



Shifts in Diabetes Health Literacy Policy and Practice in Australia—Promoting Organisational Health Literacy

 , ,
, ,
Abstract
:1. Introduction
2. Method
2.1. Context and Setting
2.2. Study Design
2.3. Environmental Scan Method
2.3.1. Grey Literature Search Strategy
2.3.2. Data Extraction, Synthesis and Analysis Procedure
2.3.3. Key Informant Consultation
2.4. Method for the Assessment of Understandability and Actionability Using PEMAT
3. Results
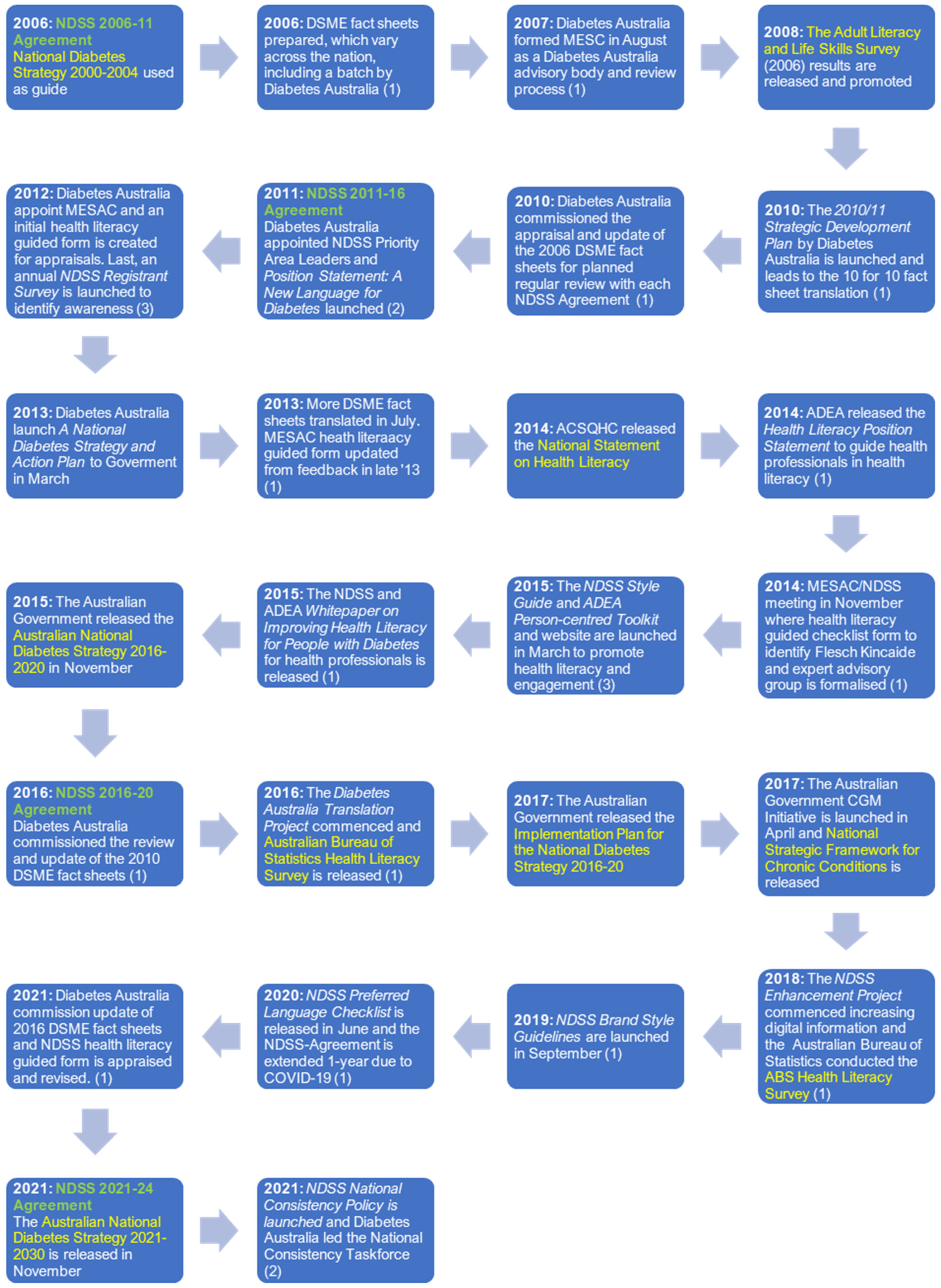
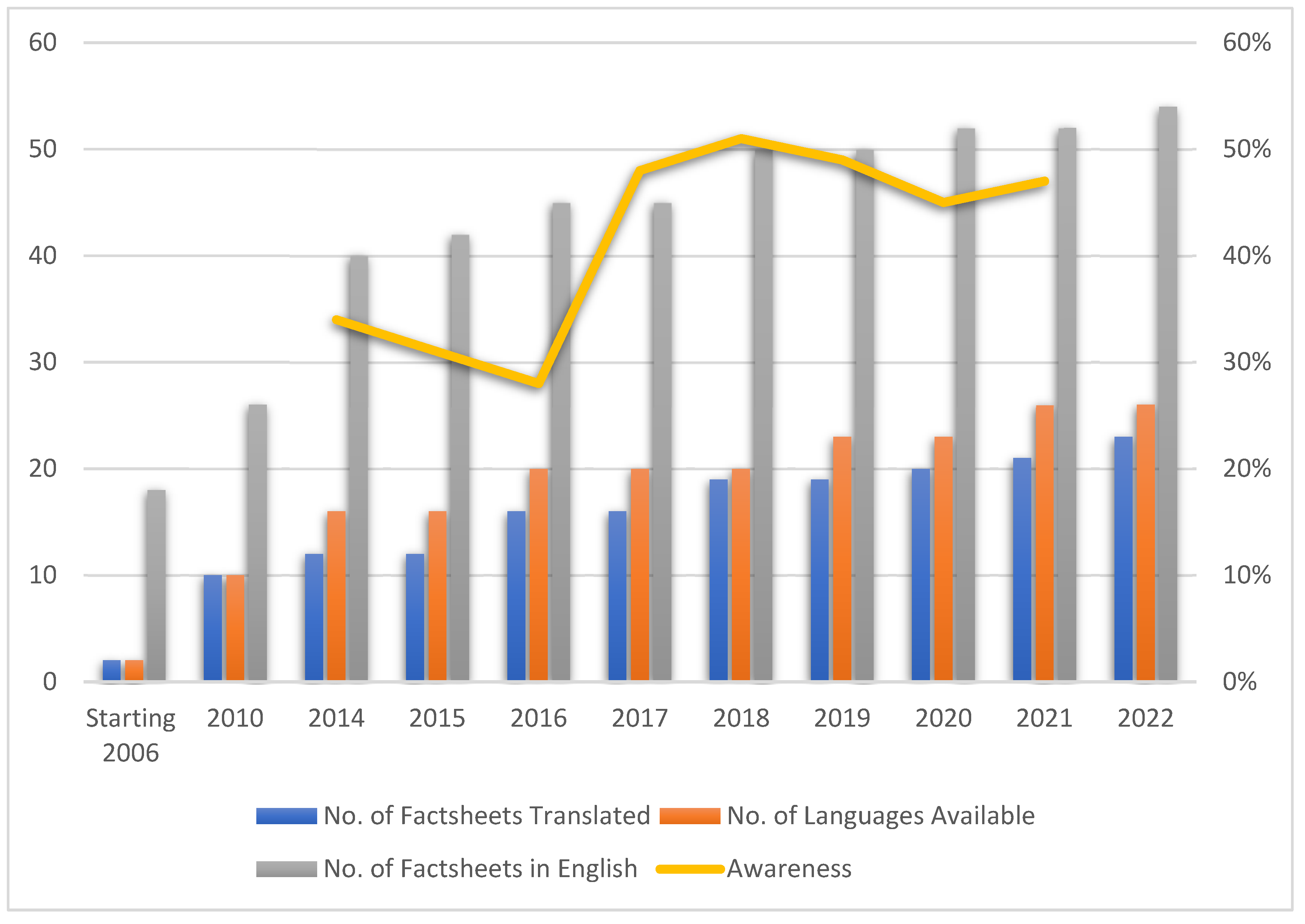
3.1. Policy and Practice Changes to Improve Organisation Health Literacy
3.1.1. The 2006 to 2011 National Diabetes Services Scheme Agreement Period
3.1.2. The 2011 to 2016 National Diabetes Services Scheme Agreement Period
3.1.3. The 2016 to 2021 National Diabetes Services Scheme Agreement Period
3.1.4. The 2021 to 2024 National Diabetes Services Scheme Agreement Period
3.2. Assessment of Understanding and Actionability
4. Discussion
4.1. Facilitators of Organisational Change to Promote Health Literacy
- National health literacy data and frameworks;
- Incremental change focusing on (a) audience reach, (b) consistency and branding, (c) person-centred language and (d) understandability and actionability;
- Group reflexivity.
4.1.1. National Health Literacy Data and Frameworks
4.1.2. Incremental Change
- I.
- Audience Reach
- II.
- Consistency and Branding
- III.
- Person-centred Language
- IV.
- Understanding and Actionability
4.1.3. Group Reflexivity
4.2. Future Considerations
4.3. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Trezona, A.; Rowlands, G.; Nutbeam, D. Progress in implementing national policies and strategies for health literacy–What have we learned so far? Int. J. Environ. Res. Public Health 2018, 15, 1554. [Google Scholar] [CrossRef]
- Nutbeam, D.; Lloyd, J.E. Understanding and responding to health literacy as a social determinant of health. Annu. Rev. Public Health 2021, 42, 159–173. [Google Scholar] [CrossRef]
- Rajah, R.; Hassali, M.; Murugiah, M.K. A systematic review of the prevalence of limited health literacy in Southeast Asian countries. Public Health 2019, 167, 8–15. [Google Scholar] [CrossRef]
- Sørensen, K.; Pelikan, J.M.; Röthlin, F.; Ganahl, K.; Slonska, Z.; Doyle, G.; Fullam, J.; Kondilis, B.; Agrafiotis, D.; Uiters, E.; et al. HLS-EU Consortium. Health literacy in Europe: Comparative results of the European health literacy survey (HLS-EU). Eur. J. Public Health 2015, 25, 1053–1058. [Google Scholar] [CrossRef] [PubMed]
- Rasu, R.S.; Bawa, W.A.; Suminski, R.; Snella, K.; Warady, B. Health Literacy Impact on National Healthcare Utilization and Expenditure. Int. J. Health Policy Manag. 2015, 4, 747–755. [Google Scholar] [CrossRef] [PubMed]
- Australian Institute of Health and Welfare. Health Literacy—Snapshot, Section: Determinants of Health. Canberra (AUS): Australian Institute of Health and Welfare. Available online: https://www.aihw.gov.au/reports/australias-health/health-literacy (accessed on 28 April 2022).
- Asharani, P.V.; Lau, J.H.; Roystonn, K.; Devi, F.; Peizhi, W.; Shafie, S.; Chang, S.; Jeyagurunathan, A.; Yiang, C.B.; Abdin, E.; et al. Health Literacy and Diabetes Knowledge: A Nationwide Survey in a Multi-Ethnic Population. Int. J. Environ. Res. Public Health 2021, 18, 9316. [Google Scholar] [CrossRef] [PubMed]
- Australian Government—Department of Health. National Preventive Health Strategy 2021–2030. December 2021. Available online: https://www.health.gov.au/resources/publications/national-preventive-health-strategy-2021-2030?language=en (accessed on 27 April 2023).
- Tajdar, D.; Lühmann, D.; Fertmann, R.; Steinberg, T.; Bussche, H.V.D.; Scherer, M.; Schäfer, I. Low health literacy is associated with higher risk of type 2 diabetes: A cross-sectional study in Germany. BMC Public Health 2021, 21, 510. [Google Scholar] [CrossRef]
- Rheault, H.; Coyer, F.; Jones, L.; Bonner, A. Health literacy in Indigenous people with chronic disease living in remote Australia. BMC Health Serv. Res. 2019, 19, 523. [Google Scholar] [CrossRef]
- Saeed, H.; Saleem, Z.; Naeem, R.; Shahzadi, I.; Islam, M. Impact of health literacy on diabetes outcomes: A cross-sectional study from Lahore, Pakistan. Public Health 2018, 156, 8–14. [Google Scholar] [CrossRef]
- Schillinger, D.; Grumbach, K.; Piette, J.; Wang, F.; Osmond, D.; Daher, C.; Palacios, J.; Sullivan, G.D.; Bindman, A.B. Association of health literacy with diabetes outcomes. JAMA 2002, 288, 475–482. [Google Scholar] [CrossRef]
- Neter, E.; Brainin, E. Association between health literacy, eHealth literacy, and health outcomes among patients with long-term conditions: A systematic review. Eur. Psychol. 2019, 24, 68–81. [Google Scholar] [CrossRef]
- Schillinger, D.; Barton, L.R.; Karter, A.J.; Wang, F.; Adler, N. Does Literacy Mediate the Relationship between Education and Health Outcomes? A Study of a Low-Income Population with Diabetes. Public Health Rep. 2006, 121, 245–254. [Google Scholar] [CrossRef] [PubMed]
- Parast, N. Improving diabetes virtual visits through health literacy assessment: A scoping review. J. Diabetes Nurs. 2021, 25, 205. [Google Scholar]
- Batterham, R.W.; Hawkins, M.; Collins, P.A.; Buchbinder, R.; Osborne, R.H. Health literacy: Applying current concepts to improve health services and reduce health inequalities. Public Health 2016, 132, 3–12. [Google Scholar] [CrossRef] [PubMed]
- Dinh NT, T.; de Graaff, B.; Campbell, J.A.; Jose, M.D.; John, B.; Saunder, T.; Kitsos, A.; Wiggins, N.; Palmer, A.J. Costs of major complications in people with and without diabetes in Tasmania, Australia. Aust. Health Rev. 2022, 46, 667–678. [Google Scholar] [CrossRef] [PubMed]
- Farmanova, E.; Bonneville, L.; Bouchard, L. Organizational health literacy: Review of theories, frameworks, guides, and implementation issues. Inquiry 2018, 55, 46958018757848. [Google Scholar] [CrossRef]
- Han, H.R.; Wu, D.; Taylor, J.; Wright, R.; Abshire, M. Consideration of health literacy in implementation science. J. Clin. Transl. Sci. 2021, 5, e118. [Google Scholar] [CrossRef]
- Charoghchian Khorasani, E.; Tavakoly Sany, S.B.; Tehrani, H.; Doosti, H.; Peyman, N. Review of organizational health literacy practice at health care centers: Outcomes, barriers and facilitators. Int. J. Environ. Res. Public Health 2020, 17, 7544. [Google Scholar] [CrossRef]
- BBremer, D.; Klockmann, I.; Jaß, L.; Härter, M.; von dem Knesebeck, O.; Lüdecke, D. Which criteria characterize a health literate health care organization?—A scoping review on organizational health literacy. BMC Health Serv. Res. 2021, 21, 664. [Google Scholar] [CrossRef]
- Lloyd, J.E.; Song, H.J.; Dennis, S.M.; Dunbar, N.; Harris, E.; Harris, M.F. A paucity of strategies for developing health literate organisations: A systematic review. PLoS ONE 2018, 13, e0195018. [Google Scholar] [CrossRef]
- Australian Government—Department of Health. National Health Literacy Strategy Framework Consultation. November 2022. Available online: https://consultations.health.gov.au/national-preventive-health-taskforce/national-health-literacy-strategy-framework-consul/ (accessed on 27 April 2023).
- National Diabetes Services Scheme. Diabetes Map. Canberra ACT: Australian Government. 2021. Available online: https://www.ndss.com.au/about-the-ndss/diabetes-facts-and-figures/australian-diabetes-map/ (accessed on 28 April 2022).
- National Indigenous Australians Agency. Tier 1—Health Status and Outcomes. Australia Government: Canberra, ACT, Australia. 2023. Available online: https://www.indigenoushpf.gov.au/measures/1-09-diabetes (accessed on 27 April 2023)Australia Government: Canberra, ACT, Australia.
- Australian Bureau of Statistics. Health Conditions Prevalence: Key Findings on Selected Long-Term Health Conditions and Prevalence in Australia 2020–2021. 2022. Available online: https://www.abs.gov.au/statistics/health/health-conditions-and-risks/health-conditions-prevalence/2020-21#key-statistics (accessed on 27 April 2023).
- Department of Health (Australian Government). National Medical Workforce Strategy 2021–2031: Investing in Our Medical Workforce to Meet Australia’s Health Needs. Publication No. DT0002141. 2022. Available online: https://www.health.gov.au/resources/publications/national-medical-workforce-strategy-2021-2031 (accessed on 27 April 2023).
- Diabetes Australia. About Us. Canberra ACT: Diabetes Australia. 2022. Available online: https://www.diabetesaustralia.com.au/about-us/ (accessed on 28 April 2022).
- National Diabetes Services Scheme. About the NDSS. Canberra ACT: Australian Government. 2022. Available online: https://www.ndss.com.au/about-the-ndss/ (accessed on 28 April 2022).
- Zhang, X.; Majid, S.; Foo, S. Environmental Scanning: An Application of Information Literacy Skills at the Workplace. J. Inf. Sci. 2010, 36, 719–732. [Google Scholar] [CrossRef]
- Charlton, P.; Doucet, S.; Azar, R.; Nagel, D.A.; Boulos, L.; Luke, A.; Mears, K.; Kelly, K.J.; Montelpare, W.J. The use of the environmental scan in health services delivery research: A scoping review protocol. BMJ Open 2019, 9, e029805. [Google Scholar] [CrossRef] [PubMed]
- Erlingsson, C.; Brysiewicz, P. A hands-on guide to doing content analysis. Afr. J. Emerg. Med. 2017, 7, 93–99. [Google Scholar] [CrossRef] [PubMed]
- McAlearney, A.S.; Walker, D.; Moss, A.D.; Bickell, N.A. Using Qualitative Comparative Analysis of Key Informant Interviews in Health Services Research: Enhancing a Study of Adjuvant Therapy Use in Breast Cancer Care. Med. Care 2016, 54, 400–405. [Google Scholar] [CrossRef]
- Jenkins, E.; McGuinness, L.; Haines-Saah, R.; Andres, C.; Ziemann, M.-J.; Morris, J.; Waddell, C. Equipping youth for meaningful policy engagement: An environmental scan. Health Promot. Int. 2020, 35, 852–865. [Google Scholar] [CrossRef]
- Rowel, R.; Moore, N.D.; Nowrojee, S.; Memiah, P.; Bronner, Y. The utility of the environmental scan for public health practice: Lessons from an urban program to increase cancer screening. J. Natl. Med. Assoc. 2005, 97, 527–534. [Google Scholar] [PubMed]
- Elliott, V. Thinking about the coding process in qualitative data analysis. Qual. Rep. 2018, 23, 2850–2861. Available online: https://nsuworks.nova.edu/tqr/vol23/iss11/14 (accessed on 27 April 2023). [CrossRef]
- Lin, S.; Ayre, J.; Muscat, D. How readable are Australian multilingual diabetes patient education materials? An evaluation of national English-language source texts. Public Health Res. Pract. 2020, 30, 3012002. [Google Scholar] [CrossRef]
- Shoemaker, S.J.; Wolf, M.S.; Brach, C. Development of the Patient Education Materials Assessment Tool (PEMAT): A new measure of understandability and actionability for print and audiovisual patient information. Patient Educ. Couns. 2014, 96, 395–403. [Google Scholar] [CrossRef]
- Agency for Healthcare Research and Quality. The Patient Education Materials Assessment Tool (PEMAT) and User’s Guide. Rockville, Maryland USA: US Department of Health and Human Services; 2022. Available online: https://www.ahrq.gov/health-literacy/patient-education/pemat-p.html (accessed on 20 June 2022).
- Lipari, M.; Berlie, H.; Saleh, Y.; Hang, P.; Moser, L. Understandability, actionability, and readability of online patient education materials about diabetes mellitus. Am. J. Health Syst. Pharm. 2019, 76, 182–186. [Google Scholar] [CrossRef]
- Lin, S.; Ayre, J.; Muscat, D. An evaluation of understandability and actionability of Australian multilingual diabetes patient education materials in English and Chinese. Aust. Diabetes Educ. 2020, 23, 1–12. [Google Scholar]
- Australian Bureau of Statistics. 4228.0—Adult Literacy and Life Skills Survey, Summary Results, Australia 2006; Australia Government: Canberra, ACT, Australia, 2013; (Released 9 January 2008 and Reissue). Available online: https://www.abs.gov.au/AUSSTATS/[email protected]/Lookup/4228.0Main+Features12006%20(Reissue) (accessed on 28 April 2022).
- Australian Bureau of Statistics. National Health Survey 2018—Health Literacy. Canberra, ACT: Australian Government. 2019. Available online: https://www.abs.gov.au/statistics/health/health-conditions-and-risks/national-health-survey-health-literacy/latest-release (accessed on 28 April 2022).
- Australian Commission on Safety and Quality in Health Care. National Statement on Health Literacy—Taking Action to Improve Safety and Quality. Sydney, NSW: Australian Government. 2014. Available online: https://www.safetyandquality.gov.au/publications-and-resources/resource-library/national-statement-health-literacy-taking-action-improve-safety-and-quality (accessed on 28 April 2022).
- Diabetes Australia. Diabetes Australia 2019–2020 Financial Report; Diabetes Australia: Canberra, ACT, Australia, 2022; Volume 11, Available online: https://www.diabetesaustralia.com.au/about-us/annual-reports/ (accessed on 28 April 2022).
- Diabetes Australia. Translated Resources; Diabetes Australia: Canberra, ACT, Australia, 2022; Available online: https://www.diabetesaustralia.com.au/news-resources/translated-resources/ (accessed on 28 April 2022).
- Martin, F.I.R. A History of Diabetes in Australia; Diabetes Australia: Canberra, ACT, Australia, 2022; Available online: https://www.diabetesaustralia.com.au/about-us/history/ (accessed on 28 April 2022).
- National Diabetes Services Scheme. NDSS Projects. 58–61. 2016. Available online: https://ade.adea.com.au/are-diabetes-consumer-education-materials-easy-to-understand-and-act-on-an-evaluation-of-multilingual-australian-resources/ (accessed on 27 April 2023).
- Speight, J.; Skinner, T.C.; Dunning, T.; Black, T.; Kilov, G.; Lee, C.; Scibilia, R.; Johnson, G. Our language matters: Improving communication with and about people with diabetes. A position statement by Diabetes Australia. Diabetes Res. Clin. Pract. 2021, 7, 108655. [Google Scholar] [CrossRef]
- Australian Diabetes Educators Association (ADEA) & Diabetes Australia. Health Literacy Position Statement–Person-Centred Care Toolkit; ADEA: Canberra, ACT, Australia, 2016; Available online: https://www.adea.com.au/wp-content/uploads/2017/06/PRINT_CDE_TOOLKIT_FINAL_170524.pdf (accessed on 11 June 2020).
- Department of Health. Australian National Diabetes Strategy 2016–2020; Australia Government: Canberra, ACT, Australia, 15 November 2015. Available online: https://www.health.gov.au/resources/publications/australian-national-diabetes-strategy-2016-2020 (accessed on 28 April 2022).
- Department of Health and Aging. Review of CGM Product Provided through the NDSS. 2021. Available online: https://www.health.gov.au/initiatives-and-programs/review-of-cgm-products-provided-through-the-ndss (accessed on 27 April 2023).
- Digital Transformation Agency. National Diabetes Services Scheme Enhancement Project—Live Assessments; Australian Government: Canberra, ACT, Australia, 2019. Available online: https://www.dta.gov.au/help-and-advice/digital-service-standard/assessment-reports/national-diabetes-services-scheme-enhancement-project-live-assessment-phase-1 (accessed on 2 June 2022).
- Cremer, G. Personal Communication with Gil Cremer, National Manager Programs, National Diabetes Services Scheme; Diabetes Australia: Canberra, ACT, Australia, 2021. [Google Scholar]
- Department of Health. Australian National Diabetes Strategy 2021–2030; Commonwealth of Australia: Canberra, ACT, Australia, 21 November 2021. Available online: https://www.health.gov.au/resources/publications/australian-national-diabetes-strategy-2021-2030 (accessed on 28 April 2022).
- Thygesen, L.C.; Ersbøll, A.K. When the entire population is the sample: Strengths and limitations in register-based epidemiology. Eur. J. Epidemiol. 2014, 29, 551–558. [Google Scholar] [CrossRef] [PubMed]
- Belair-Gagnon, V.; Nelson, J.L.; Lewis, S.C. Audience Engagement, Reciprocity, and the Pursuit of Community Connectedness in Public Media Journalism. Journal. Pract. 2019, 13, 558–575. [Google Scholar] [CrossRef]
- Alper, J.; McHugh, M.K. The Roles of Trust and Health Literacy in Achieving Health Equity Clinical Settings: Proceedings of a Workshop; (for Board on Population Health and Public Health Practice); Roundtable on Health Literacy; The National Academies Press: Washington, DC, USA, 2023; Available online: https://nap.nationalacademies.org/catalog/26888/the-roles-of-trust-and-health-literacy-in-achieving-health-equity (accessed on 27 April 2023).
- Lagasse, J. Why Branding in Healthcare is More Important than Ever, and How to Connect with Consumers. Healthcare Finance. 8 November 2018. Available online: https://www.healthcarefinancenews.com/news/why-branding-healthcare-more-important-ever-and-how-connect-consumers (accessed on 27 April 2023).
- Kemp, E.; Jillapalli, R.; Becerra, E. Healthcare branding: Developing emotionally based consumer-brand relationships. J. Serv. Mark. 2014, 28, 126–137. [Google Scholar] [CrossRef]
- Cooper, A.; Kanumilli, N.; Hill, J.; Holt, R.I.G.; Howarth, D.; Lloyd, C.E.; Kar, P.; Nagi, D.; Naik, S.; Nash, J.; et al. Language matters. Addressing the use of language in the care of people with diabetes: Position statement of the English Advisory Group. Diabet. Med. A J. Br. Diabet. Assoc. 2018, 35, 1630–1634. [Google Scholar] [CrossRef] [PubMed]
- Lewis, D.M. Language Matters in Diabetes and in Diabetes Science and Research. J. Diabetes Sci. Technol. 2022, 16, 1057–1058. [Google Scholar] [CrossRef] [PubMed]
- Banasiak, K.; Cleary, D.; Bajurny, V.; Barbieri, P.; Nagpal, S.; Sorensen, M.; Tabiou, N.; Witteman, H.; Senior, P. Language Matters–A Diabetes Canada Consensus Statement. Can. J. Diabetes 2020, 44, 370–373. [Google Scholar] [CrossRef]
- Schippers, M.C.; Rus, D.C. Optimizing decision-making processes in times of COVID-19: Using reflexivity to counteract information-processing failures. Front. Psychol. 2021, 22, 12. Available online: https://www.frontiersin.org/article/10.3389/fpsyg.2021.650525 (accessed on 27 April 2023). [CrossRef]
- Jackson, D.; Moorley, C. ‘Nothing about us without us’: Embedding participation in peer review processes. J. Adv. Nurs. 2022, 78, e75–e76. [Google Scholar] [CrossRef]
- Beck, J.M.; Elliott, K.C.; Booher, C.R.; Renn, K.A.; Montgomery, R.A. The application of reflexivity for conservation science. Biol. Conserv. 2021, 262, 109322. [Google Scholar] [CrossRef]
- Abdi, I.; Murphy, B.; Seale, H. Evaluating the health literacy demand and cultural appropriateness of online immunisation information available to refugee and migrant communities in Australia. Vaccine 2020, 38, 6410–6417. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| FACT SHEET | 2006 | 2010 | 2016 | 2021 | ||||
|---|---|---|---|---|---|---|---|---|
| Under-Standability (%) | Action- Ability (%) | Under- Standability (%) | Action- Ability (%) | Under- Standability (%) | Action- Ability (%) | Under Standability (%) | Action- Ability (%) | |
| Category GENERAL | ||||||||
| Prediabetes | 50 | 33 | 57 | 33 | 63 | 40 | 81 | 67 |
| Category LIFESTYLE | ||||||||
| Coeliac diseases and diabetes | 57 | 67 | 53 | 67 | 63 | 80 | 71 | 100 |
| Glycaemic index | 43 | 17 | 53 | 50 | 94 | 83 | 88 | 83 |
| Category MEDICAL | ||||||||
| Sick days for type 2 diabetes | 43 | 33 | 47 | 71 | 81 | 100 | 81 | 80 |
| Staying well with diabetes/diabetes-related complications | 71 | 67 | 77 | 60 | 75 | 60 | 75 | 80 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Murfet, G.O.; Lin, S.; Ridd, J.C.; Cremer, G.H.; Davidson, S.; Muscat, D.M. Shifts in Diabetes Health Literacy Policy and Practice in Australia—Promoting Organisational Health Literacy. Int. J. Environ. Res. Public Health 2023, 20, 5778. https://doi.org/10.3390/ijerph20105778
Murfet GO, Lin S, Ridd JC, Cremer GH, Davidson S, Muscat DM. Shifts in Diabetes Health Literacy Policy and Practice in Australia—Promoting Organisational Health Literacy. International Journal of Environmental Research and Public Health. 2023; 20(10):5778. https://doi.org/10.3390/ijerph20105778
Chicago/Turabian StyleMurfet, Giuliana O., Shanshan Lin, Jan C. Ridd, Gunhild H. Cremer, Susan Davidson, and Danielle M. Muscat. 2023. "Shifts in Diabetes Health Literacy Policy and Practice in Australia—Promoting Organisational Health Literacy" International Journal of Environmental Research and Public Health 20, no. 10: 5778. https://doi.org/10.3390/ijerph20105778
APA StyleMurfet, G. O., Lin, S., Ridd, J. C., Cremer, G. H., Davidson, S., & Muscat, D. M. (2023). Shifts in Diabetes Health Literacy Policy and Practice in Australia—Promoting Organisational Health Literacy. International Journal of Environmental Research and Public Health, 20(10), 5778. https://doi.org/10.3390/ijerph20105778