Measurement of Community Empowerment in Three Community Programs in Rapla (Estonia)

Abstract
:1. Introduction
1.1. The Aim of the Study
- to demonstrate the measurement process of the ODCE;
- to present the findings of the measurement of the ODCE; and
- to discuss the process, findings, limitations and implications of the study.
1.2. Context and Settings
1.3. Conceptualizing Organizational Domains of Community Empowerment
- activation of the community;
- competence of the community in solving its own problems;
- program management skills and
- creating a supportive environment.
1.4. Elaboration of the Measurement Tool
2. Methodology
2.1. Theoretical Framework
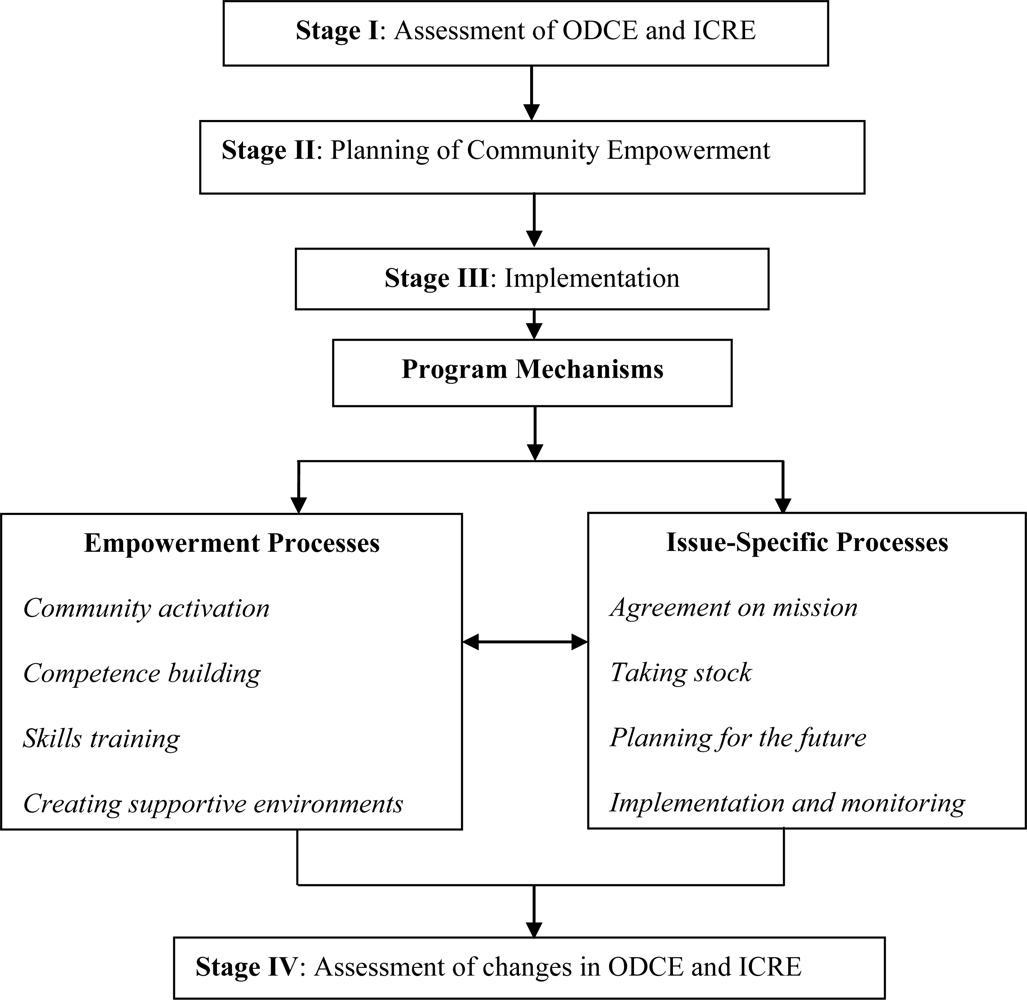
- Stage I—assessment of ODCE (undertaken by the workgroups in the three community programs) and evaluation of the individual community related empowerment (ICRE). The latter is beyond the scope of the current paper and, hence, is not reported here.
- Stage II—planning of community empowerment. This stage included the formulation and statement of the empowerment expansion, undertaken by workgroups at each of the three community programs, where goals and objectives for the empowerment expansion were defined, measurable indicators and measurement processes were identified, and action plans agreed upon.
- Stage III—comprised two parallel implementation processes:
- Empowerment expansion processes: these included numerous activities targeted on the development of the four ODCE domains (Table 2). These processes were debated on and formulated by the community that was being supported and facilitated and mediated by the health promotion practitioner and internal evaluator.
- Issue-specific processes: in which the guidelines for empowerment evaluation [39] were used, and four actions were undertaken;
- agreement on an issue-specific mission;
- taking stock (activities undertaken so far were assessed, listed, analyzed, and rated, and an evaluation matrix was developed).
- future planning (development of issue-specific goals and expected outcomes, and formulation of action plans). This step also included the selection of measurement tools, indicators and time-schedules for the issue-specific evaluation, i.e., creation of a system of processes and outcomes monitoring; and,
- implementation (including constant feedback and monitoring of issue-specific processes).
In Table 4, some activities that were undertaken by community workgroups during the issue-specific processes are presented. - Stage IV—evaluation of changes in the ODCE (and assessment of the ICRE, which is not within the scope of the current paper). Thus, the current study assessed whether there were any changes in ODCE in three community programs workgroups during the implementation of the empowerment expansion framework in the three community health promotion initiatives.
2.2. The Process on the Measurement of the ODCE
3. Findings of the Measurement of the ODCE
3.1. Safe Community Program
3.2. Drug Abuse and AIDS Prevention Program
3.3. Elderly Quality of Life Program
4. Discussion
5. Conclusions
Acknowledgments
References
- Minkler, M. Improving health through community organization and community building: A health education perspective. In Community Organizing & Community Building for Health; Minkler, M, Ed.; Rutgers University Press: London, UK, 2005; pp. 30–52. [Google Scholar]
- Wallerstein, N. What Is the Evidence of Effectiveness of Empowerment to Improve Health? WHO/EURO: Copenhagen, Denmark, 2006. [Google Scholar]
- Rappaport, J. In praise of paradox: a social policy of empowerment over prevention. Am. J. Commun. Psychol 1981, 9, 1–25. [Google Scholar]
- Minkler, M; Thompson, M; Bell, J; Rose, K. Contributions of Community Involvement to Organizational-Level Empowerment: The Federal Healthy Start Experience. Health Educ. Behav 2002, 28, 783–807. [Google Scholar]
- Tones, K; Tilford, S. Health Promotion: Effectiveness, Efficiency and Equity; Nelson Thornes Ltd: Cheltenham, UK, 2001; pp. 403–405. [Google Scholar]
- Labonte, R. Health promotion and empowerment: Reflections on professional practice. In Philosophical Foundations of Health Education; Black, JM, Furney, S, Graf, HM, Nolte, AE, Eds.; Jossey-Bass: San Francisco, CA, USA, 2010; pp. 179–195. [Google Scholar]
- World Health Organisation. Ottawa Charter for Health Promotion. 1986. Available online: http://www.who.int/hpr/NPH/docs/ottawa_charter_hp.pdf (accessed on 24 November 2010).
- van Uden-Kraan, CF; Drossaert, CHC; Taal, E; Shaw, B; Seydel, ER; van de Laar, MAFJ. Empowering processes and outcomes of participation in online support groups for patients with breast cancer, arthritis, or fibromyalgia. Qual. Health Res 2008, 18, 405–417. [Google Scholar]
- Mohan, V; Shanthirani, CS; Deepa, M; Datta, M; Williams, OD; Deepa, R. Community Empowerment—A Successful Model for Prevention of Non-communicable Diseases in India—The Chennai Urban Population Study (CUPS-17). J. Assoc. Phys. India 2006, 54, 858–862. [Google Scholar]
- Motohashi, Y; Kaneko, Y; Sasaki, H; Yamaji, M. A decrease in suicide rates in Japanese rural towns after community-based intervention by the health promotion approach. Suicide Life Threat.Behav 2007, 37, 593–599. [Google Scholar]
- Plough, A; Olafson, F. Implementing the Boston Healthy Start Initiative: A case study of community empowerment and public health. Health Edu. Q 1994, 21, 221–34. [Google Scholar]
- Geounuppakul, M; Butraporn, P; Kunstadter, P; Leemingsawat, S; Pacheun, O. An empowerment program to enhance women’s ability to prevent and control malaria in the community, Chiang Mai Province, Thailand. SE. Asian J. Trop. Med 2007, 38, 546–59. [Google Scholar]
- Wageman, R. How leaders foster self-managing team effectiveness: Design choices versus hands-on coaching. Organ. Sci 2001, 12, 559–577. [Google Scholar]
- Makara, P. Policy implications of differential health status in East and West Europe. The case of Hungary. Soc. Sci. Med 1994, 39, 1295–1302. [Google Scholar]
- Zimmerman, MA. Empowerment theory: Psychological, organizational and community levels of analysis. In Handbook of Community Psychology; Rappaport, J, Seidman, E, Eds.; Kluwer Academic/Plenum Publishers: New York, NY, USA, 2000; pp. 43–63. [Google Scholar]
- Swift, C; Levin, G. Empowerment: An emerging mental health technology. J. Prim. Prev 1987, 8, 71–94. [Google Scholar]
- Bernstein, E; Wallerstein, N; Braithwaite, R; Gutierrez, L; Labonte, R; Zimmerman, A. Empowerment forum: A dialogue between guest Editorial Board members. Health Educ. Q 1994, 21, 281–294. [Google Scholar]
- Rissel, C. Empowerment: the holy grail of health promotion? Health Promot. Int 1994, 9, 39–47. [Google Scholar]
- Laverack, G; Wallerstein, N. Measuring community empowerment: a fresh look at organizational domains. Health Promot. Int 2001, 16, 179–185. [Google Scholar]
- Minkler, M. Community organizing among the elderly poor in the United States: A case study. Int. J. Health Serv 1992, 22, 303–316. [Google Scholar]
- Fawcett, SB; Paine-Andrews, A; Francisco, VT; Schultz, JA; Richter, KP; Berkley-Patton, J; Fisher, JL; Lewis, RK; Lopez, CM; Russos, S; Williams, EL; Harris, KJ; Evensen, P. Evaluating community initiatives for health and development. In Evaluation in Health Promotion: Principles and Perspectives; Rootmann, I, Goodstadt, M, Hyndman, B, McQueen, DV, Potvin, L, Springhet, J, Ziglio, E, Eds.; WHO/EURO: Copenhagen, Denmark, 2001; pp. 241–270. [Google Scholar]
- Rich, MJ; Stoker, RP. Rethinking empowerment: Local empowerment zone programs. Urb. Aff. Rev 2009, 45, 775–796. [Google Scholar]
- Robertson, A; Minkler, N. New health promotion movement: A critical examination. In Philosophical Foundations of Health Education; Black, JM, Furney, S, Graf, HM, Nolte, AE, Eds.; Jossey-Bass: San Francisco, CA, USA, 2010; pp. 257–274. [Google Scholar]
- Geroy, GD; Wright, PC; Anderson, J. Strategic performance empowerment model. Empowerment Organ 1998, 6, 57–65. [Google Scholar]
- Laverack, G; Labonte, R. A planning framework for community empowerment goals within health promotion. Health Policy Plann 2000, 15, 255–262. [Google Scholar]
- Loewenson, R. Building voice and agency in health: public action within health systems. In Health, Economic Development and Household Poverty; Bennett, S, Gilson, L, Mills, L, Eds.; Routledge: London, UK, 2007; pp. 174–188. [Google Scholar]
- Keyser, BB; Broadbear, JT. The paradigm shift toward teaching for thinking: Perspectives, barriers, solutions and accountability. In Philosophical Foundations of Health Education; Black, JM, Furney, S, Graf, HM, Nolte, AM, Eds.; Jossey-Bass: San Francisco, CA, USA, 2010; pp. 109–118. [Google Scholar]
- Labonte, R; Laverack, G. Capacity building in health promotion, Part 2: Whose use? And with what measurement? Crit. Publ. Health 2001, 11, 128–138. [Google Scholar]
- Gibbon, M; Labonte, R; Laverack, G. Evaluating community capacity. Health Soc. Care Com 2002, 10, 485–491. [Google Scholar]
- Rapla County and Its People; Rapla Maavalitsus: Rapla, Estonia, 2002.
- Laverack, G. Addressing the Contradiction between Discourse and Practice in Health Promotion; PhD Thesis; Deakin University: Melbourne, Australia, 1999. [Google Scholar]
- Smith, N; Littlejohns, LBM; Roym, D. Measuring Community Capacity: State of the Field Review and Recommendations for Future Research; Research Report; David Thomson Health Region: Coronation, Canada, 2003. [Google Scholar]
- Hawe, P; King, L; Noort, M; Jordens, C; Lloyd, B. Indicators to Help with Capacity Building in Health Promotion; University of Sydney: Sydney, Australia, 2000. [Google Scholar]
- Bush, R; Dover, J; Mutch, A. Community Capacity Manual; University of Queensland: Melbourne, Australia, 2002. [Google Scholar]
- Gibbon, M; Labonte, R; Laverack, G. Evaluating community capacity. Health Soc. Care Com 2002, 10, 485–491. [Google Scholar]
- Bopp, J. Welcome to the swamp: Why assessing community capacity is fundamental to Ecohealth work. Eurohealth 2004, 1, 24–34. [Google Scholar]
- Luttrell, C; Quiroz, S; Scrutton, C; Bird, K. Understanding and Operationalising Empowerment; Overseas Development Institute: London, UK, 2009. [Google Scholar]
- Kasmel, A. Application of the empowerment evaluation model in community initiatives. In Book of Abstracts, 7th IUHPE Conference, Globalization and Equity: Consequences for Health Promotion Policies and Practices; Budapest, Hungary, 18–21 October 2006; Gabor, E, Ed.; NIHD: Budapest, Hungary, 2006.
- Foster-Fishman, PG; Berkowitz, SL; Lounsbury, DW; Jacobson, S; Allen, NA. Building collaborative capacity in community coalitions: A review and integrative framework. Am. J. Com. Psychol 2001, 29, 241–262. [Google Scholar]
- Fetterman, DM. Empowerment evaluation: an introduction to theory and practice. In Empowerment Evaluation: Knowledge and Tools for Self-Assessment and Accountability; Fetterman, DM, Kaftarian, SJ, Wandersman, A, Eds.; Sage: Thousand Oaks, CA, USA, 1996; pp. 3–46. [Google Scholar]
- Stanfield, RB. The Workshop Book: From Individual Creativity to Group Action; New Society Publishers: Cabriola Island, Canada, 2002. [Google Scholar]
- Robinson, KL; Elliott, SJ. The practice of community development approaches in heart health promotion. Health Educ. Res 2000, 15, 219–231. [Google Scholar]
- Laferty, CK; Mahoney, CA. A framework for evaluating comprehensive community initiatives. Health Promot. Pract 2003, 4, 31–44. [Google Scholar]
- Smyth, KF; Schorr, LP. A Lot To Lose: A Call to Rethink What Constitutes Evidence in Funding Social Interventions That Work; Working Paper Series; Harvard University: Cambridge, MA, USA, 2009. [Google Scholar]
- Fetterman, D; Deitz, J; Gesundheit, N. Empowerment evaluation: A collaborative approach to evaluating and transforming a medical school curriculum. Acad. Med 2010, 85, 813–820. [Google Scholar]
- Diaz-Puente, JM; Cazorla Montero, A; de los Rios Carmenado, I. Empowering communities through evaluation: Some lessons from rural Spain. Community Dev. J 2009, 44, 53–67. [Google Scholar]
- Goodman, RM; Noonan, RK. Empowerment evaluation for violence prevention public health programs. Health Promot. Pract 2009, 1, 11S–18S. [Google Scholar]
- Miller, W; Lennie, J. Empowerment Evaluation: A Practical Method for Evaluating a National School Breakfast Program. EJA 2009, 5, 18–26. [Google Scholar]
- Patton, MQ. Toward distinguishing empowerment evaluation and placing it in a larger context. Eval. Pract 1997, 18, 147–163. [Google Scholar]
- Scriven, M. Empowerment evaluation examined. Eval. Pract 1997, 18, 165–175. [Google Scholar]
- Crisp, BR; Swerissen, H; Duckett, SJ. Four approaches to capacity building in Health: Consequences for measurement and accountability. Health Promot. Int 2000, 15, 99–107. [Google Scholar]
- Krupka, DJ; Noonan, DS. Empowerment Zones, neighbourhood change and owner-occupied housing. Reg. Sci. Urban Econ 2009, 39, 386–396. [Google Scholar]
- Laverack, G. Public Health: Power, Empowerment and Professional Practice; Palgrave Macmillan: London, UK, 2009. [Google Scholar]


{kind=link}
| Laverack [31] | Smith et al. [32] | Hawe et al.[33] | Bopp et al. [36] | Gibbon [35] | Bush et al. [34] |
|---|---|---|---|---|---|
|
|
|
|
| Community Capacity Index
|
| Domain | Activities |
|---|---|
| Community Activation |
|
| Community Competence |
|
| Program management skills |
|
| Creation of supportive environment |
|
| I domain: Community activation Level 1 | Not at all/Very limited 1 | Somewhat 2 | Substantial 3 | Almost entirely/Entirely 4 |
|---|---|---|---|---|
| 1. There exists a group of community representatives that meets regularly to work on community goals and desired community outcomes. | ||||
| 2. The community group has an active leader(s), who motivates and enthuses members of group. | ||||
| 3. The community workgroup is committed to solving local problems and is motivated to collaborate as a team. | ||||
| I A community workgroup is constituted, which cares for community problems, have active leaders and is committed to collaborate in solving the community’s problems. | ||||
| Mean 2003 ........ | ||||
| Mean 2004 ........ | ||||
| Mean 2005 ........ | ||||
| Evidence describing the above mentioned assertions: | ||||
| 2003................................................................................................................................................................................ | ||||
| 2004................................................................................................................................................................................ | ||||
| 2005................................................................................................................................................................................ | ||||
| Community Initiative | Issue-Specific Activities |
|---|---|
| Safe Community |
|
| Drug Abuse and AIDS Prevention |
|
| Elderly Quality of Life |
|
| Community Initiative | Safe Community | Drug Abuse and AIDS Prevention | Elderly Quality of Life | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Year | 2003 | 2004 | 2005 | 2003 | 2004 | 2005 | 2003 | 2004 | 2005 |
| Male (N) | 7 | 8 | 8 | 8 | 8 | 8 | 0 | 0 | 0 |
| Female (N) | 9 | 12 | 9 | 6 | 6 | 7 | 15 | 18 | 17 |
| Total (N) | 16 | 20 | 17 | 14 | 14 | 15 | 15 | 18 | 17 |
| Age range (years) | 29–68 | 30–69 | 31–69 | 24–52 | 25–53 | 26–54 | 48–72 | 49–73 | 49–74 |
| Mean age (years) | 42.5 | 44.8 | 44.1 | 32.4 | 32.4 | 36.1 | 62.2 | 62.8 | 63.4 |
| Domain | Year 2003 N = 16 | Year 2004 N = 20 | Year 2005 N = 17 | |||
|---|---|---|---|---|---|---|
| Mean | Range | Mean | Range | Mean | Range | |
| Activation of the community | 1.96 | 1.3–2.6 | 2.53 | 2.0–3.3 | 3.20 | 2.6–4.0 |
| Competence of the community | 1.20 | 1.0–1.3 | 1.96 | 1.6–2.3 | 2.60 | 2.6–2.6 |
| Program management skills | 1.30 | 1.0–1.6 | 2.06 | 1.3–2.6 | 2.76 | 2.3–3.0 |
| Creation of a supportive environment | 1.13 | 1.0–1.3 | 1.63 | 1.3–2.0 | 2.30 | 2.0–2.6 |
| Domain | Year 2003 N = 14 | Year 2004 N = 14 | Year 2005 N = 15 | |||
|---|---|---|---|---|---|---|
| Mean | Range | Mean | Range | Mean | Range | |
| Activation of the community | 1.63 | 1.0–2.6 | 2.53 | 2.0–3.3 | 3.20 | 2.6–4.0 |
| Competence of the community | 1.20 | 1.0–1.3 | 1.96 | 1.6–2.3 | 2.6 | 2.6–2.6 |
| Program management skills | 1.30 | 1.0–1.6 | 2.06 | 1.3–2.6 | 2.76 | 2.3–3.0 |
| Creation of a supportive environment | 1.10 | 1.0–1.3 | 1.96 | 1.3–2.0 | 2.30 | 2.0–2.6 |
| Domain | Year 2003 N = 15 | Year 2004 N = 18 | Year 2005 N = 17 | |||
|---|---|---|---|---|---|---|
| Mean | Range | Mean | Range | Mean | Range | |
| Activation of the community | 1.63 | 1.3–2.0 | 2.43 | 2.0–3.0 | 2.73 | 2.6–3.0 |
| Competence of the community | 1.66 | 1.0–2.0 | 2.20 | 2.0–2.3 | 2.30 | 2.0–2.6 |
| Program management skills | 1.10 | 1.0–1.3 | 1.96 | 1.6–2.3 | 2.30 | 2.3–3.6 |
| Creation of a supportive environment | 1.63 | 1.0–2.6 | 2.16 | 1.3–2.6 | 1.63 | 1.3–2.0 |
© 2011 by the authors; licensee MDPI, Basel, Switzerland This article is an open-access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Kasmel, A.; Andersen, P.T. Measurement of Community Empowerment in Three Community Programs in Rapla (Estonia). Int. J. Environ. Res. Public Health 2011, 8, 799-817. https://doi.org/10.3390/ijerph8030799
Kasmel A, Andersen PT. Measurement of Community Empowerment in Three Community Programs in Rapla (Estonia). International Journal of Environmental Research and Public Health. 2011; 8(3):799-817. https://doi.org/10.3390/ijerph8030799
Chicago/Turabian StyleKasmel, Anu, and Pernille Tanggaard Andersen. 2011. "Measurement of Community Empowerment in Three Community Programs in Rapla (Estonia)" International Journal of Environmental Research and Public Health 8, no. 3: 799-817. https://doi.org/10.3390/ijerph8030799
APA StyleKasmel, A., & Andersen, P. T. (2011). Measurement of Community Empowerment in Three Community Programs in Rapla (Estonia). International Journal of Environmental Research and Public Health, 8(3), 799-817. https://doi.org/10.3390/ijerph8030799