Intraventricular Meningiomas: Clinical-Pathological and Genetic Features of a Monocentric Series


 ,
,  , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Cases
2.2. Ethical Issues
2.3. Mutational and Copy Number Variation Status of 409 Cancer Genes
3. Results
3.1. Cases
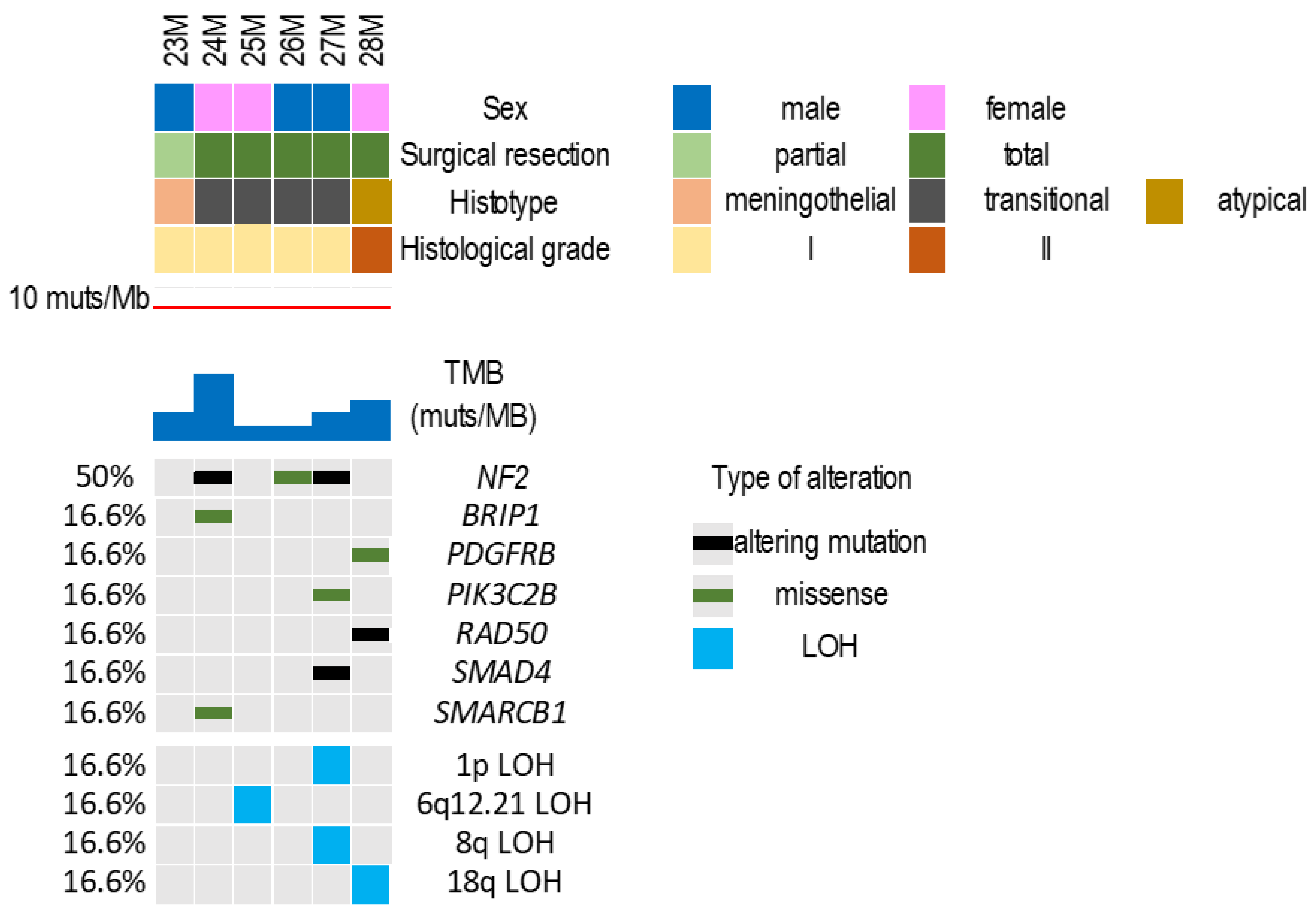
3.2. Mutational and Copy Number Variation Status of 409 Cancer Genes
3.3. Tumor Mutational Burden
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Louis, D.N.; Ohgaki, H.; Wisteler, O.D.; Cavenee, W.K.; Ellison, D.W.; Figarella-Branger, D.; Perry, A.; Refeinberger, G.; von Deimling, A. WHO Classification of Tumors of the Central Nervous System; IARC: Lyon, France, 2016. [Google Scholar]
- Yuzawa, S.; Nishihara, H.; Tanaka, S. Genetic landscape of meningioma. Brain Tumor Pathol. 2016, 33, 237–247. [Google Scholar] [CrossRef] [PubMed]
- Ius, T.; Tel, A.; Minniti, G.; Somma, T.; Solari, D.; Longhi, M.; De Bonis, P.; Scerrati, A.; Caccese, M.; Barresi, V.; et al. Advances in Multidisciplinary Management of Skull Base Meningiomas. Cancers 2021, 13, 2664. [Google Scholar] [CrossRef]
- Barresi, V.; Simbolo, M.; Fioravanzo, A.; Piredda, M.L.; Caffo, M.; Ghimenton, C.; Pinna, G.; Longhi, M.; Nicolato, A.; Scarpa, A. Molecular Profiling of 22 Primary Atypical Meningiomas Shows the Prognostic Significance of 18q Heterozygous Loss and CDKN2A/B Homozygous Deletion on Recurrence-Free Survival. Cancers 2021, 13, 903. [Google Scholar] [CrossRef]
- Goldbrunner, R.; Stavrinou, P.; Jenkinson, M.D.; Sahm, F.; Mawrin, C.; Weber, D.C.; Preusser, M.; Minniti, G.; Lund-Johansen, M.; Lefranc, F.; et al. EANO guideline on the diagnosis and management of meningiomas. Neuro-Oncology 2021, 23, 1821–1834. [Google Scholar] [CrossRef]
- Bertalanffy, A.; Roessler, K.; Koperek, O.; Gelpi, E.; Prayer, D.; Neuner, M.; Knosp, E. Intraventricular meningiomas: A report of 16 cases. Neurosurg. Rev. 2006, 29, 30–35. [Google Scholar] [CrossRef]
- Gungor, A.; Danyeli, A.E.; Akbas, A.; Eksi, M.S.; Guduk, M.; Ozduman, K.; Pamir, M.N. Ventricular Meningiomas: Surgical Strategies and a New Finding That Suggest an Origin from the Choroid Plexus Epithelium. World Neurosurg. 2019, 129, e177–e190. [Google Scholar] [CrossRef]
- Jungwirth, G.; Warta, R.; Beynon, C.; Sahm, F.; von Deimling, A.; Unterberg, A.; Herold-Mende, C.; Jungk, C. Intraventricular meningiomas frequently harbor NF2 mutations but lack common genetic alterations in TRAF7, AKT1, SMO, KLF4, PIK3CA, and TERT. Acta Neuropathol. Commun. 2019, 7, 140. [Google Scholar] [CrossRef] [Green Version]
- McDermott, M.W. Intraventricular meningiomas. Neurosurg. Clin. N. Am. 2003, 14, 559–569. [Google Scholar] [CrossRef]
- Pereira, B.J.A.; de Almeida, A.N.; Paiva, W.S.; de Aguiar, P.H.P.; Teixeira, M.J.; Marie, S.K.N. Natural history of intraventricular meningiomas: Systematic review. Neurosurg. Rev. 2020, 43, 513–523. [Google Scholar] [CrossRef]
- Clark, V.E.; Harmanci, A.S.; Bai, H.; Youngblood, M.W.; Lee, T.I.; Baranoski, J.F.; Ercan-Sencicek, A.G.; Abraham, B.J.; Weintraub, A.S.; Hnisz, D.; et al. Recurrent somatic mutations in POLR2A define a distinct subset of meningiomas. Nat. Genet. 2016, 48, 1253–1259. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simbolo, M.; Gottardi, M.; Corbo, V.; Fassan, M.; Mafficini, A.; Malpeli, G.; Lawlor, R.T.; Scarpa, A. DNA qualification workflow for next generation sequencing of histopathological samples. PLoS ONE 2013, 8, e62692. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Available online: https://github.com/ekg/vcflib (accessed on 24 September 2021).
- Cingolani, P.; Patel, V.M.; Coon, M.; Nguyen, T.; Land, S.J.; Ruden, D.M.; Lu, X. Using Drosophila melanogaster as a Model for Genotoxic Chemical Mutational Studies with a New Program, SnpSift. Front. Genet. 2012, 3, 35. [Google Scholar] [CrossRef] [Green Version]
- McLaren, W.; Pritchard, B.; Rios, D.; Chen, Y.; Flicek, P.; Cunningham, F. Deriving the consequences of genomic variants with the Ensembl API and SNP Effect Predictor. Bioinformatics 2010, 26, 2069–2070. [Google Scholar] [CrossRef]
- Robinson, J.T.; Thorvaldsdottir, H.; Winckler, W.; Guttman, M.; Lander, E.S.; Getz, G.; Mesirov, J.P. Integrative genomics viewer. Nat. Biotechnol. 2011, 29, 24–26. [Google Scholar] [CrossRef] [Green Version]
- Boeva, V.; Popova, T.; Lienard, M.; Toffoli, S.; Kamal, M.; Le Tourneau, C.; Gentien, D.; Servant, N.; Gestraud, P.; Rio Frio, T.; et al. Multi-factor data normalization enables the detection of copy number aberrations in amplicon sequencing data. Bioinformatics 2014, 30, 3443–3450. [Google Scholar] [CrossRef] [Green Version]
- Brastianos, P.K.; Galanis, E.; Butowski, N.; Chan, J.W.; Dunn, I.F.; Goldbrunner, R.; Herold-Mende, C.; Ippen, F.M.; Mawrin, C.; McDermott, M.W.; et al. Advances in multidisciplinary therapy for meningiomas. Neuro-Oncology 2019, 21, i18–i31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weller, M.; Roth, P.; Sahm, F.; Burghardt, I.; Schuknecht, B.; Rushing, E.J.; Regli, L.; Lindemann, J.P.; von Deimling, A. Durable Control of Metastatic AKT1-Mutant WHO Grade 1 Meningothelial Meningioma by the AKT Inhibitor, AZD5363. J. Natl. Cancer Inst. 2017, 109, 1–4. [Google Scholar] [CrossRef] [Green Version]
- Brastianos, P.K.; Horowitz, P.M.; Santagata, S.; Jones, R.T.; McKenna, A.; Getz, G.; Ligon, K.L.; Palescandolo, E.; Van Hummelen, P.; Ducar, M.D.; et al. Genomic sequencing of meningiomas identifies oncogenic SMO and AKT1 mutations. Nat. Genet. 2013, 45, 285–289. [Google Scholar] [CrossRef] [PubMed]
- Shorning, B.Y.; Dass, M.S.; Smalley, M.J.; Pearson, H.B. The PI3K-AKT-mTOR Pathway and Prostate Cancer: At the Crossroads of AR, MAPK, and WNT Signaling. Int. J. Mol. Sci. 2020, 21, 4507. [Google Scholar] [CrossRef]
- Mehrvarz Sarshekeh, A.; Advani, S.; Overman, M.J.; Manyam, G.; Kee, B.K.; Fogelman, D.R.; Dasari, A.; Raghav, K.; Vilar, E.; Manuel, S.; et al. Association of SMAD4 mutation with patient demographics, tumor characteristics, and clinical outcomes in colorectal cancer. PLoS ONE 2017, 12, e0173345. [Google Scholar] [CrossRef] [Green Version]
- Olar, A.; Wani, K.M.; Wilson, C.D.; Zadeh, G.; DeMonte, F.; Jones, D.T.; Pfister, S.M.; Sulman, E.P.; Aldape, K.D. Global epigenetic profiling identifies methylation subgroups associated with recurrence-free survival in meningioma. Acta Neuropathol. 2017, 133, 431–444. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abedalthagafi, M.; Bi, W.L.; Aizer, A.A.; Merrill, P.H.; Brewster, R.; Agarwalla, P.K.; Listewnik, M.L.; Dias-Santagata, D.; Thorner, A.R.; Van Hummelen, P.; et al. Oncogenic PI3K mutations are as common as AKT1 and SMO mutations in meningioma. Neuro-Oncology 2016, 18, 649–655. [Google Scholar] [CrossRef] [Green Version]
- Clark, V.E.; Erson-Omay, E.Z.; Serin, A.; Yin, J.; Cotney, J.; Ozduman, K.; Avsar, T.; Li, J.; Murray, P.B.; Henegariu, O.; et al. Genomic analysis of non-NF2 meningiomas reveals mutations in TRAF7, KLF4, AKT1, and SMO. Science 2013, 339, 1077–1080. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, L.; Huang, J.; Wang, K.; Li, J.; Yan, R.; Zhu, L.; Ye, J.; Wu, X.; Zhuang, S.; Li, D.; et al. Targeting Rad50 sensitizes human nasopharyngeal carcinoma cells to radiotherapy. BMC Cancer 2016, 16, 190. [Google Scholar] [CrossRef] [Green Version]
- Kluth, M.; Hesse, J.; Heinl, A.; Krohn, A.; Steurer, S.; Sirma, H.; Simon, R.; Mayer, P.S.; Schumacher, U.; Grupp, K.; et al. Genomic deletion of MAP3K7 at 6q12-22 is associated with early PSA recurrence in prostate cancer and absence of TMPRSS2:ERG fusions. Mod. Pathol. 2013, 26, 975–983. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ormond, D.R.; Kleinschmidt-DeMasters, B.K.; Cavalcante, D.; Smith, E.E.; Cramer, S.D.; Lucia, M.S. Prostatic adenocarcinoma CNS parenchymal and dural metastases: Alterations in ERG, CHD1 and MAP3K7 expression. J. Neurooncol. 2019, 142, 319–325. [Google Scholar] [CrossRef]
- Bi, W.L.; Nayak, L.; Meredith, D.M.; Driver, J.; Du, Z.; Hoffman, S.; Li, Y.; Lee, E.Q.; Beroukhim, R.; Rinne, M.; et al. Activity of PD-1 blockade with Nivolumab among patients with recurrent atypical/anaplastic meningioma: Phase II trial results. Neuro-Oncology 2021, noab118. [Google Scholar] [CrossRef] [PubMed]
- Bi, W.L.; Greenwald, N.F.; Abedalthagafi, M.; Wala, J.; Gibson, W.J.; Agarwalla, P.K.; Horowitz, P.; Schumacher, S.E.; Esaulova, E.; Mei, Y.; et al. Genomic landscape of high-grade meningiomas. NPJ Genom. Med. 2017, 2, 15. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Case | Age | Sex | Site | Surgery | Histotype | Post-Surgical Complications | Adjuvant Treatment | Recurrence (RFS) | TMB (muts/Mb) |
|---|---|---|---|---|---|---|---|---|---|
| 23M | 45 | M | III, LV, RV | Partial | meningothelial | respiratory failure, hydrocephalus, and surgical site infection | GK | no (40) | 1.87 |
| 24M | 47 | F | LV | Total | transitional | none | None | no (48) | 5.13 |
| 25M | 25 | F | RV | Total | transitional | pneumatocephalus | None | no (12) | 0.87 |
| 26M | 70 | M | RV | Total | transitional | pneumatocephalus | None | no (72) | 0.86 |
| 27M | 66 | M | LV | Total | transitional | hematoma in surgical site | None | not available | 1.71 |
| 28M | 31 | F | LV | Total | atypical | none | None | no (7) | 2.28 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ammendola, S.; Simbolo, M.; Ciaparrone, C.; Rizzo, P.C.; Caffo, M.; Pinna, G.; Sala, F.; Scarpa, A.; Barresi, V. Intraventricular Meningiomas: Clinical-Pathological and Genetic Features of a Monocentric Series. Curr. Oncol. 2022, 29, 178-185. https://doi.org/10.3390/curroncol29010017
Ammendola S, Simbolo M, Ciaparrone C, Rizzo PC, Caffo M, Pinna G, Sala F, Scarpa A, Barresi V. Intraventricular Meningiomas: Clinical-Pathological and Genetic Features of a Monocentric Series. Current Oncology. 2022; 29(1):178-185. https://doi.org/10.3390/curroncol29010017
Chicago/Turabian StyleAmmendola, Serena, Michele Simbolo, Chiara Ciaparrone, Paola Chiara Rizzo, Maria Caffo, Giampietro Pinna, Francesco Sala, Aldo Scarpa, and Valeria Barresi. 2022. "Intraventricular Meningiomas: Clinical-Pathological and Genetic Features of a Monocentric Series" Current Oncology 29, no. 1: 178-185. https://doi.org/10.3390/curroncol29010017
APA StyleAmmendola, S., Simbolo, M., Ciaparrone, C., Rizzo, P. C., Caffo, M., Pinna, G., Sala, F., Scarpa, A., & Barresi, V. (2022). Intraventricular Meningiomas: Clinical-Pathological and Genetic Features of a Monocentric Series. Current Oncology, 29(1), 178-185. https://doi.org/10.3390/curroncol29010017