Complications Following Irinotecan-Loaded Microsphere Chemoembolization of Colorectal Metastatic Liver Lesions Associated with Hepatic-Artery Branch Temporary Stasis


Abstract
:1. Introduction
Objectives
2. Materials and Methods
2.1. Procedure
- Grade 1: no stasis. No visible embolizate retention (or only in areas visible at tumor supply vessel level).
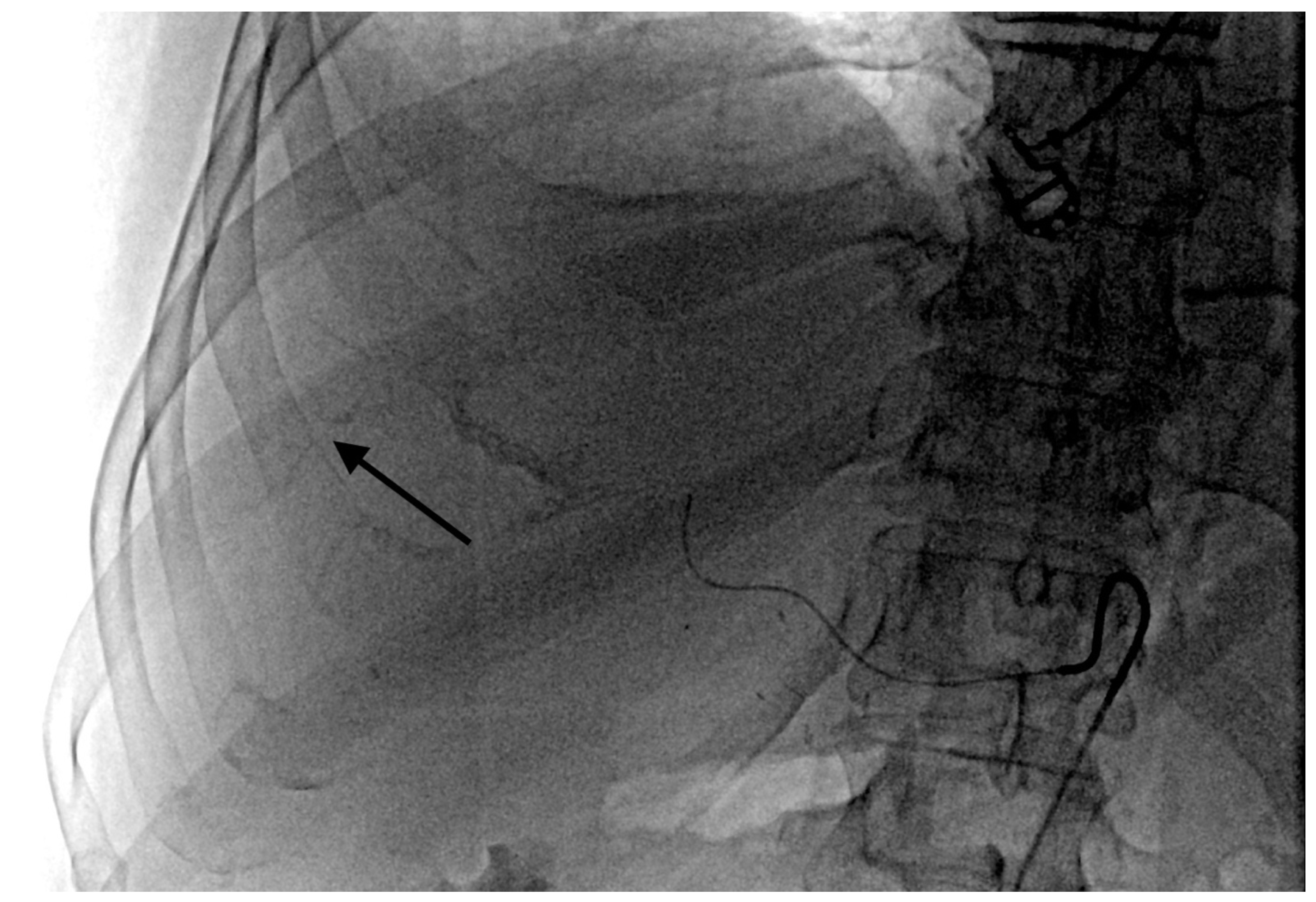
- Grade 2 stasis. Embolizate contrast at the level of tumor supply vessels (Figure 2).
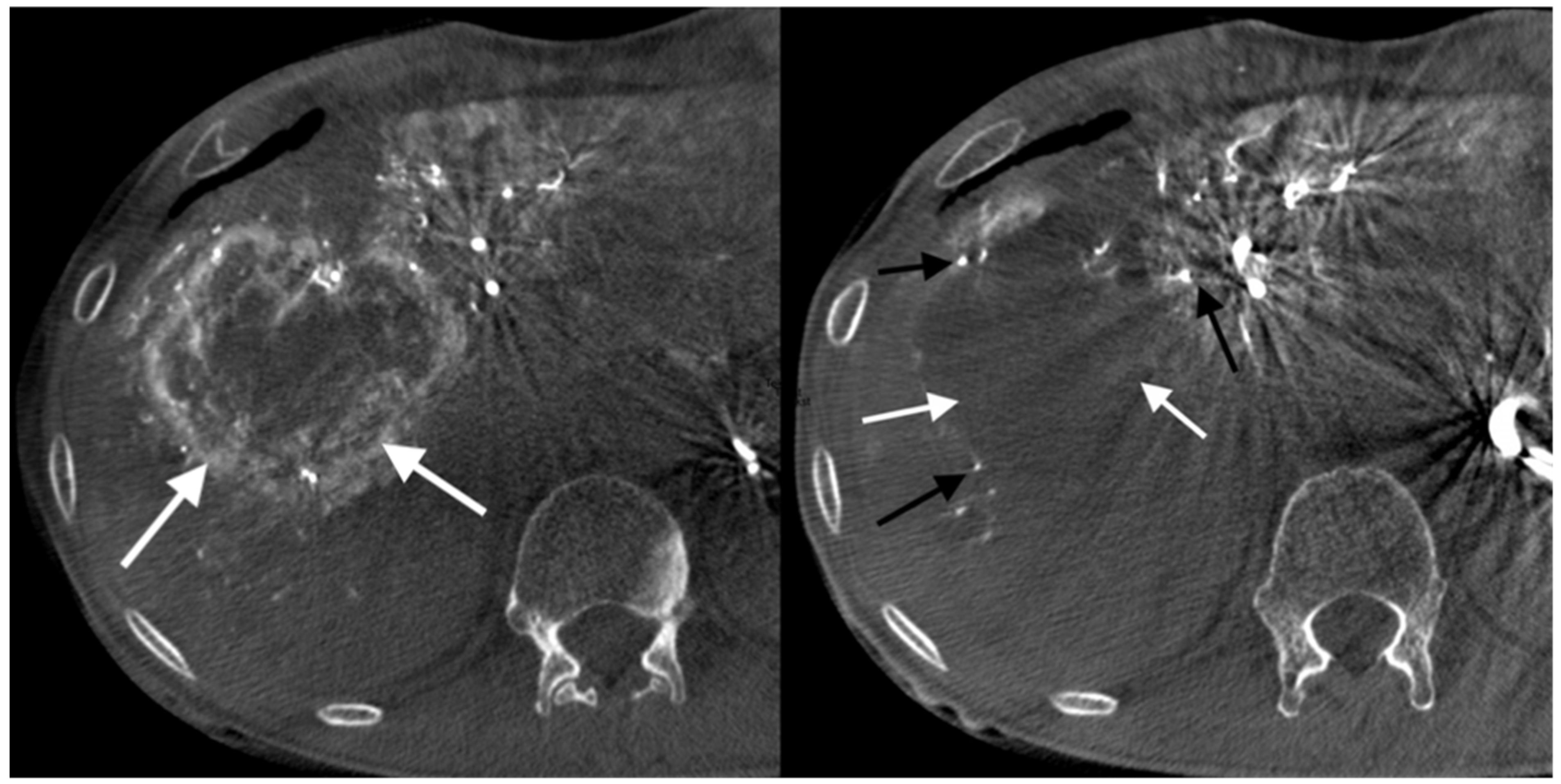
- Grade 3 stasis. Embolizate contrast in subsegmental vessels (Figure 3).
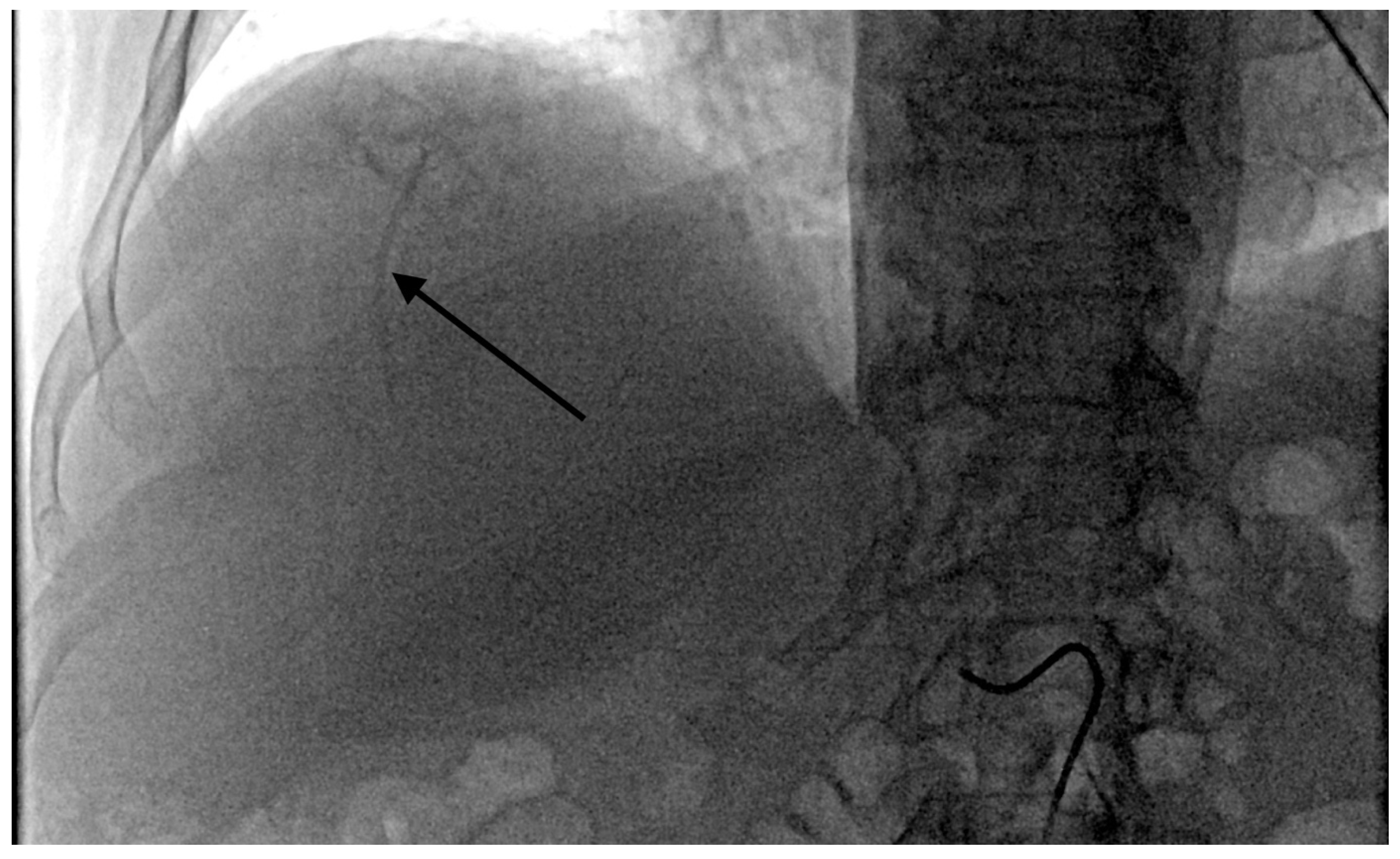
- Grade 4 stasis. Embolizate contrast in segmental vessels (Figure 4).
2.2. Adverse Event Assessment
- 0:
- no symptoms of post-embolization syndrome.
- 1:
- moderately severe post-embolization syndrome, not requiring additional treatment: moderate pain (1–5 points; pain scale given above), and increased body temperature up to 38 °C.
- 2:
- severe post-embolization syndrome requiring additional treatment: severe pain (6–10 points), fever over 38 °C, nausea, and vomiting.
2.3. Statistical Analyses
3. Results
3.1. Patient Characteristics
3.2. Chemoembolization
3.3. Adverse Events
4. Discussion
5. Conclusions
Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Slesser, A.A.; Georgiou, P.; Brown, G.; Mudan, S.; Goldin, R.; Tekkis, P. The tumour biology of synchronous and metachronous colorectal liver metastases: A systematic review. Clin. Exp. Metastasis 2013, 30, 457–470. [Google Scholar] [CrossRef]
- Ruers, T.; Bleichrodt, R.P. Treatment of liver metastases, an update on the possibilities and results. Eur. J. Cancer 2002, 38, 1023–1033. [Google Scholar] [CrossRef]
- Reddy, S.K.; Pawlik, T.M.; Zorzi, D.; Gleisner, A.L.; Ribero, D.; Assumpcao, L.; Barbas, A.S.; Abdalla, E.K.; Choti, M.A.; Vauthey, J.N. Simultaneous resections of colorectal cancer and synchronous liver metastases: A multi-institutional analysis. Ann. Surg. Oncol. 2007, 14, 3481–3491. [Google Scholar] [CrossRef]
- Fiorentini, G.; Aliberti, C.; Tilli, M.; Mulazzani, L.; Graziano, F.; Giordani, P.; Mambrini, A.; Montagnani, F.; Alessandroni, P.; Catalano, V.; et al. Intra-arterial infusion of irinotecan-loaded drug eluting beads (DEBIRI) versus intravenous therapy (FOLFIRI) forhepatic metastases from colorectal cancer: Final results of a phase III study. Anticancer Res. 2012, 32, 1387–1395. [Google Scholar]
- Vogl, T.J.; Zangos, S.; Eichler, K.; Yakoub, D.; Nabil, M. Colorectal liver metastases: Regional chemotherapy via transarterial chemoembolization (TACE) and hepatic chemoperfusion: An update. Eur. Radiol. 2007, 17, 1025–1034. [Google Scholar] [CrossRef]
- Hagan, A.; Caine, M.; Press, C.; Macfarlane, W.; Phillips, G.; Lloyd, A.; Czuczman, P.; Kilpatrick, H.; Bascal, Z.; Tang, Y.; et al. Predicting pharmacokinetic behaviour of drug release from drug-eluting embolization beads using in vitro elution methods. Eur. J. Pharm. Sci. 2019, 136, 1–24. [Google Scholar] [CrossRef]
- Tan, K.T.; Rakheja, R.; Plewes, C.; Mondal, P.; Lim, H.; Ahmed, S.; Lee, E.; Otani, R.; Luo, Y.; Shaw, J.; et al. Does Tumour Contrast Retention on CT Immediately Post Chemoembolization Predict Tumour Metabolic Response on FDG-PET in Patients with Hepatic Metastases from Colorectal Cancer? Gastroenterol. Res. Pract. 2019, 4, 7279163. [Google Scholar] [CrossRef] [Green Version]
- Kauffels, A.; Kitzmüller, M.; Gruber, A.; Nowack, H.; Bohnenberger, H.; Spitzner, M.; Kuthning, A.; Sprenger, T.; Czejka, M.; Ghadimi, M.; et al. Hepatic arterial infusion of irinotecan and EmboCept® S results in high tumor concentration of SN-38 in a rat model of colorectal liver metastases. Clin. Exp. Metastasis 2019, 36, 57–66. [Google Scholar] [CrossRef]
- Richardson, A.J.; Laurence, J.M.; Lam, V.W. Transarterial chemoembolization with irinotecan beads in the treatment of colorectal liver metastases: Systematic review. J. Vasc. Interv. Radiol. 2013, 24, 1209–1217. [Google Scholar] [CrossRef]
- Martin, R.C.; Joshi, J.; Robbins, K.; Tomalty, D.; Bosnjakovik, P.; Derner, M.; Padr, R.; Rocek, M.; Scupchenko, A.; Tatum, C. Hepatic intra-arterial injection of drug-eluting bead, irinotecan (DEBIRI) in unresectable colorectal liver metastases refractory to systemic chemotherapy: Results of multi-institutional study. Ann. Surg. Oncol. 2011, 18, 192–198. [Google Scholar] [CrossRef]
- Malagari, K.; Pomoni, M.; Moschouris, H.; Bouma, E.; Koskinas, J.; Stefaniotou, A.; Marinis, A.; Kelekis, A.; Alexopoulou, E.; Chatziioannou, A.; et al. Chemoembolization with doxorubicin-eluting beads for unresectable hepatocellularcarcinoma: Five-year survival analysis. Cardiovasc. Intervent. Radiol. 2012, 35, 1119–1128. [Google Scholar] [CrossRef] [PubMed]
- Aliberti, C.; Carandina, R.; Lonardi, S.; Dadduzio, V.; Vitale, A.; Gringeri, E.; Zanus, G.; Cillo, U. Transarterial chemoembolization with small drug-eluting beads in patients with hepatocellular carcinoma: Experience from a cohort of 421 patients at an Italian center. J. Vasc. Interv. Radiol. 2017, 28, 1495–1502. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.; Chung, J.W.; Lee, K.H.; Won, J.Y.; Chun, H.J.; Lee, H.C.; Kim, J.C.; Lee, I.J.; Hur, S.; Kim, H.-C.; et al. Korean multicenter registry of transcatheter arterial chemoembolization with drug-eluting embolic agents for nodular hepatocellular carcinomas: Six-month outcome analysis. J. Vasc. Interv. Radiol. 2017, 28, 502–512. [Google Scholar] [CrossRef]
- Popovic, P.; Stabuc, B.; Jansa, R.; Garbajs, M. Survival of patients with intermediate stage hepatocellular carcinoma treated with superselective transarterial chemoembolization using doxorubicin-loaded DC Bead under cone-beam computed tomography control. Radiol. Oncol. 2016, 50, 418–426. [Google Scholar] [CrossRef] [Green Version]
- Chung, J.W.; Park, J.H.; Han, J.K.; Choi, B.I.; Han, M.C.; Lee, H.S.; Kim, C.Y. Hepatic tumors: Predisposing factors for complications of transcatheter oily chemoembolization. Radiology 1996, 198, 33–40. [Google Scholar] [CrossRef]
- Dhand, S.; Gupta, R. Hepatic transcatheter arterial chemoembolization complicated by postembolization syndrome. Semin. Intervent. Radiol. 2011, 28, 207–211. [Google Scholar] [CrossRef] [Green Version]
- Hatamaru, K.; Azuma, S.; Akamatsu, T.; Seta, T.; Urai, S.; Uenoyama, Y.; Yamashita, Y.; Ono, K. Pulmonary embolism after arterial chemoembolization for hepatocellular carcinoma: An autopsy case report. World J. Gastroenterol. 2015, 21, 1344–1348. [Google Scholar] [CrossRef]
- Sag, A.A.; Selcukbiricik, F.; Mandel, N.M. Evidence-based medical oncology and interventional radiology paradigms for liver-dominant colorectal cancer metastases. World J. Gastroenterol. 2016, 22, 3127–3149. [Google Scholar] [CrossRef] [PubMed]
- Schicho, A.; Hellerbrand, C.; Krüger, K.; Beyer, L.P.; Wohlgemuth, W.; Niessen, C.; Hohenstein, E.; Stroszczynski, C.; Pereira, P.L.; Wiggermann, P. Impact of Different Embolic Agents for Transarterial Chemoembolization (TACE) Procedures on Systemic Vascular Endothelial Growth Factor (VEGF) Levels. J. Clin. Transl. Hepatol. 2016, 4, 288–292. [Google Scholar]
- Li, X.; Feng, G.S.; Zheng, C.S.; Zhuo, C.K.; Liu, X. Expression of plasma vascular endothelial growth factor in patients with hepatocellular carcinoma and effect of transcatheter arterial chemoembolization therapy on plasma vascular endothelial growth factor level. World J. Gastroenterol. 2004, 10, 2878–2882. [Google Scholar] [CrossRef]
- Poon, R.T.; Lau, C.; Yu, W.C.; Fan, S.T.; Wong, J. High serum levels of vascular endothelial growth factor predict poor response to transarterial chemoembolization in hepatocellular carcinoma: A prospective study. Oncol. Rep. 2004, 11, 1077–1084. [Google Scholar] [CrossRef]
- Brooks, A.J.; Hammond, J.S.; Girling, K.; Beckingham, I.J. The effect of hepatic vascular inflow occlusion on liver tissue pH, carbon dioxide, and oxygen partial pressures: Defining the optimal clamp/release regime for intermittent portal clamping. J. Surg. Res. 2007, 141, 247–251. [Google Scholar] [CrossRef]
- Tanaka, T.; Nishiofuku, H.; Hukuoka, Y.; Sato, T.; Masada, T.; Takano, M.; Gilbert, C.W.; Obayashi, C.; Kichikawa, K. Pharmacokinetics and antitumorefficacy of chemoembolization using 40μm irinotecan-loaded microspheresin a rabbit liver tumor model. J. Vasc. Interv. Radiol. 2014, 25, 1037–1044. [Google Scholar] [CrossRef] [PubMed]
- Xu, G.; Zhang, W.; Ma, M.K.; McLeod, H.L. Human carboxylesterase 2 is commonly expressed in tumor tissue and is correlated withactivation of irinotecan. Clin. Cancer Res. 2002, 8, 2605–2611. [Google Scholar]
- Gaudio, E.; Franchitto, A.; Pannarale, L.; Carpino, G.; Alpini, G.; Francis, H.; Glaser, S.; Alvaro, D.; Onori, P. Cholangiocytes and blood supply. World J. Gastroenterol. 2006, 14, 3546–3552. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Value |
|---|---|
| Number of patients | 52 |
| Age, median (range) | 67.3 (32–83) |
| Gender, male/female (n) | 23/29 |
| ECOG status: 0/1 (n) | 38/14 |
| Colon/rectal cancer (n) | 40/12 |
| Bilobar/unilobar metastases (n) | 41/11 |
| Number of liver metastases, median (range) | 5.4 (1–14) |
| Extent of liver involvement (n, <25%/>25%) | 47/5 |
| Extrahepatic metastasis (n, %) | 6 (11.5%) |
| Number of lines of prior systemic chemotherapy: | |
| (number of patients) | |
| None | 0 |
| 1 | 11 |
| 2 | 30 |
| 3 | 11 |
| Prior liver surgery/ablation (n) | 7/0 |
| Prior locoregional therapy (n) | 0 |
| Parameter | Value |
|---|---|
| Total number of treatments (n) | 202 |
| Number of treatments per patient: mean (range) | 3.88 (1–8) |
| Treatment location (n): | |
| Right | 94 |
| Left | 108 |
| Branch level selected (n): | |
| Lobar | 29 |
| Segmental | 75 |
| Subsegmental | 91 |
| Branch level with temporary stasis (n): | |
| No stasis/tumor retention only | 36 |
| Tumor supply vessel | 65 |
| Subsegmental branch(es) | 79 |
| Segmental branch(es) | 22 |
| Branch Level of Stasis | Total Number of Treatments (n) | PES Symptoms (Number of Treatments) | ||
|---|---|---|---|---|
| None | Mild | Severe | ||
| No stasis or tumor retention only | 36 | 32 | 2 | 2 |
| Tumor supply vessel | 65 | 39 | 24 | 2 |
| Sub-segmental artery | 79 | 25 | 39 | 15 |
| Segmental artery | 22 | 3 | 8 | 11 |
| Branch Level of Stasis | PES Mean Severity * |
|---|---|
| No stasis or tumor retention only | 1.17 |
| Tumor supply artery | 1.26 |
| Sub-segmental | 1.55 |
| Segmental | 1.72 |
| Total PES mean | 1.425 |
| Number and Grades of Adverse Events | |||
|---|---|---|---|
| Branch level of stasis | Adverse events grade | Total | |
| G 2 | G 3 | ||
| No stasis/tumor retention only | 0 | 1 | 1 |
| Tumor supply vessel | 2 | 1 | 3 |
| Subsegmental artery | 2 | 1 | 3 |
| Segmental artery | 4 | 4 | 8 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Szemitko, M.; Golubinska-Szemitko, E.; Sienko, J.; Falkowski, A. Complications Following Irinotecan-Loaded Microsphere Chemoembolization of Colorectal Metastatic Liver Lesions Associated with Hepatic-Artery Branch Temporary Stasis. Curr. Oncol. 2021, 28, 2296-2307. https://doi.org/10.3390/curroncol28030211
Szemitko M, Golubinska-Szemitko E, Sienko J, Falkowski A. Complications Following Irinotecan-Loaded Microsphere Chemoembolization of Colorectal Metastatic Liver Lesions Associated with Hepatic-Artery Branch Temporary Stasis. Current Oncology. 2021; 28(3):2296-2307. https://doi.org/10.3390/curroncol28030211
Chicago/Turabian StyleSzemitko, Marcin, Elzbieta Golubinska-Szemitko, Jerzy Sienko, and Aleksander Falkowski. 2021. "Complications Following Irinotecan-Loaded Microsphere Chemoembolization of Colorectal Metastatic Liver Lesions Associated with Hepatic-Artery Branch Temporary Stasis" Current Oncology 28, no. 3: 2296-2307. https://doi.org/10.3390/curroncol28030211
APA StyleSzemitko, M., Golubinska-Szemitko, E., Sienko, J., & Falkowski, A. (2021). Complications Following Irinotecan-Loaded Microsphere Chemoembolization of Colorectal Metastatic Liver Lesions Associated with Hepatic-Artery Branch Temporary Stasis. Current Oncology, 28(3), 2296-2307. https://doi.org/10.3390/curroncol28030211