Surveillance of Summer Mortality and Preparedness to Reduce the Health Impact of Heat Waves in Italy

Abstract
:1. Introduction
- - city-specific Heat Health Watch Warning Systems (HHWWS);
- - local network for the distribution of the warning bulletin;
- - national prevention guidelines;
- - local registries of at-risk subgroups of the population;
- - a rapid “real time” mortality surveillance system;
- - evaluation of warning systems and prevention programs introduced.
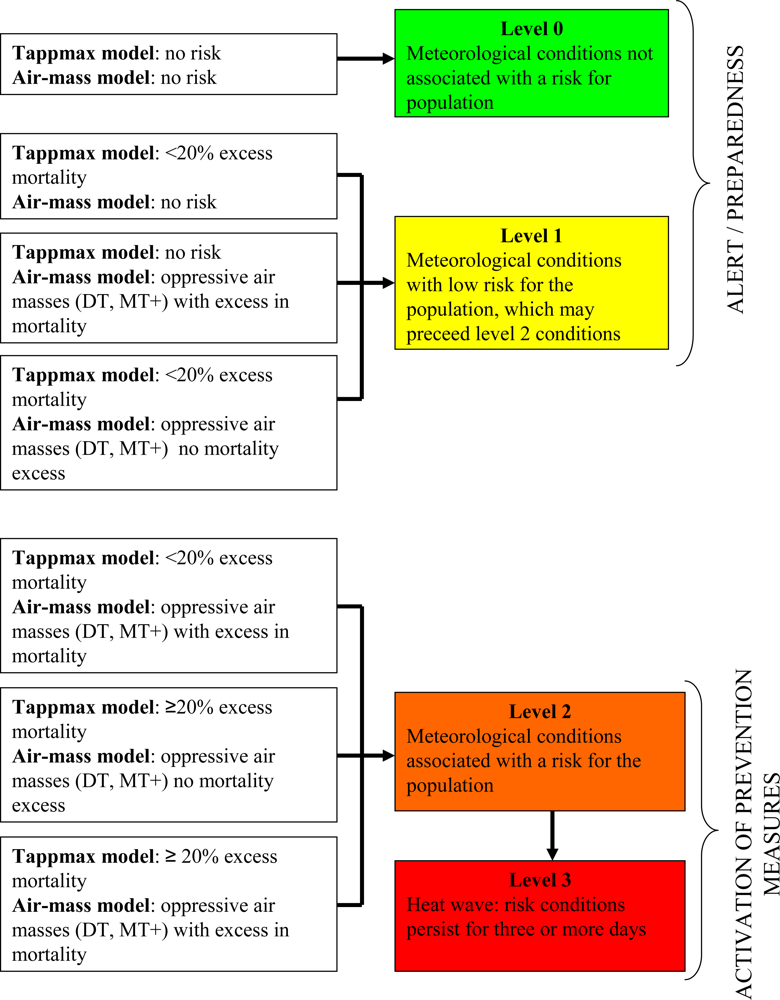
2. Heat Health Watch Warning Systems (HHWWS)
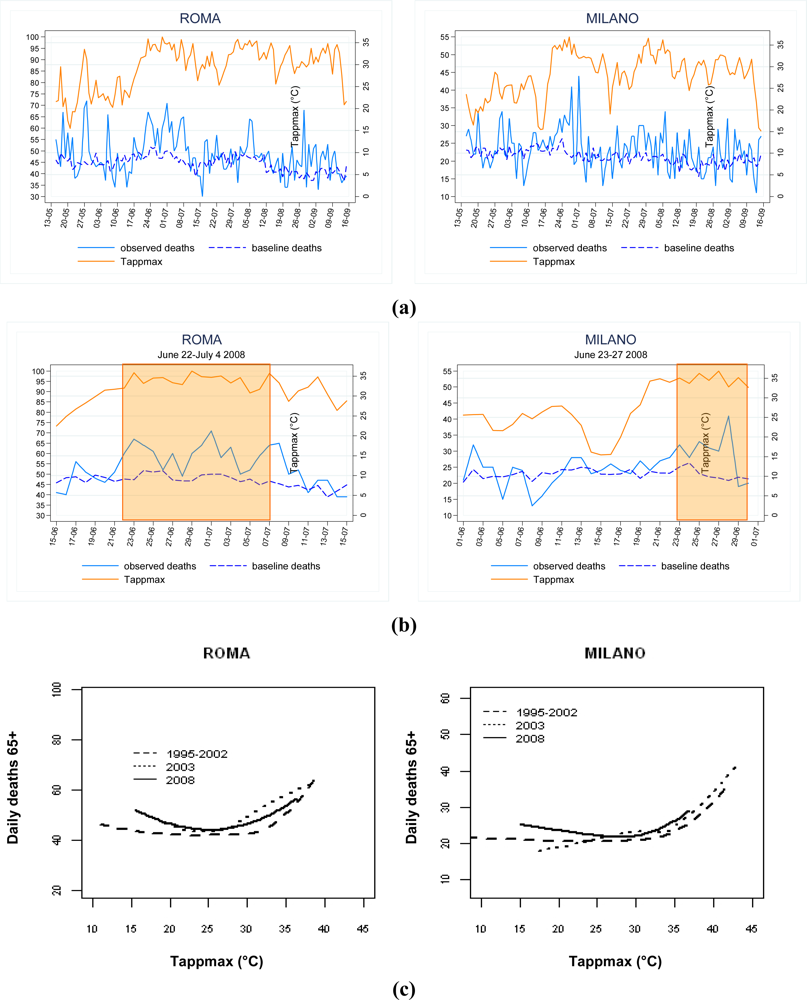
3. Mortality Surveillance System and Evaluation of the Impact of High Temperature on Mortality
- the calculation of excess mortality by month/summer season;
- the calculation of excess mortality by heat wave episode;
- the description of the dose-response curve to examine the relationship between Tappmax and mortality.
4. Identification of at-Risk Subgroups
5. Heat Prevention Plan
6. Discussion
Acknowledgments
References
- Michelozzi, P; Kirchmayer, U; Katsouyanni, K; Biggeri, A; McGregor, G; Menne, B; Kassomenos, P; Anderson, HR; Baccini, M; Accetta, G; Analytis, A; Kosatsky, T. Assessment and prevention of acute health effects of weather conditions in Europe, the PHEWE project: background, objectives, design. Environ. Health 2007, 6, 12. [Google Scholar]
- Baccini, M; Biggeri, A; Accetta, G; Kosatsky, T; Katsouyanni, K; Analitis, A; Anderson, HR; Bisanti, L; Danova, J; D’Ippoliti, D; Forsberg, B; Medina, S; Paldy, A; Rabczenko, D; Schindler, C; Michelozzi, P. Effects of apparent temperature on summer mortality in 15 European cities: results of the PHEWE project. Epidemiology 2008, 19, 711–719. [Google Scholar]
- Michelozzi, P; Accetta, G; De Sario, M; D’Ippoliti, D; Marino, C; Baccini, M; Biggeri, A; Anderson, HR; Katsouyanni, K; Ballester, F; Bisanti, L; Cadum, E; Forsberg, B; Forastiere, F; Goodman, PG; Hojs, A; Kirchmayer, U; Medina, S; Paldy, A; Schindler, C; Sunyer, J; Perucci, CA; on behalf of the PHEWE collaborative group. High Temperature and Hospitalizations for Cardiovascular and Respiratory Causes in 12 European Cities. Am. J. Respir. Crit. Care Med 2009, 179, 383–389. [Google Scholar]
- Kovats, RS; Ebi, KL. Heatwaves and public health in Europe. Eur. J. Public Health 2006, 16, 592–599. [Google Scholar]
- Michelozzi, P; de’ Donato, F; Bisanti, L; Russo, A; Cadum, E; DeMaria, M; D’Ovidio, M; Costa, G; Perucci, CA. The impact of the summer 2003 heat waves on mortality in four Italian cities. Euro. Surveill 2005, 10, 161–165. [Google Scholar]
- National Department of Civil Protection, National Coordination Centre. . Effetti sulla salute delle condizioni climatiche—Principali risultati e criticità. Estate 2008 (The impact of climatic conditions on health during summer 2008—Main results and critical aspects). Technical document (available on request).
- IPCC. Climate Change 2007: The Physical Science Basis Contribution of Working Group I to the Fourth Assessment Report of the Intergovernmental Panel on Climate Change; Solomon, S, Qin, D, Manning, M, Chen, Z, Marquis, M, Averyt, KB, Tignor, M, Miller, HL, Eds.; Cambridge University Press: United Kingdom and New York, NY, USA; p. 996.
- Gualdi, S; Navarra, A. Scenari climatici nel bacino mediterraneo. Forest 2006, 2, 19–30. (in Italian). [Google Scholar]
- Michelozzi, P; De Sario, M; Accetta, G; de’Donato, F; Kirchmayer, U; D’Ovidio, M; Perucci, CA; the HHWWS Collaborative Group. Temperature and summer mortality: Geographical and temporal variations in four Italian cities. J. Epidemiol. Community Health 2006, 60, 417–423. [Google Scholar]
- Kalkstein, LS; Barthel, CD; Green, JS; Nichols, MC. A New Spatial Synoptic classification: application to Air Mass Analysis. Int. J. Climatol 1996, 16, 983–1004. [Google Scholar]
- Sheridan, SC. The Re-development of a Weather Type Classification Scheme for North America. Int. J. Climatol 2002, 22, 51–68. [Google Scholar]
- de’ Donato, F; Michelozzi, P; Kalkstein, L; D’Ovidio, M; Kirchmayer, U; Accetta, G; Perucci, CA. The Italian project for prevention of heat-health effects during summer, findings from 2005. In Annalen der Meteorologie, Proceedings of the 17th International Congress of Biometeorology, Garmish, Germany, September 2005; 2005; 41, pp. 287–290. [Google Scholar]
- D’Ovidio, M; Marino, C; Palange, S; De Sario, M; Michelozzi, P; Perucci, CA. A rapid surveillance system of daily mortality during summer in Italy. Epidemiology 2006, 17, S448. [Google Scholar]
- Cleveland, WS. Robust locally weighted regression and smoothing scatterplots. J. Am. Stat. Assoc 1979, 74, 829–836. [Google Scholar]
- Johnson, H; Kovats, RS; McGregor, G; Stedman, J; Gibbs, M; Walton, H. The impact of the 2003 heat wave on daily mortality in England and Wales and the use of rapid weekly mortality estimates. Euro. Surveill 2005, 10, 168–171. [Google Scholar]
- Fouillet, A; Rey, G; Laurent, F; Pavillon, G; Bellec, S; Ghihenneuc-Jouyaux, C; Clavel, J; Jougla, E; Hémon, D. Excess mortality related to the August 2003 heat wave in France. Int. Arch. Occup. Environ. Health 2006, 80, 16–24. [Google Scholar] [Green Version]
- Stafoggia, M; Forastiere, F; Agostini, D; Biggeri, A; Bisanti, L; Cadum, E; Caranci, N; de’Donato, F; De Lisio, S; De Maria, M; Michelozzi, P; Miglio, R; Pandolfi, P; Picciotto, S; Rognoni, M; Russo, A; Scarnato, C; Perucci, CA. Vulnerability to heat-related mortality: a multicity, population-based, case-crossover analysis. Epidemiology 2006, 17, 315–323. [Google Scholar]
- Vandentorren, S; Bretin, P; Zeghnoun, A; Mandereau-Bruno, L; Croisier, A; Cochet, C; Ribe’ron, J; Siberan, I; Declercq, B; Ledrans, M. August 2003 heat wave in France: risk factors for death of elderly people living at home. Eur. J. Public Health 2006, 16, 583–591. [Google Scholar]
- Stafoggia, M; Forastiere, F; Agostini, D; Caranci, N; de’Donato, F; Demaria, M; Michelozzi, P; Miglio, R; Rognoni, M; Russo, A; Perucci, CA. Factors affecting in-hospital heat-related mortality: A multi-city case-crossover analysis. J. Epidemiol. Community Health 2008, 62, 209–215. [Google Scholar]
- Cesaroni, G; Agabiti, N; Rosati, R; Forastiere, F; Perucci, CA. An index of socioeconomic position based on 2001 Census, Rome. Epidemiol Prev 2006, 30, 352–357. (in Italian). [Google Scholar]
- Schifano, P; Cappai, G; De Sario, M; Michelozzi, P; Marino, C; Bargagli, AM; Perucci, CA. Susceptibility to heat wave-related mortality: a follow-up study of a cohort of elderly in Rome. Environ. Health 2009, 8, 50. [Google Scholar]
- National Centre for Diseases Prevention and Control (CCM), Italian Ministry of Health.
- Koppe, C; Kovats, S; Jendritzky, G; Menne, B. Heat-Waves: Risks and Responses; ; Health and Global Environmental Change Series, No. 2. World Health Organization: Geneva, Switzerland, 2004. [Google Scholar]
- Koppe, C; Becker, P. Comparison of operational Heat Health Warning Systems in Europe, . Working document of the project “Improving Public Health Responses to Extreme Weather/Heat-Waves—EuroHEAT”, WHO egional Office for Europe 2007. Technical document (available on request).
- Smith, GE; Cooper, DL; Loveridge, P; Chinemana, F; Gerard, E; Verlander, N. A national syndromic surveillance system for England and Wales using calls to a telephone helpline. Euro. Surveill 2006, 11, 220–224. [Google Scholar]
- Josseran, L; Nicolau, J; Caillère, N; Astagneau, P; Brücker, G. Syndromic surveillance based on emergency department activity and crude mortality: two examples. Euro. Surveill 2006, 11, 668. [Google Scholar]
- Kovats, SR; Hajat, S; Wilkinson, P. Contrasting patterns of mortality and hospital admissions during hot weather and heat waves in Greater London, UK. J. Occup. Environ. Med 2004, 61, 893–898. [Google Scholar]
- Bernard, SM; McGeehin, MA. Municipal heat wave response plans. Am. J. Public Health 2004, 94, 1520–1522. [Google Scholar]
- Luber, G; McGeehin, M. Climate change and extreme heat events. Am. J .Prev. Med 2008, 35, 429–435. [Google Scholar]
- WHO Regional Office for Europe. Heat-Health Action Plans Guidance; Matthies, F, Bickler, G, Marín, NC, Hales, S, Eds.; WHO Regional Office for Europe: Copenhagen, Denmark, 2008. [Google Scholar]
- Palecki, MA; Changnon, SA; Kunkel, KE. The Nature and Impacts of the July 1999 Heat Wave in the Midwestern United States: Learning from the Lessons of 1995. Bull. Am. Meteorol. Soc 2001, 82, 1353–1367. [Google Scholar]
- Weisskopf, M; Anderson, H; Foldy, S; Hanrahan, LP; Blair, K; Török, TJ; Rumm, PD. Heat Wave Morbidity and Mortality, Milwaukee, Wis, 1999 vs 1995: An Improved Response? Am. J. Public Health 2002, 92, 830–833. [Google Scholar]
- Ebi, K; Teisberg, TJ; Kalkstein, LS; Robinson, L; Weiher, RF. Heat watch/warning system save lives: estimated costs and benefits for Philadelphia 1995–1998. Proceedings of the 14th Conference on Applied Climatology; Symposium on Planning, Nowcasting, and Forecasting in the Urban Zone, Seattle, WA, USA, January 2004.
- Fouillet, A; Rey, G; Wagner, V; Laaidi, K; Empereur-Bissonnet, P; Le Tertre, A; Frayssinet, P; Bessemoulin, P; Laurent, F; De Crouy-Chanel, P; Jougla, E; Hémon, D. Has the impact of heat waves on mortality changed in France since the European heat wave of summer 2003? A study of the 2006 heat wave. Int. J. Epidemiol 2008, 37, 309–317. [Google Scholar]
- Braga, ALF; Zanobetti, A; Schwartz, J. The Effect of Weather on Respiratory and Cardiovascular Deaths in 12 U.S. Cities. Environ. Health. Perspect 2002, 110, 859–863. [Google Scholar]
- Hajat, S; Haines, A. Association of cold temperatures with GP consultations for respiratory and cardiovascular disease amongst the elderly in London. Int. J. Epidemiol 2002, 31, 825–830. [Google Scholar]
- Stafoggia, M; Forastiere, F; Agostini, D; Caranci, N; de’Donato, F; Demaria, M; Michelozzi, P; Miglio, R; Rognoni, M; Russo, A; Perucci, CA. Factors affecting in-hospital heat-related mortality: A multi-city case-crossover analysis. J. Epidemiol. Community Health 2008, 62, 209–215. [Google Scholar]



{kind=link}
{kind=link}
| Variables included in the model | Results* | |
|---|---|---|
| Tappmax approach | Exposure:
Other variables:
| Tappmax thresholds for 10–20% excess mortality:
Tappmax thresholds for >20% excess mortality:
|
| Air-mass approach | For each Air mass:#
| Air mass frequency:
Excess mortality in 65+ population (%):
|
| Method | Formula | Strengths | Limitations |
|---|---|---|---|
| A) Analysis by month/summer | Relative excess mortality (%)=(O-E)/E*100 Where:
|
|
|
| B) Analysis of heat wave episodes | Heat wave: ≥ 3 consecutive days with HHWWS level 2 or 3 risk conditions for health plus 3 days following the event Relative excess mortality (%)=(O-E)/E*100 Where:
|
|
|
| C) Time-series analysis of relationship between temperature and mortality | Shape of exposure-response curve Poisson generalized additive model (GAM) with smooth function of Tappmax (i.e., penalized regression spline) or locally weighted linear regression |
|
|
| Preventive measure | Level of implementation* | Description |
|---|---|---|
| Written local prevention plan | +++ | Guidelines developed at local level including prevention activities and network of health and social services available |
| Social interventions | ||
| Educational campaign | +++ | Informative fliers distributed in public places, health centers and General practitioners (GPs). Specific advice disseminated during heat waves. |
| Telephone help-line | +++ | Dedicated help-line providing social support services or regular telephone contact on demand (tele-monitoring) |
| Social support services | +++ | Home visits, personal and home care, and home pharmacy services provided by social workers or volunteers |
| Availability of air-conditioned places | + | Implementation of air-conditioning units in health and social centers and increase access during heat waves |
| Educational programmes for social and health workers | ++ | Training, seminars/workshops, diffusion of specific guidelines among health and social professionals |
| Health care interventions | ||
| Health surveillance of susceptible individuals | ++ | Phone calls and home visits by GPs. Network of health and social services triggered by a dedicated telephone line |
| Local register of susceptible individuals | ++ | Identification of susceptible individuals on the basis of demographic and health characteristics using population registries and health information systems or notification by GPs and social workers |
| Emergency protocols | ++ | Emergency measures (i.e., bed redistribution, discharge planning) to improve operational efficiency in hospitals, nursing homes and social structures |
© 2010 by the authors; licensee Molecular Diversity Preservation International, Basel, Switzerland. This article is an open-access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Michelozzi, P.; De’ Donato, F.K.; Bargagli, A.M.; D’Ippoliti, D.; De Sario, M.; Marino, C.; Schifano, P.; Cappai, G.; Leone, M.; Kirchmayer, U.; et al. Surveillance of Summer Mortality and Preparedness to Reduce the Health Impact of Heat Waves in Italy. Int. J. Environ. Res. Public Health 2010, 7, 2256-2273. https://doi.org/10.3390/ijerph7052256
Michelozzi P, De’ Donato FK, Bargagli AM, D’Ippoliti D, De Sario M, Marino C, Schifano P, Cappai G, Leone M, Kirchmayer U, et al. Surveillance of Summer Mortality and Preparedness to Reduce the Health Impact of Heat Waves in Italy. International Journal of Environmental Research and Public Health. 2010; 7(5):2256-2273. https://doi.org/10.3390/ijerph7052256
Chicago/Turabian StyleMichelozzi, Paola, Francesca K. De’ Donato, Anna Maria Bargagli, Daniela D’Ippoliti, Manuela De Sario, Claudia Marino, Patrizia Schifano, Giovanna Cappai, Michela Leone, Ursula Kirchmayer, and et al. 2010. "Surveillance of Summer Mortality and Preparedness to Reduce the Health Impact of Heat Waves in Italy" International Journal of Environmental Research and Public Health 7, no. 5: 2256-2273. https://doi.org/10.3390/ijerph7052256
APA StyleMichelozzi, P., De’ Donato, F. K., Bargagli, A. M., D’Ippoliti, D., De Sario, M., Marino, C., Schifano, P., Cappai, G., Leone, M., Kirchmayer, U., Ventura, M., Di Gennaro, M., Leonardi, M., Oleari, F., De Martino, A., & Perucci, C. A. (2010). Surveillance of Summer Mortality and Preparedness to Reduce the Health Impact of Heat Waves in Italy. International Journal of Environmental Research and Public Health, 7(5), 2256-2273. https://doi.org/10.3390/ijerph7052256