Renal and Salivary Gland Functions after Three Cycles of PSMA-617 Therapy Every Four Weeks in Patients with Metastatic Castration-Resistant Prostate Cancer

 ,
,  , ,
, ,  , ,
, , 
Abstract
:1. Introduction
2. Methods
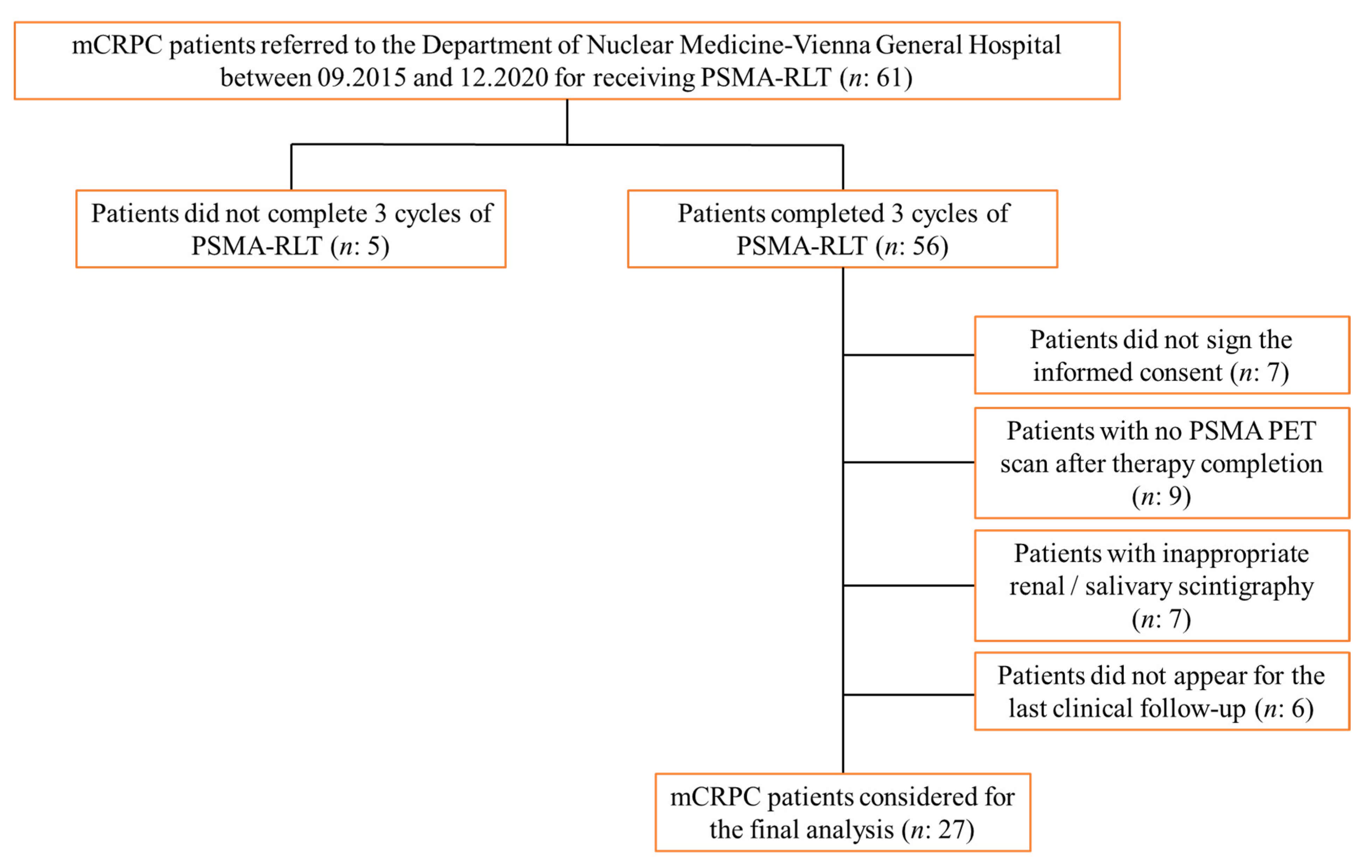
2.1. Study Population
2.2. [177Lu]Lu-PSMA-617 Radioligand Therapy
2.3. Salivary Gland Scintigraphy
2.4. Kidney Scintigraphy
2.5. PSMA-PET Imaging
2.6. Statistical Analysis
3. Results
3.1. Study Population
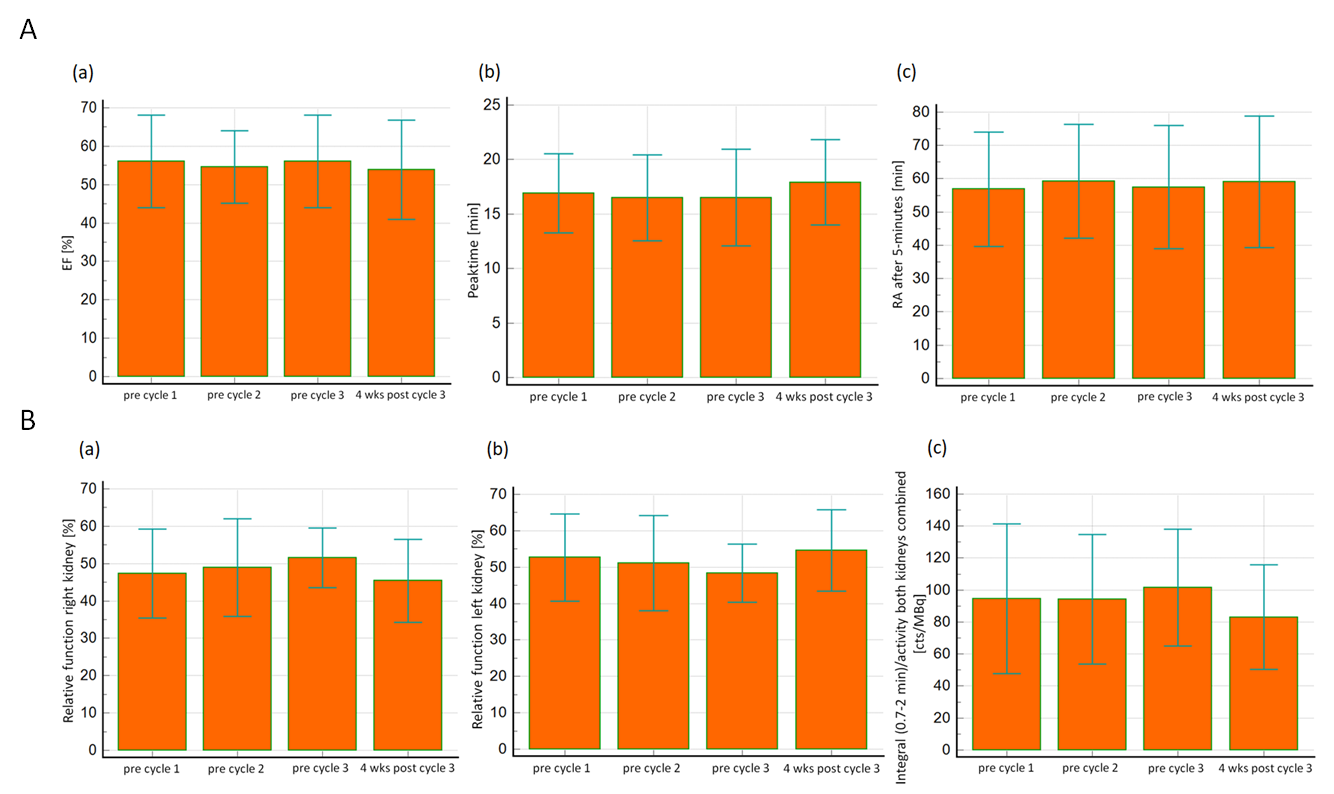
3.2. Salivary Gland Scintigraphy
3.3. Kidney Function and Scintigraphy
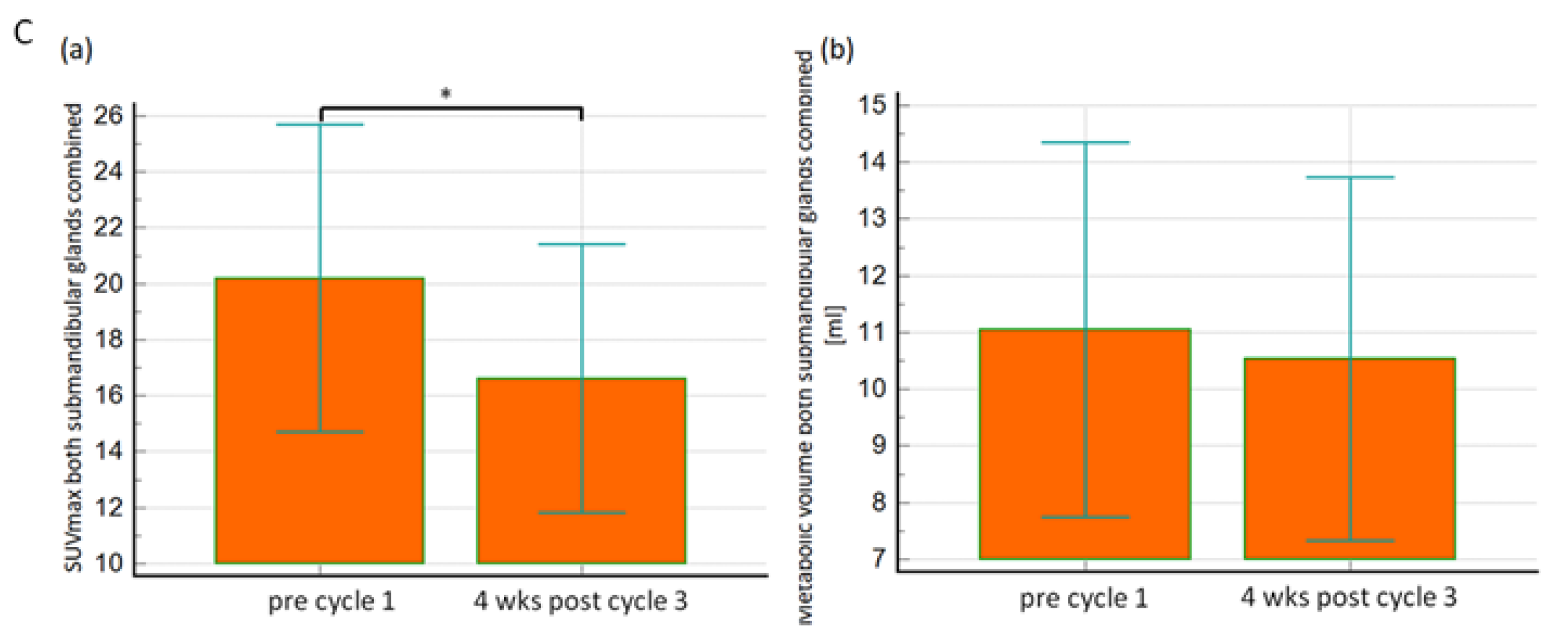
3.4. [68Ga]Ga-PSMA PET Imaging
3.5. Questionnaire
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Sweat, S.D.; Pacelli, A.; Murphy, G.P.; Bostwick, D.G. Prostate-specific membrane antigen expression is greatest in prostate adenocarcinoma and lymph node metastases. Urology 1998, 52, 637–640. [Google Scholar] [CrossRef]
- Ghosh, A.; Heston, W.D. Tumor target prostate specific membrane antigen (PSMA) and its regulation in prostate cancer. J. Cell. Biochem. 2004, 91, 528–539. [Google Scholar] [CrossRef]
- O’Keefe, D.S.; Bacich, D.J.; Huang, S.S.; Heston, W.D. A Perspective on the Evolving Story of PSMA Biology, PSMA-Based Imaging, and Endoradiotherapeutic Strategies. J. Nucl. Med. 2018, 59, 1007–1013. [Google Scholar] [CrossRef] [PubMed]
- Silver, D.A.; Pellicer, I.; Fair, W.R.; Heston, W.D.; Cordon-Cardo, C. Prostate-specific membrane antigen expression in normal and malignant human tissues. Clin. Cancer Res. 1997, 3, 81–85. [Google Scholar] [PubMed]
- Bostwick, D.G.; Pacelli, A.; Blute, M.; Roche, P.; Murphy, G.P. Prostate specific membrane antigen expression in prostatic intraepithelial neoplasia and adenocarcinoma: A study of 184 cases. Cancer 1998, 82, 2256–2261. [Google Scholar] [CrossRef]
- Hillier, S.M.; Maresca, K.P.; Lu, G.; Merkin, R.D.; Marquis, J.C.; Zimmerman, C.N.; Eckelman, W.C.; Joyal, J.L.; Babich, J.W. 99mTc-labeled small-molecule inhibitors of prostate-specific membrane antigen for molecular imaging of prostate cancer. J. Nucl. Med. 2013, 54, 1369–1376. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eder, M.; Schäfer, M.; Bauder-Wüst, U.; Hull, W.-E.; Wängler, C.; Mier, W.; Haberkorn, U.; Eisenhut, M. 68Ga-Complex Lipophilicity and the Targeting Property of a Urea-Based PSMA Inhibitor for PET Imaging. Bioconjug. Chem. 2012, 23, 688–697. [Google Scholar] [CrossRef] [PubMed]
- Weineisen, M.; Schottelius, M.; Simecek, J.; Baum, R.P.; Yildiz, A.; Beykan, S.; Kulkarni, H.R.; Lassmann, M.; Klette, I.; Eiber, M.; et al. 68Ga- and 177Lu-Labeled PSMA I&T: Optimization of a PSMA-Targeted Theranostic Concept and First Proof-of-Concept Human Studies. J. Nucl. Med. 2015, 56, 1169–1176. [Google Scholar]
- Mease, R.C.; Dusich, C.L.; Foss, C.A.; Ravert, H.T.; Dannals, R.F.; Seidel, J.; Prideaux, A.; Fox, J.J.; Sgouros, G.; Kozikowski, A.P.; et al. N-[N-[(S)-1,3-Dicarboxypropyl]Carbamoyl]-4-[18F]Fluorobenzyl-l-Cysteine, [18F]DCFBC: A New Imaging Probe for Prostate Cancer. Clin. Cancer Res. 2008, 14, 3036–3043. [Google Scholar] [CrossRef] [Green Version]
- Kratochwil, C.; Bruchertseifer, F.; Giesel, F.L.; Weis, M.; Verburg, F.A.; Mottaghy, F.; Kopka, K.; Apostolidis, C.; Haberkorn, U.; Morgenstern, A. 225Ac-PSMA-617 for PSMA-Targeted α-Radiation Therapy of Metastatic Castration-Resistant Prostate Cancer. J. Nucl. Med. 2016, 57, 1941–1944. [Google Scholar] [CrossRef] [Green Version]
- Rice, M.; Malhotra, S.V.; Stoyanova, T. Second-Generation Antiandrogens: From Discovery to Standard of Care in Castration Resistant Prostate Cancer. Front. Oncol. 2019, 9, 801. [Google Scholar] [CrossRef]
- Nuhn, P.; De Bono, J.S.; Fizazi, K.; Freedland, S.J.; Grilli, M.; Kantoff, P.W.; Sonpavde, G.; Sternberg, C.N.; Yegnasubramanian, S.; Antonarakis, E.S. Update on Systemic Prostate Cancer Therapies: Management of Metastatic Castration-resistant Prostate Cancer in the Era of Precision Oncology. Eur. Urol. 2018, 75, 88–99. [Google Scholar] [CrossRef] [PubMed]
- Nguyen-Nielsen, M.; Borre, M. Diagnostic and Therapeutic Strategies for Prostate Cancer. Semin. Nucl. Med. 2016, 46, 484–490. [Google Scholar] [CrossRef] [PubMed]
- Hofman, M.S.; Emmett, L.; Sandhu, S.; Iravani, A.; Joshua, A.M.; Goh, J.C.; Pattison, D.A.; Tan, T.H.; Kirkwood, I.D.; Ng, S.; et al. [(177)Lu]Lu-PSMA-617 versus cabazitaxel in patients with metastatic castration-resistant prostate cancer (TheraP): A randomised, open-label, phase 2 trial. Lancet 2021, 397, 797–804. [Google Scholar] [CrossRef]
- Novartis Announces Positive Result of Phase III Study with Radioligand Therapy 177Lu-PSMA-617 in Patients with Advanced Prostate Cancer. Available online: https://bit.ly/3ce0zCQ (accessed on 23 March 2021).
- Rahbar, K.; Ahmadzadehfar, H.; Kratochwil, C.; Haberkorn, U.; Schäfers, M.; Essler, M.; Baum, R.P.; Kulkarni, H.R.; Schmidt, M.; Drzezga, A.; et al. German Multicenter Study Investigating 177Lu-PSMA-617 Radioligand Therapy in Advanced Prostate Cancer Patients. J. Nucl. Med. 2017, 58, 85–90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bräuer, A.; Grubert, L.S.; Roll, W.; Schrader, A.J.; Schäfers, M.; Bögemann, M.; Rahbar, K. 177Lu-PSMA-617 radioligand therapy and outcome in patients with metastasized castration-resistant prostate cancer. Eur. J. Nucl. Med. Mol. Imaging 2017, 44, 1663–1670. [Google Scholar] [CrossRef] [PubMed]
- Kratochwil, C.; Giesel, F.L.; Eder, M.; Afshar-Oromieh, A.; Benešová, M.; Mier, W.; Kopka, K.; Haberkorn, U. [177Lu]Lutetium-labelled PSMA ligand-induced remission in a patient with metastatic prostate cancer. Eur. J. Nucl. Med. Mol. Imaging 2015, 42, 987–988. [Google Scholar] [CrossRef] [PubMed]
- Rahbar, K.; Boegemann, M.; Yordanova, A.; Eveslage, M.; Schäfers, M.; Essler, M.; Ahmadzadehfar, H. PSMA targeted radioligandtherapy in metastatic castration resistant prostate cancer after chemotherapy, abiraterone and/or enzalutamide. A retrospective analysis of overall survival. Eur. J. Nucl. Med. Mol. Imaging 2017, 45, 12–19. [Google Scholar] [CrossRef]
- O’Keefe, D.S.; Bacich, D.J.; Heston, W.D. Comparative analysis of prostate-specific membrane antigen (PSMA) versus a prostate-specific membrane antigen-like gene. Prostate 2004, 58, 200–210. [Google Scholar] [CrossRef]
- Tönnesmann, R.; Meyer, P.T.; Eder, M.; Baranski, A.-C. [177Lu]Lu-PSMA-617 Salivary Gland Uptake Characterized by Quantitative In Vitro Autoradiography. Pharmaceuticals 2019, 12, 18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yordanova, A.; Becker, A.; Eppard, E.; Kürpig, S.; Fisang, C.; Feldmann, G.; Essler, M.; Ahmadzadehfar, H. The impact of repeated cycles of radioligand therapy using [177Lu]Lu-PSMA-617 on renal function in patients with hormone refractory metastatic prostate cancer. Eur. J. Nucl. Med. Mol. Imaging 2017, 44, 1473–1479. [Google Scholar] [CrossRef]
- Delker, A.; Fendler, W.P.; Kratochwil, C.; Brunegraf, A.; Gosewisch, A.; Gildehaus, F.J.; Tritschler, S.; Stief, C.G.; Kopka, K.; Haberkorn, U.; et al. Dosimetry for 177Lu-DKFZ-PSMA-617: A new radiopharmaceutical for the treatment of metastatic prostate cancer. Eur. J. Nucl. Med. Mol. Imaging 2015, 43, 42–51. [Google Scholar] [CrossRef] [PubMed]
- Kabasakal, L.; Abuqbeitah, M.; Aygün, A.; Yeyin, N.; Ocak, M.; Demirci, E.; Toklu, T. Pre-therapeutic dosimetry of normal organs and tissues of 177Lu-PSMA-617 prostate-specific membrane antigen (PSMA) inhibitor in patients with castration-resistant prostate cancer. Eur. J. Nucl. Med. Mol. Imaging 2015, 42, 1976–1983. [Google Scholar] [CrossRef] [PubMed]
- Özkan, A.; Uçar, B.; Seymen, H.; Yarar, Y.Y.; Falay, F.O.; Demirkol, M.O. Posttherapeutic Critical Organ Dosimetry of Extensive 177Lu-PSMA Inhibitor Therapy With Metastatic Castration-Resistant Prostate Cancer: One Center Results. Clin. Nucl. Med. 2020, 45, 288–291. [Google Scholar] [CrossRef]
- Kratochwil, C.; Giesel, F.L.; Stefanova, M.; Benešová, M.; Bronzel, M.; Afshar-Oromieh, A.; Mier, W.; Eder, M.; Kopka, K.; Haberkorn, U. PSMA-Targeted Radionuclide Therapy of Metastatic Castration-Resistant Prostate Cancer with 177Lu-Labeled PSMA-617. J. Nucl. Med. 2016, 57, 1170–1176. [Google Scholar] [CrossRef] [Green Version]
- Yadav, M.P.; Ballal, S.; Sahoo, R.K.; Dwivedi, S.N.; Bal, C. Radioligand Therapy With 177Lu-PSMA for Metastatic Castration-Resistant Prostate Cancer: A Systematic Review and Meta-Analysis. Am. J. Roentgenol. 2019, 213, 275–285. [Google Scholar] [CrossRef] [PubMed]
- Rasul, S.; Hacker, M.; Kretschmer-Chott, E.; Leisser, A.; Grubmüller, B.; Kramer, G.; Shariat, S.; Wadsak, W.; Mitterhauser, M.; Hartenbach, M.; et al. Clinical outcome of standardized 177Lu-PSMA-617 therapy in metastatic prostate cancer patients receiving 7400 MBq every 4 weeks. Eur. J. Nucl. Med. Mol. Imaging 2019, 47, 713–720. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rasul, S.; Hartenbach, M.; Wollenweber, T.; Kretschmer-Chott, E.; Grubmüller, B.; Kramer, G.; Shariat, S.; Wadsak, W.; Mitterhauser, M.; Pichler, V.; et al. Prediction of response and survival after standardized treatment with 7400 MBq 177Lu-PSMA-617 every 4 weeks in patients with metastatic castration-resistant prostate cancer. Eur. J. Nucl. Med. Mol. Imaging 2020, 48, 1650–1657. [Google Scholar] [CrossRef]
- Ahmadzadehfar, H.; Rahbar, K.; Kürpig, S.; Bögemann, M.; Claesener, M.; Eppard, E.; Gärtner, F.; Rogenhofer, S.; Schäfers, M.; Essler, M. Early side effects and first results of radioligand therapy with 177Lu-DKFZ-617 PSMA of castrate-resistant metastatic prostate cancer: A two-centre study. EJNMMI Res. 2015, 5, 114. [Google Scholar] [CrossRef] [Green Version]
- Rasul, S.; Wollenweber, T.; Zisser, L.; Kretschmer-Chott, E.; Grubmüller, B.; Kramer, G.; Shariat, S.; Eidherr, H.; Mitterhauser, M.; Vraka, C.; et al. Response and Toxicity to the Second Course of 3 Cycles of 177Lu-PSMA Therapy Every 4 Weeks in Patients with Metastatic Castration-Resistant Prostate Cancer. Cancers 2021, 13, 2489. [Google Scholar] [CrossRef] [PubMed]
- Shizukuishi, K.; Nagaoka, S.; Kinno, Y.; Saito, M.; Takahashi, N.; Kawamoto, M.; Abe, A.; Jin, L.; Inoue, T. Scoring analysis of salivary gland scintigraphy in patients with Sjögren’s syndrome. Ann. Nucl. Med. 2003, 17, 627–631. [Google Scholar] [CrossRef] [PubMed]
- Vitali, C.; Bombardieri, S.; Moutsopoulos, H.M.; Coll, J.; Gerli, R.; Hatron, P.Y.; Kater, L.; Konttinen, Y.T.; Manthorpe, R.; Meyer, O.; et al. Assessment of the European classification criteria for Sjögren’s syndrome in a series of clinically defined cases: Results of a prospective multicentre study. The European Study Group on Diagnostic Criteria for Sjögren’s Syndrome. Ann. Rheum. Dis. 1996, 55, 116–121. [Google Scholar] [CrossRef]
- Klutmann, S.; Bohuslavizki, K.H.; Kröger, S.; Bleckmann, C.; Brenner, W.; Mester, J.; Clausen, M. Quantitative salivary gland scintigraphy. J. Nucl. Med. Technol. 1999, 27, 20–26. [Google Scholar]
- Taylor, A.T.; Brandon, D.C.; de Palma, D.; Blaufox, M.D.; Durand, E.; Erbas, B.; Grant, S.F.; Hilson, A.J.; Morsing, A. SNMMI Procedure Standard/EANM Practice Guideline for Diuretic Renal Scintigraphy in Adults With Suspected Upper Urinary Tract Obstruction 1.0. Semin. Nucl. Med. 2018, 48, 377–390. [Google Scholar] [CrossRef]
- Peters, A.M. Graphical analysis of dynamic data: The Patlak-Rutland plot. Nucl. Med. Commun. 1994, 15, 669–672. [Google Scholar] [CrossRef] [PubMed]
- Piepsz, A.; Kinthaert, J.; Tondeur, M.; Ham, H.R. The robustness of the Patlak-Rutland slope for the determination of split renal function. Nucl. Med. Commun. 1996, 17, 817–821. [Google Scholar] [CrossRef] [PubMed]
- Gates, G.F. Glomerular filtration rate: Estimation from fractional renal accumulation of 99mTc-DTPA (stannous). Am. J. Roentgenol. 1982, 138, 565–570. [Google Scholar] [CrossRef]
- Esteves, F.P.; Halkar, R.K.; Issa, M.M.; Grant, S.; Taylor, A. Comparison of camera-based 99mTc-MAG3 and 24-h creatinine clearances for evaluation of kidney function. Am. J. Roentgenol. 2006, 187, W316–W319. [Google Scholar] [CrossRef]
- Grubmüller, B.; Senn, D.; Kramer, G.; Baltzer, P.; D’Andrea, D.; Grubmüller, K.H.; Mitterhauser, M.; Eidherr, H.; Haug, A.R.; Wadsak, W.; et al. Response assessment using (68)Ga-PSMA ligand PET in patients undergoing (177)Lu-PSMA radioligand therapy for metastatic castration-resistant prostate cancer. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 1063–1072. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Kalmthout, L.W.M.; Lam, M.G.E.H.; De Keizer, B.; Krijger, G.C.; Ververs, T.F.T.; De Roos, R.; Braat, A.J.A.T. Impact of external cooling with icepacks on (68)Ga-PSMA uptake in salivary glands. EJNMMI Res. 2018, 8, 56. [Google Scholar] [CrossRef]
- Fendler, W.P.; Reinhardt, S.; Ilhan, H.; Delker, A.; Böning, G.; Gildehaus, F.J.; Stief, C.; Bartenstein, P.; Gratzke, C.; Lehner, S.; et al. Preliminary experience with dosimetry, response and patient reported outcome after 177Lu-PSMA-617 therapy for metastatic castration-resistant prostate cancer. Oncotarget 2016, 8, 3581–3590. [Google Scholar] [CrossRef] [Green Version]
- Ahmadzadehfar, H.; Eppard, E.; Kürpig, S.; Fimmers, R.; Yordanova, A.; Schlenkhoff, C.D.; Gartner, F.; Rogenhofer, S.; Essler, M. Therapeutic response and side effects of repeated radioligand therapy with 177Lu-PSMA-DKFZ-617 of castrate-resistant metastatic prostate cancer. Oncotarget 2016, 7, 12477–12488. [Google Scholar] [CrossRef]
- Rahbar, K.; Bode, A.; Weckesser, M.; Avramovic, N.; Claesener, M.; Stegger, L.; Bögemann, M. Radioligand Therapy With 177Lu-PSMA-617 as A Novel Therapeutic Option in Patients With Metastatic Castration Resistant Prostate Cancer. Clin. Nucl. Med. 2016, 41, 522–528. [Google Scholar] [CrossRef]
- Scarpa, L.; Buxbaum, S.; Kendler, D.; Fink, K.; Bektic, J.; Gruber, L.; Decristoforo, C.; Uprimny, C.; Lukas, P.; Horninger, W.; et al. The (68)Ga/(177)Lu theragnostic concept in PSMA targeting of castration-resistant prostate cancer: Correlation of SUV(max) values and absorbed dose estimates. Eur. J. Nucl. Med. Mol. Imaging 2017, 44, 788–800. [Google Scholar] [CrossRef]
- Hofman, M.S.; Violet, J.; Hicks, R.J.; Ferdinandus, J.; Thang, S.P.; Akhurst, T.; Iravani, A.; Kong, G.; Kumar, A.R.; Murphy, D.G.; et al. [(177)Lu]-PSMA-617 radionuclide treatment in patients with metastatic castration-resistant prostate cancer (LuPSMA trial): A single-centre, single-arm, phase 2 study. Lancet Oncol. 2018, 19, 825–833. [Google Scholar] [CrossRef]
- Wolf, P.; Freudenberg, N.; Bühler, P.; Alt, K.; Schultze-Seemann, W.; Wetterauer, U.; Elsässer-Beile, U. Three conformational antibodies specific for different PSMA epitopes are promising diagnostic and therapeutic tools for prostate cancer. Prostate 2009, 70, 562–569. [Google Scholar] [CrossRef] [PubMed]
- Taïeb, D.; Foletti, J.-M.; Bardiès, M.; Rocchi, P.; Hicks, R.J.; Haberkorn, U. PSMA-Targeted Radionuclide Therapy and Salivary Gland Toxicity: Why Does It Matter? J. Nucl. Med. 2018, 59, 747–748. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sathekge, M.M.; Bruchertseifer, F.; Vorster, M.; Morgenstern, A.; Lawal, I.O. Global experience with PSMA-based alpha therapy in prostate cancer. Eur. J. Nucl. Med. Mol. Imaging 2021, 26, 1–7. [Google Scholar]
- Filippi, L.; Chiaravalloti, A.; Schillaci, O.; Bagni, O. The potential of PSMA-targeted alpha therapy in the management of prostate cancer. Expert Rev. Anticancer. Ther. 2020, 20, 823–829. [Google Scholar] [CrossRef]
- Rosar, F.; Kochems, N.; Bartholomä, M.; Maus, S.; Stemler, T.; Linxweiler, J.; Khreish, F.; Ezziddin, S. Renal Safety of [177Lu]Lu-PSMA-617 Radioligand Therapy in Patients with Compromised Baseline Kidney Function. Cancers 2021, 13, 3095. [Google Scholar] [CrossRef] [PubMed]
- Gallyamov, M.; Meyrick, D.; Barley, J.; Lenzo, N. Renal outcomes of radioligand therapy: Experience of 177lutetium—prostate-specific membrane antigen ligand therapy in metastatic castrate-resistant prostate cancer. Clin. Kidney J. 2019, 13, 1049–1055. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ngoc, C.N.; Happel, C.; Davis, K.; Groener, D.; Mader, N.; Mandel, P.; Tselis, N.; Gruenwald, F.; Sabet, A. Renal Function after Radioligand Treatment with 177Lu-PSMA-617. J. Nucl. Med. 2020, 61 (Suppl. 1), 1279. [Google Scholar]
- Yadav, M.P.; Ballal, S.; Tripathi, M.; Damle, N.A.; Sahoo, R.K.; Seth, A.; Tselis, N.; Gruenwald, F.; Sabet, A. (177)Lu-DKFZ-PSMA-617 therapy in metastatic castration resistant prostate cancer: Safety, efficacy, and quality of life assessment. Eur. J. Nucl. Med. Mol. Imaging 2017, 44, 81–91. [Google Scholar] [CrossRef] [PubMed]
- Rahbar, K.; Schmidt, M.; Heinzel, A.; Eppard, E.; Bode, A.; Yordanova, A.; Claesener, M.; Ahmadzadehfar, H. Response and Tolerability of a Single Dose of 177Lu-PSMA-617 in Patients with Metastatic Castration-Resistant Prostate Cancer: A Multicenter Retrospective Analysis. J. Nucl. Med. 2016, 57, 1334–1338. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Features | Values |
|---|---|
| Patients (n) | 27 |
| Age (mean ± SD) years | 71 ± 7 |
| Weight (mean ± SD) kilogram | 85 ± 14 |
| Karnofsky Score (n) % | |
| <80% | (9) 33 |
| ≥80% | (18) 66 |
| ECOG-Index (n) % | |
| 0 | (0) |
| 1 | (25) 92.5 |
| 2 | (2) 7.4 |
| * PSA µg/L | 81.03 (5.91–3305) |
| Hb (mean ± SD) g/dL | 12.1 ± 1.6 |
| Leucocyte g/L | 6.9 ± 2.5 |
| Thrombocyte (mean ± SD) g/L | 242 ± 71 |
| * Creatinine mg/dL | 0.95 (0.71–1.16) |
| Previous treatments (n) % | |
| Enzalutamide/Abiraterone | (19) 70 |
| Docetaxel/Cabazitaxel | (19) 70 |
| Ra-223 (Xofigo®) | (11) 41 |
| No chemo- or hormone or Ra-223 (Xofigo®) | (2) 7 |
| Metastatic lesions (n) % | |
| cM1a | (5) 18.5 |
| cM1b | (16) 59.3 |
| cM1c | (6) 22.2 |
| Parameters Mean ± SD | 1st Cycle (n: 27) | 2nd Cycle (n: 22) | 3rd Cycle (n: 22) | 4 Weeks after 3rd Cycle (n: 27) | p-Value |
|---|---|---|---|---|---|
| Ejection fraction (%): | |||||
| All glands | 56.0 ± 12.0 | 54.6 ± 9.4 | 56.0 ± 12.1 | 53.9 ± 12.9 | p = 0.31 |
| Right parotid | 62.0 ± 11.6 | 59.3 ± 8.3 | 61.8 ± 10.8 | 57.1 ± 14.0 | p = 0.28 |
| Left parotid | 58.7 ± 14.1 | 57.6 ± 10.4 | 58.5 ± 16.1 | 54.3 ± 15.9 | p = 0.60 |
| Right submandibular | 51.1 ± 10.9 | 50.6 ± 9.3 | 52.4 ± 8.2 | 51.7 ± 10.6 | p = 0.94 |
| Left submandibular | 52.3 ± 7.2 | 51.1 ± 6.6 | 51.4 ± 9.6 | 52.5 ± 10.3 | p = 0.91 |
| Peak time (minutes): | |||||
| All glands combined | 16.9 ± 3.6 | 16.5 ± 3.9 | 16.5 ± 4.4 | 17.9 ± 3.9 | p = 0.03 * |
| Right parotid | 17.9 ± 2.5 | 17.8 ± 2.0 | 17.5 ± 3.8 | 18.6 ± 2.5 | p = 0.50 |
| Left parotid | 18.2 ± 3.2 | 17.9 ± 2.8 | 18.1 ± 3.4 | 18.9 ± 3.9 | p = 0.68 |
| Right submandibular | 15.7 ± 4.3 | 15.7 ± 5.1 | 14.6 ± 5.3 | 17.3 ± 4.0 | p = 0.23 |
| Left submandibular | 15.9 ± 3.7 | 14.6 ± 4.3 | 15.9 ± 4.4 | 16.8 ± 4.7 | p = 0.33 |
| RA after 5 min: | |||||
| All glands combined | 56.9 ± 17.2 | 59.2 ± 17.0 | 57.5 ± 18.5 | 59.0 ± 19.7 | p = 0.64 |
| Right parotid | 47.7 ± 14.9 | 53.6 ± 17.9 | 50.2 ± 16.6 | 54.7 ± 21.0 | p = 0.27 |
| Left parotid | 51.1 ± 17.2 | 55.1 ± 16.2 | 52.1 ± 18.0 | 54.9 ± 20.6 | p = 0.73 |
| Right submandibular | 63.0 ± 13.5 | 63.3 ± 17.2 | 62.1 ± 18.8 | 64.1 ± 18.6 | p = 0.98 |
| Left submandibular | 65.8 ± 16.1 | 65.0 ± 14.8 | 65.6 ± 17.0 | 62.3 ± 17.8 | p = 0.84 |
| Parameters Mean ± SD | 1st Cycle (n: 27) | 2nd Cycle (n: 22) | 3rd Cycle (n: 22) | 4 Weeks after 3rd Cycle (n: 27) | p-Value |
|---|---|---|---|---|---|
| Creatinine mg/dL | 0.98 ± 0.28 | 0.94 ± 0.27 | 0.95 ± 0.28 | 1.02 ± 0.35 | p = 0.58 |
| * Relative function: | |||||
| Right | 47.3 ± 11.9 | 48.9 ± 13.1 | 51.6 ± 8.0 | 45.4 ± 11.1 | p = 0.28 |
| Left | 52.7 ± 11.9 | 51.1 ± 13.1 | 48.4 ± 8.0 | 54.6 ± 11.1 | p = 0.28 |
| # Integral: | |||||
| All | 94.5 ± 46.7 | 94.3 ± 40.5 | 101.5 ± 36.5 | 83.1 ± 32.7 | p = 0.16 |
| Right | 88.7 ± 42.3 | 89.1 ± 38.3 | 100.8 ± 31.7 | 77.0 ± 34.2 | p = 0.20 |
| Left | 100.4 ± 50.5 | 99.7 ± 43.0 | 102.2 ± 41.8 | 89.2 ± 30.6 | p = 0.67 |
| Parameters Mean ± SD | Prior 1st Cycle (n: 27) | 4 Weeks after 3rd Therapy (n: 27) | p-Value |
|---|---|---|---|
| SUVmax.: | |||
| All (both sides submandibular) | 20.2 ± 5.5 | 16.6 ± 4.8 | p = 0.001 * |
| Right submandibular | 19.9 ± 5.4 | 16.6 ± 4.9 | p = 0.03 * |
| Left submandibular | 20.5 ± 5.7 | 16.6 ± 4.8 | p = 0.014 * |
| Metabolic volume: | |||
| All (both sides submandibular | 11.1 ± 3.3 | 10.5 ± 3.2 | p = 0.44 |
| Right submandibular | 11.3 ± 3.5 | 10.9 ± 3.3 | p = 0.65 |
| Left submandibular | 10.8 ± 3.1 | 10.2 ± 3.2 | p = 0.53 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wollenweber, T.; Zisser, L.; Kretschmer-Chott, E.; Weber, M.; Grubmüller, B.; Kramer, G.; Shariat, S.F.; Mitterhauser, M.; Schmitl, S.; Vraka, C.; et al. Renal and Salivary Gland Functions after Three Cycles of PSMA-617 Therapy Every Four Weeks in Patients with Metastatic Castration-Resistant Prostate Cancer. Curr. Oncol. 2021, 28, 3692-3704. https://doi.org/10.3390/curroncol28050315
Wollenweber T, Zisser L, Kretschmer-Chott E, Weber M, Grubmüller B, Kramer G, Shariat SF, Mitterhauser M, Schmitl S, Vraka C, et al. Renal and Salivary Gland Functions after Three Cycles of PSMA-617 Therapy Every Four Weeks in Patients with Metastatic Castration-Resistant Prostate Cancer. Current Oncology. 2021; 28(5):3692-3704. https://doi.org/10.3390/curroncol28050315
Chicago/Turabian StyleWollenweber, Tim, Lucia Zisser, Elisabeth Kretschmer-Chott, Michael Weber, Bernhard Grubmüller, Gero Kramer, Shahrokh F. Shariat, Markus Mitterhauser, Stefan Schmitl, Chrysoula Vraka, and et al. 2021. "Renal and Salivary Gland Functions after Three Cycles of PSMA-617 Therapy Every Four Weeks in Patients with Metastatic Castration-Resistant Prostate Cancer" Current Oncology 28, no. 5: 3692-3704. https://doi.org/10.3390/curroncol28050315
APA StyleWollenweber, T., Zisser, L., Kretschmer-Chott, E., Weber, M., Grubmüller, B., Kramer, G., Shariat, S. F., Mitterhauser, M., Schmitl, S., Vraka, C., Haug, A. R., Hacker, M., Hartenbach, M., & Rasul, S. (2021). Renal and Salivary Gland Functions after Three Cycles of PSMA-617 Therapy Every Four Weeks in Patients with Metastatic Castration-Resistant Prostate Cancer. Current Oncology, 28(5), 3692-3704. https://doi.org/10.3390/curroncol28050315