
White Spots: Prevention in Orthodontics—Systematic Review of the Literature

 ,
,  ,
,  ,
,  , ,
, ,  ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Protocol and Registration
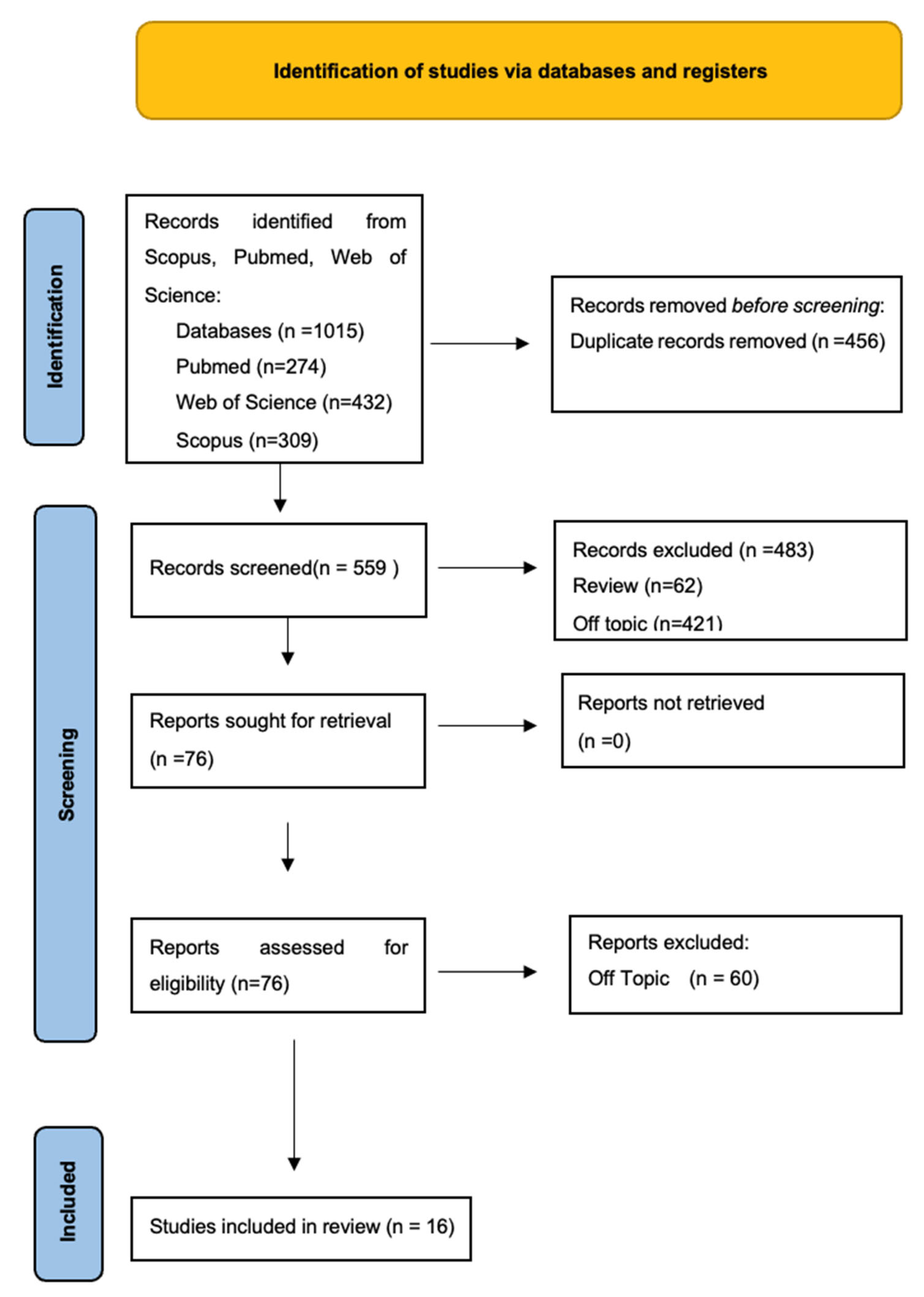
2.2. Search Processing
2.3. Eligibility Criteria
2.4. Data Processing
3. Results
4. Discussion
4.1. Fixed Orthodontics and Salivary Changes
4.2. Streptococcus mutants and Lactobacillus
4.3. Fixed Orthodontics and Caries
4.4. Enamel Etching and WS
4.5. Prevention of WS in Orthodontics
4.6. Prevention with Fluoride
4.7. Active Oxygen-Containing Toothpaste
4.8. Prevention with CO2 Laser
4.9. Primer with Antibacterial
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| FOT | Fixed orthodontic therapy |
| PT | Patient |
| RCT | Randomized Controlled Trial |
| WS | White spots |
| WSL | White spot lesion |
| ICDAS | International Caries Detection and Assessment System |
| GI | Gingival index |
| DMFT | Decay-missing-filled index |
| PE | Partial etching |
| TE | Total etching |
Appendix A

{kind=link}
{kind=link}
| Articles Excluded | Reason for Exclusion |
|---|---|
| Balbinot GS, Marcon N, Sauro S, Luxan SA, Collares FM. Alkyl trimethyl ammonium bromide for the formulation of antibacterial orthodontic resins. Clin Oral Investig. 2022 Dec;26(12):7011-7019. doi: 10.1007/s00784-022-04661-0. Epub 2022 Aug 11. PMID: 35951093. | IN VITRO |
| Choi JH, Jung EH, Lee ES, Jung HI, Kim BI. Anti-biofilm activity of chlorhexidine-releasing elastomerics against dental microcosm biofilms. J Dent. 2022 Jul;122:104153. doi: 10.1016/j.jdent.2022.104153. Epub 2022 May 5. PMID: 35526753. | IN VITRO |
| Welk A, Ratzmann A, Reich M, Krey KF, Schwahn C. Effect of self-assembling peptide P11-4 on orthodontic treatment-induced carious lesions. Sci Rep. 2020 Apr 22;10(1):6819. doi: 10.1038/s41598-020-63633-0. PMID: 32321955; PMCID: PMC7176635. | OFF TOPIC |
| Tan A, Çokakoğlu S. Effects of adhesive flash-free brackets on enamel demineralization and periodontal status. Angle Orthod. 2020 May 1;90(3):339-346. doi: 10.2319/80819-518.1. PMID: 33378441; PMCID: PMC8032304. | IN VITRO |
| Xu Y, Sun Y, Liu W, Shi Z, Jin X, Xu J, Pan X, Zhang Z, Fu B, Zhang L. Effects of an orthodontic primer containing amorphous fluorinated calcium phosphate nanoparticles on enamel white spot lesions. J Mech Behav Biomed Mater. 2023 Jan;137:105567. doi: 10.1016/j.jmbbm.2022.105567. Epub 2022 Nov 10. PMID: 36379092. | IN VITRO |
| Rajendran R, Sudhakar V, Rangarajan RS, Chinnasamy A, Vasupradha G, Jeeva JS. Evaluation of Change in Surface Enamel Microhardness in Patients Undergoing Fixed Orthodontic Appliance Therapy—A Randomized Control Trial. J Pharm Bioallied Sci. 2021 Nov;13(Suppl 2):S1106-S1110. doi: 10.4103/jpbs.jpbs_259_21. Epub 2021 Nov 10. PMID: 35017939; PMCID: PMC8687020. | IN VITRO |
| Liu L, Zou M. [Electronic probe analysis of enamel remineralization effect of casein phosphopeptide-amorphous calcium phosphate promoted by different concentrations of fluorine]. Zhonghua Kou Qiang Yi Xue Za Zhi. 2018 Jul 9;53(7):470-474. Chinese. doi: 10.3760/cma.j.issn.1002-0098.2018.07.008. PMID: 29996365. | OFF TOPIC |
| Wang YH, Liu F, Liu HN, Wang QX, Xing WZ, Li ZC. [Impact assessment on enamel remineralization after orthodontic treatment with casein phosphopeptide calcium phosphate complex]. Shanghai Kou Qiang Yi Xue. 2018 Aug;27(4):382-385. Chinese. PMID: 30483705. | OFF TOPIC |
| Atilla AO, Ozturk T, Eruz MM, Yagci A. A comparative assessment of orthodontic treatment outcomes using the quantitative light-induced fluorescence (QLF) method between direct bonding and indirect bonding techniques in adolescents: a single-centre, single-blind randomized controlled trial. Eur J Orthod. 2020 Sep 11;42(4):441-453. doi: 10.1093/ejo/cjz058. PMID: 31375814. | OFF TOPIC |
| Coordes SL, Jost-Brinkmann PG, Präger TM, Bartzela T, Visel D, Jäcker T, Müller-Hartwich R. A comparison of different sealants preventing demineralization around brackets. J Orofac Orthop. 2018 Jan;79(1):49-56. English. doi: 10.1007/s00056-017-0116-y. Epub 2018 Jan 12. PMID: 29330611. | OFF TOPIC |
| Shan D, He Y, Gao M, Liu H, Zhu Y, Liao L, Hadaegh F, Long H, Lai W. A comparison of resin infiltration and microabrasion for postorthodontic white spot lesion. Am J Orthod Dentofacial Orthop. 2021 Oct;160(4):516-522. doi: 10.1016/j.ajodo.2020.04.039. Epub 2021 Jul 31. PMID: 34344556. | OFF TOPIC |
| Yi J, Dai Q, Weir MD, Melo MAS, Lynch CD, Oates TW, Zhang K, Zhao Z, Xu HHK. A nano-CaF2-containing orthodontic cement with antibacterial and remineralization capabilities to combat enamel white spot lesions. J Dent. 2019 Oct;89:103172. doi: 10.1016/j.jdent.2019.07.010. Epub 2019 Jul 18. PMID: 31326528. | OFF TOPIC |
| Ibrahim AI, Thompson VP, Deb S. A Novel Etchant System for Orthodontic Bracket Bonding. Sci Rep. 2019 Jul 3;9(1):9579. doi: 10.1038/s41598-019-45980-9. PMID: 31270352; PMCID: PMC6610079. | OFF TOPIC |
| Bakry AS, Abbassy MA, Alharkan HF, Basuhail S, Al-Ghamdi K, Hill R. A Novel Fluoride Containing Bioactive Glass Paste is Capable of Re-Mineralizing Early Caries Lesions. Materials (Basel). 2018 Sep 6;11(9):1636. doi: 10.3390/ma11091636. PMID: 30200640; PMCID: PMC6163288. | OFF TOPIC |
| Erbe C, Hartmann L, Schmidtmann I, Ohlendorf D, Wehrbein H. A novel method quantifying caries following orthodontic treatment. Sci Rep. 2021 Nov 1;11(1):21347. doi: 10.1038/s41598-021-00561-7. PMID: 34725354; PMCID: PMC8560919. | OFF TOPIC |
| Erbe C, Jacobs C, Klukowska M, Timm H, Grender J, Wehrbein H. A randomized clinical trial to evaluate the plaque removal efficacy of an oscillating-rotating toothbrush versus a sonic toothbrush in orthodontic patients using digital imaging analysis of the anterior dentition. Angle Orthod. 2019 May;89(3):385-390. doi: 10.2319/080317-520.1. Epub 2018 Dec 5. PMID: 30516414; PMCID: PMC8117681. | OFF TOPIC |
| Kim H, Yoo KH, Yoon SY, Choi YK, Kim YI. A remineralizing orthodontic etchant that utilizes calcium phosphate ion clusters. Front Bioeng Biotechnol. 2022 Aug 31;10:944869. doi: 10.3389/fbioe.2022.944869. PMID: 36118566; PMCID: PMC9473508. | OFF TOPIC |
| Saito T, Park JH, Bay C. A Survey of Pediatric Dentists on the Treatment Timing and Modalities for White Spot Lesions in the United States. J Clin Pediatr Dent. 2019;43(1):27-33. doi: 10.17796/1053-4625-43.1.6. Epub 2018 Dec 6. PMID: 30520700. | OFF TOPIC |
| Al-Khafaji TJ, Agha B, Alhumadi A, Alhamadi WW, Mills D, Davis GR, Cresswell-Boyes AJ, Fleming PS. An assessment of mineral concentration of dental enamel neighbouring hypothetical orthodontic brackets using X-ray microtomography. J Dent. 2022 Nov;126:104306. doi: 10.1016/j.jdent.2022.104306. Epub 2022 Sep 23. PMID: 36162638. | OFF TOPIC |
| Velliyagounder K, Ardeshna A, Shah S. An In Vivo Study on the Development of Bacterial Microbiome on Clear Orthodontic Retainer. Dent J (Basel). 2022 Dec 16;10(12):239. doi: 10.3390/dj10120239. PMID: 36547055; PMCID: PMC9777160. | OFF TOPIC |
| Nafarrate-Valdez RA, Martínez-Martínez RE, Zaragoza-Contreras EA, Áyala-Herrera JL, Domínguez-Pérez RA, Reyes-López SY, Donohue-Cornejo A, Cuevas-González JC, Loyola-Rodríguez JP, Espinosa-Cristóbal LF. Anti-Adherence and Antimicrobial Activities of Silver Nanoparticles against Serotypes C and K of Streptococcus mutans on Orthodontic Appliances. Medicina (Kaunas). 2022 Jun 30;58(7):877. doi: 10.3390/medicina58070877. PMID: 35888596; PMCID: PMC9323808. | OFF TOPIC |
| Sharon E, Sharabi R, Eden A, Zabrovsky A, Ben-Gal G, Sharon E, Pietrokovski Y, Houri-Haddad Y, Beyth N. Antibacterial Activity of Orthodontic Cement Containing Quaternary Ammonium Polyethylenimine Nanoparticles Adjacent to Orthodontic Brackets. Int J Environ Res Public Health. 2018 Mar 27;15(4):606. doi: 10.3390/ijerph15040606. PMID: 29584643; PMCID: PMC5923648. | OFF TOPIC |
| Ferreira CJ, Leitune VCB, Balbinot GS, Degrazia FW, Arakelyan M, Sauro S, Mezzomo Collares F. Antibacterial and Remineralizing Fillers in Experimental Orthodontic Adhesives. Materials (Basel). 2019 Feb 21;12(4):652. doi: 10.3390/ma12040652. PMID: 30795577; PMCID: PMC6416618. | OFF TOPIC |
| Denis H, Werth R, Greuling A, Schwestka-Polly R, Stiesch M, Meyer-Kobbe V, Doll K. Antibacterial properties and abrasion-stability: Development of a novel silver-compound material for orthodontic bracket application. J Orofac Orthop. 2022 Jul 18. English. doi: 10.1007/s00056-022-00405-7. Epub ahead of print. PMID: 35849137. | OFF TOPIC |
| Yan J, Yang H, Luo T, Hua F, He H. Application of Amorphous Calcium Phosphate Agents in the Prevention and Treatment of Enamel Demineralization. Front Bioeng Biotechnol. 2022 May 13;10:853436. doi: 10.3389/fbioe.2022.853436. PMID: 35646855; PMCID: PMC9136455. | OFF TOPIC |
| Mahmood HT, Kamal AT, Khan BN, Fida M. Application of New Biomedical Materials in Orthodontic Appliances. J Coll Physicians Surg Pak. 2019 Jul;29(7):654-657. doi: 10.29271/jcpsp.2019.07.654. PMID: 31253218. | OFF TOPIC |
| Schneider BJ, Hiers RD, Currier GF, Kadioglu O, Johnston SE, Zhao YD, Esteban Florez FL, Khajotia SS. Assessment of Streptococcus mutans biofilms on orthodontic adhesives over 7 days. Am J Orthod Dentofacial Orthop. 2021 Jul;160(1):50-57. doi: 10.1016/j.ajodo.2020.03.026. Epub 2021 Jun 3. PMID: 34090735; PMCID: PMC8238838. | OFF TOPIC |
| Gulec A, Goymen M. Assessment of the resin infiltration and CPP-ACP applications before orthodontic brackets bonding. Dent Mater J. 2019 Oct 2;38(5):854-860. doi: 10.4012/dmj.2019-021. Epub 2019 Aug 22. PMID: 31434834. | OFF TOPIC |
| Al-Eesa NA, Karpukhina N, Hill RG, Johal A, Wong FSL. Bioactive glass composite for orthodontic adhesives—Formation and characterisation of apatites using MAS-NMR and SEM. Dent Mater. 2019 Apr;35(4):597-605. doi: 10.1016/j.dental.2019.02.010. Epub 2019 Feb 23. PMID: 30808559. | OFF TOPIC |
| Poornima P, Krithikadatta J, Ponraj RR, Velmurugan N, Kishen A. Biofilm formation following chitosan-based varnish or chlorhexidine-fluoride varnish application in patients undergoing fixed orthodontic treatment: a double blinded randomised controlled trial. BMC Oral Health. 2021 Sep 23;21(1):465. doi: 10.1186/s12903-021-01805-8. PMID: 34556107; PMCID: PMC8459499. | OFF TOPIC |
| Marques Ferreira de Sena L, Monielle Duarte Moura D, Helena Gurgel de Carvalho I, de Fatima Dantas de Almeida L, Ramos da Silva N, Othávio de Assunção E Souza R. Bond strength, degree of conversion, and microorganism adhesion using different bracket-to-enamel bonding protocols. J Orofac Orthop. 2022 Oct 17. English. doi: 10.1007/s00056-022-00430-6. Epub ahead of print. PMID: 36251054. | OFF TOPIC |
| Yang H, Ma Y, Xie X, Wang H, Li X, Fang D, Bai Y. Candida albicans enriched in orthodontic derived white spot lesions and shaped focal supragingival bacteriome. Front Microbiol. 2023 Jan 24;14:1084850. doi: 10.3389/fmicb.2023.1084850. PMID: 36760510; PMCID: PMC9902512. | OFF TOPIC |
| Philip N, Leishman SJ, Bandara HMHN, Walsh LJ. Casein Phosphopeptide-Amorphous Calcium Phosphate Attenuates Virulence and Modulates Microbial Ecology of Saliva-Derived Polymicrobial Biofilms. Caries Res. 2019;53(6):643-649. doi: 10.1159/000499869. Epub 2019 Jun 4. PMID: 31163430. | OFF TOPIC |
| Comert S, Oz AA. Clinical effect of a fluoride-releasing and rechargeable primer in reducing white spot lesions during orthodontic treatment. Am J Orthod Dentofacial Orthop. 2020 Jan;157(1):67-72. doi: 10.1016/j.ajodo.2019.06.013. PMID: 31901283. | OFF TOPIC |
| Kannan A, Padmanabhan S. Comparative evaluation of Icon® resin infiltration and Clinpro™ XT varnish on colour and fluorescence changes of white spot lesions: a randomized controlled trial. Prog Orthod. 2019 Jun 17;20(1):23. doi: 10.1186/s40510-019-0276-y. Erratum in: Prog Orthod. 2019 Jul 26;20(1):31. PMID: 31204437; PMCID: PMC6571438. | OFF TOPIC |
| Korkmaz YN, Yagci A. Comparing the effects of three different fluoride-releasing agents on white spot lesion prevention in patients treated with full coverage rapid maxillary expanders. Clin Oral Investig. 2019 Aug;23(8):3275-3285. doi: 10.1007/s00784-018-2749-7. Epub 2018 Nov 28. PMID: 30488120. | OFF TOPIC |
| Küçükönder A, Hatipoğlu Ö. Comparison between a glass ionomer cement and a compomer concerning bonded acrylic expander retention and white spot formation: A randomized clinical trial. J Orofac Orthop. 2023 Feb 10. English. doi: 10.1007/s00056-023-00448-4. Epub ahead of print. PMID: 36764948. | OFF TOPIC |
| Meyer-Kobbe V, Doll K, Stiesch M, Schwestka-Polly R, Demling A. Comparison of intraoral biofilm reduction on silver-coated and silver ion-implanted stainless steel bracket material: Biofilm reduction on silver ion-implanted bracket material. J Orofac Orthop. 2019 Jan;80(1):32-43. doi: 10.1007/s00056-018-00165-3. Epub 2018 Dec 10. PMID: 30535568; PMCID: PMC6334737. | OFF TOPIC |
| Knösel M, Vogel Alvarez R, Blanck-Lubarsch M, Helms HJ. Comparison of potential long-term costs for preventive dentistry treatment of post-orthodontic labial versus lingual enamel cavitations and esthetically relevant white-spot lesions: a simulation study with different scenarios. Head Face Med. 2019 Aug 9;15(1):22. doi: 10.1186/s13005-019-0204-x. PMID: 31399113; PMCID: PMC6688377. | OFF TOPIC |
| Knaup I, Kobbe C, Ehrlich EE, Esteves-Oliveira M, Abou-Ayash B, Meyer-Lueckel H, Wolf M, Wierichs RJ. Correlation of quantitative light-induced fluorescence and qualitative visual rating in infiltrated post-orthodontic white spot lesions. Eur J Orthod. 2023 Mar 31;45(2):133-141. doi: 10.1093/ejo/cjac051. PMID: 36179095. | OFF TOPIC |
| Wang Y, Hua F, Jiang H. CPP-ACP May be effective, but not Significantly Greater than using Fluorides Alone, in Preventing and Treating white Spot Lesions Around Orthodontic Brackets. J Evid Based Dent Pract. 2020 Mar;20(1):101416. doi: 10.1016/j.jebdp.2020.101416. Epub 2020 Feb 20. PMID: 32381413. | OFF TOPIC |
| Hua F, Yang H, He H. Current Enamel Remineralization Therapies Have Limited Effects on Postorthodontic White Spot Lesions. J Evid Based Dent Pract. 2018 Dec;18(4):339-342. doi: 10.1016/j.jebdp.2018.10.002. Epub 2018 Oct 16. PMID: 30514448. | OFF TOPIC |
| Cardoso AA, de Sousa ET, Steiner-Oliveira C, Nobre-Dos-Santos M. Debonding of orthodontic appliance changes salivary physicochemical properties and favors regression of active caries lesions: A 13-week follow-up study. Int J Paediatr Dent. 2022 Jul;32(4):607-616. doi: 10.1111/ipd.12939. Epub 2022 Feb 13. PMID: 34779541. | OFF TOPIC |
| Şen S, Erber R, Deurer N, Orhan G, Lux CJ, Zingler S. Demineralization detection in orthodontics using an ophthalmic optical coherence tomography device equipped with a multicolor fluorescence module. Clin Oral Investig. 2020 Aug;24(8):2579-2590. doi: 10.1007/s00784-019-03116-3. Epub 2019 Dec 17. PMID: 31848715. | OFF TOPIC |
| Umeh OD, Utomi IL, Ndukwe AN, Izuka M. Demineralization preventive practices among Nigerian orthodontists-An evidence-based approach? Niger J Clin Pract. 2020 May;23(5):589-595. doi: 10.4103/njcp.njcp_315_19. PMID: 32367863. | OFF TOPIC |
| Askar H, Krois J, Rohrer C, Mertens S, Elhennawy K, Ottolenghi L, Mazur M, Paris S, Schwendicke F. Detecting white spot lesions on dental photography using deep learning: A pilot study. J Dent. 2021 Apr;107:103615. doi: 10.1016/j.jdent.2021.103615. Epub 2021 Feb 19. PMID: 33617941. | OFF TOPIC |
| Jia A, Wang P, Tong F, Chen Z, Deng Y, Yao H, Wang L, Liu Y, Ge H. Developing a Novel Enamel Adhesive with Amorphous Calcium Phosphate and Silver Nanoparticles to Prevent Demineralization during Orthodontic Treatment. J Funct Biomater. 2023 Jan 29;14(2):77. doi: 10.3390/jfb14020077. PMID: 36826876; PMCID: PMC9966906. | OFF TOPIC |
| Sampson V, Sampson A. Diagnosis and treatment options for anterior white spot lesions. Br Dent J. 2020 Sep;229(6):348-352. doi: 10.1038/s41415-020-2057-x. Epub 2020 Sep 25. PMID: 32978577. | REVIEW |
| Yetkiner E, Gürlek Ö, Işık A, Lappin DF, Buduneli N. Do Adhesive Flash-free Brackets Affect Bacterial Plaque in Patients with Adequate Oral Hygiene? A Randomised Controlled Clinical and Microbiological Assessment. Oral Health Prev Dent. 2019;17(6):533-539. doi: 10.3290/j.ohpd.a43753. PMID: 31825025. | OFF TOPIC |
| Rafiei E, Fadaei Tehrani P, Yassaei S, Haerian A. Effect of CO2 laser (10.6 μm) and Remin Pro on microhardness of enamel white spot lesions. Lasers Med Sci. 2020 Jul;35(5):1193-1203. doi: 10.1007/s10103-020-02970-y. Epub 2020 Feb 1. PMID: 32006264. | OFF TOPIC |
| Yetkin D, Sayar G. Effect of Fluoride Releasing Bonding Materials on Shear Bond Strength of Orthodontic Brackets. Turk J Orthod. 2020 Mar 1;33(1):52-58. doi: 10.5152/TurkJOrthod.2020.19052. PMID: 32284899; PMCID: PMC7138233. | OFF TOPIC |
| Salamara O, Papadimitriou A, Mortensen D, Twetman S, Koletsi D, Gizani S. Effect of fluoride varnish with functionalized tri-calcium phosphate on post-orthodontic white spot lesions: an investigator-blinded controlled trial. Quintessence Int. 2020;51(10):854-862. doi: 10.3290/j.qi.a44810. PMID: 32577707. | OFF TOPIC |
| Ferreira RS, Ricomini-Filho AP, Tabchoury CP, Vale GC. Effect of high-fluoride dentifrice and bracket bonding composite material on enamel demineralization in situ. Clin Oral Investig. 2020 Sep;24(9):3105-3112. doi: 10.1007/s00784-019-03182-7. Epub 2020 Jan 2. PMID: 31897706. | OFF TOPIC |
| Ali A, Ismail H, Amin K. Effect of nanosilver mouthwash on prevention of white spot lesions in patients undergoing fixed orthodontic treatment—a randomized double-blind clinical trial. J Dent Sci. 2022 Jan;17(1):249-255. doi: 10.1016/j.jds.2021.03.016. Epub 2021 May 1. PMID: 35028045; PMCID: PMC8739266. | OFF TOPIC |
| Ghadirian H, Geramy A, Shallal W, Heidari S, Noshiri N, Keshvad MA. The Effect of Remineralizing Agents With/Without CO2 Laser Irradiation on Structural and Mechanical Properties of Enamel and its Shear Bond Strength to Orthodontic Brackets. J Lasers Med Sci. 2020 Spring;11(2):144-152. doi: 10.34172/jlms.2020.25. Epub 2020 Mar 15. PMID: 32273955; PMCID: PMC7118509. | OFF TOPIC |
| Alqahtani MA, Almosa NA, Alsaif KA, Alsaif NM, Aljaser YJ. Effect of topical fluoride application and diode laser-irradiation on white spot lesions of human enamel. Saudi Dent J. 2021 Dec;33(8):937-943. doi: 10.1016/j.sdentj.2021.08.007. Epub 2021 Aug 23. PMID: 34938035; PMCID: PMC8665184. | IN VITRO |
| Handa A, Chengappa D, Sharma P, Handa JK. Effectiveness of Clinpro Tooth Crème in comparison with MI Varnish with RECALDENT™ for treatment of white spot lesions: a randomized controlled trial. Clin Oral Investig. 2022 Nov 2. doi: 10.1007/s00784-022-04766-6. Epub ahead of print. PMID: 36322154. | OFF TOPIC |
| Yıldırım ZB, Ramoğlu Sİ. Effects of a flash-free system on dental plaque accumulation and bonding-debonding process: A clinical study. Am J Orthod Dentofacial Orthop. 2023 Jan;163(1):54-59. doi: 10.1016/j.ajodo.2021.08.024. Epub 2022 Oct 8. PMID: 36216622. | OFF TOPIC |
| Hennig CL, Blochberger B, Symmank J, Nitzsche Á, Nietzsche S, Steiniger F, Dederichs M, Güllmar A, Reise M, Schulze-Späte U, Sigusch B, Jacobs C. Effects of reducing excess dental adhesive on bacterial adhesion in the bracket periphery. Clin Oral Investig. 2023 Feb 21. doi: 10.1007/s00784-023-04924-4. Epub ahead of print. PMID: 36809356. | OFF TOPIC |
| Gómez C, Abellán R, Palma JC. Efficacy of photodynamic therapy vs ultrasonic scaler for preventing gingival inflammation and white spot lesions during orthodontic treatment. Photodiagnosis Photodyn Ther. 2018 Dec;24:377-383. doi: 10.1016/j.pdpdt.2018.11.001. Epub 2018 Nov 3. PMID: 30399455. | OFF TOPIC |
References
- Lucchese, A.; Gherlone, E. Prevalence of White-Spot Lesions before and during Orthodontic Treatment with Fixed Appliances. Eur. J. Orthod. 2013, 35, 664–668. [Google Scholar] [CrossRef]
- Julien, K.C.; Buschang, P.H.; Campbell, P.M. Prevalence of White Spot Lesion Formation during Orthodontic Treatment. Angle Orthod. 2013, 83, 641–647. [Google Scholar] [CrossRef]
- Sundararaj, D.; Venkatachalapathy, S.; Tandon, A.; Pereira, A. Critical Evaluation of Incidence and Prevalence of White Spot Lesions during Fixed Orthodontic Appliance Treatment: A Meta-Analysis. J. Int. Soc. Prev. Community Dent. 2015, 5, 433–439. [Google Scholar] [CrossRef] [PubMed]
- Enaia, M.; Bock, N.; Ruf, S. White-Spot Lesions during Multibracket Appliance Treatment: A Challenge for Clinical Excellence. Am. J. Orthod. Dentofac. Orthop. 2011, 140, e17–e24. [Google Scholar] [CrossRef]
- Melrose, C.A.; Appleton, J.; Lovius, B.B. A Scanning Electron Microscopic Study of Early Enamel Caries Formed in Vivo beneath Orthodontic Bands. Br. J. Orthod. 1996, 23, 43–47. [Google Scholar] [CrossRef] [PubMed]
- Gorelick, L.; Geiger, A.M.; Gwinnett, A.J. Incidence of White Spot Formation after Bonding and Banding. Am. J. Orthod. 1982, 81, 93–98. [Google Scholar] [CrossRef]
- Flynn, L.N.; Julien, K.; Noureldin, A.; Buschang, P.H. The Efficacy of Fluoride Varnish vs a Filled Resin Sealant for Preventing White Spot Lesions during Orthodontic Treatment. Angle Orthod. 2022, 92, 204–212. [Google Scholar] [CrossRef] [PubMed]
- Marinelli, G.; Inchingolo, A.D.; Inchingolo, A.M.; Malcangi, G.; Limongelli, L.; Montenegro, V.; Coloccia, G.; Laudadio, C.; Patano, A.; Inchingolo, F.; et al. White Spot Lesions in Orthodontics: Prevention and Treatment. A Descriptive Review. J. Biol. Regul. Homeost. Agents 2021, 35, 227–240. [Google Scholar] [CrossRef]
- Ogaard, B.; Rølla, G.; Arends, J. Orthodontic Appliances and Enamel Demineralization. Part 1. Lesion Development. Am. J. Orthod. Dentofac. Orthop. 1988, 94, 68–73. [Google Scholar] [CrossRef]
- Heymann, G.C.; Grauer, D. A Contemporary Review of White Spot Lesions in Orthodontics. J. Esthet. Restor. Dent. 2013, 25, 85–95. [Google Scholar] [CrossRef]
- Paolone, G.; Mazzitelli, C.; Formiga, S.; Kaitsas, F.; Breschi, L.; Mazzoni, A.; Tete, G.; Polizzi, E.; Gherlone, E.; Cantatore, G. One-Year Impact of COVID-19 Pandemic on Italian Dental Professionals: A Cross-Sectional Survey. Minerva. Dent. Oral. Sci. 2022, 71, 212–222. [Google Scholar] [CrossRef] [PubMed]
- Paolone, G.; Scolavino, S.; Gherlone, E.; Spagnuolo, G.; Cantatore, G. The “Pre-Finishing” Approach in Direct Anterior Restorations. A Case Series. Dent. J. 2021, 9, 79. [Google Scholar] [CrossRef] [PubMed]
- Chapman, J.A.; Roberts, W.E.; Eckert, G.J.; Kula, K.S.; González-Cabezas, C. Risk Factors for Incidence and Severity of White Spot Lesions during Treatment with Fixed Orthodontic Appliances. Am. J. Orthod. Dentofac. Orthop. 2010, 138, 188–194. [Google Scholar] [CrossRef]
- Folco, A.A.; Benítez-Rogé, S.C.; Iglesias, M.; Calabrese, D.; Pelizardi, C.; Rosa, A.; Brusca, M.I.; Hecht, P.; Mateu, M.E. Gingival response in orthodontic patients: Comparative study between self-ligating and conventional brackets. Acta Odontol. Latinoam. AOL 2014, 27, 120–124. [Google Scholar] [CrossRef] [PubMed]
- Taibah, S.; Abubakr, N.H.; Ziada, H. Perspectives of Orthodontists of the Diagnosis, Prevention, and Management of White Spot Lesions: A Qualitative Study. J. Int. Soc. Prev. Community Dent. 2022, 12, 117–125. [Google Scholar] [CrossRef]
- Dipalma, G.; Inchingolo, A.D.; Inchingolo, F.; Charitos, I.A.; Cosola, M.D.; Cazzolla, A.P. Focus on the Cariogenic Process: Microbial and Biochemical Interactions with Teeth and Oral Environment. J. Biol. Regul. Homeost. Agents 2021, 35, 429–440. [Google Scholar] [CrossRef]
- Tanner, A.C.R.; Sonis, A.L.; Lif Holgerson, P.; Starr, J.R.; Nunez, Y.; Kressirer, C.A.; Paster, B.J.; Johansson, I. White-Spot Lesions and Gingivitis Microbiotas in Orthodontic Patients. J. Dent. Res. 2012, 91, 853–858. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Pilli, L.N.; Singaraju, G.S.; Nettam, V.; Keerthipati, T.; Mandava, P.; Marya, A. An Extensive Comparison of the Clinical Efficiency of Acidulated Phosphate Fluoride (APF) and Neutral Sodium Fluoride (NaF) Oral Rinses in the Prevention of White Spot Lesions during Fixed Orthodontic Treatment: A Randomized Controlled Trial. Biomed Res. Int. 2022, 2022, 6828657. [Google Scholar] [CrossRef]
- Pinto, A.S.; Alves, L.S.; Maltz, M.; Zenkner, J.E.D.A. Association between Fixed Orthodontic Treatment and Dental Caries: A 1-Year Longitudinal Study. Braz. Oral Res. 2020, 35, e002. [Google Scholar] [CrossRef]
- Belcheva, A.B.; Shindova, M.P. Caries Inhibition with CO2-Laser during Orthodontic Treatment: A Study Protocol for a Randomized Split-Mouth Controlled Clinical Trial. Trials 2022, 23, 208. [Google Scholar] [CrossRef] [PubMed]
- Jurela, A.; Sudarević, K.; Budimir, A.; Brailo, V.; Lončar Brzak, B.; Janković, B. Clinical and Salivary Findings in Patients with Metal and Crystalline Conventional and Self-Ligating Orthodontic Brackets. Acta Stomatol. Croat. 2019, 53, 224–230. [Google Scholar] [CrossRef]
- Yagci, A.; Seker, E.D.; Demirsoy, K.K.; Ramoglu, S.I. Do Total or Partial Etching Procedures Effect the Rate of White Spot Lesion Formation? A Single-Center, Randomized, Controlled Clinical Trial. Angle Orthod. 2019, 89, 16–24. [Google Scholar] [CrossRef]
- Mahmoudzadeh, M.; Alijani, S.; Soufi, L.R.; Farhadian, M.; Namdar, F.; Karami, S. Effect of CO2 Laser on the Prevention of White Spot Lesions During Fixed Orthodontic Treatment: A Randomized Clinical Trial. Turk. J. Orthod. 2019, 32, 165–171. [Google Scholar] [CrossRef] [PubMed]
- Jing, D.; Hao, J.; Shen, Y.; Tang, G.; Lei, L.; Zhao, Z. Effect of Fixed Orthodontic Treatment on Oral Microbiota and Salivary Proteins. Exp. Med. 2019, 17, 4237–4243. [Google Scholar] [CrossRef] [PubMed]
- Kau, C.H.; Wang, J.; Palombini, A.; Abou-Kheir, N.; Christou, T. Effect of Fluoride Dentifrices on White Spot Lesions during Orthodontic Treatment: A Randomized Trial. Angle Orthod. 2019, 89, 365–371. [Google Scholar] [CrossRef] [PubMed]
- Gizani, S.; Petsi, G.; Twetman, S.; Caroni, C.; Makou, M.; Papagianoulis, L. Effect of the Probiotic Bacterium Lactobacillus reuteri on White Spot Lesion Development in Orthodontic Patients. Eur. J. Orthod. 2016, 38, 85–89. [Google Scholar] [CrossRef] [PubMed]
- Oz, A.Z.; Oz, A.A.; Yazicioglu, S.; Sancaktar, O. Effectiveness of an Antibacterial Primer Used with Adhesive-Coated Brackets on Enamel Demineralization around Brackets: An in Vivo Study. Prog. Orthod. 2019, 20, 15. [Google Scholar] [CrossRef]
- Cheng, H.-C.; Hu, H.-T.; Chang, Y.-C. Effectiveness of Enzyme Dentifrices on Oral Health in Orthodontic Patients: A Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2019, 16, 2243. [Google Scholar] [CrossRef]
- Shimpo, Y.; Nomura, Y.; Sekiya, T.; Arai, C.; Okada, A.; Sogabe, K.; Hanada, N.; Tomonari, H. Effects of the Dental Caries Preventive Procedure on the White Spot Lesions during Orthodontic Treatment-An Open Label Randomized Controlled Trial. J. Clin. Med. 2022, 11, 854. [Google Scholar] [CrossRef]
- Degrazia, F.W.; Altmann, A.S.P.; Ferreira, C.J.; Arthur, R.A.; Leitune, V.C.B.; Samuel, S.M.W.; Collares, F.M. Evaluation of an Antibacterial Orthodontic Adhesive Incorporated with Niobium-Based Bioglass: An In Situ Study. Braz. Oral Res. 2019, 33, e010. [Google Scholar] [CrossRef] [PubMed]
- Sonesson, M.; Brechter, A.; Abdulraheem, S.; Lindman, R.; Twetman, S. Fluoride Varnish for the Prevention of White Spot Lesions during Orthodontic Treatment with Fixed Appliances: A Randomized Controlled Trial. Eur. J. Orthod. 2020, 42, 326–330. [Google Scholar] [CrossRef] [PubMed]
- Smyth, R.S.D.; Noar, J.H. Preventing White Spot Lesions with Fluoride Pastes. Evid. Based Dent. 2019, 20, 88–89. [Google Scholar] [CrossRef] [PubMed]
- George, J.A.; Srinivasan, B.; Kailasam, V. The Effect of Active Oxygen-Containing Toothpaste on Streptococcus mutans and White Spot Lesions: An in-Vivo Randomized Controlled Trial. Am. J. Orthod. Dentofac. Orthop. 2022, 162, 594–600. [Google Scholar] [CrossRef]
- Inchingolo, A.D.; Patano, A.; Coloccia, G.; Ceci, S.; Inchingolo, A.M.; Marinelli, G.; Malcangi, G.; Montenegro, V.; Laudadio, C.; Palmieri, G.; et al. Genetic Pattern, Orthodontic and Surgical Management of Multiple Supplementary Impacted Teeth in a Rare, Cleidocranial Dysplasia Patient: A Case Report. Medicina 2021, 57, 1350. [Google Scholar] [CrossRef] [PubMed]
- Degrazia, F.W.; Genari, B.; Leitune, V.C.B.; Arthur, R.A.; Luxan, S.A.; Samuel, S.M.W.; Collares, F.M.; Sauro, S. Polymerisation, Antibacterial and Bioactivity Properties of Experimental Orthodontic Adhesives Containing Triclosan-Loaded Halloysite Nanotubes. J. Dent. 2018, 69, 77–82. [Google Scholar] [CrossRef] [PubMed]
- Maspero, C.; Abate, A.; Inchingolo, F.; Dolci, C.; Cagetti, M.G.; Tartaglia, G.M. Incidental Finding in Pre-Orthodontic Treatment Radiographs of an Aural Foreign Body: A Case Report. Children 2022, 9, 421. [Google Scholar] [CrossRef]
- Inchingolo, A.M.; Fatone, M.C.; Malcangi, G.; Avantario, P.; Piras, F.; Patano, A.; Di Pede, C.; Netti, A.; Ciocia, A.M.; De Ruvo, E.; et al. Modifiable Risk Factors of Non-Syndromic Orofacial Clefts: A Systematic Review. Children 2022, 9, 1846. [Google Scholar] [CrossRef]
- Pasciuti, E.; Coloccia, G.; Inchingolo, A.D.; Patano, A.; Ceci, S.; Bordea, I.R.; Cardarelli, F.; Di Venere, D.; Inchingolo, F.; Dipalma, G. Deep Bite Treatment with Aligners: A New Protocol. Appl. Sci. 2022, 12, 6709. [Google Scholar] [CrossRef]
- Inchingolo, A.D.; Patano, A.; Coloccia, G.; Ceci, S.; Inchingolo, A.M.; Marinelli, G.; Malcangi, G.; Di Pede, C.; Garibaldi, M.; Ciocia, A.M.; et al. Treatment of Class III Malocclusion and Anterior Crossbite with Aligners: A Case Report. Medicina 2022, 58, 603. [Google Scholar] [CrossRef]
- Ballini, A.; Cantore, S.; Signorini, L.; Saini, R.; Scacco, S.; Gnoni, A.; Inchingolo, A.D.; Vito, D.D.; Santacroce, L.; Inchingolo, F.; et al. Efficacy of Sea Salt-Based Mouthwash and Xylitol in Improving Oral Hygiene among Adolescent Population: A Pilot Study. Int. J. Environ. Res. Public Health 2021, 18, 44. [Google Scholar] [CrossRef]
- Ballini, A.; Cantore, S.; Saini, R.; Pettini, F.; Fotopoulou, E.A.; Saini, S.R.; Georgakopoulos, I.P.; Dipalma, G.; Gargiulo Isacco, C.; Inchingolo, F. Effect of Activated Charcoal Probiotic Toothpaste Containing Lactobacillus paracasei and Xylitol on Dental Caries: A Randomized and Controlled Clinical Trial. J. Biol. Regul. Homeost. Agents 2019, 33, 977–981. [Google Scholar]
- Pascotto, R.C.; de Lima Navarro, M.F.; Capelozza Filho, L.; Cury, J.A. In Vivo Effect of a Resin-Modified Glass Ionomer Cement on Enamel Demineralization around Orthodontic Brackets. Am. J. Orthod. Dentofac. Orthop. 2004, 125, 36–41. [Google Scholar] [CrossRef] [PubMed]
- Sonesson, M.; Twetman, S.; Bondemark, L. Effectiveness of High-Fluoride Toothpaste on Enamel Demineralization during Orthodontic Treatment-a Multicenter Randomized Controlled Trial. Eur. J. Orthod. 2014, 36, 678–682. [Google Scholar] [CrossRef] [PubMed]
- Nascimento, P.L.D.M.M.; Fernandes, M.T.G.; Figueiredo, F.E.D.D.; Faria-e-Silva, A.L. Fluoride-Releasing Materials to Prevent White Spot Lesions around Orthodontic Brackets: A Systematic Review. Braz. Dent. J. 2016, 27, 101–107. [Google Scholar] [CrossRef]
- Sardana, D.; Zhang, J.; Ekambaram, M.; Yang, Y.; McGrath, C.P.; Yiu, C.K.Y. Effectiveness of Professional Fluorides against Enamel White Spot Lesions during Fixed Orthodontic Treatment: A Systematic Review and Meta-Analysis. J. Dent. 2019, 82, 1–10. [Google Scholar] [CrossRef]
- Jablonowski, B.L.; Bartoloni, J.A.; Hensley, D.M.; Vandewalle, K.S. Fluoride Release from Newly Marketed Fluoride Varnishes. Quintessence Int. 2012, 43, 221–228. [Google Scholar] [PubMed]
- Inchingolo, A.M.; Malcangi, G.; Costa, S.; Fatone, M.C.; Avantario, P.; Campanelli, M.; Piras, F.; Patano, A.; Ferrara, I.; Di Pede, C.; et al. Tooth Complications after Orthodontic Miniscrews Insertion. Int. J. Environ. Res. Public Health 2023, 20, 1562. [Google Scholar] [CrossRef]
- Akhavan, A.; Sodagar, A.; Mojtahedzadeh, F.; Sodagar, K. Investigating the Effect of Incorporating Nanosilver/Nanohydroxyapatite Particles on the Shear Bond Strength of Orthodontic Adhesives. Acta Odontol. Scand. 2013, 71, 1038–1042. [Google Scholar] [CrossRef]
- Esteves-Oliveira, M.; Pasaporti, C.; Heussen, N.; Eduardo, C.P.; Lampert, F.; Apel, C. Rehardening of Acid-Softened Enamel and Prevention of Enamel Softening through CO2 Laser Irradiation. J. Dent. 2011, 39, 414–421. [Google Scholar] [CrossRef]
- Altmann, A.S.P.; Collares, F.M.; Balbinot, G.D.S.; Leitune, V.C.B.; Takimi, A.S.; Samuel, S.M.W. Niobium Pentoxide Phosphate Invert Glass as a Mineralizing Agent in an Experimental Orthodontic Adhesive. Angle Orthod. 2017, 87, 759–765. [Google Scholar] [CrossRef] [PubMed]
- Degrazia, F.W.; Leitune VC, B.; Garcia, I.M.; Arthur, R.A.; Samuel, S.M.W.; Collares, F.M. Effect of Silver Nanoparticles on the Physicochemical and Antimicrobial Properties of an Orthodontic Adhesive. J. Appl. Oral Sci. 2016, 24, 404–410. [Google Scholar] [CrossRef] [PubMed]
- Fan, C.; Chu, L.; Rawls, H.R.; Norling, B.K.; Cardenas, H.L.; Whang, K. Development of an Antimicrobial Resin--a Pilot Study. Dent. Mater. 2011, 27, 322–328. [Google Scholar] [CrossRef]
- Steiner-Oliveira, C.; Nobre-dos-Santos, M.; Zero, D.T.; Eckert, G.; Hara, A.T. Effect of a Pulsed CO2 Laser and Fluoride on the Prevention of Enamel and Dentine Erosion. Arch. Oral Biol. 2010, 55, 127–133. [Google Scholar] [CrossRef] [PubMed]
- Mirhashemi, A.H.; Hakimi, S.; Ahmad Akhoundi, M.S.; Chiniforush, N. Prevention of Enamel Adjacent to Bracket Demineralization Following Carbon Dioxide Laser Radiation and Titanium Tetra Fluoride Solution Treatment: An In Vitro Study. J. Lasers Med. Sci. 2016, 7, 192–196. [Google Scholar] [CrossRef] [PubMed]
- Tepper, S.A.; Zehnder, M.; Pajarola, G.F.; Schmidlin, P.R. Increased Fluoride Uptake and Acid Resistance by CO2 Laser-Irradiation through Topically Applied Fluoride on Human Enamel in Vitro. J. Dent. 2004, 32, 635–641. [Google Scholar] [CrossRef]
- Rechmann, P.; Charland, D.A.; Rechmann, B.M.T.; Le, C.Q.; Featherstone, J.D.B. In-Vivo Occlusal Caries Prevention by Pulsed CO2 -Laser and Fluoride Varnish Treatment--a Clinical Pilot Study. Lasers Surg. Med. 2013, 45, 302–310. [Google Scholar] [CrossRef] [PubMed]
- Inchingolo, A.D.; Patano, A.; Coloccia, G.; Ceci, S.; Inchingolo, A.M.; Marinelli, G.; Malcangi, G.; Montenegro, V.; Laudadio, C.; Pede, C.D.; et al. The Efficacy of a New AMCOP® Elastodontic Protocol for Orthodontic Interceptive Treatment: A Case Series and Literature Overview. Int. J. Envrion. Res. Public Health 2022, 19, 988. [Google Scholar] [CrossRef]
- Chang, H.S.; Walsh, L.J.; Freer, T.J. Enamel Demineralization during Orthodontic Treatment. Aetiology and Prevention. Aust. Dent. J. 1997, 42, 322–327. [Google Scholar] [CrossRef]
- Lovrov, S.; Hertrich, K.; Hirschfelder, U. Enamel Demineralization during Fixed Orthodontic Treatment—Incidence and Correlation to Various Oral-Hygiene Parameters. J. Orofac. Orthop. 2007, 68, 353–363. [Google Scholar] [CrossRef]
- Inchingolo, A.D.; Carpentiere, V.; Piras, F.; Netti, A.; Ferrara, I.; Campanelli, M.; Latini, G.; Viapiano, F.; Costa, S.; Malcangi, G.; et al. Orthodontic Surgical Treatment of Impacted Mandibular Canines: Systematic Review and Case Report. Appl. Sci. 2022, 12, 8008. [Google Scholar] [CrossRef]
- McCambridge, J.; de Bruin, M.; Witton, J. The Effects of Demand Characteristics on Research Participant Behaviours in Non-Laboratory Settings: A Systematic Review. PLoS ONE 2012, 7, e39116. [Google Scholar] [CrossRef] [PubMed]
- Benson, P.E.; Parkin, N.; Dyer, F.; Millett, D.T.; Furness, S.; Germain, P. Fluorides for the Prevention of Early Tooth Decay (Demineralised White Lesions) during Fixed Brace Treatment. Cochrane Database Syst. Rev. 2013, CD003809. [Google Scholar] [CrossRef]
- Uysal, T.; Amasyali, M.; Ozcan, S.; Koyuturk, A.E.; Sagdic, D. Effect of Antibacterial Monomer-Containing Adhesive on Enamel Demineralization around Orthodontic Brackets: An in-Vivo Study. Am. J. Orthod. Dentofac. Orthop. 2011, 139, 650–656. [Google Scholar] [CrossRef] [PubMed]
- Oz, A.Z.; Oz, A.A.; Yazıcıoglu, S. In Vivo Effect of Antibacterial and Fluoride-Releasing Adhesives on Enamel Demineralization around Brackets: A Micro-CT Study. Angle Orthod. 2017, 87, 841–846. [Google Scholar] [CrossRef] [PubMed]
- Paschos, E.; Kurochkina, N.; Huth, K.C.; Hansson, C.S.; Rudzki-Janson, I. Failure Rate of Brackets Bonded with Antimicrobial and Fluoride-Releasing, Self-Etching Primer and the Effect on Prevention of Enamel Demineralization. Am. J. Orthod. Dentofac. Orthop. 2009, 135, 613–620. [Google Scholar] [CrossRef] [PubMed]
- Sunna, S.; Rock, W.P. Clinical Performance of Orthodontic Brackets and Adhesive Systems: A Randomized Clinical Trial. Br. J. Orthod. 1998, 25, 283–287. [Google Scholar] [CrossRef]
- Cirulli, N.; Inchingolo, A.D.; Patano, A.; Ceci, S.; Marinelli, G.; Malcangi, G.; Coloccia, G.; Montenegro, V.; Di Pede, C.; Ciocia, A.M.; et al. Innovative Application of Diathermy in Orthodontics: A Case Report. Int. J. Environ. Res. Public Health 2022, 19, 7448. [Google Scholar] [CrossRef]


| Article screening Strategy | Database: Scopus, Web of Science and Pubmed |
| Keywords: A “WS”; B “fixed orthodont*” | |
| Boolean variable: AND | |
| Timespan: 2018–2023 | |
| Language: English |
| Authors | Type of Study | Object | Study Design and Timeline | Results |
|---|---|---|---|---|
| Pilli et al., 2022 [19] | RCT | Comparison of efficiency of one rinse per week with NaF and daily rinse with APF (acid phosphate) in preventing WS associated with FOT. | A total of 90 patients, weekly and daily administration (see subject) and subsequent evaluation with ICDAS (International Caries Detection and Assessment System) and GI (Gingival Index) indices. | For the prevention of WS, daily use of acid phosphate mouthwash is more effective than the once-weekly use of sodium fluoride mouthwash. |
| Pinto et al., 2020 [20] | Longitudinal study | To assess the incidence of active caries in PT undergoing fixed therapy. | 135 patients divided into 2 groups, 1 without treatment and 1 with orthodontic treatment, observed for 1 year. | Individuals in fixed therapy for a period of one year had a higher incidence and increase in active carious lesions than did those without fixed braces. |
| Belcheva et al., 2022 [21] | RCT | Analyze how well the CO2 laser and a fluorine-based varnish work together to prevent WS during fixed therapy. | Children who need fixed therapy between the ages of 12 and 18. The buccal surfaces of the anterior upper teeth of the patients in the first group were treated with the CO2 laser in conjunction with fluorotherapy, whereas the patients in the second group were treated with a fluoride-based varnish before having brackets placed. Following up is scheduled for 6 and 12 months. | Using CO2 lasers to prevent dental caries has enormous potential. |
| Jurela et al., 2019 [22] | Clinical trial | The primary objective was to assess patients’ DMFTs wearing various types of brackets and ligatures, before and six months into fixed therapy. Finding out how orthodontic treatment affected these individuals’ plaque indices, salivary pHs, flows, and prevalence of WS, was the secondary goal. | 52 women and 31 men out of 83 patients were tracked for 2 years. | Fixed therapy may impact intraoral homeostasis, regardless of the attachment and ligature type, since DMFT (decay-missing-filled teeth) index and salivary flow increased significantly while salivary pH declined significantly in all patient groups. |
| Yagci et al., 2019 [23] | RCT | Determine whether partial or full etching has an impact on the presence of WS. | At the T0, three (T1), and six (T2) months into orthodontic therapy, as well as when the procedure was complete, fluorescence measurements of the enamel surface were taken (T3). | As time goes on, there is no distinction between PE (partial etching) and TE (total etching), in terms of the formation of WSLs. |
| Mahmoudzadeh et al., 2019 [24] | RCT | Impact of CO2 laser during fixed therapy on profilaxis of WS. | 95 patients, aged 12 to 30, have 554 anterior upper teeth. In four areas (gingival, incisal, mesial, and distal), at both the initial period and six months following CO2 laser irradiation, the incidence, extent, and gravity of lesions were evaluated. | The incidence of WS seems to be reduced thanks to CO2 laser irradiation. |
| Jing et al., 2019 [25] | Prospective comparative cohort study | To investigate changes in the bacteria Lactobacillus and Streptococcus (S.) mutans in the saliva of individuals with FOT. | During FOT, 15 patients’ immune responses and inflammatory processes, as well as secretory immunoglobulin A (sIgA), myeloperoxidase (MPO), and lactate dehydrogenase (LDH), were examined. | Patients receiving fixed therapy have been found to have an increase in S. mutans bacteria in the oral microbiota. |
| Kau et al., 2019 [26] | RCT | To establish how some fluoride-containing products (Clinpro 5000, Clinpro Tooth Crème, and MI-Paste Plus) influence the development of WS in patients receiving fixed therapy. | 120 individuals were recruited for the 3 prospective groups, each of which consisted of 40 orthodontic patients. During four months, the chosen product was brushed twice daily for two minutes. Four months of monthly evaluations were conducted on the subjects. At each visit, EDI was utilized to calculate the quantity of WS per square inch. | All products effectively prevented WS. |
| Gizani et al., 2016 [27] | RCT | The aim of the study is to evaluate the impact of the daily intake of probiotic bacteria on the appearance of WS and salivary lactobacilli (LB) and mutans streptococci (SM) counts in patients undergoing orthodontic therapy with fixed appliances. | 85 patients were randomly divided into 2 groups. Probiotic tablets containing two strains of Lactobacillus reuteri were given to the test group once a day. A similar tablet was provided to the placebo group, but it did not contain live bacteria. | Probiotic supplements have not been shown to reduce the appearance of WS. |
| Oz et al., 2019 [28] | In vivo study | The aim of the study is to investigate the ability of a primer containing antibacterial monomer on the prevention of WS during fixed treatment. | 35 patients with a mean age of 14.4 years were identified for (1) optimal oral hygiene; (2) permanent teeth; (3) no restorations on the buccal sides of the teeth; and (4) absence of evident WS on the enamel surfaces of the buccal teeth. Before gluing the fixed appliances, each tooth was thoroughly cleaned and polished. | Throughout the duration of orthodontic therapy, there was no significant difference between the group using antibacterial monomer primers and the control group, in terms of demineralization reduction. The best way to prevent WS during fixed therapy is still considered to be good oral hygiene. |
| Cheng et al., 2019 [29] | RCT | Comparison of three types of toothpaste: (1) containing enzymes (amyloglucosidase and glucose oxidase); (2) containing fluoride; and (3) natural, chemical-free toothpastes. | 42 orthodontic patients (25 women and 17 men, mean age 22.7 ± 4.2 years), divided into 3 groups and assigned to use 3 different types of toothpastes during the first 3 months of treatment. | There are no substantial differences between enzyme-containing toothpaste and fluoride-containing toothpaste, in preventing WS in the first 3 months of fixed therapy. |
| Shimpo et al., 2022 [30] | RCT | The aim of the study was to investigate the ability of a disinfectant applied to the tooth surface, together with fluorine, to prevent WS during fixed treatment. | Patients aged 13–35 years, on fixed therapy, at high risk of caries due to high levels of Streptococcus mutans, who have not taken antibiotics in the weeks prior to salivary sampling. | Tooth surface disinfection together with fluoride application reduces WS during fixed treatment. |
| Degrazia et al., 2019 [31] | In situ study | This in-depth study tested an experimental orthodontic adhesive with triazine and niobium phosphate bioglass placed around brackets for its ability to fight bacteria and prevent demineralization. | Adhesion of brackets to enamel with adhesives containing triazine and niobium phosphate inverted glass reduces demineralization and/or contributes to the recovery of the mineral content of the enamel. The item can stop enamel from losing minerals, preventing the development of WS. | |
| Sonesson et al., 2020 [32] | RCT | To determine if a new fluoride varnish recipe (1.5% ammonium fluoride) is effective at preventing WS in teenagers receiving multiple orthodontic brackets. | 166 patients were divided into 2 groups. Fluoride varnish was administered to the test group’s brackets every six weeks. Placebo group: fluoride-free paint. | The incidence of WS as an adverse effect of fixed therapy was reduced by routine applications of an ammonium fluoride varnish. |
| Smythe and Noar 2019 [33] | RCT | Clinpro Tooth Crème, Clinpro 5000, and MI Paste Plus on WS development in pt with fixed appliances is the goal of this study. Casein phosphopeptide-amorphous calcium phosphate is present in MI Paste Plus. The toothpastes Clinpro 5000 and Clinpro Tooth Crème each include sodium fluoride. | Use of one of the three products for four months in each of three groups of patients receiving fixed therapy. | The products tested were all able to prevent WS. |
| George et al., 2022 [34] | RCT | The objective of this study was to evaluate how well fixed treatment patients’ salivary Streptococcus mutans growth was inhibited by active oxygen. | Two groups of patients, one used toothpaste with added active oxygen and the other group used fluoride toothpaste. | There is no discernible difference, in preventing WS, between toothpastes containing fluoride and toothpastes with active oxygen. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Patano, A.; Malcangi, G.; Sardano, R.; Mastrodonato, A.; Garofoli, G.; Mancini, A.; Inchingolo, A.D.; Di Venere, D.; Inchingolo, F.; Dipalma, G.; et al. White Spots: Prevention in Orthodontics—Systematic Review of the Literature. Int. J. Environ. Res. Public Health 2023, 20, 5608. https://doi.org/10.3390/ijerph20085608
Patano A, Malcangi G, Sardano R, Mastrodonato A, Garofoli G, Mancini A, Inchingolo AD, Di Venere D, Inchingolo F, Dipalma G, et al. White Spots: Prevention in Orthodontics—Systematic Review of the Literature. International Journal of Environmental Research and Public Health. 2023; 20(8):5608. https://doi.org/10.3390/ijerph20085608
Chicago/Turabian StylePatano, Assunta, Giuseppina Malcangi, Roberta Sardano, Antonio Mastrodonato, Grazia Garofoli, Antonio Mancini, Alessio Danilo Inchingolo, Daniela Di Venere, Francesco Inchingolo, Gianna Dipalma, and et al. 2023. "White Spots: Prevention in Orthodontics—Systematic Review of the Literature" International Journal of Environmental Research and Public Health 20, no. 8: 5608. https://doi.org/10.3390/ijerph20085608
APA StylePatano, A., Malcangi, G., Sardano, R., Mastrodonato, A., Garofoli, G., Mancini, A., Inchingolo, A. D., Di Venere, D., Inchingolo, F., Dipalma, G., & Inchingolo, A. M. (2023). White Spots: Prevention in Orthodontics—Systematic Review of the Literature. International Journal of Environmental Research and Public Health, 20(8), 5608. https://doi.org/10.3390/ijerph20085608