
Evaluating Somatic Experiencing® to Heal Cancer Trauma: First Evidence with Breast Cancer Survivors



Abstract
:1. Introduction
The Somatic Experiencing® Model
2. Aim and Hypothesis
3. Materials and Methods
3.1. The Intervention
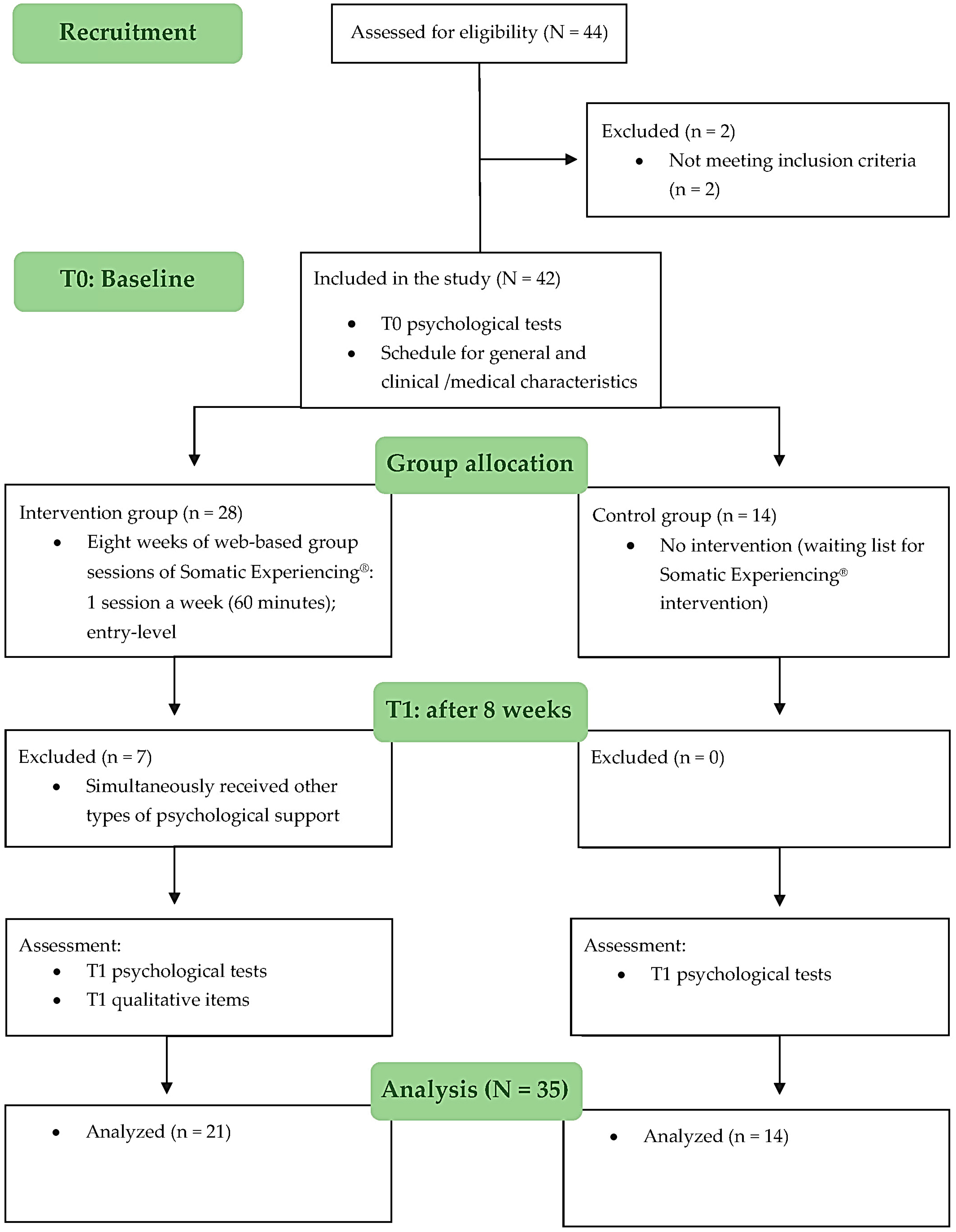
3.2. Study Design and Participants
3.3. Procedure and Data Collection
3.4. Measures
4. Data Analysis
5. Results
5.1. Sample Characteristics
5.2. Group Comparisons
5.3. Qualitative Findings at the End of the Intervention (n = 21, Somatic Experiencing® Group)
6. Discussion
Limitations and Future Directions of Research
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Swartzman, S.; Booth, J.N.; Munro, A.; Sani, F. Posttraumatic stress disorder after cancer diagnosis in adults: A meta-analysis. Depress. Anxiety 2017, 34, 327–339. [Google Scholar] [CrossRef] [Green Version]
- Arnaboldi, P.; Riva, S.; Crico, C.; Pravettoni, G. A systematic literature review exploring the prevalence of post-traumatic stress disorder and the role played by stress and traumatic stress in breast cancer diagnosis and trajectory. Breast Cancer Targets Ther. 2017, 9, 473. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dinapoli, L.; Colloca, G.; di Capua, B.; Valentini, V. Psychological Aspects to Consider in Breast Cancer Diagnosis and Treatment. Curr. Oncol. Rep. 2021, 23, 38. [Google Scholar] [CrossRef] [PubMed]
- Saita, E.; Acquati, C.; Molgora, S.; Vagnini, D.; Piccolo, E.M.; Valenti, F.; Stratta, G.; Grassi, M.M. Locally advanced breast cancer (LABC) and delayed care: A qualitative analysis of psychosocial factors. Psychol. Health Med. 2023, 28, 408–418. [Google Scholar] [CrossRef]
- Álvarez-Pardo, S.; De Paz, J.A.; Montserrat Romero-Pérez, E.; Portilla-Cueto, K.M.; Horta-Gim, M.A.; González-Bernal, J.J.; Fernández-Solana, J.; Mielgo-Ayuso, J.; García-Valverde, A.; González-Santos, J. Factors Associated with Body Image and Self-Esteem in Mastectomized Breast Cancer Survivors. Int. J. Environ. Res. Public Health 2023, 20, 5154. [Google Scholar] [CrossRef]
- Kuhfuß, M.; Maldei, T.; Hetmanek, A.; Baumann, N. Somatic experiencing—Effectiveness and key factors of a body-oriented trauma therapy: A scoping literature review. Eur. J. Psychotraumatol. 2021, 12, 1929023. [Google Scholar] [CrossRef]
- Thakur, M.; Sharma, R.; Mishra, A.K.; Gupta, B. Body image Disturbances Among Breast Cancer Survivors: A Narrative Review of Prevalence and Correlates. Cancer Res. Treat. 2022, 5, 90. [Google Scholar] [CrossRef]
- Tumori. Available online: https://www.epicentro.iss.it/tumori/aggiornamenti (accessed on 19 March 2023).
- De Vrieze, T.; Nevelsteen, I.; Thomis, S.; De Groef, A.; Tjalma, W.A.A.; Gebruers, N.; Devoogdt, N. What are the economic burden and costs associated with the treatment of breast cancer-related lymphoedema? A systematic review. Support. Care Cancer 2020, 28, 439–449. [Google Scholar] [CrossRef] [PubMed]
- Giese-Davis, J.; Collie, K.; Rancourt, K.M.S.; Neri, E.; Kraemer, H.C.; Spiegel, D. Decrease in Depression Symptoms is Associated with Longer Survival in Patients with Metastatic Breast Cancer: A secondary Analysis. J. Clin. Oncol. 2011, 29, 413–420. [Google Scholar] [CrossRef] [Green Version]
- Saita, E.; Ferraris, G.; Acquati, C.; Molgora, S.; Sorge, A.; Valenti, F.; Grassi, M.M.; Vagnini, D. Dyadic Profiles of Couples Coping with Body Image Concerns after Breast Cancer: Preliminary Results of a Cluster Analysis. Front. Psychol. 2022, 13, 869905. [Google Scholar] [CrossRef] [PubMed]
- Spiegel, D.; Bloom, J.R.; Kraemer, H.C.; Gottheil, E. Effect of Psychosocial Treatment on Survival of Patients with Metastatic Breast Cancer. Lancet 1989, 2, 888–891. [Google Scholar] [CrossRef]
- Sun, Y.; Shigaki, C.L.; Armer, J.M. Return to work among breast cancer survivors: A literature review. Support. Care Cancer 2017, 25, 709–718. [Google Scholar] [CrossRef] [PubMed]
- Almeida, A.K.; Macedo, S.C.G.D.M.; Sousa, M.B.C.D. A systematic review of somatic intervention treatments in PTSD: Does Somatic Experiencing® (SE®) have the potential to be a suitable choice? Estud. Psicol. (Natal) 2019, 24, 237–246. [Google Scholar] [CrossRef]
- Husebø, A.M.L.; Husebø, T.L. Quality of life and breast cancer: How can mind–body exercise therapies help? An overview study. Sports 2017, 5, 79. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muehsam, D.; Lutgendorf, S.; Mills, P.J.; Rickhi, B.; Chevalier, G.; Bat, N.; Chopra, D.; Gurfein, B. The embodied mind: A review on functional genomic and neurological correlates of mind-body therapies. Neurosci. Biobehav. Rev. 2017, 73, 165–181. [Google Scholar] [CrossRef] [PubMed]
- Taylor, A.G.; Goehler, L.E.; Galper, D.I.; Innes, K.E.; Bourguignon, C. Top-down and bottom-up mechanisms in mind-body medicine: Development of an integrative framework for psychophysiological research. Explore 2010, 6, 29–41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carlson, L.E.; Zelinski, E.; Toivonen, K.; Flynn, M.; Qureshi, M.; Piedalue, K.A.; Grant, R. Mind-Body Therapies in Cancer: What Is the Latest Evidence? Curr. Oncol. Rep. 2017, 19, 67. [Google Scholar] [CrossRef] [PubMed]
- Appling, S.E.; Scarvalone, S.; MacDonald, R.; McBeth, M.; Helzlsouer, K.J. Fatigue in breast cancer survivors: The impact of a mind-body medicine intervention. Oncol. Nurs. Forum 2012, 39, 278–286. [Google Scholar] [CrossRef]
- Morone, N.E.; Greco, C.M. Mind-body interventions for chronic pain in older adults: A structured review. Pain Med. 2007, 8, 359–375. [Google Scholar] [CrossRef]
- Taylor, P.J.; Saint-Laurent, R. Group Psychotherapy Informed by the Principles of Somatic Experiencing: Moving Beyond Trauma to Embodied Relationship. Int. J. Group Psychother. 2017, 67, S171–S181. [Google Scholar] [CrossRef] [Green Version]
- Larson, J.L.; Rosen, A.B.; Wilson, F.A. The effect of telehealth interventions on quality of life of cancer survivors: A systematic review and meta-analysis. Health Inform. J. 2020, 26, 1060–1078. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rocque, G.B.; Halilova, K.I.; Varley, A.L.; Williams, C.P.; Taylor, R.A.; Masom, D.G.; Wright, W.J.; Partridge, E.E.; Kvale, E.A. Feasibility of a Telehealth Educational Program on Self-Management of Pain and Fatigue in Adult Cancer Patients. J. Pain Symptom Manag. 2017, 53, 1071–1078. [Google Scholar] [CrossRef]
- Sansom-Daly, N.; Thongseiratch, T. Online Interventions to Improve Mental Health of Pediatric, Adolescent, and Young Adult Cancer Survivors: A Systematic Review and Meta-Analysis. Front. Psychiatry 2021, 12, 784615. [Google Scholar] [CrossRef]
- Levine, P. A Waking the Tiger: Healing Trauma; North Atlantic Books: Berkeley, CA, USA, 1997. [Google Scholar]
- Levine, P.A. An Unspoken Voice: How the Body Releases Trauma and Restores Goodness; North Atlantic Books: Berkeley, CA, USA, 2010. [Google Scholar]
- Levine, P.A. Somatic Experiencing: Esperienze Somatiche Nella Risoluzione del Trauma; Casa Editrice Astrolabio: Roma, Italy, 2014. [Google Scholar]
- Levine, P.A.; Blakeslee, A.; Sylvae, J. Reintegrating Fragmentation of the Primitive Self: Discussion of “Somatic Experiencing”. Psychoanal. Dialogues 2018, 28, 620–628. [Google Scholar] [CrossRef]
- Payne, P.; Levine, P.; Crane-Godreau, M. Somatic experiencing: Using interoception and proprioception as core elements of trauma therapy. Front. Psychol. 2015, 6, 93. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levit, D. Somatic Experiencing: In the Realms of Trauma and Dissociation—What We Can Do, When What We Do, Is Really Not Good Enough. Psychoanal. Dialogues 2018, 28, 586–601. [Google Scholar] [CrossRef]
- Porges, S.W. The Polyvagal Theory: Neurophysiological Foundations of Emotions, Attachment, Communication, and Self-Regulation; Norton: New York, NY, USA, 2011. [Google Scholar]
- Van der Kolk, B. The Body Keeps Score: Brain, Mind, and Body in the Healing of Trauma; Penguin Book: London, UK, 2014. [Google Scholar]
- Brom, D.; Stokar, Y.; Lawi, C.; Nuriel-Porat, V.; Ziv, Y.; Lerner, K.; Ross, G. Somatic experiencing for posttraumatic stress disorder: A randomized controlled outcome study. J. Trauma Stress 2017, 30, 304–312. [Google Scholar] [CrossRef] [PubMed]
- Leitch, M.L. Somatic experiencing treatment with tsunami survivors in Thailand: Broadening the scope of early intervention. Traumatology 2007, 13, 11–20. [Google Scholar] [CrossRef] [Green Version]
- Leitch, M.L.; Vanslyke, J.; Allen, M. Somatic experiencing treatment with social service workers following Hurricanes Katrina and Rita. Soc. Work 2009, 54, 9–18. [Google Scholar] [CrossRef] [Green Version]
- Parker, C.; Doctor, R.M.; Selvam, R. Somatic therapy treatment effects with tsunami survivors. Traumatology 2008, 14, 103–109. [Google Scholar] [CrossRef] [Green Version]
- Andersen, T.E.; Lahav, Y.; Ellegaard, H.; Manniche, C. A randomized controlled trial of brief somatic experiencing for chronic low back pain and comorbid post-traumatic stress disorder symptoms. Eur. J. Psychotraumatol. 2017, 8, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Briggs, P.C.; Hayes, S.; Changaris, M. Somatic Experiencing® informed therapeutic group for the care and treatment of biopsychosocial effects upon a gender diverse identity. Front. Psychiatry 2018, 9, 53. [Google Scholar] [CrossRef] [Green Version]
- Winblad, N.E.; Changaris, M.; Stein, P.K. Effect of somatic experiencing resiliency-based trauma treatment training on quality of life and psychological health as potential markers of resilience in treating professionals. Front. Neurosc. 2018, 12, 70. [Google Scholar] [CrossRef] [Green Version]
- Levine, G.N.; Cohen, B.E.; Commodore-Mensah, Y.; Fleury, J.; Huffman, J.C.; Khalid, U.; Labarthe, D.R.; Lavretsky, H.; Michos, E.D.; Spatz, E.S.; et al. Psychological Health, Well-Being, and the Mind-Heart-Body Connection: A Scientific Statement from the American Heart Association. Circulation 2021, 143, e763–e783. [Google Scholar] [CrossRef] [PubMed]
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.G. Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum Associates Publishers: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Vaske, J.J.; Beaman, J.; Sponarski, C.C. Rethinking internal consistency in Cronbach’s alpha. Leis. Sci. 2017, 39, 163–173. [Google Scholar] [CrossRef]
- Zigmond, A.S.; Snaith, R.P. The Hospital Anxiety and Depression Scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef] [Green Version]
- Costantini, M.; Musso, M.; Viterbori, P.; Bonci, F.; Del Mastro, L.; Garrone, O.; Venturini, M.; Morassi, G. Detecting psychological distress in cancer patients: Validity of the Italian version of the Hospital Anxiety and Depression Scale. Support. Care Cancer 1999, 7, 121–127. [Google Scholar] [CrossRef]
- Watson, M.; Greer, S.; Young, J.; Inayat, Q.; Burgess, C.; Robertson, B. Development of a questionnaire measure of adjustment to cancer: The MAC scale. Psychol. Med. 1988, 18, 203–209. [Google Scholar] [CrossRef]
- Grassi, L.; Buda, P.; Cavana, L.; Annunziata, M.A.; Torta, R.; Varetto, A. Styles of coping with cancer: The Italian version of the Mini-Mental Adjustment to Cancer (Mini-MAC) scale. Psychooncology 2005, 14, 115–124. [Google Scholar] [CrossRef]
- Bonanno, G.A.; Pat-Horenczyk, R. Coping flexibility and trauma: The Perceived Ability to Cope with Trauma (PACT) Scale. Psychol. Trauma 2011, 3, 117–129. [Google Scholar] [CrossRef] [Green Version]
- Saita, E.; Acquati, C.; Fenaroli, V.; Zuliani, C.; Bonanno, G.A. A Confirmatory factor analysis of the perceived ability to cope with trauma (PACT) scale. Test. Psychomet. Methodol. Appl. Psychol. 2017, 24, 255–258. [Google Scholar]
- Hopwood, P.; Fletcher, I.; Lee, A.; Al Ghazal, S. A body image scale for use with cancer patients. Eur. J. Cancer 2001, 37, 189–197. [Google Scholar] [CrossRef]
- Cheli, S.; Agostini, A.; Herd-Smith, A.; Caligiani, L.; Martella, F.; Fioretto, L. The Italian Version of Body Image Scale. Reliability and Sensitivity in a sample of Breast Cancer Patients. Psicoterapia Cogn. Comportament. 2016, 22, 65–79. [Google Scholar] [CrossRef]
- Saita, E.; Ferraris, G.; Molgora, S.; Fenaroli, V.; Grassi, M. Body image in women with breast cancer. A research within a relational perspective. Ricerche Psicol. 2018, 41, 729–743. [Google Scholar] [CrossRef]
- IBM Corp. IBM SPSS Statistics for Macintosh, Version 27.0; IBM Corp: Armonk, NY, USA, 2020. [Google Scholar]
- Lakens, D. Calculating and reporting effect size to facilitate cumulative science: A practical primer for t-tests and ANOVAs. Front. Psychol. 2013, 4, 863. [Google Scholar] [CrossRef] [Green Version]
- Adams, C.; van Manen, M.A. Teaching phenomenological research and writing. Qual. Health Res. 2017, 27, 780–791. [Google Scholar] [CrossRef]
- Cohen, J. A coefficient of agreement for nominal scales. Educ. Psychol. Meas. 1960, 20, 37–46. [Google Scholar] [CrossRef]
- Breidenbach, C.; Heidkamp, P.; Hiltrop, K.; Pfaff, H.; Enders, A.; Ernstmann, N.; Kowalski, C. Prevalence and determinants of anxiety and depression in long-term breast cancer survivors. BMC Psychiatry 2022, 22, 101. [Google Scholar] [CrossRef]
- Yang, M.; Zhang, Z.; Nice, E.C.; Wang, C.; Zhang, W.; Huang, C. Psychological intervention to treat distress: An emerging frontier in cancer prevention and therapy. Biochim. Biophys. Acta Rev. Cancer 2022, 1877, 188665. [Google Scholar] [CrossRef] [PubMed]
- Dunn, S.L. Hopelessness as a response to physical illness. J. Nurs. Sch. 2005, 37, 148–154. [Google Scholar] [CrossRef] [PubMed]
- Gottlieb, B.H.; Wachala, E.D. Cancer support groups: A critical review of empirical studies. Psychooncology 2007, 16, 379–400. [Google Scholar] [CrossRef] [PubMed]
- Hu, J.; Wang, X.; Guo, S.; Chen, F.; Wu, Y.Y.; Ji, F.J.; Fang, X. Peer support interventions for breast cancer patients: A systematic review. Breast Cancer Res. Treat. 2019, 174, 325–341. [Google Scholar] [CrossRef]
- Saita, E.; Molgora, S.; Acquati, C. Development and evaluation of the Cancer Dyads Group Intervention: Preliminary findings. J. Psychosoc. Oncol. 2014, 32, 647–664. [Google Scholar] [CrossRef]
- Vagnini, D.; Lamperti, N.; Molgora, S.; Barile, F.; Facchin, F.; Mazza, U.; Saita, E. Mental Health Issues as a Consequence of the Pandemic: Group Psycho-Educational Intervention to Support Patients Recovered from COVID-19 Infection. Int. J. Environ. Res. Public Health 2023, 20, 6105. [Google Scholar] [CrossRef]
- McAlpine, H.; Joubert, L.; Martin-Sanchez, F.; Merolli, M.; Drummond, K.J. A systematic review of types and efficacy of online interventions for cancer patients. Patient Educ. Couns. 2015, 98, 283–295. [Google Scholar] [CrossRef]
- Ihrig, A.; Karschuck, P.; Haun, M.W.; Thomas, C.; Huber, J. Online peer-to-peer support for persons affected by prostate cancer: A systematic review. Patient Educ. Couns. 2020, 103, 2107–2115. [Google Scholar] [CrossRef]
- Ziegler, E.; Hill, J.; Lieske, B.; Klein, J.; von dem Knesebeck, O.; Kofahl, C. Empowerment in cancer patients: Does peer support make a difference? A systematic review. Psychooncology 2022, 31, 683–704. [Google Scholar] [CrossRef]
- Durosini, I.; Savioni, L.; Triberti, S.; Guiddi, P.; Pravettoni, G. The Motivation Journey: A Grounded Theory Study on Female Cancer Survivors’ Experience of a Psychological Intervention for Quality of Life. Int. J. Environ. Res. Public Health 2021, 18, 950. [Google Scholar] [CrossRef]
- Pino, O.; Cadena, R.T.; Poli, D. A Comprehensive Review on Multifaceted Mechanisms Involved in the Development of Breast Cancer Following Adverse Childhood Experiences (ACEs). Int. J. Environ. Res. Public Health 2022, 19, 12615. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Module | Aims | Practices and Skills |
|---|---|---|
| [Welcome] (1) Breathing | Developing awareness that changes in breathing are normal when we perceive an external threat. Learning strategies to calm down and send an important message to the nervous system: there is “No Danger”. Learning that the way we breathe is what makes the difference. | Conscious breathing to achieve relaxation responses in the body: inhale and exhale following the practitioner’s guidance. The ultimate goal of any breath work practice is to activate the peripheral nervous system. |
| (2) Grounding | Grounding practices help to connect to the present. They also allow the body to find its inner balance and to be physically and emotionally in contact with what is really happening in the “here and now” in order to: | Finding balance on your own legs, noticing how your feet make contact with the ground. Various practices can be explored, for example: |
|
| |
| (3) Felt-Sense | Felt-sense describes internal bodily awareness of the changes that our internal landscape goes through (i.e., senses, emotions, and feelings). It stimulates a healthy mind–body connection and helps the body to feel safe from within. Awareness is key to: |
|
| ||
| (4) Movement | Learning that the body has a memory and how emotions and sensations find their way to expression. Reconnect the body to movement as the antidote to the freeze response and, therefore, immobility, and provide flexibility back to the body to relieve tension and pain. Provide the body a new experience as it can move and protect itself, and reduce, relieve, or eliminate the debilitating symptoms of trauma stuck in the body (i.e., “frozen”). | Gentle movement practices, and self-touch where the stress is stuck in the body and release the tension and pain: |
| ||
| (5) Healthy Boundaries | Gain self-awareness and establish healthy boundaries, crucial for self-care and positive relationships. Strengthen your boundary awareness by exploring the cues in your body that give you feedback about your needs or limits. Setting clear, but flexible, boundaries involves listening to and respecting your somatic cues. Strong sensations often serve as important signals that can help you to recognize what is right or wrong for you and allow you to gain a personal space where you can be confident and protect yourself (e.g., learn to say “No” when necessary). | Protect your space: Place your right hand on your left shoulder and vice versa, and feel your space. Push hands against the wall: Regain confidence about your safe space and body, and the capacity to keep the required distance in various circumstances. |
| (6) Self-regulation | Learn how the body is able to self-regulate and how the autonomic nervous system receives information about the body and external environment, and how it responds by stimulating body processes. Detect tension and pain as a result of negative emotions or thoughts, and relieve the stress response through self-regulation resources and techniques. | Self-regulation is when you learn and develop your own tools to calm yourself down. Self-regulation tools are taught to help you move through big emotions and feelings, and find stabilization. By recognizing the body’s signals, you can facilitate energy discharge under the practitioner’s guidance. Tune into your body through: |
| ||
| (7) Freeze Response | Understanding that unsolved trauma symptoms develop from the freeze response, when trapped energy does not get discharged, but is stuck in the body: e.g., dissociation or immobility (paralysis, denial), debilitating emotional states (e.g., panic attacks, hypervigilance, and impotence), and chronic fatigue. Understanding medical trauma and the best way to avoid it, especially in conditions of recurrence of the disease and during medical procedures. Learning how to heal medical trauma by adopting the right techniques and resources. | Understand what happens in the body when you experience fear or anxiety (e.g., during medical procedures), and self-regulate or prepare to reduce or avoid trauma symptoms. Understand the dilemma of rationally wanting to obtain treatment and the survival instinct that is trying to escape it. Passive acceptance to avoid medical trauma is key. |
| (8) Recall Session: Questions, Comments, and Conclusion [Greetings] | Discussion of key topics and allowing everybody to comment and share. Discussing changes and quality of life awareness. | Get in touch with your own body and the available resources. Share your personal inventory of resources and recognize who you can ask for help. Breathing practice. |
| Intervention Group (n = 21) | Control Group (n = 14) | Baseline (T0) Differences | |
|---|---|---|---|
| Age—M (SD) range | 54.14 (5.51) 39–62 | 50.00 (8.99) 33–66 | t(33) = 1.695, p = 0.100, Cohen’s d a = 0.585 |
| Marital status—n (%) Single Married Cohabitation | 5 (23.81) 15 (71.43) 1 (4.76) | 1 (7.14) 4 (28.57) 9 (64.29) | χ2(2) = 14.620, p = 0.0001 **, Cramer’s V b = 0.646 |
| Children—n (%) Yes No | 12 (57.14) 9 (42.86) | 9 (64.29) 5 (35.71) | χ2(1) = 0.179, p = 0.673, Cramer’s V b = 0.071 |
| Educational level—n (%) Elementary school Middle school High school University | 0 (0) 5 (23.81) 10 (47.62) 6 (28.57) | 0 (0) 3 (21.43) 7 (50.00) 4 (28.57) | χ2(2) = 0.031, p = 0.985, Cramer’s V b = 0.030 |
| Diagnosis: Year—n (%) 2016–2017 2019–2020 | 10 (47.62) 11 (52.38) | 3 (21.43) 11 (78.57) | χ2(1) = 2.468, p = 0.116, Cramer’s V b = 0.266 |
| Surgery: Type—n (%) Quadrantectomy Mastectomy | 15 (71.43) 6 (28.57) | 11 (78.57) 3 (21.43) | χ2(1) = 0.224, p = 0.636, Cramer’s V b = 0.080 |
| Medical treatments—n (%) Radiotherapy Chemotherapy Hormonal therapy Radio. and hormonal therapy Chemo and hormonal therapy Radio, chemo, and hormonal therapy No treatments | 0 (0) 0 (0) 3 (14.29) 11 (52.38) 2 (9.52) 4 (19.05) 1 (4.76) | 1 (7.14) 1 (7.14) 0 6 (42.86) 3 (21.43) 3 (21.43) 0 | χ2(6) = 6.681, p = 0.351, Cramer’s V b = 0.437 |
| Main caregiver—n (%) Father/mother Other family member A friend Romantic partner/husband | 1 (4.76) 3 (14.29) 3 (14.29) 14 (66.66) | 1 (7.14) 1 (7.14) 1 (7.14) 11 (78.58) | χ2(3) = 1.000, p = 0.801, Cramer’s V b = 0.169 |
| Body image (T0: BIS)—n (%) Good body image (scores 0–10) Composite body image (scores 11–20) Impaired body image (scores 21–30) | 6 (28.57) 11 (52.38) 4 (19.05) | 1 (7.14) 6 (42.86) 7 (50.00) | χ2(2) = 4.646, p = 0.098, Cramer’s V b = 0.364 |
| Symptoms of anxiety (T0: HADS-A)—n (%) Normal level (scores 0–7) Borderline level (scores 8–10) Abnormal level (scores 11–21) | 12 (57.14) 3 (14.29) 6 (28.57) | 3 (21.43) 6 (42.86) 5 (35.71) | χ2(2) = 5.303, p = 0.071, Cramer’s V b = 0.389 |
| Symptoms of depression (T0: HADS-D)—n (%) Normal level (scores 0–7) Borderline level (scores 8–10) Abnormal level (scores 11–21) | 16 (76.19) 5 (23.81) 0 (0) | 8 (57.14) 6 (42.86) 0 (0) | χ2(1) = 1.414, p = 0.234, Cramer’s V b = 0.201 |
| Intervention Group (n = 21) T0: Baseline | Control Group (n = 14) T0: Baseline | Independent t-test | ES a | ||
|---|---|---|---|---|---|
| Measures (Range) | M (SD) | M (SD) | t(df) | p Value | Cohen’s d |
| Anxiety: HADS-A (0–21) | 7.57 (4.06) | 9.14 (2.68) | −1.272(33) | 0.212 | −0.439 |
| Depression: HADS-D (0–21) | 4.76 (3.08) | 6.64 (2.31) | −1.946(33) | 0.060 | −0.671 |
| Distress: HADS (0–42) | 12.33 (5.56) | 15.79 (4.17) | −1.743(33) | 0.091 | −0.602 |
| Fighting spirit: Mini-MAC (1–4) | 3.06 (0.58) | 2.95 (0.72) | 0.515(33) | 0.610 | 0.178 |
| Hopeless/helplessness: Mini-MAC (1–4) | 1.54 (0.52) | 1.91 (0.68) | −1.805(33) | 0.080 | −0.623 |
| Anxious preoccupation: Mini-MAC (1–4) | 2.07 (0.67) | 2.47 (0.52) | −1.893(33) | 0.067 | −0.653 |
| Fatalism: Mini-MAC (1–4) | 3.04 (0.60) | 2.92 (0.67) | 0.539(33) | 0.593 | 0.186 |
| Avoidance: Mini-MAC (1–4) | 2.90 (0.82) | 2.46 (0.80) | 1.571(33) | 0.126 | 0.542 |
| Forward Focus: PACT (1–7) | 5.19 (1.12) | 4.50 (1.29) | 1.702(33) | 0.098 | 0.587 |
| Trauma Focus: PACT (1–7) | 4.91 (1.22) | 4.87 (1.22) | 1.109(33) | 0.914 | 0.038 |
| Flexibility: PACT (0–1) | 0.86 (0.06) | 0.82 (0.08) | 1.701(33) | 0.098 | 0.587 |
| Body image: BIS (0–30) | 14.43 (6.98) | 18.64 (5.08) | −1.940(33) | 0.061 | −0.669 |
| Intervention Group (n = 21) | Control Group (n = 14) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Measures (Range) | T0 | T1 | Paired t-Test | ES a | T0 | T1 | Paired t-Test | ES a | ||
| M (SD) | M (SD) | t(df) | p Value | d | M (SD) | M (SD) | t(df) | p Value | d | |
| Anxiety: HADS-A (0–21) | 7.57 (4.06) | 5.29 (2.94) | 2.788(20) | 0.011 * | 0.608 | 9.14 (2.68) | 10.57 (3.98) | −1.439(13) | 0.174 | −0.385 |
| Depression: HADS-D (0–21) | 4.76 (3.08) | 2.95 (2.87) | 2.682(20) | 0.014 * | 0.585 | 6.64 (2.31) | 7.14 (3.11) | −0.584(13) | 0.569 | −0.156 |
| Distress: HADS (0–42) | 12.33 (5.56) | 8.24 (5.33) | 3.107(20) | 0.006 * | 0.678 | 15.79 (4.17) | 17.71 (5.24) | −1.422(13) | 0.179 | −0.380 |
| Fighting spirit: Mini-MAC (1–4) | 3.06 (0.58) | 3.20 (0.65) | −1.474(20) | 0.156 | −0.322 | 2.95 (0.72) | 3.04 (1.00) | −0.330(13) | 0.747 | −0.088 |
| Hopeless/ helplessness: Mini-MAC (1–4) | 1.54 (0.52) | 1.45 (0.50) | 1.789(20) | 0.089 | 0.390 | 1.91 (0.68) | 2.96 (0.74) | −5.192(13) | 0.0001 ** | −1.388 |
| Anxious preoccupation: Mini-MAC (1–4) | 2.07 (0.67) | 1.73 (0.71) | 4.198(20) | 0.0001 ** | 0.916 | 2.47 (0.52) | 2.64 (0.49) | −1.686(13) | 0.116 | −0.450 |
| Fatalism: Mini-MAC (1–4) | 3.04 (0.60) | 3.09 (0.50) | −0.384(20) | 0.705 | −0.084 | 2.92 (0.67) | 3.03 (0.79) | −0.591(13) | 0.565 | −0.158 |
| Avoidance: Mini-MAC (1–4) | 2.90 (0.82) | 2.83 (0.86) | 0.487(20) | 0.631 | 0.106 | 2.46 (0.80) | 3.32 (0.60) | −3.397(13) | 0.005 * | −0.908 |
| Forward focus: PACT (1–7) | 5.19 (1.12) | 5.58 (0.98) | −2.920(20) | 0.008 * | −0.637 | 4.50 (1.29) | 4.33 (1.34) | 0.602(13) | 0.557 | 0.161 |
| Trauma focus: PACT (1–7) | 4.91 (1.22) | 5.17 (0.95) | −1.425(20) | 0.170 | −0.311 | 4.87 (1.22) | 4.36 (1.09) | 1.257(13) | 0.231 | 0.336 |
| Flexibility: PACT (0–1) | 0.86 (0.06) | 0.87 (0.06) | −0.818(20) | 0.423 | −0.179 | 0.82 (0.08) | 0.80 (0.08) | 0.949(13) | 0.360 | 0.254 |
| Body image: BIS (0–30) | 14.43 (6.98) | 7.95 (3.54) | 6.234(20) | 0.0001 ** | 1.360 | 18.64 (5.08) | 22.43 (6.11) | −1.717 | 0.110 | −0.459 |
| Themes | Responses | Meaningful Quotes |
|---|---|---|
| Significant moments | Responses = 63 | |
| “Feeling the connection with the body and deep emotional experiences” | 51% (n = 32) | “The first time I entered into a connection with my body and my inner experiences it was as if I knew myself for the first time, or rather, as if I were looking at myself for the first time”. (ID code: UU121) “The moment I liked it most was when we experienced grounding. I realized that along with breathing, it is the technique that helps me the most to take care of myself and my needs in everyday life”. (ID code: AD21I) |
| “Realizing that it worked” | 27% (n = 17) | “I have always looked forward to each session with joy, I was impatient. It was a meaningful experience. I saw the change in the facial expression of the other women, and so I realized they felt better, we all felt better”. (ID code: ER13E) |
| “Reflections in group” | 22% (n = 14) | “I remember with gratitude the first personal reflection in group, it was difficult, but it was also liberating. I felt welcomed, strong, and safe”. (ID code: RC23A) |
| Important learnings | Responses = 63 | |
| “Take care of yourself” | 57% (n = 36) | “I realized that my body is a precious ally, I realized that my body does not suck and I should not be afraid. My body is wise and I learned to listen to it to give it, and then give it to myself, what is needed to feel good”. (ID code: SI22I) |
| “Live in the ‘here and now” | 43% (n = 27) | “What I learned is ‘take away without necessarily adding’, that is, I learned to live without being always in a hurry and I learned to notice the life around me. […] Now I know the importance of empowering myself to take time to better cope with life’s difficulties”. (ID code: VR33A). |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vagnini, D.; Grassi, M.M.; Saita, E. Evaluating Somatic Experiencing® to Heal Cancer Trauma: First Evidence with Breast Cancer Survivors. Int. J. Environ. Res. Public Health 2023, 20, 6412. https://doi.org/10.3390/ijerph20146412
Vagnini D, Grassi MM, Saita E. Evaluating Somatic Experiencing® to Heal Cancer Trauma: First Evidence with Breast Cancer Survivors. International Journal of Environmental Research and Public Health. 2023; 20(14):6412. https://doi.org/10.3390/ijerph20146412
Chicago/Turabian StyleVagnini, Denise, Massimo Maria Grassi, and Emanuela Saita. 2023. "Evaluating Somatic Experiencing® to Heal Cancer Trauma: First Evidence with Breast Cancer Survivors" International Journal of Environmental Research and Public Health 20, no. 14: 6412. https://doi.org/10.3390/ijerph20146412
APA StyleVagnini, D., Grassi, M. M., & Saita, E. (2023). Evaluating Somatic Experiencing® to Heal Cancer Trauma: First Evidence with Breast Cancer Survivors. International Journal of Environmental Research and Public Health, 20(14), 6412. https://doi.org/10.3390/ijerph20146412