
Outcomes of Transcatheter Aortic Valve Implantation Comparing Medtronic’s Evolut PRO and Evolut R: A Systematic Review and Meta-Analysis of Observational Studies

 , , , , , , ,
, , , , , , ,  , ,
, ,  on behalf of the Thoracic Research Centreadd
Show full author list
on behalf of the Thoracic Research Centreadd
Show full author list
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources and Search Strategy
2.2. Selection Criteria and Quality Assessment
2.3. Endpoints Selection
2.4. Statistical Analysis
3. Results
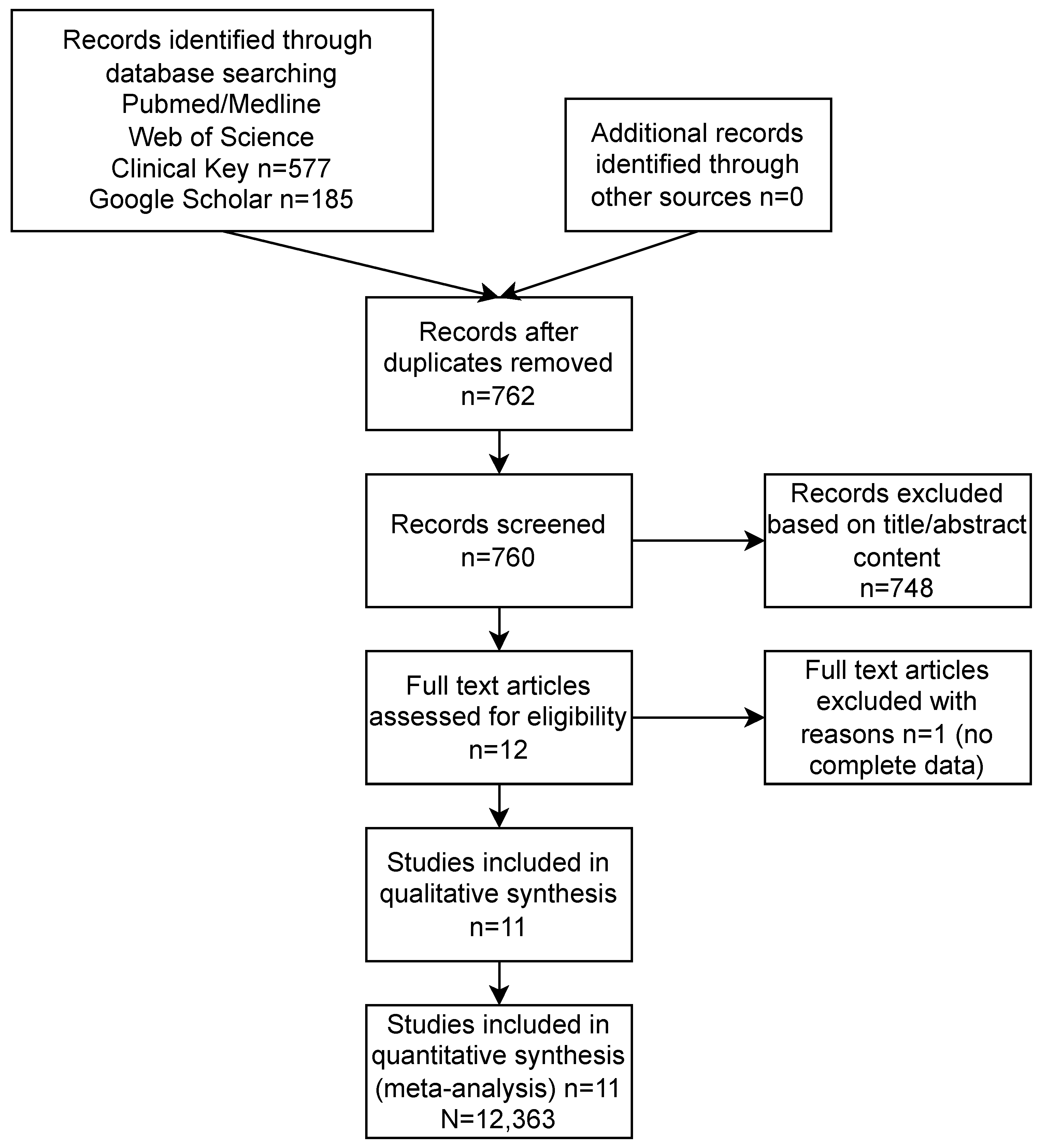
3.1. Study Selection
3.2. Patients’ Characteristics
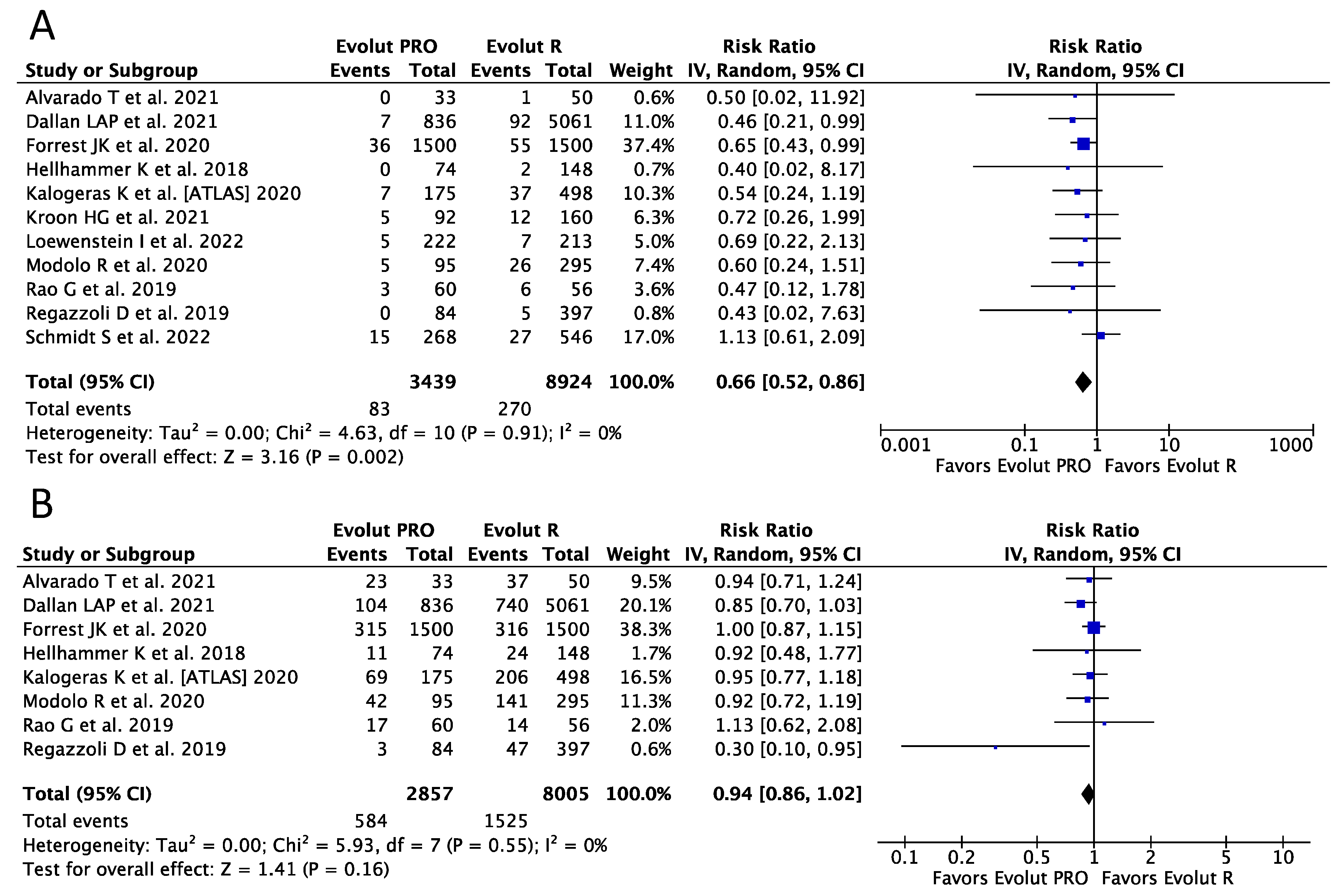
3.3. Procedural Outcomes
3.4. Functional Outcomes
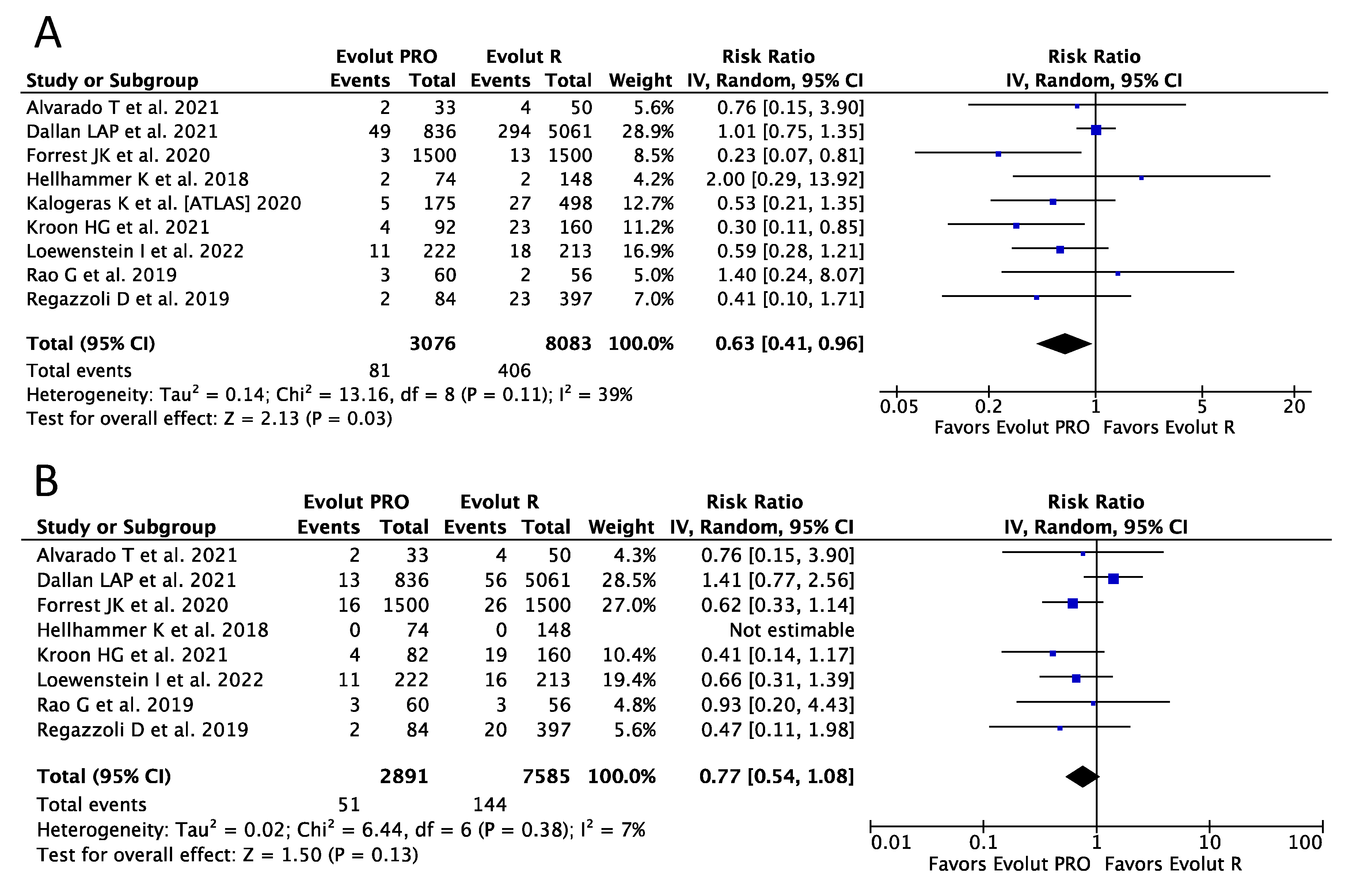
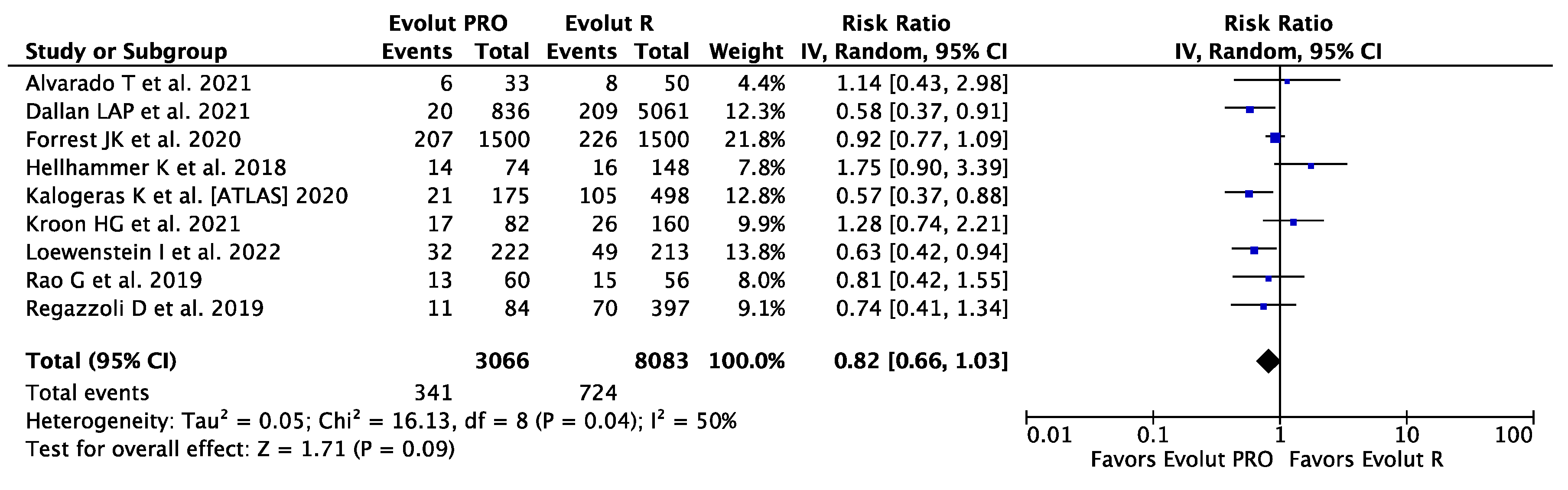
3.5. Clinical Outcomes
3.6. Sensitivity Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Leon, M.B.; Smith, C.R.; Mack, M.; Miller, D.C.; Moses, J.W.; Svensson, L.G.; Tuzcu, E.M.; Webb, J.G.; Fontana, G.P.; Makkar, R.R.; et al. Transcatheter aortic-valve implantation for aortic stenosis in patients who cannot undergo surgery. N. Engl. J. Med. 2010, 363, 1597–1607. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, C.R.; Leon, M.B.; Mack, M.J.; Miller, D.C.; Moses, J.W.; Svensson, L.G.; Tuzcu, E.M.; Webb, J.G.; Fontana, G.P.; Makkar, R.R.; et al. Transcatheter versus surgical aortic-valve replacement in high-risk patients. N. Engl. J. Med. 2011, 364, 2187–2198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mack, M.J.; Leon, M.B.; Smith, C.R.; Miller, D.C.; Moses, J.W.; Tuzcu, E.M.; Webb, J.G.; Douglas, P.S.; Anderson, W.N.; Blackstone, E.H.; et al. 5-year outcomes of transcatheter aortic valve replacement or surgical aortic valve replacement for high surgical risk patients with aortic stenosis (PARTNER 1): A randomised controlled trial. Lancet 2015, 385, 2477–2484. [Google Scholar] [CrossRef] [PubMed]
- Deeb, G.M.; Reardon, M.J.; Chetcuti, S.; Patel, H.J.; Grossman, P.M.; Yakubov, S.J.; Kleiman, N.S.; Coselli, J.S.; Gleason, T.G.; Lee, J.S.; et al. 3-Year Outcomes in High-Risk Patients Who Underwent Surgical or Transcatheter Aortic Valve Replacement. J. Am. Coll. Cardiol. 2016, 67, 2565–2574. [Google Scholar] [CrossRef]
- Thourani, V.H.; Kodali, S.; Makkar, R.R.; Herrmann, H.C.; Williams, M.; Babaliaros, V.; Smalling, R.; Lim, S.; Malaisrie, S.C.; Kapadia, S.; et al. Transcatheter aortic valve replacement versus surgical valve replacement in intermediate-risk patients: A propensity score analysis. Lancet 2016, 387, 2218–2225. [Google Scholar] [CrossRef] [PubMed]
- Leon, M.B.; Smith, C.R.; Mack, M.J.; Makkar, R.R.; Svensson, L.G.; Kodali, S.K.; Thourani, V.H.; Tuzcu, E.M.; Miller, D.C.; Herrmann, H.C.; et al. Transcatheter or Surgical Aortic-Valve Replacement in Intermediate-Risk Patients. N. Engl. J. Med. 2016, 374, 1609–1620. [Google Scholar] [CrossRef]
- Reardon, M.J.; Van Mieghem, N.M.; Popma, J.J.; Kleiman, N.S.; Søndergaard, L.; Mumtaz, M.; Adams, D.H.; Deeb, G.M.; Maini, B.; Gada, H.; et al. Surgical or Transcatheter Aortic-Valve Replacement in Intermediate-Risk Patients. N. Engl. J. Med. 2017, 376, 1321–1331. [Google Scholar] [CrossRef]
- Mack, M.J.; Leon, M.B.; Thourani, V.H.; Makkar, R.; Kodali, S.K.; Russo, M.; Kapadia, S.R.; Malaisrie, S.C.; Cohen, D.J.; Pibarot, P.; et al. Transcatheter Aortic-Valve Replacement with a Balloon-Expandable Valve in Low-Risk Patients. N. Engl. J. Med. 2019, 380, 1695–1705. [Google Scholar] [CrossRef]
- Leon, M.B.; Mack, M.J.; Hahn, R.T.; Thourani, V.H.; Makkar, R.; Kodali, S.K.; Alu, M.C.; Madhavan, M.V.; Chau, K.H.; Russo, M.; et al. Outcomes 2 Years After Transcatheter Aortic Valve Replacement in Patients at Low Surgical Risk. J. Am. Coll. Cardiol. 2021, 77, 1149–1161. [Google Scholar] [CrossRef]
- Popma, J.J.; Deeb, G.M.; Yakubov, S.J.; Mumtaz, M.; Gada, H.; O’Hair, D.; Bajwa, T.; Heiser, J.C.; Merhi, W.; Kleiman, N.S.; et al. Transcatheter Aortic-Valve Replacement with a Self-Expanding Valve in Low-Risk Patients. N. Engl. J. Med. 2019, 380, 1706–1715. [Google Scholar] [CrossRef]
- Kodali, S.K.; Williams, M.R.; Smith, C.R.; Svensson, L.G.; Webb, J.G.; Makkar, R.R.; Fontana, G.P.; Dewey, T.M.; Thourani, V.H.; Pichard, A.D.; et al. Two-year outcomes after transcatheter or surgical aortic-valve replacement. N. Engl. J. Med. 2012, 366, 1686–1695. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jones, B.M.; Tuzcu, E.M.; Krishnaswamy, A.; Popovic, Z.; Mick, S.; Roselli, E.E.; Gul, S.; Devgun, J.; Mistry, S.; Jaber, W.A.; et al. Prognostic significance of mild aortic regurgitation in predicting mortality after transcatheter aortic valve replacement. J. Thorac. Cardiovasc. Surg. 2016, 152, 783–790. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stroup, D.F.; Berlin, J.A.; Morton, S.C.; Olkin, I.; Williamson, G.D.; Rennie, D.; Moher, D.; Becker, B.J.; Sipe, T.A.; Thacker, S.B. Meta-analysis of observational studies in epidemiology: A proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group. JAMA 2000, 283, 2008–2012. [Google Scholar] [CrossRef] [PubMed]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef]
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [Green Version]
- Kappetein, A.P.; Head, S.J.; Généreux, P.; Piazza, N.; van Mieghem, N.M.; Blackstone, E.H.; Brott, T.G.; Cohen, D.J.; Cutlip, D.E.; van Es, G.A.; et al. Updated standardized endpoint definitions for transcatheter aortic valve implantation: The Valve Academic Research Consortium-2 consensus document. J. Am. Coll. Cardiol. 2012, 60, 1438–1454. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [Green Version]
- Wan, X.; Wang, W.; Liu, J.; Tong, T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med. Res. Methodol. 2014, 14, 135. [Google Scholar] [CrossRef] [Green Version]
- Alvarado, T.; Rivero, F.; Diego, G.; García-Guimaraes, M.; Salamanca, J.; Díez-Villanueva, P.; Cuesta, J.; Antuña, P.; Jiménez-Borreguero, J.; Alfonso, F. Transcatheter aortic valve replacement using the new Evolut-Pro system: A prospective comparison with the Evolut-R device. J. Thorac. Dis. 2021, 13, 4023–4032. [Google Scholar] [CrossRef]
- Dallan, L.A.P.; Forrest, J.K.; Reardon, M.J.; Szeto, W.Y.; George, I.; Kodali, S.; Kleiman, N.S.; Yakubov, S.J.; Grubb, K.J.; Liu, F.; et al. Transcatheter Aortic Valve Replacement With Self-Expandable Supra-Annular Valves for Degenerated Surgical Bioprostheses: Insights From Transcatheter Valve Therapy Registry. J. Am. Heart Assoc. 2021, 10, e021871. [Google Scholar] [CrossRef]
- Forrest, J.K.; Kaple, R.K.; Tang, G.H.L.; Yakubov, S.J.; Nazif, T.M.; Williams, M.R.; Zhang, A.; Popma, J.J.; Reardon, M.J. Three Generations of Self-Expanding Transcatheter Aortic Valves: A Report From the STS/ACC TVT Registry. JACC Cardiovasc. Interv. 2020, 13, 170–179. [Google Scholar] [CrossRef] [PubMed]
- Hellhammer, K.; Piayda, K.; Afzal, S.; Kleinebrecht, L.; Makosch, M.; Hennig, I.; Quast, C.; Jung, C.; Polzin, A.; Westenfeld, R.; et al. The Latest Evolution of the Medtronic CoreValve System in the Era of Transcatheter Aortic Valve Replacement: Matched Comparison of the Evolut PRO and Evolut R. JACC Cardiovasc. Interv. 2018, 11, 2314–2322. [Google Scholar] [CrossRef] [PubMed]
- Kalogeras, K.; Ruparelia, N.; Kabir, T.; Jabbour, R.; Naganuma, T.; Vavuranakis, M.; Nakamura, S.; Wang, B.; Sen, S.; Hadjiloizou, N.; et al. Comparison of the self-expanding Evolut-PRO transcatheter aortic valve to its predecessor Evolut-R in the real world multicenter ATLAS registry. Int. J. Cardiol. 2020, 310, 120–125. [Google Scholar] [CrossRef] [PubMed]
- Kroon, H.G.; van Gils, L.; Ziviello, F.; van Wiechen, M.P.H.; Ooms, J.F.W.; Rahhab, Z.; El Faquir, N.; Maugenest, A.; Goudzwaard, J.A.; Cummins, P.; et al. Clinical consequences of consecutive self-expanding transcatheter heart valve iterations. Neth. Heart J. 2022, 30, 140–148. [Google Scholar] [CrossRef]
- Loewenstein, I.; Merdler, I.; Hochstadt, A.; Zahler, D.; Finkelstein, A.; Banai, S.; Topilsky, Y.; Halkin, A.; Konigstein, M.; Bazan, S.; et al. Generational Differences in Outcomes of Self-Expanding Valves for Transcatheter Aortic Valve Replacement. J. Invasive Cardiol. 2022, 34, E326–E333. [Google Scholar]
- Modolo, R.; Chang, C.C.; Abdelghani, M.; Kawashima, H.; Ono, M.; Tateishi, H.; Miyazaki, Y.; Pighi, M.; Wykrzykowska, J.J.; de Winter, R.J.; et al. Quantitative Assessment of Acute Regurgitation Following TAVR: A Multicenter Pooled Analysis of 2,258 Valves. JACC Cardiovasc. Interv. 2020, 13, 1303–1311. [Google Scholar] [CrossRef]
- Rao, G.; Sheth, S.; Donnelly, J.; Scatola, A.; Tariq, U.; Laighold, S.; Grines, C.; Rutkin, B. Early Real-World Experience with CoreValve Evolut PRO and R Systems for Transcatheter Aortic Valve Replacement. J. Interv. Cardiol. 2019, 2019, 1906814. [Google Scholar] [CrossRef] [Green Version]
- Regazzoli, D.; Chiarito, M.; Cannata, F.; Pagnesi, M.; Miura, M.; Ziviello, F.; Picci, A.; Reifart, J.; De Marco, F.; Bedogni, F.; et al. Transcatheter Self-Expandable Valve Implantation for Aortic Stenosis in Small Aortic Annuli: The TAVI-SMALL Registry. JACC Cardiovasc. Interv. 2020, 13, 196–206. [Google Scholar] [CrossRef]
- Schmidt, S.; Fortmeier, V.; Ludwig, S.; Wienemann, H.; Körber, M.I.; Lee, S.; Meertens, M.; Macherey, S.; Iliadis, C.; Kuhn, E.; et al. Hemodynamics of self-expanding versus balloon-expandable transcatheter heart valves in relation to native aortic annulus anatomy. Clin. Res. Cardiol. 2022, 111, 1336–1347. [Google Scholar] [CrossRef]
- Gotzmann, M.; Korten, M.; Bojara, W.; Lindstaedt, M.; Rahlmann, P.; Mügge, A.; Ewers, A. Long-term outcome of patients with moderate and severe prosthetic aortic valve regurgitation after transcatheter aortic valve implantation. Am. J. Cardiol. 2012, 110, 1500–1506. [Google Scholar] [CrossRef]
- Little, S.H.; Oh, J.K.; Gillam, L.; Sengupta, P.P.; Orsinelli, D.A.; Cavalcante, J.L.; Chang, J.D.; Adams, D.H.; Zorn, G.L., 3rd; Pollak, A.W.; et al. Self-Expanding Transcatheter Aortic Valve Replacement Versus Surgical Valve Replacement in Patients at High Risk for Surgery: A Study of Echocardiographic Change and Risk Prediction. Circ. Cardiovasc. Interv. 2016, 9, e003426. [Google Scholar] [CrossRef]
- Ando, T.; Briasoulis, A.; Telila, T.; Afonso, L.; Grines, C.L.; Takagi, H. Does mild paravalvular regurgitation post transcatheter aortic valve implantation affect survival? A meta-analysis. Catheter. Cardiovasc. Interv. 2018, 91, 135–147. [Google Scholar] [CrossRef]
- Barbanti, M.; Binder, R.K.; Freeman, M.; Wood, D.A.; Leipsic, J.; Cheung, A.; Ye, J.; Tan, J.; Toggweiler, S.; Yang, T.H.; et al. Impact of low-profile sheaths on vascular complications during transfemoral transcatheter aortic valve replacement. EuroIntervention 2013, 9, 929–935. [Google Scholar] [CrossRef]
- Mach, M.; Okutucu, S.; Kerbel, T.; Arjomand, A.; Fatihoglu, S.G.; Werner, P.; Simon, P.; Andreas, M. Vascular Complications in TAVR: Incidence, Clinical Impact, and Management. J. Clin. Med. 2021, 10, 5046. [Google Scholar] [CrossRef]
- Forrest, J.K.; Mangi, A.A.; Popma, J.J.; Khabbaz, K.; Reardon, M.J.; Kleiman, N.S.; Yakubov, S.J.; Watson, D.; Kodali, S.; George, I.; et al. Early Outcomes With the Evolut PRO Repositionable Self-Expanding Transcatheter Aortic Valve With Pericardial Wrap. JACC Cardiovasc. Interv. 2018, 11, 160–168. [Google Scholar] [CrossRef]
- Choudhury, T.; Solomonica, A.; Bagur, R. The Evolut R and Evolut PRO transcatheter aortic valve systems. Expert Rev. Med. Devices 2019, 16, 3–9. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Evolut PRO | Evolut R |
|---|---|
 | |
| Supra-annular design Self-expanding nitinol frame Strong and pliable porcine tissue Ability to recapture and resheath the prosthesis 16-F introducer sheath Valve diameter: 23 mm, 26 mm, 29 mm Unique valve design with an outer wrap | Supra-annular design Self-expanding nitinol frame Strong and pliable porcine tissue Ability to recapture and resheath the prosthesis 14-F introducer sheath Valve diameter: 23 mm, 26 mm, 29 mm, 34 mm - |
| Study | Design | Intervention | Cohort | Follow-Up (Months) | VARC-2 Definitions | ROBINS-I |
|---|---|---|---|---|---|---|
| Alvarado T et al., 2021 [19] | SC RCS | Evolut PRO | 33 | 12.0 ± 0.2 | yes | moderate |
| Evolut R | 50 | 11.0 ± 0.5 | ||||
| Dallan LAP et al., 2021 [20] | MC PCS | Evolut PRO | 836 | 12 | yes | moderate |
| Evolut R | 5061 | |||||
| Forrest JK et al., 2020 [21] | MC RCS, PM | Evolut PRO | 1500 | NR | yes | moderate |
| Evolut R | 1500 | |||||
| Hellhammer K et al., 2018 [22] | SC RCS, PM | Evolut PRO | 74 | 1 | yes | moderate |
| Evolut R | 148 | |||||
| Kalogeras K et al. (ATLAS) 2020 [23] | MC RCS | Evolut PRO | 175 | 12 | yes | moderate |
| Evolut R | 498 | |||||
| Kroon HG et al., 2021 [24] | SC PCS | Evolut PRO | 92 | 1 | yes | moderate |
| Evolut R | 160 | |||||
| Loewenstein I et al., 2022 [25] | MC RCS, PM | Evolut PRO | 222 | 1 | yes | moderate |
| Evolut R | 213 | |||||
| Modolo R et al., 2020 [26] | MC RCS | Evolut PRO | 95 | NR | NR | moderate |
| Evolut R | 295 | |||||
| Rao G et al., 2019 [27] | SC RCS | Evolut PRO | 60 | 1 | yes | moderate |
| Evolut R | 56 | |||||
| Regazzoli D et al., 2019 [28] | MC RCS | Evolut PRO | 84 | 12 | yes | moderate |
| Evolut R | 397 | |||||
| Schmidt S et al., 2022 [29] | MC RCS | Evolut PRO | 268 | NR | yes | moderate |
| Evolut R | 546 |
| Study | Intervention | Age | Females (%) | BMI (kg/m2) | NYHA III/IV(%) | STS–PROM (%) | EuroSCORE II (%) | Mean Gradient [mmHg] | Annulus diameter (mm) | Transfemoral Access (%) |
|---|---|---|---|---|---|---|---|---|---|---|
| Alvarado T et al., 2021 [19] | Evolut PRO | 85.0 ± 4.0 | 79 | NR | 48 | NR | NR | 42.0 ± 13.0 | 23.0 ± 1.8 | 100 |
| Evolut R | 85 ± 0.5.0 | 52 | 68 | 45 ± 0.18.0 | 24.0 ± 4.3 | 100 | ||||
| Dallan LAP et al., 2021 [20] | Evolut PRO | 74.6 ± 10.3 | 41.6 | NR | 79.7 | 7.2 ± 7.1 | NR | NR | NR | 95.4 |
| Evolut R | 75.2 ± 10.5 | 41.2 | 80.4 | 7.7 ± 6.5 | 95.0 | |||||
| Forrest JK et al., 2020 [21] | Evolut PRO | 81.6 ± 7.7 | 65.9 | NR | 75.5 | 7.2 ± 4.8 | NR | 42.4 ± 14.4 | NR | 94.1 |
| Evolut R | 81.3 ± 7.5 | 65.2 | 78.1 | 7.2 ± 4.5 | 43.3 ± 15.2 | 93.5 | ||||
| Hellhammer K et al., 2018 [22] | Evolut PRO | 81.4 ± 4.5 | 67.5 | 26.2 ± 4.4 | NR | NR | 24.9 ± 12.5 * | NR | 23.8 ± 1.8 | 100 |
| Evolut R | 81.2 ± 5.6 | 74.3 | 26.9 ± 5.8 | 24.7 ± 13.7 * | 23.0 ± 1.9 | 100 | ||||
| Kalogeras K et al. (ATLAS) 2020 [23] | Evolut PRO | 82.3 ± 6.3 | 59.4 | 26.8 ± 8.4 | NR | NR | 9.4 ± 7.2 * | 40.3 ±19.9 | NR | 100 |
| Evolut R | 81.7 ± 7.2 | 58.8 | 26.8 ± 5.7 | 14.4 ±9.2 * | 46.5 ±18.8 | NR | 94 | |||
| Kroon HG et al., 2021 [24] | Evolut PRO | 89.7 ± 2.2 | 54 | 27.0 ± 5.0 | 68 | 4.4 ± 3.1 | NR | NR | 23.7 ± 1.8 | 97 |
| Evolut R | 78.7 ± 2.1 | 46 | 27.0 ± 5.0 | 58 | 4.4 ± 2.8 | 23.7 ± 1.9 | 89 | |||
| Loewenstein I et al., 2022 [25] | Evolut PRO | 81.1 ± 6.7 | 62.2 | 28.2 ± 5.2 | NR | 3.9 ± 2.4 | 4.0 ± 3.8 | 48.3 ± 14.8 | ||
| Evolut R | 82.2 ± 7.6 | 63.4 | 27.6 ± 5.1 | 5.0 ± 4.0 | 5.6 ± 6.1 | 47.4 ± 17.6 | ||||
| Modolo R et al., 2020 [26] | Evolut PRO | NR | NR | NR | NR | NR | NR | NR | NR | NR |
| Evolut R | ||||||||||
| Rao G et al., 2019 [27] | Evolut PRO | 84.6 ± 6.3 | 82 | 27.5 ± 6.8 | NR | 7.1 ± 4.0 | NR | NR | NR | 95.1 |
| Evolut R | 80.4 ± 9.4 | 53.6 | 28.8 ± 7.2 | 6.5 ± 4.8 | 94.6 | |||||
| Regazzoli D et al., 2019 [28] | Evolut PRO | 83.5 ± 0.7 | 89.3 | 26.5 ± 0.9 | 81 | 5.5 ± 0.4 | NR | 51.6 ± 1.9 | 21.4 ± 0.1 | 91.7 |
| Evolut R | 82.0 ± 0.4 | 89.2 | 26.8 ± 0.4 | 74.1 | 5.9 ± 0.3 | 50.6 ± 0.8 | 21.2 ± 0.1 | 92.4 | ||
| Schmidt S et al., 2022 [29] | Evolut PRO | 82.0 ± 5.6 | 61.2 | 26.5 ± 5.0 | NR | NR | 4.7 ± 4.3 | 48.1 ± 19.5 | 23.4 ± 1.7 | NR |
| Evolut R | 82.1 ± 6.1 | 61.2 | 26.8 ± 5.2 | 5.7 ± 6.8 | 34.9 ± 20.7 | 23.8 ± 2.5 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gozdek, M.; Kuźma, Ł.; Dąbrowski, E.J.; Janiak, M.; Pietrzak, M.; Skonieczna, K.; Woźnica, M.; Wydeheft, L.; Makhoul, M.; Matteucci, M.; et al. Outcomes of Transcatheter Aortic Valve Implantation Comparing Medtronic’s Evolut PRO and Evolut R: A Systematic Review and Meta-Analysis of Observational Studies. Int. J. Environ. Res. Public Health 2023, 20, 3439. https://doi.org/10.3390/ijerph20043439
Gozdek M, Kuźma Ł, Dąbrowski EJ, Janiak M, Pietrzak M, Skonieczna K, Woźnica M, Wydeheft L, Makhoul M, Matteucci M, et al. Outcomes of Transcatheter Aortic Valve Implantation Comparing Medtronic’s Evolut PRO and Evolut R: A Systematic Review and Meta-Analysis of Observational Studies. International Journal of Environmental Research and Public Health. 2023; 20(4):3439. https://doi.org/10.3390/ijerph20043439
Chicago/Turabian StyleGozdek, Mirosław, Łukasz Kuźma, Emil Julian Dąbrowski, Michał Janiak, Martyna Pietrzak, Karolina Skonieczna, Mikołaj Woźnica, Lidia Wydeheft, Maged Makhoul, Matteo Matteucci, and et al. 2023. "Outcomes of Transcatheter Aortic Valve Implantation Comparing Medtronic’s Evolut PRO and Evolut R: A Systematic Review and Meta-Analysis of Observational Studies" International Journal of Environmental Research and Public Health 20, no. 4: 3439. https://doi.org/10.3390/ijerph20043439
APA StyleGozdek, M., Kuźma, Ł., Dąbrowski, E. J., Janiak, M., Pietrzak, M., Skonieczna, K., Woźnica, M., Wydeheft, L., Makhoul, M., Matteucci, M., Litwinowicz, R., Kowalówka, A., Wańha, W., Pasierski, M., Ronco, D., Massimi, G., Jiritano, F., Fina, D., Martucci, G., ... Kowalewski, M., on behalf of the Thoracic Research Centre. (2023). Outcomes of Transcatheter Aortic Valve Implantation Comparing Medtronic’s Evolut PRO and Evolut R: A Systematic Review and Meta-Analysis of Observational Studies. International Journal of Environmental Research and Public Health, 20(4), 3439. https://doi.org/10.3390/ijerph20043439