Lymph Node Dissection Is a Risk Factor for Short-Term Cough after Pulmonary Resection


Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Selection
2.2. Surgical Techniques
2.3. Postoperative Management
2.4. Evaluation Methods and Grouping Criteria for Cough
2.5. Statistical Analysis
3. Results
3.1. Patients’ Clinical and Pathological Data and Univariate Analysis of Postoperative Cough
3.2. Treatment Results
3.3. Analysis of the Short-Term Postoperative LCQ Score
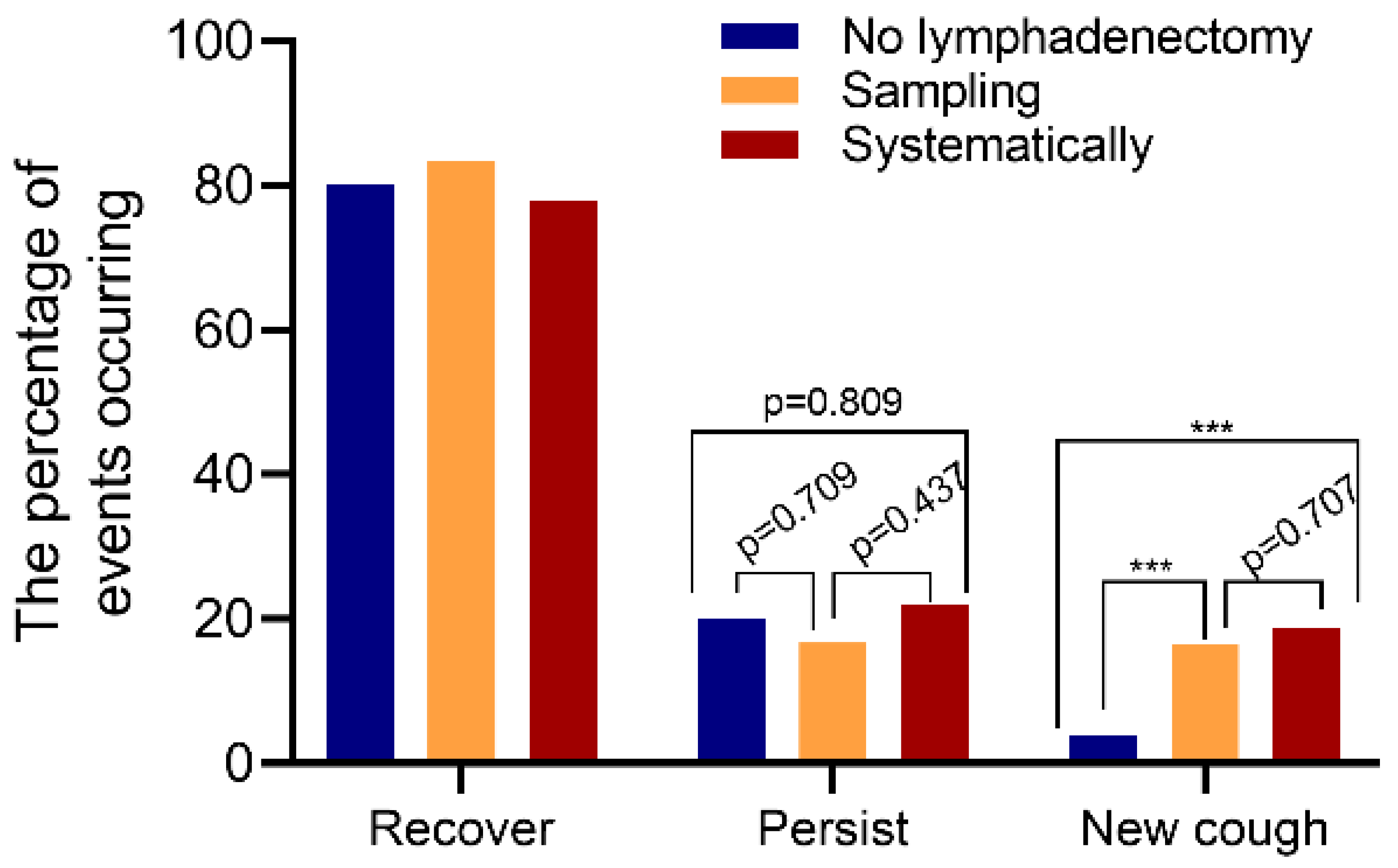
3.4. Multivariate Regression Analysis of Cough after Pulmonary Resection and Changes of Postoperative Cough State
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dai, F.; Meng, S.; Mei, L.; Guan, C.; Ma, Z. Single-port video-assisted thoracic surgery in the treatment of non-small cell lung cancer: A propensity-matched comparative analysis. J. Thorac. Dis. 2016, 8, 2872–2878. [Google Scholar] [CrossRef] [Green Version]
- Nwogu, C.E.; D’Cunha, J.; Pang, H.; Gu, L.; Wang, X.; Richards, W.G.; Veit, L.J.; Demmy, T.L.; Sugarbaker, D.J.; Kohman, L.J.; et al. VATS Lobectomy Has Better Perioperative Outcomes Than Open Lobectomy: CALGB 31001, an Ancillary Analysis of CALGB 140202 (Alliance). Ann. Thorac. Surg. 2015, 99, 399–405. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xie, D.; Zhong, Y.; Deng, J.; She, Y.; Zhang, L.; Fan, J.; Jiang, G.; Zhu, Y.; Jiang, L.; Chen, C. Comparison of uniportal video-assisted thoracoscopic versus thoracotomy bronchial sleeve lobectomy with pulmonary arterioplasty for centrally located non-small-cell lung cancer. Eur. J. Cardio-Thorac. Surg. 2021, 59, 978–986. [Google Scholar] [CrossRef] [PubMed]
- Sarna, L.; Evangelista, L.; Tashkin, D.; Padilla, G.; Holmes, C.; Brecht, M.L.; Grannis, F. Impact of Respiratory Symptoms and Pulmonary Function on Quality of Life of Long-term Survivors of Non-Small Cell Lung Cancer. Chest 2004, 125, 439–445. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, R.; Che, G. Risk factors of cough in non-small cell lung cancer patients after video-assisted thoracoscopic surgery. J. Thorac. Dis. 2018, 10, 5368–5375. [Google Scholar] [CrossRef] [PubMed]
- Yang, P.; Cheville, A.L.; Wampfler, J.A.; Garces, Y.I.; Jatoi, A.; Clark, M.M.; Cassivi, S.D.; Midthun, D.E.; Marks, R.S.; Aubry, M.-C.; et al. Quality of Life and Symptom Burden among Long-Term Lung Cancer Survivors. J. Thorac. Oncol. 2012, 7, 64–70. [Google Scholar] [CrossRef] [Green Version]
- McCool, F.D. Global physiology and pathophysiology of cough: ACCP evidence-based clinical practice guidelines. Chest 2006, 129, 48S–53S. [Google Scholar] [CrossRef]
- Shannon, R.; Baekey, D.M.; Morris, K.F.; Lindsey, B.G. Ventrolateral medullary respiratory network and a model of cough motor pattern generation. J. Appl. Physiol. 1998, 84, 2020–2035. [Google Scholar] [CrossRef]
- Pan, L.-Y.; Peng, L.-P.; Xu, C.; Ding, C.; Chen, J.; Wang, W.-Y.; Zhu, X.-Y.; Zhao, J.; Li, C. Predictive factors of cough after uniportal video-assisted thoracoscopic pulmonary resection. J. Thorac. Dis. 2020, 12, 5958–5969. [Google Scholar] [CrossRef]
- Xie, M.; Zhu, Y.; Zhou, M.; Wu, S.; Xu, G.; Xu, S.; Xu, M. Analysis of factors related to chronic cough after lung cancer surgery. Thorac. Cancer 2019, 10, 898–903. [Google Scholar] [CrossRef]
- Chen, Z.; Dong, Q.; Liang, L. Effect of different thoracic anesthesia on postoperative cough. J. Thorac. Dis. 2018, 10, 3539–3547. [Google Scholar] [CrossRef]
- McGarvey, L.; Nishino, T. Acute and chronic cough. Pulm. Pharmacol. Ther. 2004, 17, 351–354. [Google Scholar] [CrossRef]
- Detterbeck, F.C.; Boffa, D.J.; Kim, A.W.; Tanoue, L.T. The Eighth Edition Lung Cancer Stage Classification. Chest 2017, 151, 193–203. [Google Scholar] [CrossRef] [PubMed]
- National Health Commission of the People’s Republic of China. Chinese guidelines for diagnosis and treatment of primary lung cancer 2018 (English version). Chin. J. Cancer Res. 2019, 31, 1–28. [Google Scholar] [CrossRef] [PubMed]
- Gao, Y.-H.; Guan, W.-J.; Xu, G.; Lin, Z.-Y.; Tang, Y.; Li, H.-M.; Luo, Q.; Zhong, N.-S.; Birring, S.S.; Chen, R.-C. Validation of the Mandarin Chinese version of the Leicester Cough Questionnaire in bronchiectasis. Int. J. Tuberc. Lung Dis. 2014, 18, 1431–1437. [Google Scholar] [CrossRef]
- Lin, R.; Che, G. Validation of the Mandarin Chinese version of the Leicester Cough Questionnaire in non-small cell lung cancer patients after surgery. Thorac. Cancer 2018, 9, 486–490. [Google Scholar] [CrossRef] [PubMed]
- Irwin, R.S. Assessing cough severity and efficacy of therapy in clinical research: ACCP evidence-based clinical practice guidelines. Chest 2006, 129, 232S–237S. [Google Scholar] [CrossRef] [Green Version]
- Yousaf, N.; Lee, K.K.; Jayaraman, B.; Pavord, I.D.; Birring, S.S. The assessment of quality of life in acute cough with the Leicester Cough Questionnaire (LCQ-acute). Cough 2011, 7, 4. [Google Scholar] [CrossRef] [Green Version]
- Ward, N.; Stiller, K.; Rowe, H.; Holland, A.E. The psychometric properties of the Leicester Cough Questionnaire and Respiratory Symptoms in CF tool in cystic fibrosis: A preliminary study. J. Cyst. Fibros. 2017, 16, 425–432. [Google Scholar] [CrossRef] [Green Version]
- Wang, Z.; Wang, M.; Wen, S.; Yu, L.; Xu, X. Types and applications of cough-related questionnaires. J. Thorac. Dis. 2019, 11, 4379–4388. [Google Scholar] [CrossRef]
- Li, X.; Li, X.; Zhang, W.; Liu, Q.; Gao, Y.; Chang, R.; Zhang, C. Factors and potential treatments of cough after pulmonary resection: A systematic review. Asian J. Surg. 2021, 44, 1029–1036. [Google Scholar] [CrossRef]
- Song, W.; Chang, Y.-S. Cough hypersensitivity as a neuro-immune interaction. Clin. Transl. Allergy 2015, 5, 24. [Google Scholar] [CrossRef] [Green Version]
- Morice, A.H.; Jakes, A.D.; Faruqi, S.; Birring, S.S.; McGarvey, L.; Canning, B.J.; Smith, J.; Parker, S.M.; Chung, K.F.; Lai, K.; et al. A worldwide survey of chronic cough: A manifestation of enhanced somatosensory response. Eur. Respir. J. 2014, 44, 1149–1155. [Google Scholar] [CrossRef] [Green Version]
- Wu, J.; Dai, L.; Lou, W. Incidence and risk factor for short term postoperative cough after thyroidectomy. BMC Cancer 2020, 20, 888. [Google Scholar] [CrossRef]
- Mitchell, V.; Dravid, R.M.; Patel, A.; Swampillai, C.; Higgs, A. Difficult Airway Society Guidelines for the management of tracheal extubation. Anaesthesia 2012, 67, 318–340. [Google Scholar] [CrossRef]
- Shuying, L.; Ping, L.; Juan, N.; Dong, L. Different interventions in preventing opioid-induced cough: A meta-analysis. J. Clin. Anesth. 2016, 34, 440–447. [Google Scholar] [CrossRef]
- White, P.F.; Tang, J.; Wender, R.H.; Yumul, R.; Stokes, O.J.; Sloninsky, A.; Naruse, R.; Kariger, R.; Norel, E.; Mandel, S.; et al. Desflurane Versus Sevoflurane for Maintenance of Outpatient Anesthesia: The Effect on Early Versus Late Recovery and Perioperative Coughing. Anesth. Analg. 2009, 109, 387–393. [Google Scholar] [CrossRef]
- Li, Y.; Wang, J. Analysis of lymph node impact on conversion of complete thoracoscopic lobectomy to open thoracotomy. Thorac. Cancer 2015, 6, 704–708. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sawabata, N.; Maeda, H.; Takeda, S.-I.; Inoue, M.; Koma, M.; Tokunaga, T.; Matsuda, H. Persistent Cough Following Pulmonary Resection: Observational and Empiric Study of Possible Causes. Ann. Thorac. Surg. 2005, 79, 289–293. [Google Scholar] [CrossRef] [PubMed]
- Widdicombe, J. Afferent receptors in the airways and cough. Respir. Physiol. 1998, 114, 5–15. [Google Scholar] [CrossRef]
- Birring, S.S.; Prudon, B.; Carr, A.J.; Singh, S.J.; Morgan, M.D.L.; Pavord, I. Development of a symptom specific health status measure for patients with chronic cough: Leicester Cough Questionnaire (LCQ). Thorax 2003, 58, 339–343. [Google Scholar] [CrossRef] [Green Version]
- Watanabe, S.-I. Lymph node dissection for lung cancer: Past, present, and future. Gen. Thorac. Cardiovasc. Surg. 2014, 62, 407–414. [Google Scholar] [CrossRef] [PubMed]
- Ogata, D.; Tanese, K.; Nakamura, Y.; Otsuka, M.; Namikawa, K.; Funakoshi, T.; Yoshikawa, S.; Tsutsui, K.; Nakama, K.; Jinnai, S.; et al. Impact of the changes in the completion lymph node dissection criteria and approval of adjuvant therapies on the real-world outcomes of Japanese stage III melanoma patients. Int. J. Clin. Oncol. 2021, 26, 2338–2346. [Google Scholar] [CrossRef]
- Weijs, T.J.; Ruurda, J.P.; Luyer, M.D.P.; Nieuwenhuijzen, G.A.P.; Van Hillegersberg, R.; Bleys, R.L.A.W. Topography and extent of pulmonary vagus nerve supply with respect to transthoracic oesophagectomy. J. Anat. 2015, 227, 431–439. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manouras, A.; Markogiannakis, H.; Koutras, A.S.; Antonakis, P.T.; Drimousis, P.; Lagoudianakis, E.E.; Kekis, P.; Genetzakis, M.; Koutsoumanis, K.; Bramis, I. Thyroid surgery: Comparison between the electrothermal bipolar vessel sealing system, harmonic scalpel, and classic suture ligation. Am. J. Surg. 2008, 195, 48–52. [Google Scholar] [CrossRef] [PubMed]
- Mathialagan, A.; Verma, R.K.; Panda, N.K. Comparison of spinal accessory dysfunction following neck dissection with harmonic scalpel and electrocautery—A randomized study. Oral Oncol. 2016, 61, 142–145. [Google Scholar] [CrossRef] [PubMed]
- Liddy, W.; Wu, C.; Dionigi, G.; Donatini, G.; Giles Senyurek, Y.; Kamani, D.; Iwata, A.; Wang, B.; Okose, O.; Cheung, A.; et al. Varied RLN Course is Associated with Increased Risk of Nerve Dysfunction during Thyroidectomy: Results of the Surgical Anatomy of the RLN in Thyroid Surgery (SAR) Study, an International Multicenter Prospective Anatomic and Electrophysiologic Study of 1000 Monitored Nerves at Risk from the International Neural Monitoring Study Group (INMSG). Thyroid Off. J. Am. Thyroid Assoc. 2021, 31, 1730–1740. [Google Scholar]
- Sun, X.; Chang, T.; Xu, Y.; Jing, Q.; Cao, S.; Tian, L.; Li, C. Effects of different doses of cisatracurium on intraoperative nerve monitoring in thyroid surgery: A randomised controlled trial. Br. J. Anaesth. 2021, 127, e67–e69. [Google Scholar] [CrossRef] [PubMed]
- Yuda, M.; Nishikawa, K.; Ishikawa, Y.; Takahashi, K.; Kurogochi, T.; Tanaka, Y.; Matsumoto, A.; Tanishima, Y.; Mitsumori, N.; Ikegami, T. Intraoperative nerve monitoring during esophagectomy reduces the risk of recurrent laryngeal nerve palsy. Surg. Endosc. 2021, 1–8. [Google Scholar] [CrossRef]
- Fujimoto, D.; Taniguchi, K.; Kobayashi, H. Intraoperative neuromonitoring during prone thoracoscopic esophagectomy for esophageal cancer reduces the incidence of recurrent laryngeal nerve palsy: A single-center study. Update Surg. 2021, 73, 587–595. [Google Scholar] [CrossRef] [PubMed]
- Harper, C.M. Intraoperative cranial nerve monitoring. Muscle Nerve 2004, 29, 339–351. [Google Scholar] [CrossRef] [PubMed]
- Muavha, D.A.; Ras, L.; Jeffery, S. Laparoscopic surgical anatomy for pelvic floor surgery. Best Pract. Res. Clin. Obstet. Gynaecol. 2018, 54, 89–102. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Total (%) | No Cough (%) | Cough (%) | χ2/t | p-Value |
|---|---|---|---|---|---|
| Patients (n) | 517 | 310 (59.96) | 207 (40.04) | ||
| Gender (n (%)) | 1.826 | 0.177 | |||
| Male | 365 (70.60) | 212 (68.39) | 153 (73.91) | ||
| Female | 152 (29.40) | 98 (31.61) | 54 (26.09) | ||
| Age (years) | 59.18 ± 9.50 | 57.81 ± 9.59 | 1.601 | 0.110 | |
| Smoking status | 0.008 | 0.930 | |||
| Absent | 226 (43.71) | 136 (43.87) | 90 (43.48) | ||
| Present | 291 (56.29) | 174 (56.13) | 117 (56.52) | ||
| Drinking status | 0.876 | 0.349 | |||
| Absent | 200 (38.68) | 125 (40.32) | 75 (36.23) | ||
| Present | 317 (61.32) | 185 (59.68) | 132 (63.77) | ||
| BMI (kg/m2) | 22.45 ± 3.12 | 22.41 ± 2.86 | 0.133 | 0.894 | |
| FEV1 (L) | 2.04 ± 0.43 | 1.95 ± 0.41 | 1.065 | 0.288 | |
| FEV1 % | 85.42 ± 15.74 | 83.68 ± 14.60 | 1.235 | 0.218 | |
| CCI | 2.02 ± 1.34 | 1.95 ± 1.45 | 0.609 | 0.543 | |
| Tumor size (cm) | 2.03 ± 0.91 | 2.44 ± 3.79 | −1.835 | 0.067 | |
| Tumor location | |||||
| Right upper lobe | 166 (32.11) | 100 (32.26) | 66 (31.88) | 2.538 | 0.638 |
| Right middle lobe | 26 (5.03) | 16 (5.16) | 10 (4.83) | ||
| Right lower lobe | 107 (20.70) | 66 (21.29) | 41 (19.81) | ||
| Left upper lobe | 122 (23.60) | 77 (24.84) | 45 (21.74) | ||
| Left lower lobe | 96 (18357) | 51 (16.45) | 45 (21.74) |
| Results | No Cough (n = 310) | Cough (n = 207) | χ2/τ | p-Value |
|---|---|---|---|---|
| Operation time (min) | 122.03 ± 53.55 | 146.11 ± 46.72 | −5.412 | 0.000 |
| Blood loss (mL) | 113.85 ± 71.47 | 142.46 ± 106.01 | −3.666 | 0.000 |
| Tumor | 45.929 | 0.000 | ||
| Benign | 163 (52.58) | 47 (22.71) | ||
| Malignant | 147 (47.42) | 160 (77.29) | ||
| Type of incision | 1.545 | 0.214 | ||
| Single-port | 173 (55.81) | 104 (50.24) | ||
| Two-port | 137 (44.19) | 103 (49.76) | ||
| Type of resection | 23.594 | 0.000 | ||
| Wedge resection | 68 (21.94) | 13 (6.28) | ||
| Segmentectomy | 89 (28.71) | 54 (26.09) | ||
| Lobectomy | 153 (49.35) | 140 (67.63) | ||
| Type of lymphadenectomy | 118.04 | 0.000 | ||
| No lymphadenectomy | 179 (57.74) | 30 (14.49) | ||
| Sampling | 71 (22.90) | 50 (24.15) | ||
| Systematically | 60 (19.36) | 127 (61.36) | ||
| Drainage (days) | 3.87 ± 2.33 | 4.34 ± 2.96 | −2.202 | 0.028 |
| Hospital stay (days) | 7.58 ± 3.84 | 8.32 ± 3.81 | −2.121 | 0.034 |
| Characteristics | No Cough (n = 153) | Cough (n = 140) | χ2/τ | p-Value |
|---|---|---|---|---|
| Gender (n (%)) | 0.289 | 0.591 | ||
| Male | 106 (69.28) | 101 (72.14) | ||
| Female | 47 (30.72) | 39 (27.86) | ||
| Age (years) | 59.54 ± 8.92 | 57.56 ± 9.33 | 1.996 | 0.057 |
| Smoking status | 0.028 | 0.867 | ||
| Absent | 63 (41.18) | 59 (42.14) | ||
| Present | 90 (58.82) | 81 (57.86) | ||
| Drinking status | 0.382 | 0.536 | ||
| Absent | 60 (39.22) | 50 (35.71) | ||
| Present | 93 (90.78) | 90 (64.29) | ||
| BMI (kg/m2) | 22.26 ± 3.04 | 22.66 ± 2.80 | −1.149 | 0.252 |
| FEV1 (L) | 2.05 ± 0.49 | 1.99 ± 0.43 | 1.135 | 0.257 |
| FEV1 % | 86.58 ± 15.52 | 83.95 ± 15.96 | 1.428 | 0.154 |
| CCI | 2.08 ± 1.33 | 1.92 ± 1.49 | 0.953 | 0.341 |
| Tumor size (cm) | 2.60 ± 0.87 | 2.93 ± 4.52 | −0.89 | 0.374 |
| Tumor location | ||||
| Right upper lobe | 53 (34.64) | 44 (31.43) | 3.003 | 0.557 |
| Right middle lobe | 9 (5.88) | 6 (4.29) | ||
| Right lower lobe | 36 (23.53) | 30 (21.43) | ||
| Left upper lobe | 28 (18.30) | 24 (17.14) | ||
| Left lower lobe | 27 (17.65) | 36 (25.71) | ||
| Type of lymphadenectomy | 70.697 | 0.000 | ||
| No lymphadenectomy | 94 (61.44) | 19 (13.57) | ||
| Systematically | 59 (38.56) | 121 (86.43) | ||
| lymphatic metastasis | 1.994 | 0.158 | ||
| Negative | 50 (73.53) | 85 (82.52) | ||
| Positive | 18 (26.47) | 18 (17.48) | ||
| Stage 7 lymph node metastasis | 0.839 | 0.360 | ||
| Negative | 51 (86.44) | 110 (90.91) | ||
| Positive | 8 (13.56) | 11 (9.09) | ||
| Operation time (min) | 143.78 ± 41.23 | 156.31 ± 40.01 | −2.636 | 0.009 |
| Blood loss (mL) | 135.59 ± 64.94 | 158.96 ± 117.34 | −2.133 | 0.034 |
| Drainage (days) | 4.31 ± 2.83 | 4.38 ± 3.13 | −0.205 | 0.838 |
| Hospital stay (days) | 8.41 ± 4.40 | 8.31 ± 3.51 | 0.22 | 0.826 |
| Characteristics | No Cough (n = 147) | Cough (n = 160) | χ2/τ | p-Value |
|---|---|---|---|---|
| Gender (n (%)) | 2.205 | 0.138 | ||
| Male | 96 (65.31) | 117 (73.13) | ||
| Female | 51 (34.69) | 43 (26.88) | ||
| Age (years) | 59.36 ± 10.48 | 58.44 ± 9.96 | 0.791 | 0.429 |
| BMI (kg/m2) | 22.22 ± 3.10 | 22.40 ± 2.73 | −0.545 | 0.586 |
| Tumor size (cm) | 2.04 ± 0.98 | 2.42 ± 4.29 | −1.061 | 0.290 |
| Tumor location | ||||
| Right upper lobe | 46 (31.29) | 47 (29.38) | 2.462 | 0.652 |
| Right middle lobe | 6 (4.08) | 7 (4.38) | ||
| Right lower lobe | 36 (24.49) | 39 (24.38) | ||
| Left upper lobe | 37 (25.17) | 33 (20.63) | ||
| Left lower lobe | 22 (14.97) | 34 (21.23) | ||
| Type of resection | 12.23 | 0.006 | ||
| Wedge resection | 10 (6.80) | 3 (1.88) | ||
| Segmentectomy | 69 (46.94) | 54 (33.75) | ||
| Lobectomy | 68 (46.26) | 103 (64.38) | ||
| Type of lymphadenectomy | 31.685 | 0.000 | ||
| Sampling | 95 (64.63) | 52 (32.50) | ||
| Systematically | 52 (35.37) | 108 (67.50) | ||
| lymphatic metastasis | 0.395 | 0.530 | ||
| Negative | 125 (85.03) | 140 (87.50) | ||
| Positive | 22 (14.97) | 20 (12.50) | ||
| Stage 7 lymph node metastasis | 1.748 | 0.253 | ||
| Negative | 115 (93.50) | 153 (96.84) | ||
| Positive | 8 (6.50) | 5 (3.16) | ||
| Operation time (min) | 138.98 ± 40.79 | 150.90 ± 39.49 | −2.601 | 0.010 |
| Blood loss (mL) | 133.81 ± 66.09 | 150.66 ± 107.24 | −1.640 | 0.018 |
| Variables * | B | S.E. | Wals | OR (95% CI) | p-Value |
|---|---|---|---|---|---|
| Tumor size | 0.009 | 0.043 | 0.440 | 1.009 (0.927–1.099) | 0.835 |
| Operation time | 0.003 | 0.003 | 1.612 | 1.003 (0.998–1.009) | 0.204 |
| Blood loss | 0.000 | 0.001 | 0.123 | 1.000 (0.997–1.002) | 0.726 |
| Pathologic types | −0.032 | 0.303 | 0.011 | 0.969 (0.535–1.755) | 0.916 |
| Type of resection | −0.204 | 0.212 | 0.931 | 0.815 (0.538–1.235) | 0.335 |
| Type of lymphadenectomy | 1.302 | 0.194 | 45.079 | 3.677 (2.514–5.378) | 0.000 |
| Drainage time | 0.058 | 0.048 | 1.464 | 1.060 (0.965–1.164) | 0.226 |
| Hospital stay | 0.021 | 0.033 | 0.413 | 1.022 (0.957–1.091) | 0.521 |
| Groups | Cases (n) | 3 POD | 6 Weeks | Cough Recover | Cough Persist | Develop a New Cough |
|---|---|---|---|---|---|---|
| No lymphadenectomy | 209 | |||||
| No cough | 179 | 196 | 7 (3.9%) | |||
| Cough | 30 | 13 | 24 (80.0%) | 6 (20.0%) | ||
| Sampling | 121 | |||||
| No cough | 73 | 101 | 12 (16.4%) | |||
| Cough | 48 | 20 | 40 (83.3%) | 8 (16.7%) | ||
| Systematic | 187 | |||||
| No cough | 69 | 148 | 13 (18.8%) | |||
| Cough | 118 | 39 | 92 (78.0%) | 26 (22.0%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, X.; Xing, H.; Chen, P.; Ma, J.; Wang, X.; Mao, C.; Zhao, X.; Dai, F. Lymph Node Dissection Is a Risk Factor for Short-Term Cough after Pulmonary Resection. Curr. Oncol. 2022, 29, 294-307. https://doi.org/10.3390/curroncol29010027
Wu X, Xing H, Chen P, Ma J, Wang X, Mao C, Zhao X, Dai F. Lymph Node Dissection Is a Risk Factor for Short-Term Cough after Pulmonary Resection. Current Oncology. 2022; 29(1):294-307. https://doi.org/10.3390/curroncol29010027
Chicago/Turabian StyleWu, Xiaoli, Hanyang Xing, Ping Chen, Jihua Ma, Xintian Wang, Chengyi Mao, Xiaoying Zhao, and Fuqiang Dai. 2022. "Lymph Node Dissection Is a Risk Factor for Short-Term Cough after Pulmonary Resection" Current Oncology 29, no. 1: 294-307. https://doi.org/10.3390/curroncol29010027
APA StyleWu, X., Xing, H., Chen, P., Ma, J., Wang, X., Mao, C., Zhao, X., & Dai, F. (2022). Lymph Node Dissection Is a Risk Factor for Short-Term Cough after Pulmonary Resection. Current Oncology, 29(1), 294-307. https://doi.org/10.3390/curroncol29010027