Surgical Management of the Axilla in Invasive Lobular Carcinoma in the Z1071 Era: A Propensity-Score Matched Analysis of the National Cancer Database

 , ,
, ,
Abstract
:1. Introduction
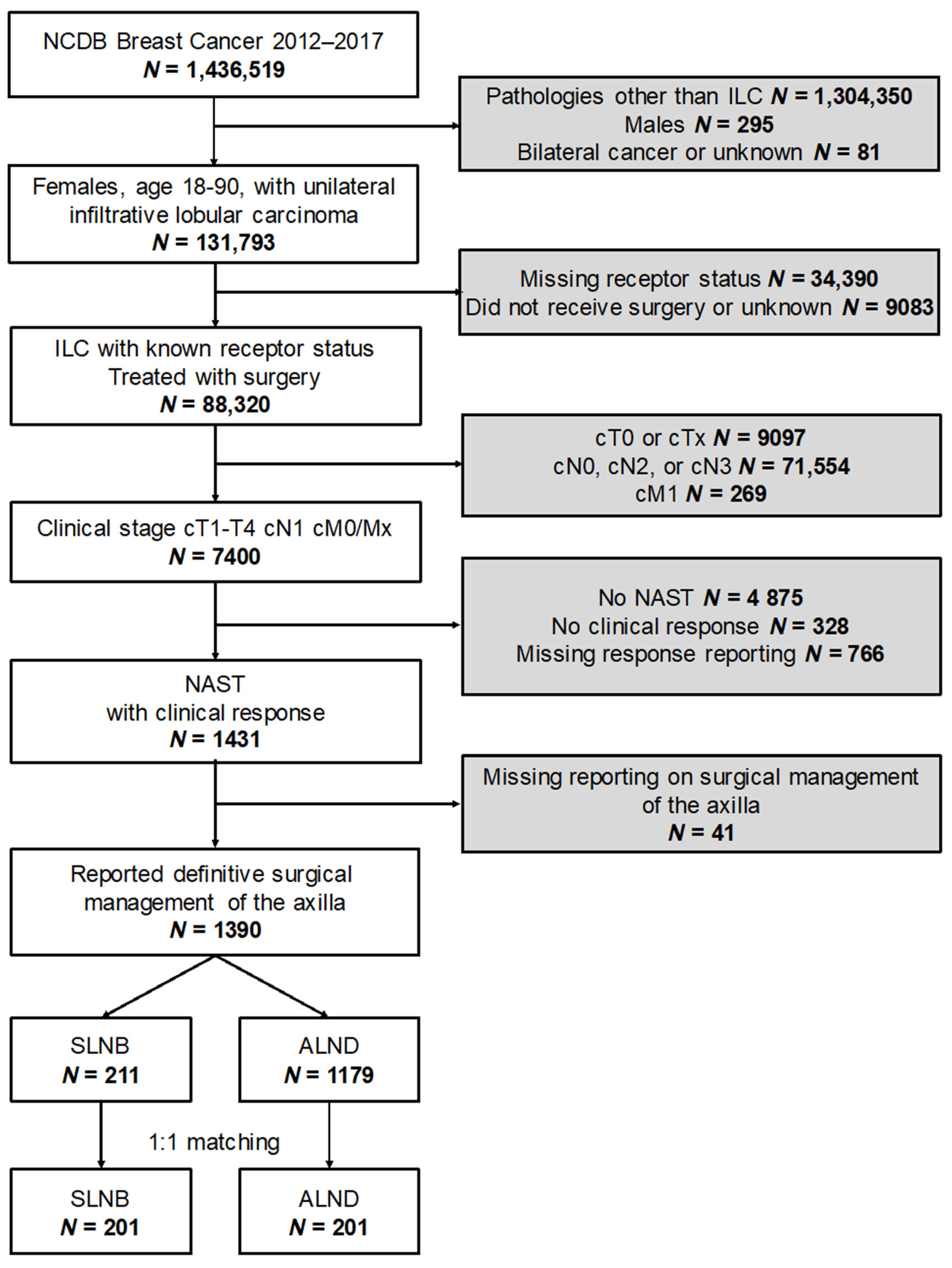
2. Methods
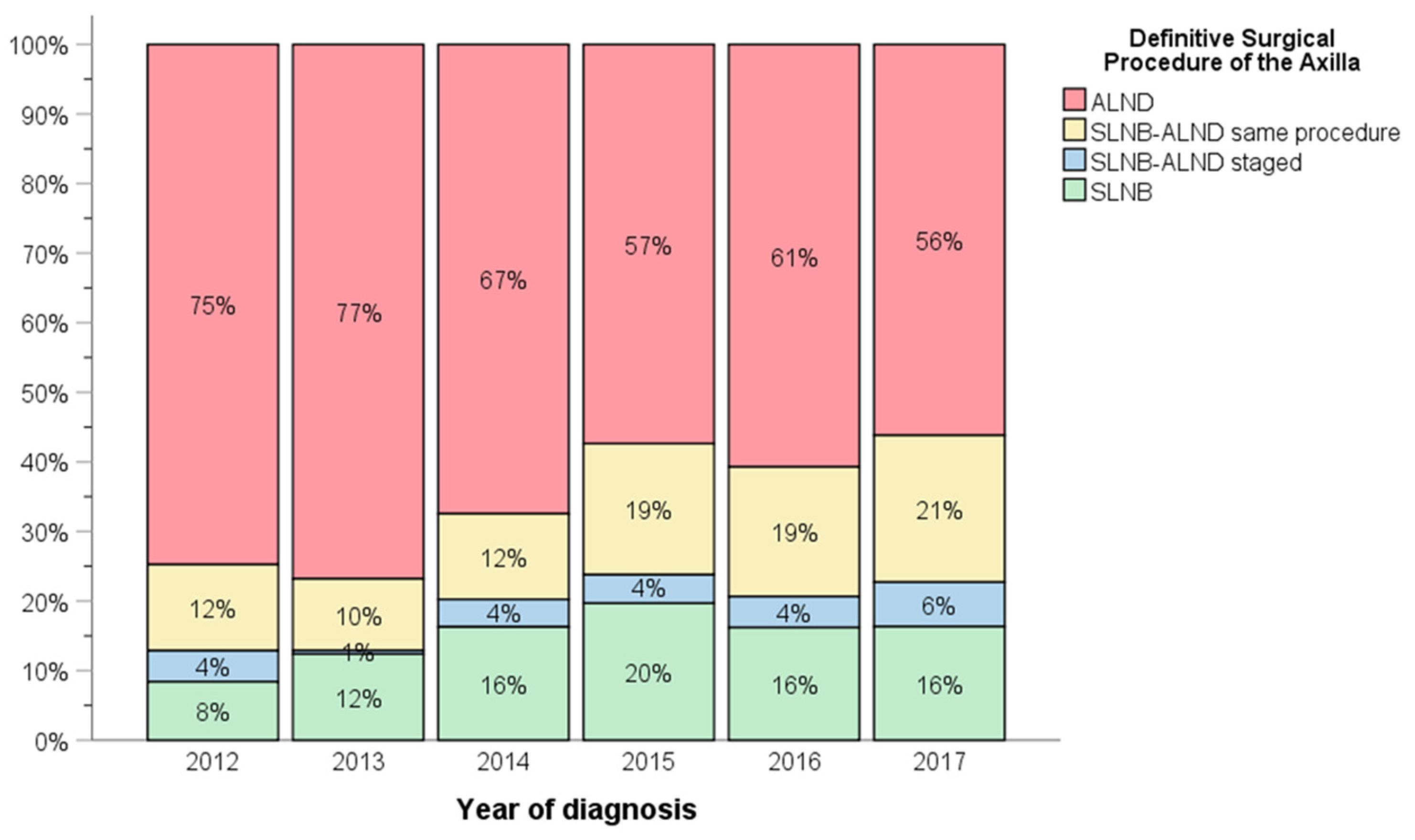
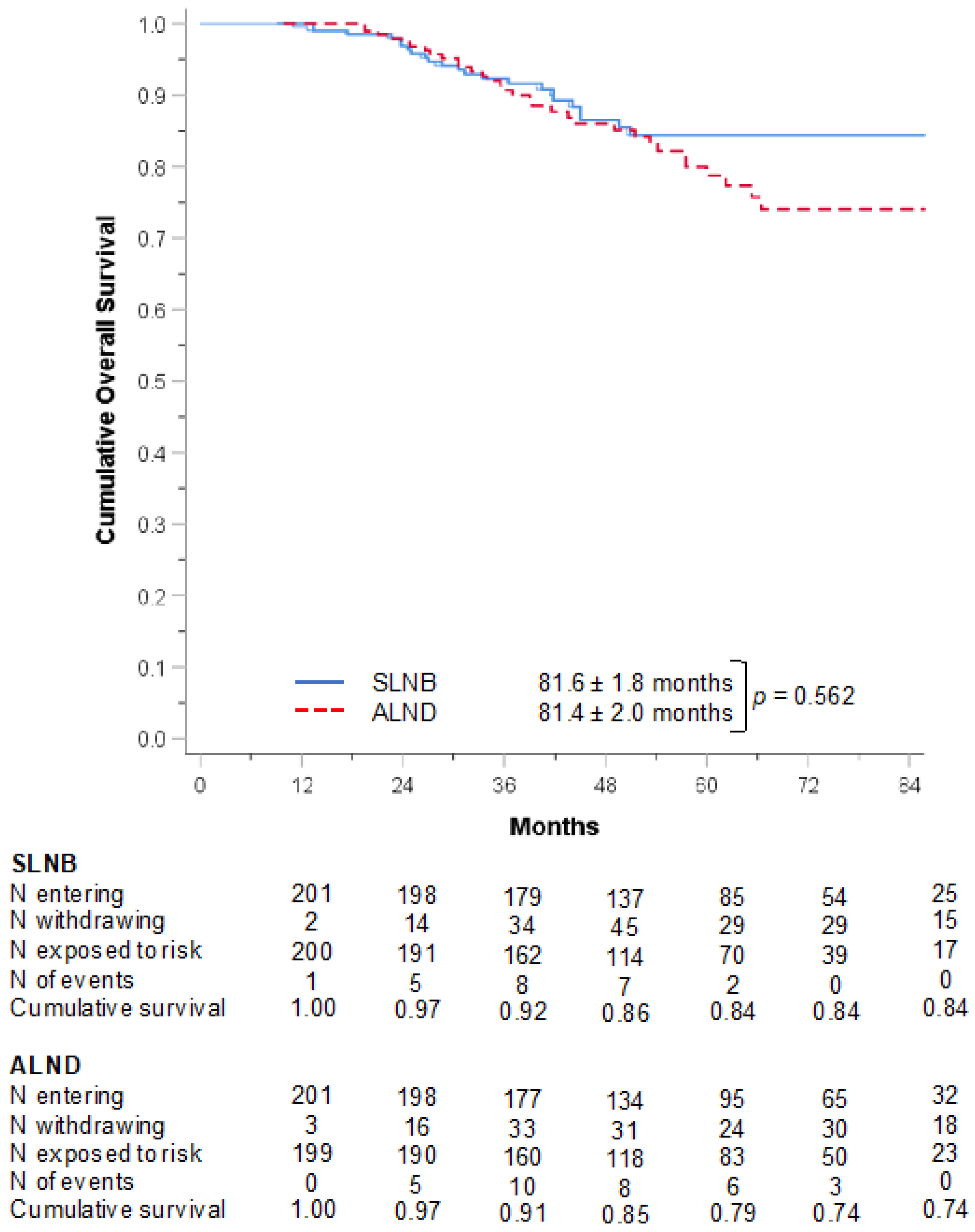
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Dossus, L.; Benusiglio, P.R. Lobular breast cancer: Incidence and genetic and non-genetic risk factors. Breast Cancer Res. 2015, 17, 37. [Google Scholar] [CrossRef] [Green Version]
- Li, C.I.; Uribe, D.J.; Daling, J.R. Clinical characteristics of different histologic types of breast cancer. Br. J. Cancer 2005, 93, 1046–1052. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Silverstein, M.J.; Lewinsky, B.S.; Waisman, J.R.; Gierson, E.D.; Colburn, W.J.; Senofsky, G.M.; Gemagami, P. Infiltrating lobular carcinoma. Is it different from infiltrating duct carcinoma? Cancer 1994, 73, 1673–1677. [Google Scholar] [CrossRef]
- Li, C.I.; Anderson, B.O.; Daling, J.R.; Moe, R.E. Trends in incidence rates of invasive lobular and ductal breast carcinoma. JAMA 2003, 289, 1421–1424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Evans, D.G.; Howell, S.J.; Gandhi, A.; van Veen, E.M.; Woodward, E.R.; Harvey, J.; Barr, L.; Wallace, A.; Lalloo, F.; Wilson, M.; et al. Breast cancer incidence and early diagnosis in a family history risk and prevention clinic: 33-year experience in 14,311 women. Breast Cancer Res. Treat. 2021, 189, 677–687. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, D.J.; Davey, M.G.; Barkley, L.R.; Kerin, M.J. Differences in sensitivity to neoadjuvant chemotherapy among invasive lobular and ductal carcinoma of the breast and implications on surgery-A systematic review and meta-analysis. Breast 2022, 61, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Krag, D.N.; Anderson, S.J.; Julian, T.B.; Brown, A.B.; Harlow, S.P.; Ashikaga, T.; Weaver, D.L.; Miller, B.J.; Jalovec, L.M.; Frazier, T.G.; et al. Technical outcomes of sentinel-lymph-node resection and conventional axillary-lymph-node dissection in patients with clinically node-negative breast cancer: Results from the NSABP B-32 randomised phase III trial. Lancet Oncol. 2007, 8, 881–888. [Google Scholar] [CrossRef]
- Hunt, K.K.; Yi, M.; Mittendorf, E.A.; Guerrero, C.; Babiera, G.V.; Bedrosian, I.; Hwang, R.F.; Kuerer, H.M.; Ross, M.I.; Meric-Bernstam, F. Sentinel lymph node surgery after neoadjuvant chemotherapy is accurate and reduces the need for axillary dissection in breast cancer patients. Ann. Surg. 2009, 250, 558–566. [Google Scholar] [CrossRef] [PubMed]
- Boughey, J.C.; Suman, V.J.; Mittendorf, E.A.; Ahrendt, G.M.; Wilke, L.G.; Taback, B.; Leitch, A.M.; Kuerer, H.M.; Bowling, M.; Flippo-Morton, T.S.; et al. Sentinel lymph node surgery after neoadjuvant chemotherapy in patients with node-positive breast cancer: The ACOSOG Z1071 (Alliance) clinical trial. JAMA 2013, 310, 1455–1461. [Google Scholar] [CrossRef] [PubMed]
- Thornton, M.J.; Williamson, H.V.; Westbrook, K.E.; Greenup, R.A.; Plichta, J.K.; Rosenberger, L.H.; Gupta, A.M.; Hyslop, T.; Hwang, E.S.; Fayanju, O.M. Neoadjuvant endocrine therapy versus neoadjuvant chemotherapy in node-positive invasive lobular carcinoma. Ann. Surg. Oncol. 2019, 26, 3166–3177. [Google Scholar] [CrossRef] [PubMed]
- Cao, L.; Sugumar, K.; Keller, E.; Li, P.; Rock, L.; Simpson, A.; Freyvogel, M.; Montero, A.J.; Shenk, R.; Miller, M.E. Neoadjuvant endocrine therapy as an alternative to neoadjuvant chemotherapy among hormone receptor positive breast cancer patients: Pathologic and surgical outcomes. Ann. Surg. Oncol. 2021, 28, 5730–5741. [Google Scholar] [CrossRef] [PubMed]
- Mukhtar, R.A.; Hoskin, T.L.; Habermann, E.B.; Day, C.N.; Boughey, J.C. Changes in management strategy and impact of neoadjuvant therapy on extent of surgery in invasive lobular carcinoma of the breast: Analysis of the national cancer database (NCDB). Ann. Surg. Oncol. 2021, 28, 5867–5877. [Google Scholar] [CrossRef] [PubMed]
- Giuliano, A.E.; Haigh, P.I.; Brennan, M.B.; Hansen, N.M.; Kelley, M.C.; Ye, W.; Glass, E.C.; Turner, R.R. Prospective observational study of sentinel lymphadenectomy without further axillary dissection in patients with sentinel node-negative breast cancer. J. Clin. Oncol. 2000, 18, 2553–2559. [Google Scholar] [CrossRef] [PubMed]
- Giuliano, A.E.; Hunt, K.K.; Ballman, K.V.; Beitsch, P.D.; Whitworth, P.W.; Blumencranz, P.W.; Leitch, A.M.; Saha, S.; McCall, L.M.; Morrow, M. Axillary dissection vs no axillary dissection in women with invasive breast cancer and sentinel node metastasis: A randomized clinical trial. JAMA 2011, 305, 569–575. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | N (%) | |
|---|---|---|
| Age | Mean ± SD (median) | 58.4 ± 10.3 (58) |
| Race/Ethnicity | White | 1077 (77.5%) |
| Black | 151 (10.9%) | |
| Other | 162 (11.7%) | |
| Charlson Score | 0 | 1186 (85.3%) |
| 1 | 166 (11.9%) | |
| 2 | 25 (1.8%) | |
| 3+ | 13 (0.9%) | |
| Laterality | Right | 677 (48.7%) |
| Left | 713 (51.3%) | |
| Receptor status | Luminal A | 1192 (85.8%) |
| Luminal B | 74 (5.3%) | |
| HR- HER2+ | 55 (4.0%) | |
| Triple negative | 69 (5.0%) | |
| Nottingham grade | Low | 231 (16.6%) |
| Intermediate | 817 (58.8%) | |
| High | 170 (12.2%) | |
| Not reported | 172 (12.4%) | |
| Clinical T stage | cT1 | 153 (11.0%) |
| cT2 | 475 (34.2%) | |
| cT3 | 594 (42.7%) | |
| cT4 | 168 (12.1%) | |
| Clinical response | ||
| Complete | 143 (10.3%) | |
| Partial | 1247 (89.7%) | |
| Breast surgery | Lumpectomy | 486 (35.0%) |
| Mastectomy | 904 (65.0%) | |
| Axillary management | SLNB | 211 (15.2%) |
| SLNB-ALND staged | 57 (4.1%) | |
| SLNB-ALND same | 221 (15.9%) | |
| ALND | 901 (64.8%) | |
| In-breast response | Complete response | 126 (9.1%) |
| Partial response | 561 (40.4%) | |
| No response | 703 (50.6%) | |
| Pathologic node status | Negative | 239 (17.2%) |
| Positive | 1151 (82.8%) | |
| Whole breast radiation | 446 (32.1%) | |
| Axillary radiation | 690 (49.6%) | |
| Endocrine therapy | 1175 (84.5%) | |
| Adjuvant systemic therapy | 827 (59.5%) |
| KERRYPNX | Unmatched Dataset | 1:1 Matched Dataset | ||||
|---|---|---|---|---|---|---|
| SLNB | ALND | p | SLNB | ALND | p | |
| N | 211 | 1179 | 201 | 201 | ||
| Age | 60.0 ± 10.8 | 58.1 ± 10.2 | 0.013 * | 59.8 ± 10.8 | 59.6 ± 10.7 | 0.886 |
| Race/Ethnicity | 0.932 | 0.326 | ||||
| White | 163 (77.3%) | 914 (77.5%) | 158 (78.6%) | 156 (77.6%) | ||
| Black | 22 (10.4%) | 129 (10.9%) | 21 (10.4%) | 29 (14.4%) | ||
| Other | 26 (12.3%) | 136 (11.5%) | 22 (10.9%) | 16 (8.0%) | ||
| Charlson Score | 0.593 | 0.836 | ||||
| 0 | 177 (83.9%) | 1009 (85.6%) | 169 (84.1%) | 164 (81.6%) | ||
| 1 | 30 (14.2%) | 136 (11.5%) | 28 (13.9%) | 34 (16.9%) | ||
| 2 | 3 (14%) | 22 (1.9%) | 3 (1.5%) | 2 (1.0%) | ||
| 3+ | 1 (0.5%) | 12 (1.0%) | 1 (0.5%) | 1 (0.5%) | ||
| Receptors | 0.493 | 0.913 | ||||
| Luminal A | 177 (83.9%) | 1015 (86.1%) | 169 (84.1%) | 170 (84.6%) | ||
| Luminal B | 10 (4.7%) | 64 (5.4%) | 10 (5.0%) | 11 (5.5%) | ||
| HR- HER2+ | 12 (5.7%) | 43 (3.6%) | 10 (5.0%) | 11 (5.5%) | ||
| Triple negative | 12 (5.7%) | 57 (4.8%) | 12 (6.0%) | 9 (4.5%) | ||
| Grade | 0.282 | 0.761 | ||||
| Low | 34 (16.1%) | 197 (16.7%) | 34 (16.9%) | 31 (15.4%) | ||
| Intermediate | 130 (61.6%) | 687 (58.3%) | 121 (60.2%) | 121 (60.2%) | ||
| High | 29 (13.7%) | 141 (12.0%) | 28 (13.9%) | 25 (12.4%) | ||
| Not reported | 18 (8.5%) | 154 (13.1%) | 18 (9.0%) | 24 (11.9%) | ||
| Clinical T stage | 0.040 * | 0.456 | ||||
| cT1 | 28 (13.3%) | 125 (10.6%) | 27 (13.4%) | 18 (9.0%) | ||
| cT2 | 80 (37.9%) | 395 (33.5%) | 76 (37.8%) | 73 (36.3%) | ||
| cT3 | 89 (42.2%) | 505 (42.8%) | 84 (41.8%) | 93 (46.3%) | ||
| cT4 | 14 (6.6%) | 154 (13.1%) | 14 (7.0%) | 17 (8.5%) | ||
| Clinical response | 0.073 | 0.401 | ||||
| Complete | 29 (13.7%) | 114 (9.7%) | 27 (13.4%) | 33 (16.4%) | ||
| Partial | 182 (86.3%) | 1065 (90.3%) | 174 (86.6%) | 168 (83.8%) | ||
| Breast surgery | <0.001 * | 0.690 | ||||
| Lumpectomy | 111 (52.6%) | 375 (31.8%) | 101 (50.2%) | 97 (48.3%) | ||
| Mastectomy | 100 (47.4%) | 804 (68.2%) | 100 (49.8%) | 104 (51.7%) | ||
| In-breast response | 0.037 * | 0.229 | ||||
| pCR | 29 (13.7%) | 97 (8.2%) | 27 (13.4%) | 30 (14.9%) | ||
| pPR | 81 (384%) | 480 (40.7%) | 75 (37.3%) | 89 (44.3%) | ||
| pNR | 101 (47.9%) | 602 (51.1%) | 99 (49.3%) | 82 (40.8%) | ||
| Path node status | <0.001 * | 0.835 | ||||
| Negative | 81 (38.4%) | 158 (13.4%) | 71 (35.3%) | 73 (36.3%) | ||
| Positive | 130 (61.6%) | 1021 (86.6%) | 130 (64.7%) | 128 (63.7%) | ||
| Adjuvant chemotherapy | 124 (58.8%) | 703 (59.6%) | 0.815 | 119 (59.2%) | 108 (53.7%) | 0.268 |
| Axillary radiation | 76 (36.0%) | 614 (52.1%) | <0.001 * | 76 (37.8%) | 75 (37.3%) | 0.918 |
| Endocrine therapy | 177 (83.9%) | 998 (84.6%) | 0.287 | 169 (84.1%) | 166 (82.6%) | 0.688 |
| Hazard Ratio (95% CI) | p | ||
|---|---|---|---|
| Age | 1.020 (1.007–1.033) | 0.002 * | |
| Grade | Low | Referent | |
| Intermediate | 1.881 (1.207–2.930) | 0.005 * | |
| High | 2.040 (1.170–3.558) | 0.012 * | |
| Not reported | 1.461 (0.847–2.521) | 0.173 | |
| Receptor status | Luminal A | Referent | |
| Luminal B | 0.940 (0.490–1.804) | 0.853 | |
| HR- HER2+ | 2.465 (1.331–4.565) | 0.004 * | |
| Triple negative | 3.202 (2.091–4.905) | <0.001 * | |
| Clinical response | Complete | Referent | |
| Partial | 2.496 (1.405–4.433) | 0.002 * | |
| Hazard Ratio (95% CI) | p | ||
|---|---|---|---|
| Age | 1.019 (1.005–1.034) | 0.010 * | |
| Receptor status | Luminal A | Referent | |
| Luminal B | 0.840 (0.341–2.071) | 0.705 | |
| HR- HER2+ | 4.616 (2.362–9.020) | <0.001 * | |
| Triple negative | 4.077 (2.496–6.662) | <0.001 * | |
| Clinical T stage | T1 | Referent | |
| T2 | 0.910 (0.530–1.561) | 0.732 | |
| T3 | 1.380 (0.825–2.308) | 0.221 | |
| T4 | 1.798 (1.114–3.232) | 0.030 * | |
| Clinical response | Complete | Referent | |
| Partial | 2.455 (1.180–5.108) | 0.016 * | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sinner, H.F.; Naffouje, S.; Selfridge, J.M.; Lee, M.C.; Hoover, S.J.; Laronga, C. Surgical Management of the Axilla in Invasive Lobular Carcinoma in the Z1071 Era: A Propensity-Score Matched Analysis of the National Cancer Database. Curr. Oncol. 2022, 29, 8197-8206. https://doi.org/10.3390/curroncol29110647
Sinner HF, Naffouje S, Selfridge JM, Lee MC, Hoover SJ, Laronga C. Surgical Management of the Axilla in Invasive Lobular Carcinoma in the Z1071 Era: A Propensity-Score Matched Analysis of the National Cancer Database. Current Oncology. 2022; 29(11):8197-8206. https://doi.org/10.3390/curroncol29110647
Chicago/Turabian StyleSinner, Heather F., Samer Naffouje, Julia M. Selfridge, Marie C. Lee, Susan J. Hoover, and Christine Laronga. 2022. "Surgical Management of the Axilla in Invasive Lobular Carcinoma in the Z1071 Era: A Propensity-Score Matched Analysis of the National Cancer Database" Current Oncology 29, no. 11: 8197-8206. https://doi.org/10.3390/curroncol29110647
APA StyleSinner, H. F., Naffouje, S., Selfridge, J. M., Lee, M. C., Hoover, S. J., & Laronga, C. (2022). Surgical Management of the Axilla in Invasive Lobular Carcinoma in the Z1071 Era: A Propensity-Score Matched Analysis of the National Cancer Database. Current Oncology, 29(11), 8197-8206. https://doi.org/10.3390/curroncol29110647