1. Introduction
Alarming and relatively recent increases in childhood obesity [
1–
3] have fueled public health action in British Columbia (BC), Canada and globally [
3]. It is well accepted that the current environment predisposes both children and adults to sedentary lifestyles and over consumption of energy dense foods of low nutritious value [
3–
5]. An obesogenic environment has been defined as a place where the influence of the surroundings and social context combine to promote obesity in populations or individuals [
6]. Unfortunately, the potential health and social consequences of the development of obesogenic environments are far reaching [
3,
7].
There is growing recognition in the public health sector that solutions to childhood obesity should be more ecological in nature; recognizing the interplay between individuals and multiple environments and levels of influence from friends and family, to community and provincial policy [
3,
8–
10]. Recent obesity prevention recommendations identify public service venues, including recreation facilities, as environments in which to increase access to healthy food options [
11].
In British Columbia (BC), Canada, for instance, approximately fifty million visits to recreation facilities occur annually [
12]. This is the equivalent of thirteen visits per British Columbian per year. Many of the benefits of recreation facilities cited by users and non-users alike are the activities for children, youth and families and evidence shows that children are spending more time in structured activities (e.g., sports and arts) or daycare than in previous years [
13]. As such, recreation facilities have become a potential environment/setting of influence on children’s health behaviour [
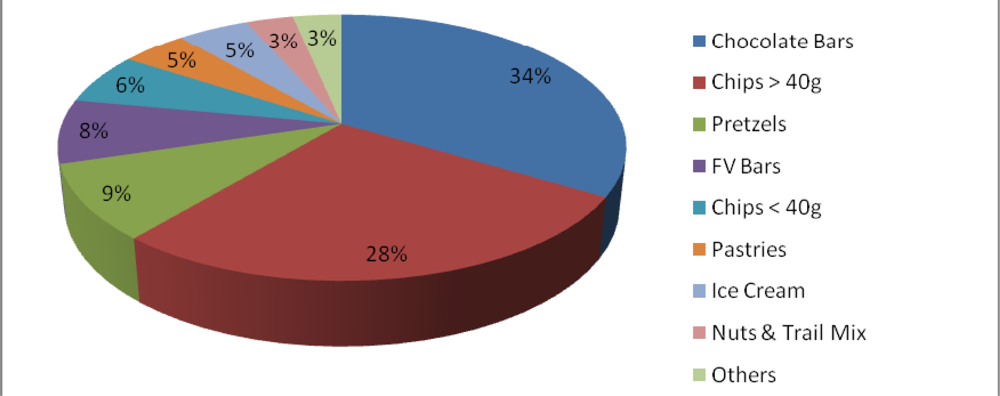
13]. Anecdotal reports and observations have suggested that there are many exposures to energy dense, low nutrient foods in the recreation environment, but there is limited evidence in the literature to support these claims. One Canadian study completed in 2006 looked at the foods offered in sports, recreational and cultural facilities in Quebec City and found that most items in the vending machines and snacks were of low nutritional value [
14]. Some evidence suggests that public recreation staff are willing to collaborate with health promotion professionals to advance shared goals for physical activity promotion [
15], which could also be extended to address nutritional concerns. The purpose of this study was to describe the public recreation food environment and explore the current context and facilitators and barriers to change.
Focus Groups
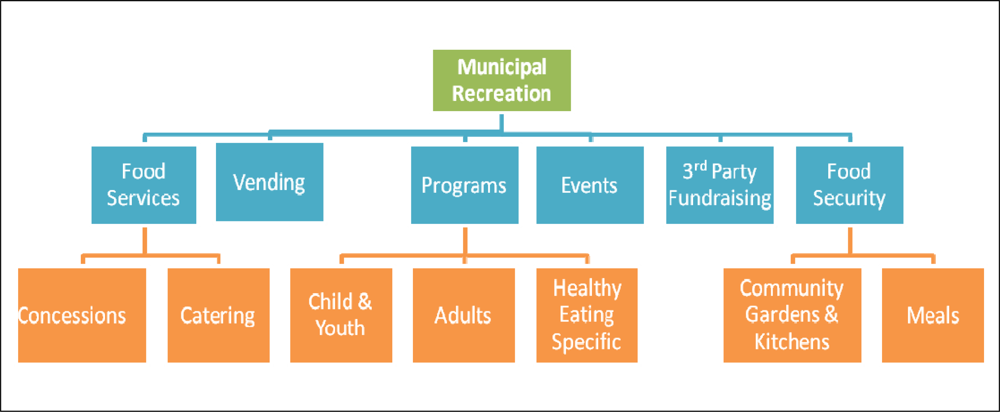
The data collected from the audit broadly indicated that the food environments were not particularly healthy in most recreation facilities, but staff were interested and engaged in some improvement initiatives. In response, focus groups were conducted to gain a better understanding of the barriers and facilitators that recreation facilities may face. The information collected from the focus groups has been grouped into ten key themes, which are explained below. Both results and recommendations from the findings are presented in this section.
Theme 1: Education
The recreation staff expressed a need to educate staff and the public on healthy eating, and making healthy choices. They felt that staff did not have adequate nutritional education necessary for selecting the most appropriate healthy choices for vending machines and concession operation. For example one staff member stated, “we need some education for food service staff”. Staff indicated that education needed to go beyond staff at recreation facilities and extend to educating the public: “we need more info to give parents and kids about healthy choices”.
Theme 2: Food Security
Food security emerged as an important concern for many communities. The definition for food security adopted by the World Health Organization is “when all people, at all times, have physical and economic access to sufficient, safe and nutritious food to meet their dietary needs and food preferences for an active and healthy life” [
25]. Food security provides conditions that promote health by providing essential nutrients and minimizing food related stress [
26]. Many comments arising in the focus groups reflected concerns related to proper nutrition and basic food security issues. Although the topic arose in all focus groups, comments regarding food security were more prevalent in recreation centers situated in lower income neighborhoods. One focus group participant said, “any child, if they are hungry on the playground, we automatically feed them”. Another staff member stated that “kids can come in to the recreation centre and get food on school breaks if they have [no food]”. Since recreation facilities are places where youth frequent during their school breaks and children spend significant time before and after school, they also become regular food access locations, especially in neighborhoods where food security is an issue. With this in mind, recreation centers may benefit from access to support (information, grants and partnerships) for providing nutritious foods in their facilities, and increasing food security.
Theme 3: Programs
Similar to the MRFEAT audit results, focus groups highlighted that some recreation centers had implemented programs that promoted and provided healthy choices in their facilities. One staff member commented on a healthy eating program they had started:
“We have child/preschool programs going on in which there are cooking classes which have switched to incorporate all the food groups and decrease the amount of cookies and treats being made, for example they cooked a vegetable curry and it was a success”.
Participants indicated that they would like to learn about best practice models and success stories from other recreation centers, in order to engage with programs that have been successful. In particular, one person requested “examples of models that are working, how, why, where and when”. Another person stated that “we need some examples of people who have done this successfully, and how they went about it”.
Theme 4: Partnerships
Recreation centers indicated that partnerships were instrumental to the successful promotion of healthy eating. In particular, one person indicated the “need to cultivate corporate relationships that work together”. The literature indicates that partnerships are an effective way to help promote and sustain health promotion initiatives [
27].
Theme 5: Vending
Vending machines were repeatedly discussed in the focus group sessions, specifically concerning the food sold in the vending machines and the contracts with vending companies. The types of concerns raised included,
“…how is it possible to change the food in the vending machines? What is the duration that milk is going to last? How do you do it? People are concerned about if it is even possible … so they are just turning off the idea”.
Many facilities are committed to long term contracts with vending companies, therefore, resources to assist recreation centers with developing healthy request for proposals (RFPs), as well as for approaching negotiations with vending companies to offer healthier options were desired. At the time of the focus groups, the number of vending companies that were offering healthy options was limited but increasing. Some comments also focused on the importance of vending as a source of revenue for recreation centers, and the difficulty of accessing alternative funds if vending machines changed or were removed. For example, one person emphasized the need to be “point[ed]…in the direction where we won’t lose money, but maintain healthy choices”. For many recreation facilities, however, “the problem lies within the costs, unless items are subsidized [people won’t pay more for them and] the company will pull the machines unless they make some profit”. As a result, many recreation facilities felt pressured to keep sales high by selling unhealthy choices.
Theme 6: Policy Implementation
Policy related to food and beverages was discussed as a key ingredient for ensuring healthier options were available in vending machines, at concessions, fundraising events, and in child and youth programs. One participant commented “…we really don’t have any policies in terms of what we’re going to serve to the children … nothing that is written, no procedures”. Similarly, another participant stated that they “don’t have any policies or guidelines”. From the responses, it was evident that most recreation centers did not have healthy eating policies in place; however, staff indicated that having a policy may help them to implement healthy choices. This supported the results of the MRFEAT audit.
Theme 7: Facilitation of Change
When discussing the motivation to change in the focus groups, recreation staff indicated that change would be most successful if it was done in a slow, step by step manner. “None of this happens overnight, and we have to be patient when we are trying to create change”. Also, it was expressed that they “…should take baby steps to get the best reaction”. These comments are consistent with the body of knowledge from implementation research, that change is best accepted when done slowly [
28]. Change also occurs best when stakeholders are involved in the changes that will be made [
29]. Therefore when facilitating change in the recreation centers it is important to incorporate staff ideas, and involve them in the process.
Theme 8: Environment
Focus group participants stated that the recreation environment impacts healthy eating in two ways. First, if vending machines provided unhealthy options, children would choose those options over healthier ones. For example one participant stated, “…for me it’s all about accessibility, it’s my own kids, little kids, they see a vending machine and they want something, if they don’t see it, they don’t ask for it”. Second, participants felt that providing healthier choices was imperative and that changes would have to be made in order to achieve this. The following comment reflects this: “concession stands are selling unhealthy snacks and need to be monitored”. Recreation centers needed information on how to provide healthier options in their concession stands, as well as how to improve vending options.
Theme 9: Barriers
Many barriers and issues were raised by focus group participants as to why it was a challenge to provide healthy food options in recreation centers. Some of the typical responses included, “we are unsure of how we will plan and promote change”, and “[healthy food] takes longer to prepare and more [cooking equipment] is needed”, and finally, “accessibility of [healthy food supplies] … is another obstacle”.
Theme 10: Facilitators
Participants had many suggestions of facilitators for offering healthier food and beverages in recreation facilities. They commented on resources that would be useful, including posters to advertise healthier choices, online resources, information on ways to provide healthier food, as well as general educational material on nutrition. One participant commented it would be useful to “maybe even start with a booklet of alternate ways to provide things, modifications to things you might be selling that are healthier”.
4. Conclusions and Recommendations
Publicly funded recreation is a critical setting for action on healthy eating. To our knowledge this is the second published study about this important environment and its potential to support public health goals. Our data highlighted however, that recreation environments were not offering or promoting healthy choices and in many cases promoted food and beverages that are considered major culprits in the increasing obesity epidemic. There was a strong interest and motivation among select recreation facility staff and stakeholders to change their situation. The recreation facilities expressed that changing the food environment would require support, and would not happen quickly. Implementation would need to be founded on inclusion of recreation stakeholders throughout the process and support for change. In addition, a resource toolkit and other supports for action were necessary to address barriers and facilitators to change and successfully change the food environment in recreation.
Since the majority of facilities had food and beverage services on site and reported having control over what food items were sold, opportunities existed for staff to influence the nutritional quality of food services. However, few facilities had committees or initiatives underway to help promote and provide healthier choices and the focus group results challenged the notion of control over the food items sold when long-term vending contracts were in place and there was potential for loss of revenue. In addition, children’s nearly unlimited access to snack bars and vending machines suggests that changing products as well as limiting access to unhealthy food choices may be recommended. Although few facilities offered meals to children in programs, staff had many opportunities to influence the snacks served, as well as educate parents about sending healthy lunches. The implementation of food policies in recreation would support the efforts of staff in initiating healthy changes to the food environment, and should be pursued further.
The results from the focus groups provided in-depth information and feedback related to staff perceptions about promotion and provision of healthy food in the facilities. From these discussions it is evident that recreation staff required increased education and support for healthy eating, and that it was important that they understood the rationale for the changes. Furthermore, many communities faced food security issues. Some facilities offered programs that promoted or provided healthy food; however, the majority did not, so this may present another opportunity for recreation to support community health.
Information on healthy eating and food security initiatives or programs that are currently being implemented in recreation centers should be shared with other recreation centers. This transfer of knowledge may motivate and assist other recreation centers in adopting programs that have been successfully implemented elsewhere.
The strengths of this study were the mixed methods design that allowed for corroboration across data sources and participants as well as in-depth discussion with stakeholders. These findings are limited by the self-report nature of the data, high variability across facilities and a low response rate that may have led to a positive response bias and consequently an overstatement of the situation. The response rate was attributed to the length and difficulty of the audit and the timing during which the audit was completed (following 2 years of infrastructure surveys).
Data on changing the food environment in recreation facilities is limited, and the one recent study of sports, recreational and cultural facilities in Quebec City [
14] confirmed the findings of this study—a majority of foods and beverages served had low nutritional value and there were a limited number of healthy choices.
This study validates the need for further research on effective setting-based approaches to changing food environments in recreation facilities. The impact of environmental change interventions on food products, sales and patron responses within the context of municipal recreation should be researched further. The data gathered in this study indicates the need for policy, adequate resources, partnerships and information to design and facilitate healthier choices in municipal recreation facilities.

 ,
, 



{kind=link}
{kind=link}
{kind=link}