubMed]
- Mailliez, M.; Griffiths, M.D.; Carre, A. Validation of the French version of the fear of COVID-19 scale and its associations with depression, anxiety, and differential emotions. Int. J. Ment. Health Addict. 2022, 20, 2057–2071. [Google Scholar] [CrossRef] [PubMed]
- Soraci, P.; Ferrari, A.; Abbiati, F.A.; Del Fante, E.; De Pace, R.; Urso, A.; Griffiths, M.D. Validation and psychometric evaluation of the Italian version of the fear of COVID-19 scale. Int. J. Ment. Health Addict. 2022, 20, 1913–1922. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Lorca, M.; Martínez-Lorca, A.; Criado-Álvarez, J.J.; Armesilla, M.D.C.; Latorre, J.M. The fear of COVID-19 scale: Validation in Spanish university students. Psychiatry Res. 2020, 293, 113350. [Google Scholar] [CrossRef]
- Tsipropoulou, V.; Nikopoulou, V.A.; Holeva, V.; Nasika, Z.; Diakogiannis, I.; Sakka, S.; Kostikidou, S.; Varvara, C.; Spyridopoulou, E.; Parlapani, E. Psychometric properties of the Greek version of FCV-19S. Int. J. Ment. Health Addict. 2021, 19, 2279–2288. [Google Scholar] [CrossRef]
- Satici, B.; Gocet-Tekin, E.; Deniz, M.E.; Satici, S.A. Adaptation of the fear of COVID-19 scale: Its association with psychological distress and life satisfaction in Turkey. Int. J. Ment. Health Addict. 2021, 19, 1980–1988. [Google Scholar] [CrossRef]
- Iversen, M.M.; Norekvål, T.M.; Oterhals, K.; Fadnes, L.T.; Mæland, S.; Pakpour, A.H.; Breivik, K. Psychometric Properties of the Norwegian version of the fear of COVID-19 Scale. Int. J. Ment. Health Addict. 2022, 20, 1446–1464. [Google Scholar] [CrossRef]
- Stănculescu, E. Fear of COVID-19 in Romania: Validation of the Romanian version of the fear of COVID-19 scale using graded response model analysis. Int. J. Ment. Health Addict. 2022, 20, 1094–1109. [Google Scholar] [CrossRef]
- Perz, C.A.; Lang, B.A.; Harrington, R. Validation of the fear of COVID-19 scale in a US college sample. Int. J. Ment. Health Addict. 2022, 20, 273–283. [Google Scholar] [CrossRef] [PubMed]
- de Medeiros, E.D.; Reis, L.M.; Guimarães, C.L.C.; da Silva, P.G.N.; Monteiro, R.P.; Coelho, G.L.; Guimarães, C.M.; Martins, E.R.; de França, L.L. Psychometric properties of the Brazilian version of the fear of COVID-19 scale (FCV-19S). Curr. Psychol. 2021, 1–10. [Google Scholar] [CrossRef]
- Lin, C.Y.; Hou, W.L.; Mamun, M.A.; Aparecido da Silva, J.; Broche-Pérez, Y.; Ullah, I.; Masuyama, A.; Wakashima, K.; Mailliez, M.; Carre, A.; et al. Fear of COVID-19 Scale (FCV-19S) across countries: Measurement invariance issues. Nurs. Open. 2021, 8, 1892–1908. [Google Scholar] [CrossRef] [PubMed]
- Nikopoulou, V.A.; Holeva, V.; Parlapani, E.; Karamouzi, P.; Voitsidis, P.; Porfyri, G.N.; Blekas, A.; Papigkioti, K.; Patsiala, S.; Diakogiannis, I. Mental health screening for COVID-19: A proposed cutoff score for the Greek version of the fear of COVID-19 scale (FCV-19S). Int. J. Ment. Health Addict. 2022, 20, 907–920. [Google Scholar] [CrossRef]
- Miyawaki, A.; Tabuchi, T.; Tomata, Y.; Tsugawa, Y. Association between participation in the government subsidy programme for domestic travel and symptoms indicative of COVID-19 infection in Japan: Cross-sectional study. BMJ Open 2021, 11, e049069. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5); American Psychiatric Publishing: Washington DC, USA, 2003. [Google Scholar]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B.; Löwe, B. The Patient Health Questionnaire Somatic, Anxiety, and Depressive Symptom Scales: A systematic review. Gen. Hosp. Psychiatry 2010, 32, 345–359. [Google Scholar] [CrossRef]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.; Löwe, B. A brief measure for assessing generalized anxiety disorder: The GAD-7. Arch. Intern. Med. 2006, 166, 1092–1097. [Google Scholar] [CrossRef] [Green Version]
- Mantri, S.; Lawson, J.M.; Wang, Z.; Koenig, H.G. Identifying moral injury in healthcare professionals: The moral injury symptom scale-HP. J. Relig. Health. 2020, 59, 2323–2340. [Google Scholar] [CrossRef]
- Kessler, R.C.; Barker, P.R.; Colpe, L.J.; Epstein, J.F.; Gfroerer, J.C.; Hiripi, E.; Howes, M.J.; Normand, S.L.; Manderscheid, R.W.; Walters, E.E.; et al. Screening for serious mental illness in the general population. Arch. Gen. Psychiatry 2003, 60, 184–189. [Google Scholar] [CrossRef]
- Furukawa, T.A.; Kawakami, N.; Saitoh, M.; Ono, Y.; Nakane, Y.; Nakamura, Y.; Tachimori, H.; Iwata, N.; Uda, H.; Nakane, H.; et al. The performance of the Japanese version of the K6 and K10 in the World Mental Health Survey Japan. Int. J. Methods Psychiatr. Res. 2008, 17, 152–158. [Google Scholar] [CrossRef]
- Sakurai, K.; Nishi, A.; Kondo, K.; Yanagida, K.; Kawakami, N. Screening performance of K6/K10 and other screening instruments for mood and anxiety disorders in Japan. Psychiatry Clin. Neurosci. 2011, 65, 434–441. [Google Scholar] [CrossRef] [PubMed]
- Prochaska, J.J.; Sung, H.Y.; Max, W.; Shi, Y.; Ong, M. Validity study of the K6 scale as a measure of moderate mental distress based on mental health treatment need and utilization. Int. J. Methods Psychiatr. Res. 2012, 21, 88–97. [Google Scholar] [CrossRef] [PubMed]
- Fluss, R.; Faraggi, D.; Reiser, B. Estimation of the Youden Index and its associated cutoff point. Biom. J. 2005, 47, 458–472. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barua, L.; Zaman, M.S.; Omi, F.R.; Faruque, M. Psychological burden of the COVID-19 pandemic and its associated factors among frontline doctors of Bangladesh: A cross-sectional study. F1000Research 2020, 9, 1304. [Google Scholar] [CrossRef] [PubMed]
- Pacella, M.L.; Hruska, B.; Delahanty, D.L. The physical health consequences of PTSD and PTSD symptoms: A meta-analytic review. J. Anxiety Disord. 2013, 27, 33–46. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristics | Characteristics Name | n (%) | Women | Men | ||
|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | |||
| Age group (years) | 20–39 | 7321 (27.9) | 18.50 | 5.10 | 17.69 | 5.64 |
| 40–64 | 11,794 (44.9) | 18.70 | 4.96 | 17.76 | 5.40 | |
| 65–79 | 7171 (27.3) | 19.05 | 4.51 | 18.40 | 4.69 | |
| Education | ≤High School Unknown | 11,570 (44) | 18.93 | 4.89 | 18.13 | 5.46 |
| >High School | 14,716 (56) | 18.56 | 4.87 | 17.78 | 5.20 | |
| Marital status | Single | 7254 (27.6) | 18.16 | 5.14 | 17.66 | 5.69 |
| Divorced Bereaved | 2767 (10.5) | 18.70 | 4.85 | 17.35 | 5.33 | |
| Married | 16,265 (61.9) | 18.99 | 4.77 | 18.09 | 5.09 | |
| Cohabitant | No | 5469 (20.8) | 18.02 | 5.03 | 17.36 | 5.60 |
| Yes | 20,817 (79.2) | 18.91 | 4.83 | 18.06 | 5.21 | |
| Occupation | Self-employment | 1799 (6.8) | 17.86 | 5.16 | 17.61 | 5.41 |
| Part-time job | 5177 (19.7) | 18.76 | 4.88 | 17.92 | 5.31 | |
| Employed | 9996 (38) | 18.37 | 5.13 | 17.80 | 5.39 | |
| Unemployed | 9314 (35.4) | 19.02 | 4.70 | 18.26 | 5.05 | |
| Income | <2,000,000 JPY | 2225 (8.5) | 18.86 | 5.27 | 18.48 | 6.31 |
| ≥2,000,000– <6,000,000 JPY | 10,555 (40.2) | 18.60 | 4.77 | 18.03 | 5.17 | |
| ≥6,000,000– <12,000,000 JPY | 6771 (25.8) | 18.39 | 4.76 | 17.51 | 5.11 | |
| ≥12,000,000 JPY | 1372 (5.2) | 17.95 | 5.37 | 16.84 | 5.11 | |
| Other/Unknown | 5363 (20.4) | 19.36 | 4.87 | 18.53 | 5.46 | |
| K6 | ≥5 | 9094 (34.6) | 20.34 | 5.21 | 19.60 | 5.52 |
| <5 | 17,192 (65.4) | 17.85 | 4.45 | 17.06 | 4.98 | |
| Problems due to the fear of COVID-19 | Yes | 4022 (15.3) | 22.58 | 5.39 | 22.68 | 5.86 |
| No | 22,264 (84.7) | 17.99 | 4.40 | 17.13 | 4.77 | |
| χ2 | (df) | p | CFI | TLI | RMSEA | AIC | |
|---|---|---|---|---|---|---|---|
| One-factor | 382.98 | 8 | <0.001 | 0.996 | 0.990 | 0.042 | 422.98 |
| Two-factor | 713.57 | 10 | <0.001 | 0.993 | 0.984 | 0.052 | 749.57 |
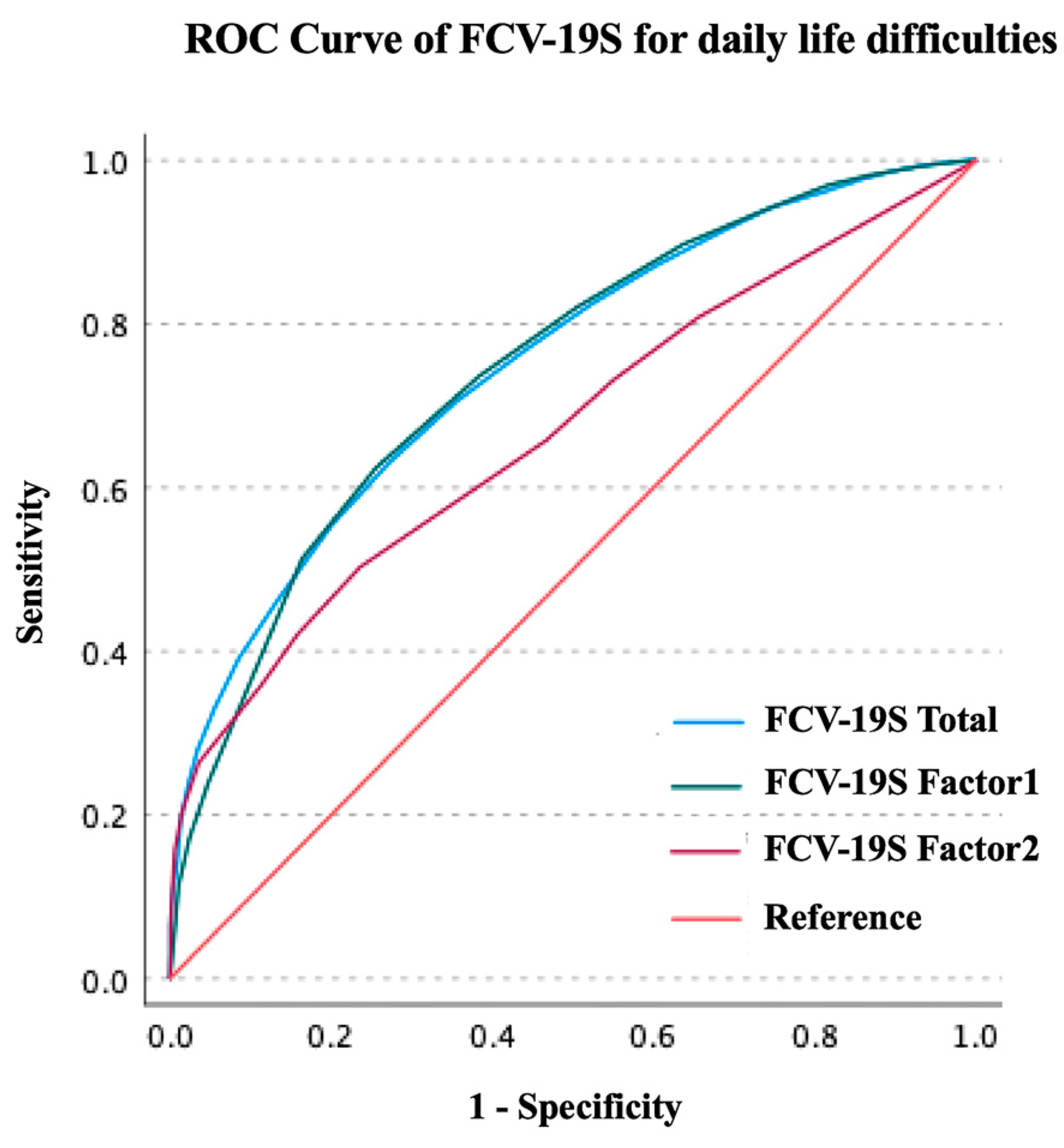
| FCV-19S Type | Cut-Off | Sensitivity | Specificity | AUC | 95% CI | Significance | Youden’s Index |
|---|---|---|---|---|---|---|---|
| FCV-19S Total | 21 | 0.630 | 0.728 | 0.751 | 0.742–0.759 | <0.001 | 0.359 |
| FCV-19S Factor 1 | 15 | 0.624 | 0.744 | 0.747 | 0.739–0.756 | <0.001 | 0.369 |
| FCV-19S Factor 2 | 7 | 0.503 | 0.764 | 0.669 | 0.659–0.679 | <0.001 | 0.267 |
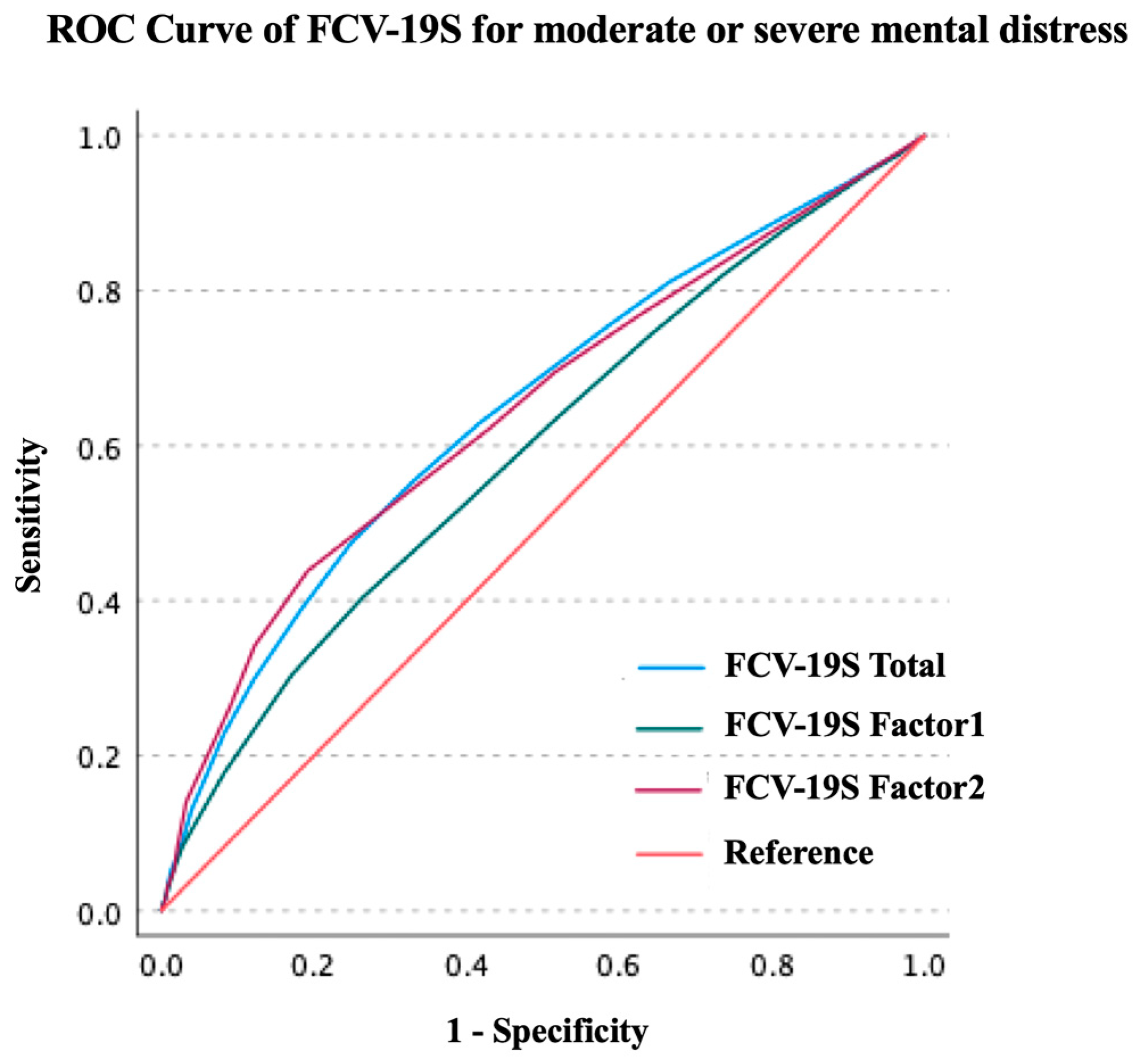
| FCV-19S Type | Cut-Off | Sensitivity | Specificity | AUC | 95% CI | Significance | Youden’s Index |
|---|---|---|---|---|---|---|---|
| FCV-19S Total | 21 | 0.388 | 0.817 | 0.645 | 0.638–0.652 | <0.001 | 0.226 |
| FCV-19S Factor 1 | 15 | 0.404 | 0.737 | 0.594 | 0.587–0.602 | <0.001 | 0.140 |
| FCV-19S Factor 2 | 7 | 0.438 | 0.808 | 0.645 | 0.637–0.652 | <0.001 | 0.247 |
| FCV-19S Total | FCV-19S Factor 1 | FCV-19S Factor 2 | ||||||
|---|---|---|---|---|---|---|---|---|
| Cut-off | Sensitivity | Specificity | Cut-off | Sensitivity | Specificity | Cut-off | Sensitivity | Specificity |
| 13 | 0.977 | 0.140 | 7 | 0.995 | 0.051 | 4 | 0.808 | 0.344 |
| 14 | 0.962 | 0.186 | 8 | 0.992 | 0.076 | 5 | 0.731 | 0.450 |
| 15 | 0.942 | 0.254 | 9 | 0.981 | 0.135 | 6 | 0.658 | 0.533 |
| 16 | 0.911 | 0.319 | 10 | 0.969 | 0.185 | 7 | 0.503 | 0.764 |
| 17 | 0.872 | 0.396 | 11 | 0.938 | 0.266 | 8 | 0.421 | 0.842 |
| 18 | 0.825 | 0.476 | 12 | 0.897 | 0.363 | 9 | 0.358 | 0.887 |
| 19 | 0.768 | 0.559 | 13 | 0.821 | 0.494 | 10 | 0.264 | 0.965 |
| 20 | 0.705 | 0.646 | 14 | 0.736 | 0.617 | 11 | 0.203 | 0.985 |
| 21 | 0.630 | 0.728 | 15 | 0.624 | 0.744 | 12 | 0.156 | 0.994 |
| 22 | 0.553 | 0.800 | 16 | 0.513 | 0.836 | 13 | 0.090 | 0.998 |
| 23 | 0.461 | 0.868 | 17 | 0.316 | 0.920 | 14 | 0.070 | 0.999 |
| 24 | 0.392 | 0.915 | 18 | 0.239 | 0.953 | 15 | 0.058 | 1.000 |
| FCV-19S total | FCV-19S Factor 1 | FCV-19S Factor 2 | ||||||
|---|---|---|---|---|---|---|---|---|
| Cut-off | Sensitivity | Specificity | Cut-off | Sensitivity | Specificity | Cut-off | Sensitivity | Specificity |
| 13 | 0.918 | 0.143 | 7 | 0.966 | 0.050 | 4 | 0.771 | 0.370 |
| 14 | 0.891 | 0.192 | 8 | 0.952 | 0.075 | 5 | 0.695 | 0.484 |
| 15 | 0.851 | 0.263 | 9 | 0.912 | 0.132 | 6 | 0.622 | 0.571 |
| 16 | 0.811 | 0.334 | 10 | 0.879 | 0.183 | 7 | 0.438 | 0.808 |
| 17 | 0.755 | 0.413 | 11 | 0.820 | 0.264 | 8 | 0.342 | 0.878 |
| 18 | 0.694 | 0.496 | 12 | 0.743 | 0.359 | 9 | 0.264 | 0.910 |
| 19 | 0.630 | 0.583 | 13 | 0.631 | 0.487 | 10 | 0.141 | 0.967 |
| 20 | 0.555 | 0.669 | 14 | 0.520 | 0.607 | 11 | 0.085 | 0.978 |
| 21 | 0.474 | 0.751 | 15 | 0.404 | 0.737 | 12 | 0.052 | 0.984 |
| 22 | 0.388 | 0.817 | 16 | 0.304 | 0.829 | 13 | 0.029 | 0.992 |
| 23 | 0.298 | 0.879 | 17 | 0.178 | 0.917 | 14 | 0.020 | 0.993 |
| 24 | 0.228 | 0.918 | 18 | 0.124 | 0.949 | 15 | 0.016 | 0.994 |
| Characteristics | Characteristics Name | FCV-19S | |||
|---|---|---|---|---|---|
| ≥21 | <21 | p | Cramer’s V | ||
| Sex | Women | 4683 (34.6) | 8871 (65.4) | <0.001 | 0.04 |
| Men | 3901 (30.6) | 8831 (69.4) | |||
| Age group | 20–39 | 2342 (32) | 4979 (68) | <0.001 | 0.02 |
| 40–64 | 3794 (32.2) | 8000 (67.8) | |||
| 65–79 | 2448 (34.1) | 4,723 (65.9) | |||
| Education | ≤High School/Unknown | 4053 (35) | 7517 (65) | <0.001 | 0.05 |
| >High School | 4531 (30.8) | 10,185 (69.2) | |||
| Marital status | Single | 2245 (30.9) | 5009 (69.1) | <0.001 | 0.02 |
| Divorced/Bereaved | 890 (32.2) | 1877 (67.8) | |||
| Married | 5449 (33.5) | 10,816 (66.5) | |||
| Cohabitant | No | 1599 (29.2) | 3870 (70.8) | <0.001 | 0.04 |
| Yes | 6985 (33.6) | 13,832 (66.4) | |||
| Occupation | Self-employment | 528 (29.3) | 1271 (70.7) | <0.001 | 0.04 |
| Part time job | 1746 (33.7) | 3431 (66.3) | |||
| Employed | 3080 (30.8) | 6916 (69.2) | |||
| Unemployed | 3230 (34.7) | 6084 (65.3) | |||
| Income | <2,000,000 JPY | 808 (36.3) | 1417 (63.7) | <0.001 | 0.08 |
| ≥2,000,000– <6,000,000 JPY | 3403 (32.2) | 7152 (67.8) | |||
| ≥6,000,000– <12,000,000 JPY | 1976 (29.2) | 4795 (70.8) | |||
| ≥12,000,000 JPY | 344 (25.1) | 1028 (74.9) | |||
| Other/Unknown | 2053 (38.3) | 3310 (61.7) | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Midorikawa, H.; Tachikawa, H.; Aiba, M.; Shiratori, Y.; Sugawara, D.; Kawakami, N.; Okubo, R.; Tabuchi, T. Proposed Cut-Off Score for the Japanese Version of the Fear of Coronavirus Disease 2019 Scale (FCV-19S): Evidence from a Large-Scale National Survey in Japan. Int. J. Environ. Res. Public Health 2023, 20, 429. https://doi.org/10.3390/ijerph20010429
Midorikawa H, Tachikawa H, Aiba M, Shiratori Y, Sugawara D, Kawakami N, Okubo R, Tabuchi T. Proposed Cut-Off Score for the Japanese Version of the Fear of Coronavirus Disease 2019 Scale (FCV-19S): Evidence from a Large-Scale National Survey in Japan. International Journal of Environmental Research and Public Health. 2023; 20(1):429. https://doi.org/10.3390/ijerph20010429
Chicago/Turabian StyleMidorikawa, Haruhiko, Hirokazu Tachikawa, Miyuki Aiba, Yuki Shiratori, Daichi Sugawara, Naoaki Kawakami, Ryo Okubo, and Takahiro Tabuchi. 2023. "Proposed Cut-Off Score for the Japanese Version of the Fear of Coronavirus Disease 2019 Scale (FCV-19S): Evidence from a Large-Scale National Survey in Japan" International Journal of Environmental Research and Public Health 20, no. 1: 429. https://doi.org/10.3390/ijerph20010429
APA StyleMidorikawa, H., Tachikawa, H., Aiba, M., Shiratori, Y., Sugawara, D., Kawakami, N., Okubo, R., & Tabuchi, T. (2023). Proposed Cut-Off Score for the Japanese Version of the Fear of Coronavirus Disease 2019 Scale (FCV-19S): Evidence from a Large-Scale National Survey in Japan. International Journal of Environmental Research and Public Health, 20(1), 429. https://doi.org/10.3390/ijerph20010429