

Developing a Model for Integrating of Tuberculosis, Human Immunodeficiency Virus and Primary Healthcare Services in Oliver Reginald (O.R) Tambo District, Eastern Cape, South Africa


{kind=link}
Abstract
:1. Introduction
2. Study Aim and Setting
3. Methods
3.1. Part 1
3.2. Part 2
3.3. Part 3
3.4. Validity
3.5. Reliability
3.6. Definition of Operational Concepts
4. Results
4.1. Some Key Findings from the Original Investigations (Parts 1, 2, and 3)
4.2. Model Synthesis
4.3. Derivation
4.4. Deductive Reasoning
4.5. Inductive Reasoning
4.6. Concept Analysis
4.7. The model Validation Phase
4.8. Model Validation
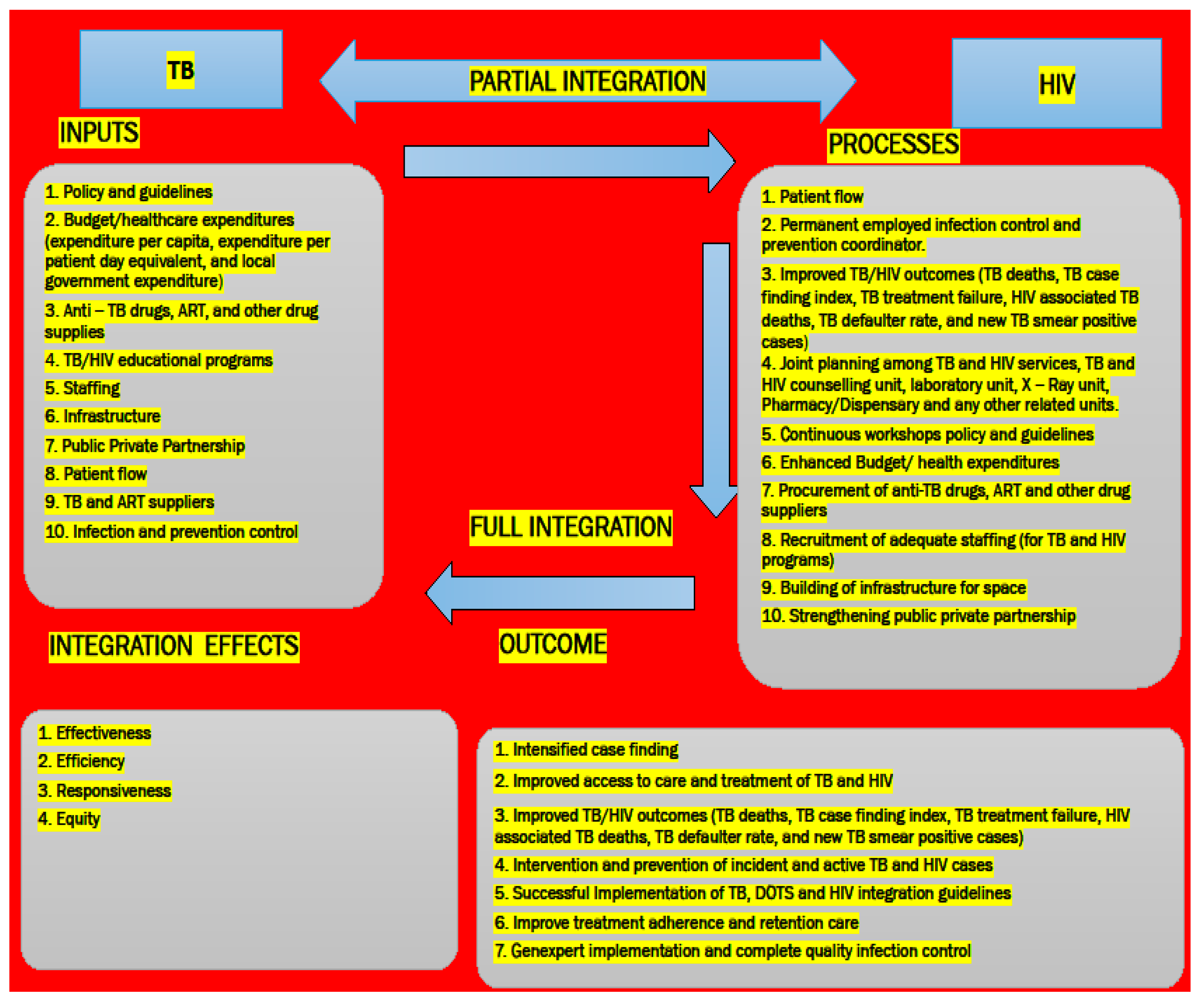
5. Discussion: Creation of the Model
5.1. Inputs
5.2. Processes
5.3. Outcome
5.4. Integration Effects
5.5. Building Capacity through Instruction and Guidance
6. Conclusions and Recommendations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. HIV-Associated Tuberculosis; WHO, Ed.; WHO: Geneva, Switzerland, 2015. [Google Scholar]
- Croome, N.; Ahluwalia, M.; Hughes, L.D.; Abas, M. Patient-reported barriers and facilitators to antiretroviral adherence in sub-Saharan Africa. AIDS 2017, 31, 995–1007. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Policy on Collaborative TB/HIV Activities Guidelines for National Programmes and Other Stakeholders; World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- National Department of Health. A Practical Guide for TB and HIV Service Integration at Primary Health Care Facilities; National Department of Health: Pretoria, South Africa, 2012. [Google Scholar]
- World Health Organization. Global Tuberculosis Report; WHO: Geneva, Switzerland, 2019. [Google Scholar]
- Silva Escada, R.O.; Velasque, L.; Ribeiro, S.R.; Cardoso, S.W.; Spindola Marins, L.M.; Grinsztejn, E.; da Silva Lourenço, M.C.; Grinsztejn, B.; Veloso, V.G. Mortality in patients with HIV-1 and tuberculosis co-infection in Rio de Janeiro, Brazil—Associated factors and causes of death. BMC Infect. Dis. 2017, 17, 373. [Google Scholar] [CrossRef] [PubMed]
- Legido-Quigley, L.; Montgomery, C.M.; Khan, P.; Atun, R.; Fakoya, A.; Getahun, H.; Grant, A.D. Integrating tuberculosis and HIV services in low- and- middle-income countries: A systematic review. Trop. Med. Int. Health 2013, 18, 199–211. [Google Scholar] [CrossRef]
- World Health Organization. Global Tuberculosis Report; World Health Organization: Geneva, Switzerland, 2020; Available online: https://apps.who.int/iris/bitstream/handle/10665/336069/9789240013131-eng.pdf (accessed on 28 March 2023).
- Harries, A.D.; Lin, Y.; Kumar, A.M.V.; Satyanarayana, S.; Takarinda, K.C.; Dlodlo, R.A.; Zachariah, R.; Olliaro, P. What can national TB control programmes in low- and middle-income countries do to end tuberculosis by 2030? F1000Research 2018, 7, 1011. [Google Scholar] [CrossRef]
- Owiti, P.; Zachariah, R.; Bissell, K.; Kumar, A.M.; Diero, L.; Carter, E.J.; Gardner, A. Integrating tuberculosis and HIV services in rural Kenya: Uptake and outcomes. Public Health Action 2015, 5, 36–44. [Google Scholar] [CrossRef]
- Anku, P.J.; Amo-Adjei, J.; Doku, D.T.; Kumi-Kyereme, A. Integration of tuberculosis and HIV services: Exploring the perspectives of co-infected patients in Ghana. Glob. Public Health 2018, 13, 1192–1203. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Tuberculosis Report; World Health Organization: Geneva, Switzerland, 2021; Available online: https://www.who.int/publications/i/item/9789240037021 (accessed on 29 March 2023).
- UNAIDS. Tuberculosis and HIV UNAIDS. In Joint United Nations Programme on HIV/AIDS 2019; Wolters Kluwer: Alphen aan den Rijn, The Netherlands, 2019. [Google Scholar]
- Herce, M.E.; Morse, J.; Luhanga, D.; Harris, J.; Smith, H.J.; Besa, S.; Samungole, G.; Kancheya, N.; Muyoyeta, M.; Reid, S.E. Integrating HIV care and treatment into tuberculosis clinics in Lusaka, Zambia: Results from a before-after quasi-experimental study. BMC Infect Dis. 2018, 18, 536. [Google Scholar] [CrossRef]
- Burnett, S.M.; Zawedde-Muyanja, S.; Hermans, S.M.; Weaver, M.R.; Colebunders, R.; Manabe, Y.C. Effect of TB/HIV Integration on TB and HIV Indicators in Rural Ugandan Health Facilities. J. Acquir. Immune Defic. Syndr. 2018, 79, 605–611. [Google Scholar] [CrossRef]
- Torpey, K.; Agyei-Nkansah, A.; Ogyiri, L.; Forson, A.; Lartey, M.; Ampofo, W.; Akamah, J.; Puplampu, P. Management of TB/HIV co-infection: The state of the evidence. Ghana Med. J. 2020, 54, 186–196. [Google Scholar] [CrossRef]
- Cazabon, D.; Alsdurf, H.; Satyanarayana, S.; Nathavitharana, R.; Subbaraman, R.; Daftary, A.; Pai, M. Quality of tuberculosis care in high burden countries: The urgent need to address gaps in the care cascade. Int. J. Infect. Dis. 2017, 56, 111–116. [Google Scholar] [CrossRef]
- Dlatu, N.; Oladimeji, K.E.; Apalata, T. Voices from the Patients: A Qualitative Study of the Integration of Tuberculosis, Human Immunodeficiency Virus and Primary Healthcare Services in O.R Tambo District, Eastern Cape, South Africa. Infect. Dis. Rep. 2023, 15, 158–170. [Google Scholar] [CrossRef]
- Chakaya, J.; Castro, J.L.; Jensen, P.M.; Fujiwara, P.I. A new era for global tuberculosis: Holding leaders accountable for promises. Int. J. Tuberc. Lung Dis. 2018, 22, 1387. [Google Scholar] [CrossRef] [PubMed]
- Padayatchi, N.; Daftary, A.; Naidu, N.; Naidoo, K.; Pai, M. Tuberculosis: Treatment failure, or failure to treat? Lessons from India and South Africa. BMJ Glob. Health 2019, 4, e001097. [Google Scholar] [CrossRef] [PubMed]
- Manson, S. Simplifying complexity: A review of complexity theory. Geoforum 2001, 32, 405–414. [Google Scholar] [CrossRef]
- Duarte, R.; Lönnroth, K.; Carvalho, C.; Lima, F.; Carvalho, A.C.C.; Muñoz-Torrico, M.; Centis, R. Tuberculosis, social determinants and co-morbidities (including HIV). Pulmonology 2018, 24, 115–119. [Google Scholar] [CrossRef]
- Loveday, M.; Padayatchi, N.; Wallengren, K.; Roberts, J.; Brust, J.C.M.; Ngozo, J.; Master, I.; Voce, A. Association between Health Systems Performance and Treatment Outcomes in Patients Co-Infected with MDR-TB and HIV in KwaZulu-Natal, South Africa: Implications for TB Programmes. PLoS ONE 2014, 9, e94016. [Google Scholar] [CrossRef]
- De Vries, S.G.; Cremers, A.L.; Heuvelings, C.C.; Greve, P.F.; Visser, B.J.; Belard, S.; Janssen, S.; Spijker, R.; Shaw, B.; Hill, R.A.; et al. Barriers and facilitators to the uptake of tuberculosis diagnostic and treatment services by hard-to-reach populations in countries of low and medium tuberculosis incidence: A systematic review of qualitative literature. Lancet Infect. Dis. 2017, 17, e128–e143. [Google Scholar] [CrossRef]
- Pai, M.; Temesgen, Z. Quality: The missing ingredient in TB care and control. J. Clin. Tuberc. Other Mycobact. Dis. 2019, 14, 12–13. [Google Scholar] [CrossRef]
- Sinshaw, Y.; Alemu, S.; Fekadu, A.; Gizachew, M. Successful TB treatment outcome and its associated factors among TB/HIV co infected patients attending Gondar University Referral Hospital, Northwest Ethiopia: An institution based cross sectional study. BMC Infect. Dis. 2017, 17, 132. [Google Scholar] [CrossRef] [PubMed]
- Secretary of Jan Swasthya Sahyog; Laux, T.S.; Patil, S. Predictors of tuberculosis treatment outcomes among a retrospective cohort in rural, Central India. J. Clin. Tuberc. Other Mycobact. Dis. 2018, 12, 41–47. [Google Scholar]
- South African National Department of Health. Let Our Actions Count: South Africa’s National Strategic Plan on HIV, AIDS, and STIs 2017–2022. 2017. Available online: http://sanac.org.za/wp-content/uploads/2017/05/NSP_FullDocument_FINAL.pdf (accessed on 25 May 2023).
- World Health Organization (WHO). The End TB Strategy. Global Strategy and Targets for Tuberculosis Prevention, Care and Control after 2015; WHO: Geneva, Switzerland, 2015; p. 2. [Google Scholar]
- Uyei, J.; Coetzee, D.; Macinko, J.; Weinberg, S.L.; Guttmacher, S. Measuring the degree of integrated tuberculosis and HIV service delivery in Cape Town. South Afr. Health Policy Plan. 2014, 29, 42–55. [Google Scholar] [CrossRef] [PubMed]
- Dlatu, N.; Longo-Mbenza, B.; Apalata, T. Predictors of tuberculosis incidence and the effects of multiple deprivation indices on tuberculosis management in O.R Tambo district over a 5-year period. PLoS ONE 2022, 17, e0264811. [Google Scholar] [CrossRef] [PubMed]
- Statistics South Africa. Census 2011 Statistical Release, Pretoria, South Africa—P0301.4; Statistics South Africa: Pretoria, South Africa, 2012. [Google Scholar]
- Obaromi, D.; Ndege, J.; Yongsong, Q. Disease mapping of tuberculosis prevalence in Eastern Cape Province, South Africa. J. Public Health 2018, 27, 241–248. [Google Scholar] [CrossRef]
- Brink, H.; Van der Walt, C.; Van Rensburg, G. Fundamentals of Research Methodology for Health Care Professionals, 3rd ed.; Juta & Co.: Cape Town, South Africa, 2012. [Google Scholar]
- Dlatu, N.; Longo-Mbenza, B.; Apalata, T. Research Square: Models of Integration of TB and HIV Services and Factors associated with Perceived Quality of TB-HIV integrated Service Delivery in OR Tambo District, South Africa. Res. Sq. 2022. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dlatu, N.; Longo-Mbenza, B.; Oladimeji, K.E.; Apalata, T. Developing a Model for Integrating of Tuberculosis, Human Immunodeficiency Virus and Primary Healthcare Services in Oliver Reginald (O.R) Tambo District, Eastern Cape, South Africa. Int. J. Environ. Res. Public Health 2023, 20, 5977. https://doi.org/10.3390/ijerph20115977
Dlatu N, Longo-Mbenza B, Oladimeji KE, Apalata T. Developing a Model for Integrating of Tuberculosis, Human Immunodeficiency Virus and Primary Healthcare Services in Oliver Reginald (O.R) Tambo District, Eastern Cape, South Africa. International Journal of Environmental Research and Public Health. 2023; 20(11):5977. https://doi.org/10.3390/ijerph20115977
Chicago/Turabian StyleDlatu, Ntandazo, Benjamin Longo-Mbenza, Kelechi Elizabeth Oladimeji, and Teke Apalata. 2023. "Developing a Model for Integrating of Tuberculosis, Human Immunodeficiency Virus and Primary Healthcare Services in Oliver Reginald (O.R) Tambo District, Eastern Cape, South Africa" International Journal of Environmental Research and Public Health 20, no. 11: 5977. https://doi.org/10.3390/ijerph20115977
APA StyleDlatu, N., Longo-Mbenza, B., Oladimeji, K. E., & Apalata, T. (2023). Developing a Model for Integrating of Tuberculosis, Human Immunodeficiency Virus and Primary Healthcare Services in Oliver Reginald (O.R) Tambo District, Eastern Cape, South Africa. International Journal of Environmental Research and Public Health, 20(11), 5977. https://doi.org/10.3390/ijerph20115977