2.2. Health Impact Assessment
In order to analyze the magnitude of the burden of cholera attributable to climate change, it is useful to decide on the different scenarios that the analysis will be based on. For this purpose, climate-change predictions for the specific locality, as well as population growth and economic development, will need to be considered. The approach used in this study follows the methodological framework suggested by Chiabai
et al. [
34], who estimated the additional costs of planned adaptation in the health sector in India for 2030. Two scenarios are suggested.
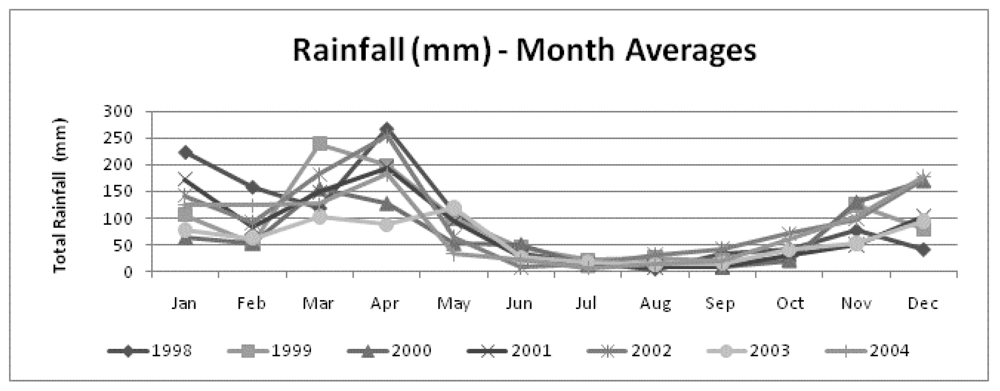
Figure 2.
Seasonal distribution of rainfall in Tanzania: Monthly averages (mm).
Figure 2.
Seasonal distribution of rainfall in Tanzania: Monthly averages (mm).
Scenario C0, for 2030, is the baseline scenario and does not include climate change. The scenario is based on the baseline projections of Mathers and Loncar [
35]. These projections include estimates for diarrheal diseases in 2030 for the main world regions, based on WHO estimates for 2002. The estimates are based on past correlations between increased growth and mortality trends for specific illnesses. The estimates make two main assumptions. First, economic development in the form of increasing GDP and other socio-economic developments are expected to have a positive influence on the performance of the health sector. Therefore, the relative burden of disease in 2030 is expected to decrease considerably when compared with current levels due to economic development, with improvements in the performance of the health sector and increased coverage of water and sanitation (basic preventive adaptation measures). Secondly, developing countries are expected to have constant growth without crises or negative impacts on economic development. Mathers and Loncar [
35] take into account GDP per capita, years of schooling by adults and the impact of technology on population health measured with a time variable. Population projections for 2030 are included based on UN-projected population figures [
36], taking into account the fertility rate and immigration.
As the projections for diarrheal diseases are not released at country levels but are only available at the regional level, the initial step was to downscale the projected number of deaths at the country level. This was done using the projections of Mathers and Loncar [
35] of total deaths from diarrheal diseases to calculate the percentage contribution of each country in Sub-Saharan Africa to the projected regional burden of disease. As the projections are provided only for diarrheal diseases as an aggregate, the next step was to calculate the corresponding number of deaths for cholera. For this purpose the proportion of deaths caused by cholera with respect to diarrheal deaths in Tanzania was calculated based on
WHO Weekly Epidemiological Reports 2000–2010 [
37]. Next, the number of cholera cases was estimated based on the derived estimate of deaths using the average case fatality rate (CFR) of 3.18 percent for cholera deaths in Tanzania, which was also based on the
WHO Weekly Epidemiological Reports 2000–2010. The results from the econometric analysis described in the next section suggest a CFR equal to 0.078. However, the dataset available for this estimation comprised only 15 observations, which compromises the reliability of this estimate. Therefore, the average CFR for cholera in Tanzania provided by the WHO was used, which is also a more conservative estimate (0.0318).
Lastly, to supplement the estimated deaths and cases, a measure of population health has been estimated by combining data on mortality and non-fatal health outcomes into a single figure. For this purpose, Disability-Adjusted Life-Years (DALY) was applied. Several other measures, besides DALY, have been devised in the literature, including the Quality-Adjusted Life Year (QALY), Disability-Adjusted Life Expectancy (DALE) and the Healthy Life Year (HeaLY) [
38,
39,
40,
41]. The benefits and challenges of the various measures have been examined [
42,
43,
44,
45]. It should nonetheless be noted that the DALY measure has been criticized because it does not use different weights for sexes or different age weights, does not discount future years lost, and, lastly, it does not use severity weighting of disabilities. However, since DALY has been the most widely used measure and is often used as an index in the comparison of health impacts in studies of disease, the DALY metric has been used for the purpose of this study.
DALY measures disease burden and combines years of life lost (YLL) from premature deaths with years of life lived with disabilities (YLD).
YLL is estimated as
YLL =
ND ×
EX where
ND is number of deaths, and
EX is life expectancy at age of death. A life expectancy at birth of 63.8 years (both sexes combined) by 2030 based on the UN World Population Prospects [
35] is used. To allow for the estimate of life expectancy at age of death, it is necessary to obtain the age distribution of cholera deaths. For this purpose, WHO estimates of the distribution of diarrheal diseases between age groups in Sub-Saharan Africa are used, assuming that this distribution is the same for Tanzania [
14]. Here, a limitation of this study must be acknowledged given the availability of data, since it has not been possible to retrieve the age distribution specifically for cholera deaths in Tanzania as a whole, nor on a regional basis. Nonetheless, the estimates include cholera (and other diarrheal diseases). It may, however, have an impact on the results, since there may be an overweight of the share of deaths among children under 5 years of age, which may not be the same for cholera as it is for diarrhea.
YLD is estimated as
YLD =
I ×
DW ×
L, where I is the total number of cases,
DW is disability weight, and
L is the duration of each cholera episode.
YLD estimates are limited to loss of health experienced by individuals, and do not take into account other aspects of the quality of life or well-being, or the impacts of one individual’s health condition on other people. Disability weight captures valuation of time lived in a non-optimal health state viewed from societal preferences. The disability weight ranges between 0 (health condition is equivalent to full health) and 1 (health condition is equivalent to death) and quantifies judgments about the overall levels of health associated with different health states, not judgments on the relative values of lives lived, persons, overall well-being, quality of life or utility. In estimating
YLD a disability weight of 0.15 is used. This is equivalent to that used by the WHO [
46], which is intended to reflect average global valuations. Again, the data availability limits the estimates to use the weight provided for diarrheal diseases as an aggregate. Information on the average duration of a cholera episode (5 days) was obtained from the Tanzanian Ministry of Health. In the estimates, it was assumed that age-sex-specific incidence ratios would remain constant into the future, as would average durations and disability weights.
The second scenario,
Scenario C1, builds on
Scenario C0 and estimates the number of cholera cases, deaths and DALYs in the light of projected climate-change impacts. The estimates are produced by taking into account the relative risk of contracting cholera projected for 2030, which represents the relative change in the dependent variable given a one-unit change in the explanatory variable. The relative risk applied here is based on an econometric analysis of the relationship between climate variability and cases of cholera as described in the next section. The relative risks are applied to the projected number of cases calculated in
Scenario C0. The difference between the estimates derived in the two scenarios (with and without climate change) represents the burden of disease attributable to climate change. The calculations for
Scenario C1 assume a 1 and 2 degree Celsius temperature increase respectively, based on the IPCC [
3], A1B middle scenario, temperature predictions for Tanzania for 2030.
Calculations of the burden of disease attributable to climate change are based on the Impact Fraction suggested by McMichael
et al. [
5]. The Impact Fraction is the fraction of the total disease burden attributable to climate change, and is calculated by combining the proportion of population exposed with the relative risks:
where IFi is defined as the impact fraction attributable to climate change for disease i; Pi is the proportion of the population exposed to the disease; and RRi is the relative risk of the disease under different climate scenarios.
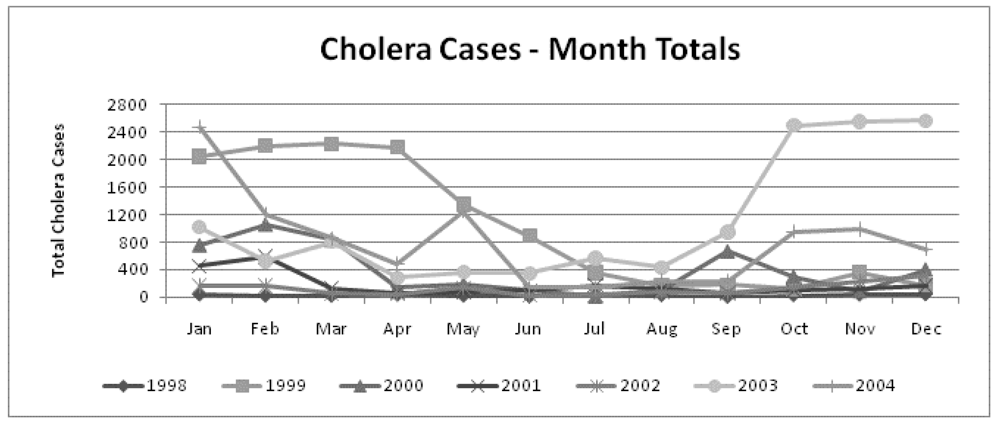
Assessing the Relationship Between Climate Variability and Cholera Cases
In order to investigate trends in the seasonal pattern, regression analyses, using Stata/SE version 10.1 for Windows, were conducted where a dummy variable, ‘drought’, equals 1 between June and October and zero at other times. A time-trend variable was also used to capture the possible socio-economic effects on cholera cases that were not available at the month level. For example, it seems reasonable to assume that the population, the percentage of the population with access to safe water and sanitation, education levels and income all grew over time between 1998 and 2004.
In order to investigate the potential relationship between climate variability and cases of cholera to identify the relative risk, Poisson regression analysis was initially used (similar to others in the field; see e.g., Singh
et al. [
13]; Kuhn
et al. [
47]; Tango [
48]). A Poisson regression is used to fit models of the number of occurrences or counts of an event (dependent variable) assuming that they follow a Poisson distribution. However, the Poisson regression analysis requires that the data present conditional variance equal to the conditional mean. Therefore, we performed log-likelihood (goodness of fit) tests after all Poisson models initially estimated and confirmed that the required non-dispersion assumption is violated. In other words, the count data present over dispersion, invalidating the use of Poisson models, and alternative models were required for the analysis, such as the negative binomial model [we do not present the Poisson models’ results in the annex since they were not used in our calculations due to the overdispersion problem. Instead, we present in the annex our preferred negative binomial models based on the usual tests (e.g., log-likelihood test; Wald-test; Akaike test; BIC)]. A negative binomial regression model estimates the expected value of the dependent variable as a log-linear function of a set of independent variables and regression parameters, while correcting for data over dispersion [
49]. The specifications used in the negative binomial models are of the general form:
![Ijerph 08 04386 i002]()
where health endpoint is the incidence of cholera cases or deaths in period t (month or year); climate variable represents rainfall or temperature; and X is a vector of socioeconomic factors that may explain the health endpoint (population growth, GDP, water and sanitation coverage, literacy rate and cassava production per capita). For each dataset, different models have been tested with specifications combining all the available explanatory variables. The preferred models were chosen according to the level of significance of regressors in each model and the goodness-of-fit of each model (log-likelihood; Wald chi-squared; and Akaike and Bayesian information criteria). Details of the preferred models are given in Annex 1. A time-trend variable was integrated into the model to capture the effect of other socioeconomic variables that potentially influence cholera cases and that were absent from this dataset.


{kind=link}
{kind=link}



