
The Impact of Air Pollution on Asthma Severity among Residents Living near the Main Industrial Complex in Oman: A Cross-Sectional Study
 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Study Population
2.2. Asthma Severity Assessment
2.3. Exposure Zones
2.4. Sample Size Determination
2.5. Data Collection
2.6. Statistical Analysis
2.7. Ethical Considerations
3. Results
3.1. Distribution of Asthma Severity among Omani Patients
3.2. Industrial Zones in Sohar and Severe Asthma
3.3. Industrial Areas and Prevalence of Severe Asthma
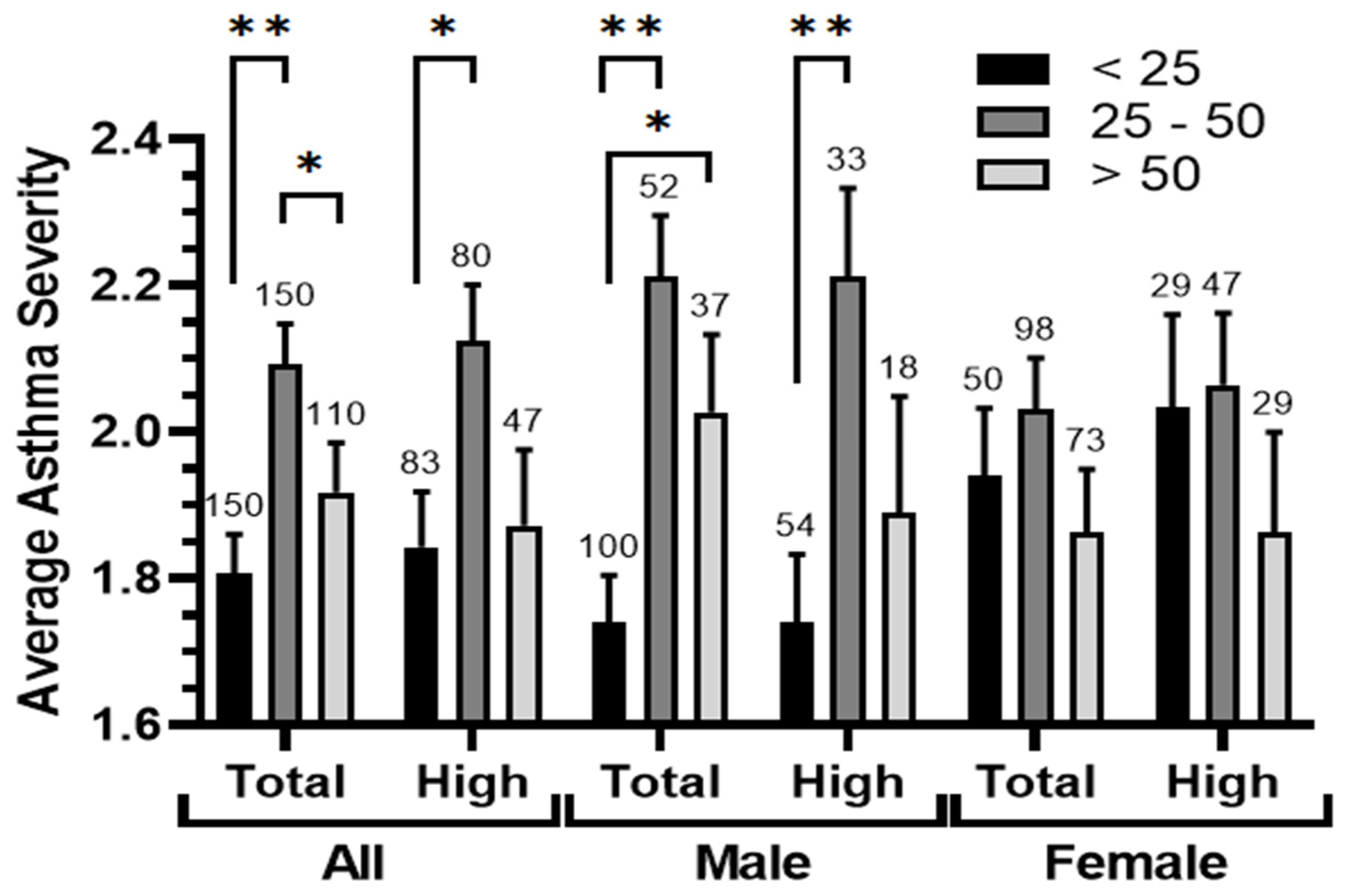
3.4. Age-Related Patterns in Asthma Severity
3.5. Asthma Severity and Smoking Status
3.6. Asthma Severity and Air Contaminants
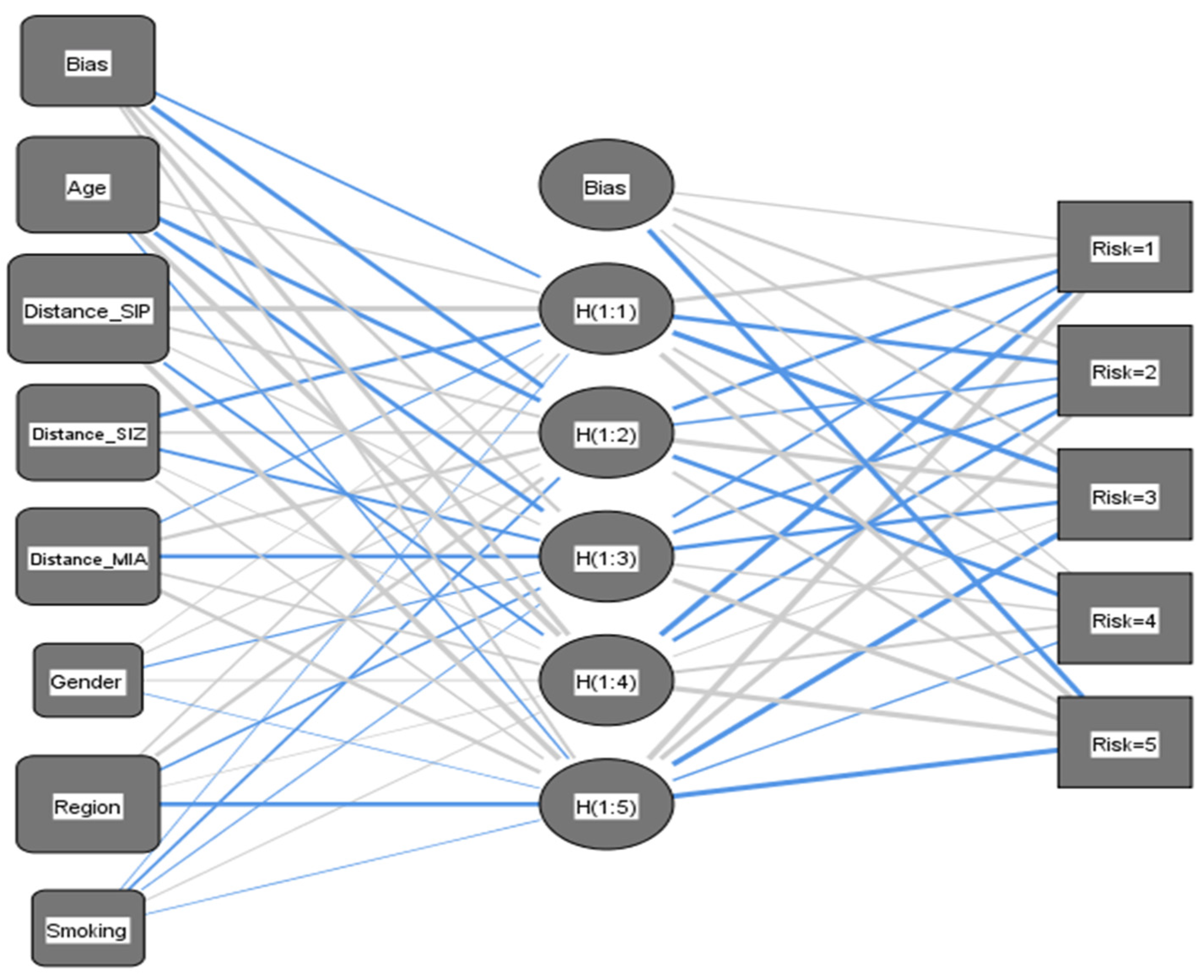
3.7. Predicting Asthma Risk Using Artificial Neural Networks
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Garcia, E.; Berhane, K.T.; Islam, T.; McConnell, R.; Urman, R.; Chen, Z.; Gilliland, F.D. Association of Changes in Air Quality with Incident Asthma in Children in California, 1993–2014. JAMA 2019, 321, 1906–1915. [Google Scholar] [CrossRef]
- Simkovich, S.M.; Goodman, D.; Roa, C.; Crocker, M.E.; Gianella, G.E.; Kirenga, B.J.; Wise, R.A.; Checkley, W. The health and social implications of household air pollution and respiratory diseases. NPJ Prim. Care Respir. Med. 2019, 29, 12. [Google Scholar] [CrossRef] [PubMed]
- Cheng, C.; Han, C.; Fang, Q.; Liu, Y.; Chi, X.; Li, X. Associations between air pollutants and hospital admissions for chronic obstructive pulmonary disease in Jinan: Potential benefits from air quality improvements. Environ. Sci. Pollut. Res. Int. 2023, 30, 46435–46445. [Google Scholar] [CrossRef] [PubMed]
- Anenberg, S.C.; Henze, D.K.; Tinney, V.; Kinney, P.L.; Raich, W.; Fann, N.; Malley, C.S.; Roman, H.; Lamsal, L.; Duncan, B.; et al. Estimates of the Global Burden of Ambient PM2.5, Ozone, and NO2 on Asthma Incidence and Emergency Room Visits. Environ. Health Perspect. 2018, 126, 107004. [Google Scholar] [CrossRef] [PubMed]
- D’Antona, S.; Castiglioni, I.; Porro, D.; Cava, C. Consequences of exposure to pollutants on respiratory health: From genetic correlations to causal relationships. PLoS ONE 2022, 17, e0277235. [Google Scholar] [CrossRef] [PubMed]
- Cohen, A.J.; Brauer, M.; Burnett, R.; Anderson, H.R.; Frostad, J.; Estep, K.; Balakrishnan, K.; Brunekreef, B.; Dandona, L.; Dandona, R.; et al. Estimates and 25-year trends of the global burden of disease attributable to ambient air pollution: An analysis of data from the Global Burden of Diseases Study 2015. Lancet 2017, 389, 1907–1918. [Google Scholar] [CrossRef] [PubMed]
- Thurston, G.D.; Balmes, J.R.; Garcia, E.; Gilliland, F.D.; Rice, M.B.; Schikowski, T.; Van Winkle, L.S.; Annesi-Maesano, I.; Burchard, E.G.; Carlsten, C.; et al. Outdoor Air Pollution and New-Onset Airway Disease. An Official American Thoracic Society Workshop Report. Ann. Am. Thorac. Soc. 2020, 17, 387–398. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.-K.; Lin, Y.-K.; Lin, C.-W.; Su, M.-W.; Chu, H.-W.; Wu, C.-D.; Zeng, Y.-T.; Chang, B.-L. Effects of long-term exposure to major outdoor air pollutants for the risk of chronic inflammatory airway diseases in adults with potential interaction detection in Taiwan Biobank. Atmos. Environ. 2022, 288, 119296. [Google Scholar] [CrossRef]
- Kim, D.; Chen, Z.; Zhou, L.-F.; Huang, S.-X. Air pollutants and early origins of respiratory diseases. Chronic Dis. Transl. Med. 2018, 4, 75–94. [Google Scholar] [CrossRef]
- Guarnieri, M.; Balmes, J.R. Outdoor air pollution and asthma. Lancet 2014, 383, 1581–1592. [Google Scholar] [CrossRef]
- Carr, T.F.; Bleecker, E. Asthma heterogeneity and severity. World Allergy Organ. J. 2016, 9, 41. [Google Scholar] [CrossRef] [PubMed]
- GBD 2016 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet 2017, 390, 1211–1259. [Google Scholar] [CrossRef] [PubMed]
- GBD 2015 Chronic Respiratory Disease Collaborators. Global, regional, and national deaths, prevalence, disability-adjusted life years, and years lived with disability for chronic obstructive pulmonary disease and asthma, 1990–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet Respir. Med. 2017, 5, 691–706. [Google Scholar] [CrossRef] [PubMed]
- Reddel, H.K.; Bateman, E.D.; Becker, A.; Boulet, L.-P.; Cruz, A.A.; Drazen, J.M.; Haahtela, T.; Hurd, S.S.; Inoue, H.; de Jongste, J.C.; et al. A summary of the new GINA strategy: A roadmap to asthma control. Eur. Respir. J. 2015, 46, 622–639. [Google Scholar] [CrossRef] [PubMed]
- Tarraf, H.; Aydin, O.; Mungan, D.; Albader, M.; Mahboub, B.; Doble, A.; Lahlou, A.; Tariq, L.; Aziz, F.; El Hasnaoui, A. Prevalence of asthma among the adult general population of five Middle Eastern countries: Results of the SNAPSHOT program. BMC Pulm. Med. 2018, 18, 68. [Google Scholar] [CrossRef] [PubMed]
- Al-Busaidi, N.; Soriano, J.B. Asthma Control in Oman: National Results within the Asthma Insights and Reality in the Gulf and the Near East (AIRGNE) Study. Sultan Qaboos Univ. Med. J. 2011, 11, 45–51. [Google Scholar] [PubMed]
- Al-Busaidi, N.; Habibulla, Z.; Bhatnagar, M.; Al-Lawati, N.; Al-Mahrouqi, Y. The burden of asthma in Oman. Sultan Qaboos Univ. Med. J. 2015, 15, e184-90. [Google Scholar]
- Al-Busaidi, N.H.; Habibullah, Z.; Soriano, J.B. The asthma cost in Oman. Sultan Qaboos Univ. Med. J. 2013, 13, 218–223. [Google Scholar] [CrossRef] [PubMed]
- Kauffmann, F.; Demenais, F. Gene-environment interactions in asthma and allergic diseases: Challenges and perspectives. J. Allergy Clin. Immunol. 2012, 130, 1229–1240. [Google Scholar] [CrossRef]
- Burbank, A.J.; Sood, A.K.; Kesic, M.J.; Peden, D.B.; Hernandez, M.L. Environmental determinants of allergy and asthma in early life. J. Allergy Clin. Immunol. 2017, 140, 1–12. [Google Scholar] [CrossRef]
- Hall, R.; Hall, I.P.; Sayers, I. Genetic risk factors for the development of pulmonary disease identified by genome-wide association. Respirology 2019, 24, 204–214. [Google Scholar] [CrossRef] [PubMed]
- Moheimani, F.; Hsu, A.C.-Y.; Reid, A.T.; Williams, T.; Kicic, A.; Stick, S.M.; Hansbro, P.M.; Wark, P.A.B.; Knight, D.A. The genetic and epigenetic landscapes of the epithelium in asthma. Respir. Res. 2016, 17, 119. [Google Scholar] [CrossRef] [PubMed]
- Zhang, T.; Huang, P.; Qiu, C. Progresses in epigenetic studies of asthma from the perspective of high-throughput analysis technologies: A narrative review. Ann. Transl. Med. 2022, 10, 493. [Google Scholar] [CrossRef] [PubMed]
- Salvi, S.; Limaye, S. Effects of air pollution on allergy and asthma. In Textbook of Allergy for the Clinician, 2nd ed.; Vedanthan, P.K., Nelson, H.S., Agashe, S.N., Mahesh, P.A., Katial, R., Eds.; CRC Press: Boca Raton, FL, USA, 2021; pp. 219–230. ISBN 9780367854706. [Google Scholar]
- Platts-Mills, T.A.; Commins, S.P. Increasing Prevalence of Asthma and Allergic Rhinitis and the Role of Environmental Factors. UpToDate. 2016. Available online: https://medilib.ir/uptodate/show/5548 (accessed on 1 March 2024).
- Lin, W.; Brunekreef, B.; Gehring, U. Meta-analysis of the effects of indoor nitrogen dioxide and gas cooking on asthma and wheeze in children. Int. J. Epidemiol. 2013, 42, 1724–1737. [Google Scholar] [CrossRef] [PubMed]
- Delfino, R.J.; Wu, J.; Tjoa, T.; Gullesserian, S.K.; Nickerson, B.; Gillen, D.L. Asthma morbidity and ambient air pollution: Effect modification by residential traffic-related air pollution. Epidemiology 2014, 25, 48–57. [Google Scholar] [CrossRef] [PubMed]
- Bowatte, G.; Lodge, C.; Lowe, A.J.; Erbas, B.; Perret, J.; Abramson, M.J.; Matheson, M.; Dharmage, S.C. The influence of childhood traffic-related air pollution exposure on asthma, allergy and sensitization: A systematic review and a meta-analysis of birth cohort studies. Allergy 2015, 70, 245–256. [Google Scholar] [CrossRef] [PubMed]
- Khreis, H.; Kelly, C.; Tate, J.; Parslow, R.; Lucas, K.; Nieuwenhuijsen, M. Exposure to traffic-related air pollution and risk of development of childhood asthma: A systematic review and meta-analysis. Environ. Int. 2017, 100, 1–31. [Google Scholar] [CrossRef]
- Jung, C.-R.; Chen, W.-T.; Tang, Y.-H.; Hwang, B.-F. Fine particulate matter exposure during pregnancy and infancy and incident asthma. J. Allergy Clin. Immunol. 2019, 143, 2254–2262.e5. [Google Scholar] [CrossRef] [PubMed]
- Toskala, E.; Kennedy, D.W. Asthma risk factors. Int. Forum Allergy Rhinol. 2015, 5 (Suppl. S1), S11–S16. [Google Scholar] [CrossRef]
- Feng, M.; Yang, Z.; Pan, L.; Lai, X.; Xian, M.; Huang, X.; Chen, Y.; Schröder, P.C.; Roponen, M.; Schaub, B.; et al. Associations of early life exposures and environmental factors with asthma among children in rural and urban areas of Guangdong, China. Chest 2016, 149, 1030–1041. [Google Scholar] [CrossRef]
- Soto-Martínez, M.E.; Soto-Quiros, M.E.; Custovic, A. Childhood Asthma: Low and Middle-Income Countries Perspective. Acta Med. Acad. 2020, 49, 181–190. [Google Scholar] [CrossRef] [PubMed]
- GBD 2019 Universal Health Coverage Collaborators. Measuring universal health coverage based on an index of effective coverage of health services in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1250–1284. [Google Scholar] [CrossRef] [PubMed]
- Zeitouni, M.O.; Al-Moamary, M.S.; Coussa, M.L.; Riachy, M.; Mahboub, B.; AlHuraish, F.; Zidan, M.H.; Metwally, M.M.; Aksu, K.; Yavuz, E.; et al. Challenges and recommendations for the management of asthma in the Middle East and Africa. Ann. Thorac. Med. 2022, 17, 71–80. [Google Scholar] [CrossRef] [PubMed]
- Farahat, A. Air quality in the Gulf Cooperation Council (GCC) countries. In Asian Atmospheric Pollution; Elsevier: Amsterdam, The Netherlands, 2022; pp. 201–226. ISBN 9780128166932. [Google Scholar]
- Yousif, J.; Alattar, N.; Fekihal, M. Forecasting Models Based CO2 Emission for Sultanate of Oman. Int. J. Appl. Eng. Res. 2012, 12, 95–100. [Google Scholar]
- Al-Wahaibi, A.; Zeka, A. Health impacts from living near a major industrial park in Oman. BMC Public Health 2015, 15, 524. [Google Scholar] [CrossRef] [PubMed]
- Baawain, M.S.; Al-Serihi, A.S. Systematic Approach for the Prediction of Ground-Level Air Pollution (around an Industrial Port) Using an Artificial Neural Network. Aerosol Air Qual. Res. 2014, 14, 124–134. [Google Scholar] [CrossRef]
- GINA Global Initiative for Asthma—GINA. Available online: https://ginasthma.org/gina-reports/ (accessed on 1 January 2022).
- To, T.; Zhu, J.; Villeneuve, P.J.; Simatovic, J.; Feldman, L.; Gao, C.; Williams, D.; Chen, H.; Weichenthal, S.; Wall, C.; et al. Chronic disease prevalence in women and air pollution—A 30-year longitudinal cohort study. Environ. Int. 2015, 80, 26–32. [Google Scholar] [CrossRef] [PubMed]
- Henderson, S.B.; Beckerman, B.; Jerrett, M.; Brauer, M. Application of land use regression to estimate long-term concentrations of traffic-related nitrogen oxides and fine particulate matter. Environ. Sci. Technol. 2007, 41, 2422–2428. [Google Scholar] [CrossRef]
- Zhang, Y.; Ni, H.; Bai, L.; Cheng, Q.; Zhang, H.; Wang, S.; Xie, M.; Zhao, D.; Su, H. The short-term association between air pollution and childhood asthma hospital admissions in urban areas of Hefei City in China: A time-series study. Environ. Res. 2019, 169, 510–516. [Google Scholar] [CrossRef]
- Hinton, G.E.; Salakhutdinov, R.R. Reducing the dimensionality of data with neural networks. Science 2006, 313, 504–507. [Google Scholar] [CrossRef]
- Nielsen, G.D.; Larsen, S.T.; Wolkoff, P. Recent trend in risk assessment of formaldehyde exposures from indoor air. Arch. Toxicol. 2013, 87, 73–98. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.Y.; Chiu, J.F.; Cheng, M.F.; Lin, M.C. Effects of indoor environmental factors on respiratory health of children in a subtropical climate. Environ. Res. 1997, 75, 49–55. [Google Scholar] [CrossRef] [PubMed]
- Mock, K.; Palma, A.M.; Wu, J.; Billimek, J.; Lu, K.D. Breathing room: Industrial zoning and asthma incidence using school district health records in the city of Santa Ana, California. Int. J. Environ. Res. Public Health 2022, 19, 4820. [Google Scholar] [CrossRef] [PubMed]
- Lwebuga-Mukasa, J.S.; Oyana, T.J.; Wydro, P. Risk factors for asthma prevalence and chronic respiratory illnesses among residents of different neighbourhoods in Buffalo, New York. J. Epidemiol. Community Health 2004, 58, 951–957. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; Cho, J.; Wen, F.; Choi, S. The built environment and asthma: Los Angeles case study. J. Public Health 2023, 31, 57–64. [Google Scholar] [CrossRef]
- Orellano, P.; Quaranta, N.; Reynoso, J.; Balbi, B.; Vasquez, J. Effect of outdoor air pollution on asthma exacerbations in children and adults: Systematic review and multilevel meta-analysis. PLoS ONE 2017, 12, e0174050. [Google Scholar] [CrossRef] [PubMed]
- Jin, Y.; Andersson, H.; Zhang, S. Air pollution control policies in China: A retrospective and prospects. Int. J. Environ. Res. Public Health 2016, 13, 1219. [Google Scholar] [CrossRef] [PubMed]
- Cesaroni, G.; Forastiere, F.; Stafoggia, M.; Andersen, Z.J.; Badaloni, C.; Beelen, R.; Caracciolo, B.; de Faire, U.; Erbel, R.; Eriksen, K.T.; et al. Long term exposure to ambient air pollution and incidence of acute coronary events: Prospective cohort study and meta-analysis in 11 European cohorts from the ESCAPE Project. BMJ 2014, 348, f7412. [Google Scholar] [CrossRef]
- Raaschou-Nielsen, O.; Vineis, P.; Brunekreef, B.; Nieuwenhuijsen, M.; Hoffmann, B.; Forastiere, F.; Oudin, A.; Hoek, G.; Katsouyanni, K.; Schwarze, P.; et al. Air pollution and lung cancer in Europe—Authors’ reply. Lancet Oncol. 2013, 14, e440. [Google Scholar] [CrossRef]
- Al-Rawas, O.A.; Al-Maniri, A.A.; Al-Riyami, B.M. Home exposure to Arabian incense (bakhour) and asthma symptoms in children: A community survey in two regions in Oman. BMC Pulm. Med. 2009, 9, 23. [Google Scholar] [CrossRef]
- Khreis, H.; Cirach, M.; Mueller, N.; de Hoogh, K.; Hoek, G.; Nieuwenhuijsen, M.J.; Rojas-Rueda, D. Outdoor air pollution and the burden of childhood asthma across Europe. Eur. Respir. J. 2019, 54, 1802194. [Google Scholar] [CrossRef] [PubMed]
- Pierangeli, I.; Nieuwenhuijsen, M.J.; Cirach, M.; Rojas-Rueda, D. Health equity and burden of childhood asthma-related to air pollution in Barcelona. Environ. Res. 2020, 186, 109067. [Google Scholar] [CrossRef] [PubMed]
- Gehring, U.; Wijga, A.H.; Koppelman, G.H.; Vonk, J.M.; Smit, H.A.; Brunekreef, B. Air pollution and the development of asthma from birth until young adulthood. Eur. Respir. J. 2020, 56, 2000147. [Google Scholar] [CrossRef] [PubMed]
- Tiotiu, A.I.; Novakova, P.; Nedeva, D.; Chong-Neto, H.J.; Novakova, S.; Steiropoulos, P.; Kowal, K. Impact of air pollution on asthma outcomes. Int. J. Environ. Res. Public Health 2020, 17, 6212. [Google Scholar] [CrossRef] [PubMed]
- Balmes, J.R.; Cisternas, M.; Quinlan, P.J.; Trupin, L.; Lurmann, F.W.; Katz, P.P.; Blanc, P.D. Annual average ambient particulate matter exposure estimates, measured home particulate matter, and hair nicotine are associated with respiratory outcomes in adults with asthma. Environ. Res. 2014, 129, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Moscato, G.; Apfelbacher, C.; Brockow, K.; Eberle, C.; Genuneit, J.; Mortz, C.G.; Quecchia, C.; Quirce, S.; Siracusa, A.; Tarlo, S.M.; et al. Gender and occupational allergy: Report from the task force of the EAACI Environmental and Occupational Allergy Interest Group. Allergy 2020, 75, 2753–2763. [Google Scholar] [CrossRef] [PubMed]
- Kogevinas, M.; Zock, J.-P.; Jarvis, D.; Kromhout, H.; Lillienberg, L.; Plana, E.; Radon, K.; Torén, K.; Alliksoo, A.; Benke, G.; et al. Exposure to substances in the workplace and new-onset asthma: An international prospective population-based study (ECRHS-II). Lancet 2007, 370, 336–341. [Google Scholar] [CrossRef]
- Fuseini, H.; Newcomb, D.C. Mechanisms driving gender differences in asthma. Curr. Allergy Asthma Rep. 2017, 17, 19. [Google Scholar] [CrossRef] [PubMed]
- Sit, G.; Letellier, N.; Iwatsubo, Y.; Goldberg, M.; Leynaert, B.; Nadif, R.; Ribet, C.; Roche, N.; Roquelaure, Y.; Varraso, R.; et al. Occupational exposures to organic solvents and asthma symptoms in the CONSTANCES cohort. Int. J. Environ. Res. Public Health 2021, 18, 9258. [Google Scholar] [CrossRef]
- Ilmarinen, P.; Tuomisto, L.E.; Kankaanranta, H. Phenotypes, Risk Factors, and Mechanisms of Adult-Onset Asthma. Mediat. Inflamm. 2015, 2015, 514868. [Google Scholar] [CrossRef]
- Golden, R. Identifying an indoor air exposure limit for formaldehyde considering both irritation and cancer hazards. Crit. Rev. Toxicol. 2011, 41, 672–721. [Google Scholar] [CrossRef] [PubMed]
- Kan, H.; London, S.J.; Chen, G.; Zhang, Y.; Song, G.; Zhao, N.; Jiang, L.; Chen, B. Season, sex, age, and education as modifiers of the effects of outdoor air pollution on daily mortality in Shanghai, China: The Public Health and Air Pollution in Asia (PAPA) Study. Environ. Health Perspect. 2008, 116, 1183–1188. [Google Scholar] [CrossRef] [PubMed]
- Katanoda, K.; Sobue, T.; Satoh, H.; Tajima, K.; Suzuki, T.; Nakatsuka, H.; Takezaki, T.; Nakayama, T.; Nitta, H.; Tanabe, K.; et al. An association between long-term exposure to ambient air pollution and mortality from lung cancer and respiratory diseases in Japan. J. Epidemiol. 2011, 21, 132–143. [Google Scholar] [CrossRef]
- Beelen, R.; Hoek, G.; van den Brandt, P.A.; Goldbohm, R.A.; Fischer, P.; Schouten, L.J.; Jerrett, M.; Hughes, E.; Armstrong, B.; Brunekreef, B. Long-term effects of traffic-related air pollution on mortality in a Dutch cohort (NLCS-AIR study). Environ. Health Perspect. 2008, 116, 196–202. [Google Scholar] [CrossRef]
- Miller, K.A.; Siscovick, D.S.; Sheppard, L.; Shepherd, K.; Sullivan, J.H.; Anderson, G.L.; Kaufman, J.D. Long-term exposure to air pollution and incidence of cardiovascular events in women. N. Engl. J. Med. 2007, 356, 447–458. [Google Scholar] [CrossRef]
- Chambers, L.; Finch, J.; Edwards, K.; Jeanjean, A.; Leigh, R.; Gonem, S. Effects of personal air pollution exposure on asthma symptoms, lung function and airway inflammation. Clin. Exp. Allergy 2018, 48, 798–805. [Google Scholar] [CrossRef]
- Young, M.T.; Sandler, D.P.; DeRoo, L.A.; Vedal, S.; Kaufman, J.D.; London, S.J. Ambient air pollution exposure and incident adult asthma in a nationwide cohort of U.S. women. Am. J. Respir. Crit. Care Med. 2014, 190, 914–921. [Google Scholar] [CrossRef] [PubMed]
- Becklake, M.R.; Kauffmann, F. Gender differences in airway behaviour over the human life span. Thorax 1999, 54, 1119–1138. [Google Scholar] [CrossRef] [PubMed]
- Kim, C.S.; Hu, S.C. Regional deposition of inhaled particles in human lungs: Comparison between men and women. J. Appl. Physiol. 1998, 84, 1834–1844. [Google Scholar] [CrossRef]
- Kohlhäufl, M.; Brand, P.; Scheuch, G.; Meyer, T.S.; Schulz, H.; Häussinger, K.; Heyder, J. Increased fine particle deposition in women with asymptomatic nonspecific airway hyperresponsiveness. Am. J. Respir. Crit. Care Med. 1999, 159, 902–906. [Google Scholar] [CrossRef]
- Tan, D.J.; Walters, E.H.; Perret, J.L.; Burgess, J.A.; Johns, D.P.; Lowe, A.J.; Lodge, C.J.; Hayati Rezvan, P.; Simpson, J.A.; Morrison, S.; et al. Clinical and functional differences between early-onset and late-onset adult asthma: A population-based Tasmanian Longitudinal Health Study. Thorax 2016, 71, 981–987. [Google Scholar] [CrossRef] [PubMed]
- Bowatte, G.; Erbas, B.; Lodge, C.J.; Knibbs, L.D.; Gurrin, L.C.; Marks, G.B.; Thomas, P.S.; Johns, D.P.; Giles, G.G.; Hui, J.; et al. Traffic-related air pollution exposure over a 5-year period is associated with increased risk of asthma and poor lung function in middle age. Eur. Respir. J. 2017, 50, 1602357. [Google Scholar] [CrossRef]
- Rönmark, E.; Lindberg, A.; Watson, L.; Lundbäck, B. Outcome and severity of adult onset asthma—Report from the obstructive lung disease in northern Sweden studies (OLIN). Respir. Med. 2007, 101, 2370–2377. [Google Scholar] [CrossRef] [PubMed]
- Bronnimann, S.; Burrows, B. A prospective study of the natural history of asthma. Remission and relapse rates. Chest 1986, 90, 480–484. [Google Scholar] [CrossRef]
- Maestrelli, P. Natural History of Adult-Onset Asthma. Am. J. Respir. Crit. Care Med. 2004, 169, 331–332. [Google Scholar] [CrossRef]
- Settipane, G.A.; Greisner, W.A.; Settipane, R.J. Natural history of asthma: A 23-year followup of college students. Ann. Allergy Asthma Immunol. 2000, 84, 499–503. [Google Scholar] [CrossRef]
- Bauer, B.A.; Reed, C.E.; Yunginger, J.W.; Wollan, P.C.; Silverstein, M.D. Incidence and outcomes of asthma in the elderly. A population-based study in Rochester, Minnesota. Chest 1997, 111, 303–310. [Google Scholar] [CrossRef] [PubMed]
- Reed, C.E. The natural history of asthma in adults: The problem of irreversibility. J. Allergy Clin. Immunol. 1999, 103, 539–547. [Google Scholar] [CrossRef]
- Masoli, M.; Fabian, D.; Holt, S.; Beasley, R. Global Initiative for Asthma (GINA) Program The global burden of asthma: Executive summary of the GINA Dissemination Committee report. Allergy 2004, 59, 469–478. [Google Scholar] [CrossRef]
- Cook, Q.; Argenio, K.; Lovinsky-Desir, S. The impact of environmental injustice and social determinants of health on the role of air pollution in asthma and allergic disease in the United States. J. Allergy Clin. Immunol. 2021, 148, 1089–1101.e5. [Google Scholar] [CrossRef]
- Bronte-Moreno, O.; González-Barcala, F.-J.; Muñoz-Gall, X.; Pueyo-Bastida, A.; Ramos-González, J.; Urrutia-Landa, I. Impact of air pollution on asthma: A scoping review. Open Respir. Arch. 2023, 5, 100229. [Google Scholar] [CrossRef] [PubMed]
- Fiter, R.J.; Murphy, L.J.; Gong, M.N.; Cleven, K.L. The impact of air pollution on asthma: Clinical outcomes, current epidemiology, and health disparities. Expert Rev. Respir. Med. 2023, 17, 1237–1247. [Google Scholar] [CrossRef] [PubMed]
- Feng, Y.; Wang, Y.; Zeng, C.; Mao, H. Artificial intelligence and machine learning in chronic airway diseases: Focus on asthma and chronic obstructive pulmonary disease. Int. J. Med. Sci. 2021, 18, 2871–2889. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Huang, S.; Jiao, A.; Yang, X.; Yun, J.; Wang, Y.; Xue, X.; Chu, Y.; Liu, F.; Liu, Y.; et al. Association between ambient fine particulate matter and preterm birth or term low birth weight: An updated systematic review and meta-analysis. Environ. Pollut. 2017, 227, 596–605. [Google Scholar] [CrossRef]
- Ho, W.-C.; Hartley, W.R.; Myers, L.; Lin, M.-H.; Lin, Y.-S.; Lien, C.-H.; Lin, R.-S. Air pollution, weather, and associated risk factors related to asthma prevalence and attack rate. Environ. Res. 2007, 104, 402–409. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Exposure Zone | Total | Severe | Moderate | Mild | |
|---|---|---|---|---|---|
| (Exposure Zones %) | Case Number (Asthma Severity %–Exposure Zones %) | ||||
| All | High (<6 km) | 210 (51.2%) | 56 (26.7%–51.9%) | 107 (51%–49.1%) | 47 (22.4%–56%) |
| Middle (6–12 km) | 146 (35.6%) | 38 (26%–35.2%) | 76 (52.1%–34.9%) | 32 (21.9%–38.1%) | |
| Low (>12 km) | 54 (13.2%) | 14 (25.9%–13%) | 35 (64.8%–16.1%) | 5 (9.3%–6%) | |
| Male | High (<6 km) | 105 (55.6%) | 31 (29.5%–63.3%) | 52 (49.5%–49.5%) | 22 (21%–62.9%) |
| Middle (6–12 km) | 61 (32.3%) | 14 (23%–28.6%) | 35 (57.4%–33.3%) | 12 (19.7%–34.3%) | |
| Low (>12 km) | 23 (12.2%) | 4 (17.4%–8.2%) | 18 (78.3%–17.1%) | 1 (4.3%–2.9%) | |
| Female | High (<6 km) | 105 (47.5%) | 25 (23.8%–42.4%) | 55 (52.4%-48.7%) | 25 (23.8%–51%) |
| Middle (6–12 km) | 85 (38.5%) | 24 (28.2%–40.7%) | 41 (48.2%–36.3%) | 20 (23.5%–40.8%) | |
| Low (>12 km) | 31 (14%) | 10 (32.3%–16.9%) | 17 (54.8%–15%) | 4 (12.9%–8.2%) | |
| Valid Samples | High | Low | Severe Asthma (High/Low) | Moderate and Mild Asthma (High/Low) | RR (CI95%) | X2 | |
|---|---|---|---|---|---|---|---|
| SIP | 264 | <6 km | >12 km | 47/5 | 163/49 | 2.42 (1.01–5.78) | 0.031 * |
| SIZ | 264 | <10 km | >20 km | 40/11 | 122/64 | 1.68 (0.92–3.09) | 0.081 |
| MIA | 176 | <6 km | >12 km | 27/11 | 72/66 | 1.91 (1.01–3.6) | 0.038 * |
| CA | 323 | <8 km | >12 km | 25/41 | 118/139 | 0.77 (0.49–1.2) | 0.241 |
| SIP—North | 223 | Middle | North | 23/20 | 82/98 | 1.29 (0.75–2.21) | 0.349 |
| SIP—South | 269 | Middle | South | 23/40 | 82/124 | 0.9 (0.57–1.41) | 0.639 |
| Distance from SIP (km) | Distance from SIZ (km) | Distance from MIA (km) | Total N | Severe Asthma N | Moderate and Mild Asthma N | Severe Asthma % | Latitude | Longitude | RR (CI95%) | χ2 | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Ghadhfan | 2.6 | 11.3 | 5.3 | 30 | 8 | 22 | 27% | 24.471 | 56.602 | 2.88 (1.03–8.02) | 0.035 * |
| Al Hadd | 3.4 | 13.8 | 6.2 | 21 | 5 | 16 | 24% | 24.487 | 56.585 | 2.57 (0.83–7.98) | 0.10 |
| Liwa | 4.0 | 16.0 | 8.8 | 22 | 5 | 17 | 23% | 24.512 | 56.586 | 2.45 (0.79–7.65) | 0.12 |
| Harmul | 4.1 | 16.7 | 10.3 | 21 | 5 | 16 | 24% | 24.523 | 56.596 | 2.57 (0.83–7.98) | 0.10 |
| Al Khuwayriyyah | 4.7 | 8.0 | 6.1 | 12 | 2 | 10 | 17% | 24.449 | 56.626 | 1.8 (0.4–8.2) | 0.45 |
| Al Eqdah | 5.1 | 15.7 | 7.2 | 13 | 3 | 10 | 23% | 24.498 | 56.569 | 2.49 (0.68–9.12) | 0.17 |
| Mikhaylif | 5.1 | 16.5 | 8.4 | 19 | 2 | 17 | 11% | 24.508 | 56.572 | 1.14 (0.24–5.38) | 0.87 |
| Majees | 6.0 | 8.2 | 9.6 | 72 | 17 | 55 | 24% | 24.455 | 56.657 | 2.55 (1–6.48) | 0.036 * |
| Harat Ash Shaykh | 6.1 | 6.8 | 7.6 | 8 | 2 | 6 | 25% | 24.442 | 56.641 | 2.7 (0.63–11.65) | 0.19 |
| Falaj Al Qabail | 6.4 | 6.4 | 5.9 | 69 | 19 | 50 | 28% | 24.433 | 56.626 | 2.97 (1.19–7.45) | 0.011 * |
| Az Zahiyah | 7.7 | 19.7 | 11.5 | 40 | 5 | 35 | 13% | 24.537 | 56.563 | 1.35 (0.42–4.35) | 0.61 |
| Nabr | 10.1 | 22.5 | 14.5 | 20 | 5 | 15 | 25% | 24.563 | 56.559 | 2.7 (0.87–8.35) | 0.08 |
| Rumelah | 10.7 | 23.1 | 15.4 | 7 | 1 | 6 | 14% | 24.572 | 56.563 | 1.54 (0.21–11.37) | 0.67 |
| Control | 19.0 | 26.0 | 18.8 | 54 | 5 | 49 | 9% | 24.505 | 56.499 | - | - |
| Exposure Zone | Age Range | Total | Severe | Moderate | Mild | All | Male | Female | |||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Age Ranges (%) | Case Number (Asthma Severity %–Age Range %) | RR (CI95%) | χ2 | RR (CI95%) | χ2 | RR (CI95%) | χ2 | ||||
| Total | <25 | 150 (36.6%) | 20 (13.3%–23.8%) | 81 (54%–37.2%) | 49 (32.7%–45.4%) | - | - | - | - | - | - |
| 25–50 | 150 (36.6%) | 41 (27.3%–48.8%) | 82 (54.7%–37.6%) | 27 (18%–25%) | 2.05 (1.26–3.33) | 0.003 * | 2.8 (1.4–5.58) | 0.002 * | 1.417 (0.72–2.80) | 0.304 | |
| >50 | 110 (26.8%) | 23 (20.9%–27.4%) | 55 (50%–25.2%) | 32 (29.1%–29.6%) | 1.57 (0.91–2.71) | 0.104 | 1.97 (0.86–4.5) | 0.11 | 1.14 (0.54–2.4) | 0.727 | |
| High <6 km from SIP | <25 | 83 (39.5%) | 14 (16.9%–29.8%) | 42 (50.6%–39.3%) | 27 (32.5%–48.2%) | - | - | - | - | - | - |
| 25–50 | 80 (38.1%) | 24 (30%–51.1%) | 42 (52.5%–39.3%) | 14 (17.5%–25%) | 1.78 (0.99–3.19) | 0.047 * | 2.81 (1.23–6.4) | 0.1 | 1.058 (0.47–2.38) | 0.892 | |
| >50 | 47 (22.4%) | 9 (19.1%–19.1%) | 23 (48.9%–21.5%) | 15 (31.9%–26.8%) | 1.14 (0.53–2.42) | 0.743 | 1.286 (0.37–4.46) | 0.694 | 0.857 (0.33–2.24) | 0.753 | |
| Exposure Zone | Smoking State | All | Male/Female | Severe * | Moderate * | Mild * | Severe/Mild | Severe/Comb ** | ||
|---|---|---|---|---|---|---|---|---|---|---|
| (Smoking Groups %) | Case Number (Asthma Severity %–Smoking Groups %) | RR (CI 95%) | χ2 | RR (CI 95%) | χ2 | |||||
| Total | Non- Smoker | 347 (84.6%) | 155/192 (82.0%–86.9%) | 71 (20.5%–84.5%) | 178 (51.3%–81.6%) | 98 (28.2%–90.7%) | - | - | - | - |
| Smoker | 22 (5.4%) | 19/3 (10.1%–1.4%) | 5 (22.7%–5.9%) | 15 (68.2%–6.9%) | 2 (9.1%–1.8%) | 1.7 (1.03–2.81) | 0.12 | 1.11 (0.5–2.47) | 0.80 | |
| Passive Smoker | 41 (10%) | 15/26 (7.9%–11.8%) | 8 (19.5%–9.5%) | 25 (61%–11.5%) | 8 (19.5%–7.4%) | 1.19 (0.71–2) | 0.54 | 0.95 (0.5–1.84) | 0.89 | |
| High <6 km from SIP | Non- Smoker | 179 (85.2%) | 89/90 (84.8%–85.7%) | 43 (24%–91.5%) | 85 (47.5%–79.4%) | 51 (28.5%–91.1%) | - | - | - | - |
| Smoker | 9 (4.3%) | 8/1 (7.6%–1.0%) | 1 (11.1%–2.1%) | 7 (77.8%–6.5%) | 1 (11.1%–1.8%) | 1.09 (0.27–4.45) | 0.90 | 0.46 (0.07–2.99) | 0.37 | |
| Passive Smoker | 22 (10.5%) | 8/14 (7.6%–13.3%) | 3 (13.6%–6.4%) | 15 (68.2%–14%) | 4 (18.2%–7.1%) | 0.94 (0.39–2.27) | 0.88 | 0.57 (0.19–1.68) | 0.27 | |
| Contaminants | Respondent N | Respondent % | Responses % | Severe Asthma % | Severe Asthma Y/N | Comb Asthma Y/N | Total | High (<6 km) | ||
|---|---|---|---|---|---|---|---|---|---|---|
| RR (CI95%) | χ2 | RR (CI95%) | χ2 | |||||||
| Yes | 281 | 68.5% | - | 19.2% | 54 | 227 | 0.83 (0.56–1.23) | 0.347 | 0.76 (0.45–1.28) | 0.303 |
| Uncertain | 129 | 31.5% | - | 23.3% | 30 | 99 | - | - | - | - |
| Dust | 186 | 67.9% | 27.7% | 22.6% | 42/42 | 144/182 | 1.2 (0.82–1.76) | 0.339 | 1.02 (0.61–1.69) | 0.951 |
| Incense | 224 | 81.8% | 33.4% | 20.1% | 45/39 | 179/147 | 0.96 (0.65–1.4) | 0.826 | 1 (0.6–1.67) | 0.99 |
| Perfume | 180 | 65.7% | 26.8% | 21.7% | 39/45 | 141/185 | 1.11 (0.76–1.62) | 0.601 | 1.21 (0.73–2.01) | 0.457 |
| Smoke | 81 | 29.6% | 12.1% | 24.7% | 20/64 | 61/265 | 1.27 (0.82–1.97) | 0.295 | 1.41 (0.81–2.47) | 0.238 |
| Total Respondents | 274 | 100.0% | - | 19.3% | 53 | 221 | - | - | - | - |
| Total Responses | 671 | - | 100.0% | 21.8% | 146 | 525 | - | - | - | - |
| Predicted | |||||||
|---|---|---|---|---|---|---|---|
| Very Low Risk | Low Risk | Average Risk | High Risk | Very High Risk | Percent Correct | ||
| Training | Very Low Risk | 47 | 1 | 0 | 0 | 0 | 97.9% |
| Low Risk | 1 | 59 | 4 | 0 | 0 | 92.2% | |
| Average Risk | 0 | 1 | 53 | 1 | 3 | 91.4% | |
| High Risk | 0 | 0 | 0 | 57 | 2 | 96.6% | |
| Very High Risk | 0 | 0 | 1 | 1 | 55 | 96.5% | |
| Overall Percent | 16.8% | 21.3% | 20.3% | 20.6% | 21.0% | 94.8% | |
| Testing | Very Low Risk | 29 | 0 | 0 | 0 | 0 | 100.0% |
| Low Risk | 1 | 24 | 1 | 1 | 1 | 88.9% | |
| Average Risk | 0 | 0 | 17 | 2 | 3 | 77.3% | |
| High Risk | 0 | 0 | 1 | 18 | 2 | 85.7% | |
| Very High Risk | 17.7 | 0 | 0 | 1 | 24 | 96.0% | |
| Overall Percent | 23.4% | 19.4% | 15.3% | 17.7% | 24.2% | 90.3% | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al Okla, S.M.; Al Rasbi, F.A.Z.K.; Al Marhubi, H.S.; Al Mataani, S.S.; Al Sawai, Y.M.; Mohammed, H.I.; Al Mamari, M.A.S.; Al Balushi, S.A.A.; Abbady, A.Q. The Impact of Air Pollution on Asthma Severity among Residents Living near the Main Industrial Complex in Oman: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2024, 21, 553. https://doi.org/10.3390/ijerph21050553
Al Okla SM, Al Rasbi FAZK, Al Marhubi HS, Al Mataani SS, Al Sawai YM, Mohammed HI, Al Mamari MAS, Al Balushi SAA, Abbady AQ. The Impact of Air Pollution on Asthma Severity among Residents Living near the Main Industrial Complex in Oman: A Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2024; 21(5):553. https://doi.org/10.3390/ijerph21050553
Chicago/Turabian StyleAl Okla, Souad Mahmoud, Fatima Al Zahra Khamis Al Rasbi, Hawida Said Al Marhubi, Shima Salim Al Mataani, Yusra Mohammed Al Sawai, Hasa Ibrahim Mohammed, Muna Ali Salim Al Mamari, Salwa Abdullah Abdulrahim Al Balushi, and Abdul Qader Abbady. 2024. "The Impact of Air Pollution on Asthma Severity among Residents Living near the Main Industrial Complex in Oman: A Cross-Sectional Study" International Journal of Environmental Research and Public Health 21, no. 5: 553. https://doi.org/10.3390/ijerph21050553
APA StyleAl Okla, S. M., Al Rasbi, F. A. Z. K., Al Marhubi, H. S., Al Mataani, S. S., Al Sawai, Y. M., Mohammed, H. I., Al Mamari, M. A. S., Al Balushi, S. A. A., & Abbady, A. Q. (2024). The Impact of Air Pollution on Asthma Severity among Residents Living near the Main Industrial Complex in Oman: A Cross-Sectional Study. International Journal of Environmental Research and Public Health, 21(5), 553. https://doi.org/10.3390/ijerph21050553