Tobacco Smoking Behaviors in Cancer Survivors: The Mediation Effect of Personality and Emotional Intelligence



Abstract
:1. Introduction
1.1. Smoking Behaviors and Personality
1.2. Smoking and the Management of Emotions
1.3. Aim and Hypothesis
2. Materials and Methods
2.1. Procedure and Measures
2.2. Data Analysis
3. Results
3.1. Participants
3.2. The Impact of the Diagnosis and Smoking Behaviors: Differences among Groups
3.3. Mediation Analyses
3.3.1. The Mediation Effect of Emotional Intelligence on Traumatic Experiences (IES)
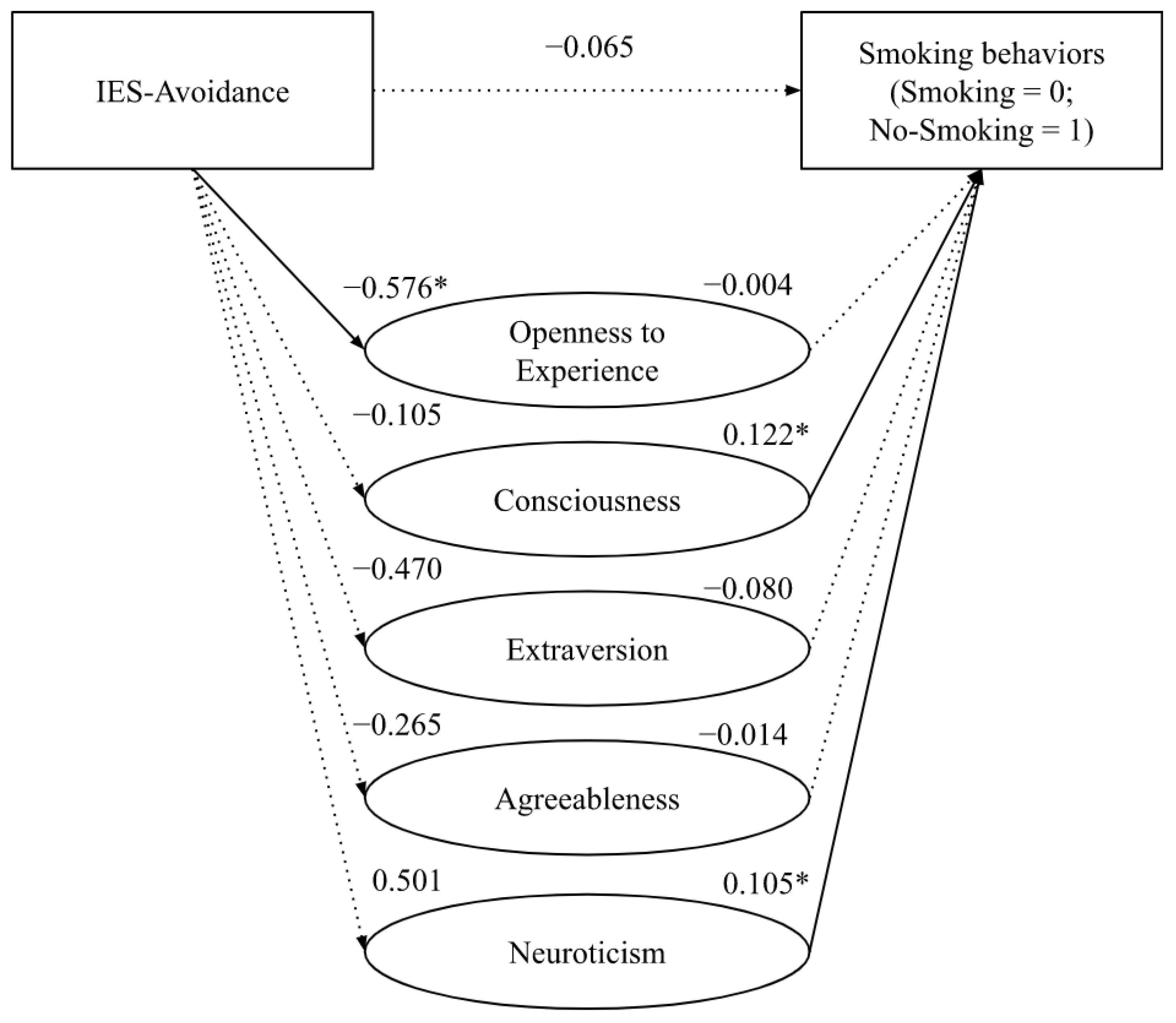
3.3.2. The Mediation Effect of Personality Traits on Traumatic Experiences (IES)
4. Discussion
Limitations and Future Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jassem, J. Tobacco smoking after diagnosis of cancer: Clinical aspects. Transl. Lung Cancer Res. 2019, 8 (Suppl. S1), S50. [Google Scholar] [CrossRef] [PubMed]
- Mullan, F. Seasons of Survivorship. N. Engl. J. Med. 1985, 313, 270–273. [Google Scholar] [CrossRef] [PubMed]
- De Pas, T.M.; Toffalorio, F.; Giovannetti, E.; Radice, D.; Russo, F.; Angeli, I.; Calamai, G.; Spitaleri, G.; Catania, C.; Noberasco, C.; et al. Optimizing pemetrexed-gemcitabine combination in patients with advanced non-small cell lung cancer: A pharmacogenetic approach. J. Thorac. Oncol. 2011, 6, 768–773. [Google Scholar] [CrossRef] [PubMed]
- Gritz, E.R.; Toll, B.A.; Warren, G.W. Tobacco use in the oncology setting: Advancing clinical practice and research. Cancer Epidemiol. Biomark. Prev. 2014, 23, 3–9. [Google Scholar] [CrossRef] [Green Version]
- Toll, B.A.; Brandon, T.H.; Gritz, E.R.; Warren, G.W.; Herbst, R.S. Assessing Tobacco Use by Cancer Patients and Facilitating Cessation: An American Association for Cancer Research Policy StatementAACR Tobacco Statement. Clin. Cancer Res. 2013, 19, 1941–1948. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petros, W.P.; Younis, I.R.; Ford, J.N.; Weed, S.A. Effects of tobacco smoking and nicotine on cancer treatment. Pharmacother. J. Hum. Pharmacol. Drug Ther. 2012, 32, 920–931. [Google Scholar] [CrossRef] [Green Version]
- Lucchiari, C.; Masiero, M.; Botturi, A.; Pravettoni, G. Helping patients to reduce tobacco consumption in oncology: A narrative review. SpringerPlus 2016, 5, 1–18. [Google Scholar] [CrossRef] [Green Version]
- Lucchiari, C.; Masiero, M.; Veronesi, G.; Maisonneuve, P.; Spina, S.; Jemos, C.; Salè, E.O.; Pravettoni, G. Benefits of E-cigarettes Among heavy smokers undergoing a lung cancer screening program: Randomized controlled trial protocol. JMIR Res. Protoc. 2016, 5, e4805. [Google Scholar] [CrossRef]
- Eysenck, H.J.; Tarrant, M.; Woolf, M.; England, L. Smoking and personality. Br. Med. J. 1960, 1, 1456. [Google Scholar] [CrossRef] [Green Version]
- Bolger, N.; Schilling, E.A. Personality and the problems of everyday life: The role of neuroticism in exposure and reactivity to daily stressors. J. Personal. 1991, 59, 355–386. [Google Scholar] [CrossRef]
- Sutin, A.R.; Terracciano, A.; Deiana, B.; Naitza, S.; Ferrucci, L.; Uda, M.; Schlessinger, D.; Costa, P.T. High neuroticism and low conscientiousness are associated with interleukin-6. Psychol. Med. 2010, 40, 1485–1493. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Contrada, R.J.; Cather, C.; O’Leary, A. Personality and health: Dispositions and processes in disease susceptibility and adaptation to illness. In Handbook of Personality: Theory and Research; Pervin, L.A., John, O.P., Eds.; Guilford Press: New York, NY, USA, 1999; pp. 576–604. [Google Scholar]
- Terracciano, A.; Costa, P.T., Jr. Smoking and the Five-Factor Model of personality. Addiction 2004, 99, 472–481. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Turiano, N.A.; Whiteman, S.D.; Hampson, S.E.; Roberts, B.W.; Mroczek, D.K. Personality and substance use in midlife: Conscientiousness as a moderator and the effects of trait change. J. Res. Personal. 2012, 46, 295–305. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Friedman, H.S. Long-term relations of personality and health: Dynamisms, mechanisms, tropisms. J. Personal. 2000, 68, 1089–1107. [Google Scholar] [CrossRef]
- Weston, S.J.; Jackson, J.J. Identification of the healthy neurotic: Personality traits predict smoking after disease onset. J. Res. Personal. 2015, 54, 61–69. [Google Scholar] [CrossRef]
- Costa, P.T., Jr.; McCrae, R.R. Neuroticism, somatic complaints, and disease: Is the bark worse than the bite? J. Personal. 1987, 55, 299–316. [Google Scholar] [CrossRef]
- Bogg, T. Conscientiousness, the transtheoretical model of change, and exercise: A neo-socioanalytic integration of trait and social-cognitive frameworks in the prediction of behavior. J. Personal. 2008, 76, 775–802. [Google Scholar] [CrossRef]
- Hill, P.L.; Roberts, B.W. The role of adherence in the relationship between conscientiousness and perceived health. Health Psychol. 2011, 30, 797–804. [Google Scholar] [CrossRef] [Green Version]
- Vollrath, M.; Torgersen, S. Who takes health risks? A probe into eight personality types. Personal. Individ. Differ. 2002, 32, 1185–1197. [Google Scholar] [CrossRef]
- Cloninger, C.R.; Sigvardsson, S.; Przybeck, T.R.; Svrakic, D.M. Personality antecedents of alcoholism in a national area probability sample. Eur. Arch. Psychiatry Clin. Neurosci. 1995, 245, 239–244. [Google Scholar] [CrossRef]
- Cloninger, C.R.; Svrakic, D.M.; Przybeck, T.R. A psychobiological model of temperament and character. Arch. Gen. Psychiatry 1993, 50, 975–990. [Google Scholar] [CrossRef] [PubMed]
- Hartman, C.; Hopfer, C.; Corley, R.; Hewitt, J.; Stallings, M. Using Cloninger’s temperament scales to predict substance-related behaviors in adolescents: A prospective longitudinal study. Am. J. Addict. 2013, 22, 246–251. [Google Scholar] [CrossRef] [PubMed]
- Etter, J.F. Smoking and Cloningers temperament and character inventory. Nicotine Tob. Res. 2010, 12, 919–926. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Munafo, M.R.; Zetteler, J.I.; Clark, T.G. Personality and smoking status: A meta-analysis. Nicotine Tob. Res. 2007, 9, 405–413. [Google Scholar] [CrossRef] [PubMed]
- Masiero, M.; Cutica, I.; Mazzocco, K.; Zunino, A.; Cropley, M.; Pravettoni, G. A Comprehensive Model of Tobacco Cigarette Smoking in Adolescence: The Role of Attachment Style and Personality. J. Psychol. 2021, 155, 589–605. [Google Scholar] [CrossRef]
- Khantzian, E.J. The self-medication hypothesis of substance use disorders: A reconsideration and recent applications. Harv. Rev. Psychiatry 1997, 4, 231–244. [Google Scholar] [CrossRef]
- Currie, S.R. Confirmatory factor analysis of the Reasons for Smoking Scale in alcoholics. Nicotine Tob. Res. 2004, 6, 465–470. [Google Scholar] [CrossRef]
- Masiero, M.; Cropley, M.; Pravettoni, G. Increasing smoking cessation adherence: Do we need to consider the role of executive function and rumination? Eur. J. Psychol. 2020, 16, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Tomkins, S.S. Psychological model for smoking behavior. Am. J. Public Health Nations Health 1966, 56 (Suppl. S12), 17–20. [Google Scholar] [CrossRef]
- Williams, F.; Jeanetta, S.C. Lived experiences of breast cancer survivors after diagnosis, treatment and beyond: Qualitative study. Health Expect. 2016, 19, 631–642. [Google Scholar] [CrossRef]
- Lucas, A.R.; Focht, B.C.; Cohn, D.E.; Klatt, M.D.; Buckworth, J. Recruiting endometrial cancer survivors to studies examining lifestyle behaviors and quality of life: Challenges faced and lessons learned. J. Cancer Educ. 2018, 33, 857–864. [Google Scholar] [CrossRef] [PubMed]
- Sebri, V.; Durosini, I.; Triberti, S.; Pravettoni, G. The efficacy of psychological intervention on body image in breast cancer patients and survivors: A systematic-review and meta-analysis. Front. Psychol. 2021, 12, 611954. [Google Scholar] [CrossRef] [PubMed]
- Słowik, A.J.; Jabłoński, M.J.; Michałowska-Kaczmarczyk, A.M.; Jach, R. Evaluation of quality of life in women with breast cancer, with particular emphasis on sexual satisfaction, future perspectives and body image, depending on the method of surgery. Psychiatr. Pol. 2017, 51, 871–888. [Google Scholar] [CrossRef] [PubMed]
- Mazzocco, K.; Masiero, M.; Carriero, M.C.; Pravettoni, G. The role of emotions in cancer patients decision-making. Ecancermedicalscience 2019, 13, 914. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Durosini, I.; Pravettoni, G. Emozioni e salute: Commento all articolo bersaglio di Grecucci, Messina e Monachesi. G. Ital. Psicol. 2021, 48, 773–778. [Google Scholar] [CrossRef]
- Dunn, L.B.; Langford, D.J.; Paul, S.M.; Berman, M.B.; Shumay, D.M.; Kober, K.; Merriman, J.; West, C.; Neuhaus, J.M.; Miaskowski, C. Trajectories of fear of recurrence in women with breast cancer. Support. Care Cancer 2015, 23, 2033–2043. [Google Scholar] [CrossRef] [Green Version]
- Williamson, T.J.; Ostroff, J.S.; Haque, N.; Martin, C.M.; Hamann, H.A.; Banerjee, S.C.; Shen, M.J. Dispositional shame and guilt as predictors of depressive symptoms and anxiety among adults with lung cancer: The mediational role of internalized stigma. Stigma Health 2020, 5, 425–433. [Google Scholar] [CrossRef]
- McBride, C.M.; Ostroff, J.S. Teachable moments for promoting smoking cessation: The context of cancer care and survivorship. Cancer Control 2003, 10, 325–333. [Google Scholar] [CrossRef]
- Trinidad, D.R.; Unger, J.B.; Chou, C.P.; Johnson, C.A. Emotional intelligence and acculturation to the United States: Interactions on the perceived social consequences of smoking in early adolescents. Subst. Use Misuse 2005, 40, 1697–1706. [Google Scholar] [CrossRef]
- Kun, B.; Urbán, R.; Paksi, B.; Griffiths, M.D.; Richman, M.J.; Demetrovics, Z. The effects of trait emotional intelligence on adolescent substance use: Findings from a Hungarian representative survey. Front. Psychiatry 2019, 10, 367. [Google Scholar] [CrossRef]
- González-Yubero, S.; Lázaro-Visa, S.; Palomera Martín, R. The protective association of trait and ability emotional intelligence with adolescent tobacco use. Int. J. Environ. Res. Public Health 2020, 17, 6865. [Google Scholar] [CrossRef] [PubMed]
- Salovey, P.; Mayer, J.D. Emotional intelligence. Imagin. Cogn. Personal. 1990, 9, 185–211. [Google Scholar] [CrossRef]
- Goleman, D.P. Emotional Intelligence: Why It Can Matter More than IQ for Character, Health and Lifelong Achievement; Bantam Books: New York, NY, USA, 1995. [Google Scholar]
- Schutte, N.S.; Malouff, J.M.; Hall, L.E.; Haggerty, D.J.; Cooper, J.T.; Golden, C.J.; Dornheim, L. Development and validation of a measure of emotional intelligence. Personal. Individ. Differ. 1998, 25, 167–177. [Google Scholar] [CrossRef]
- Mayer, J.D.; Caruso, D.R.; Salovey, P. The ability model of emotional intelligence: Principles and updates. Emot. Rev. 2016, 8, 290–300. [Google Scholar] [CrossRef] [Green Version]
- Petrides, K.V. Ability and trait emotional intelligence. In The Wiley-Blackwell Handbook of Individual Differences; Chamorro-Premuzic, T., von Stumm, S., Furnham, A., Eds.; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2011; pp. 656–678. [Google Scholar]
- Davies, K.A.; Lane, A.M.; Devonport, T.J.; Scott, J.A. Validity and reliability of a brief emotional intelligence scale (BEIS-10). J. Individ. Differ. 2010, 31, 198–208. [Google Scholar] [CrossRef] [Green Version]
- Durosini, I.; Triberti, S.; Ongaro, G.; Pravettoni, G. Validation of the Italian version of the brief emotional intelligence scale (BEIS-10). Psychol. Rep. 2021, 124, 2356–2376. [Google Scholar] [CrossRef]
- Limonero, J.T.; Tomás-Sábado, J.; Fernández-Castro, J. Perceived emotional intelligence and its relation to tobacco and cannabis use among university students. Psicothema 2006, 18, 95–100. [Google Scholar]
- Megías-Robles, A.; Perea-Baena, J.M.; Fernández-Berrocal, P. The protective role of emotional intelligence in smoking relapse during a 12-month follow-up smoking cessation intervention. PLoS ONE 2020, 15, e0234301. [Google Scholar] [CrossRef]
- John, O.P.; Srivastava, S. The Big-Five trait taxonomy: History, measurement, and theoretical perspectives. In Handbook of Personality: Theory and Research; Pervin, L.A., John, O.P., Eds.; Guilford Press: New York, NY, USA, 1999; Volume 2, pp. 102–138. [Google Scholar]
- Ubbiali, A.; Chiorri, C.; Hampton, P. Italian big five inventory. Psychometric properties of the Italian adaptation of the big five inventory (BFI). BPA-Appl. Psychol. Bull. (Boll. Psicol. Appl.) 2013, 59, 37–48. [Google Scholar]
- Horowitz, M.; Wilner, N.; Alvarez, W. Impact of Event Scale: A measure of subjective stress. Psychosom. Med. 1979, 41, 209–218. [Google Scholar] [CrossRef] [Green Version]
- Pietrantonio, F.; De Gennaro, L.; Di Paolo, M.C.; Solano, L. The impact of event scale: Validation of an Italian version. J. Psychosom. Res. 2003, 55, 389–393. [Google Scholar] [CrossRef]
- Heatherton, T.F.; Kozlowski, L.T.; Frecker, R.C.; Fagerstrom, K.O. The Fagerström test for nicotine dependence: A revision of the Fagerstrom Tolerance Questionnaire. Br. J. Addict. 1991, 86, 1119–1127. [Google Scholar] [CrossRef] [PubMed]
- Fekketich, A.K.; Fossati, R.; Apolone, G. An evaluation of the Italian version of the Fagerström Test for Nicotine Dependence. Psychol. Rep. 2008, 102, 687–694. [Google Scholar] [CrossRef] [PubMed]
- Preacher, K.J.; Hayes, A.F. Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behav. Res. Methods 2008, 40, 879–891. [Google Scholar] [CrossRef] [PubMed]
- Hayes, A.F.; Scharkow, M. The relative trustworthiness of inferential tests of the indirect effect in statistical mediation analysis: Does method really matter? Psychol. Sci. 2013, 24, 1918–1927. [Google Scholar] [CrossRef]
- Triberti, S.; Durosini, I.; Pravettoni, G. Social distancing is the right thing to do: Dark Triad behavioral correlates in the COVID-19 quarantine. Personal. Individ. Differ. 2021, 170, 110453. [Google Scholar] [CrossRef]
- Masiero, M.; Renzi, C.; Mazzocco, K.; Pravettoni, G. Not Just a Pill: Toward a Tailored Antismoking Intervention for Respiratory Diseases. J. Addict. Nurs. 2019, 30, E1–E4. [Google Scholar] [CrossRef]
- Masiero, M.; Lucchiari, C.; Maisonneuve, P.; Pravettoni, G.; Veronesi, G.; Mazzocco, K. The attentional bias in current and former smokers. Front. Behav. Neurosci. 2019, 13, 154. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Smokers (n = 51) | Non-Smokers (n = 43) | |||||
|---|---|---|---|---|---|---|
| Descriptive Data | n | % | n | % | X2 (df) | p |
| Tumor | 7.62 (8) | 0.471 | ||||
| Breast | 41 | 85.4 | 37 | 86.0 | ||
| Bowel | 1 | 2.1 | 1 | 2.3 | ||
| Lung | 0 | 0 | 1 | 2.3 | ||
| Pancreas | 1 | 2.1 | 0 | 0 | ||
| Kidney | 1 | 2.1 | 0 | 0 | ||
| Uterus | 4 | 8.3 | 2 | 4.7 | ||
| Skin | 0 | 0 | 1 | 2.3 | ||
| Bones | 0 | 0 | 1 | 2.3 | ||
| Level of education | 3.561 (3) | 0.313 | ||||
| Secondary school | 5 | 9.8 | 2 | 4.7 | ||
| High school | 22 | 43.1 | 15 | 34.9 | ||
| Master Degree | 17 | 33.3 | 14 | 32.6 | ||
| Post University Degree | 7 | 13.7 | 12 | 27.9 | ||
| Employment | 6.87 (3) | 0.076 | ||||
| Unemployed | 13 | 25.5 | 6 | 14.0 | ||
| White collar | 26 | 51 | 24 | 55.8 | ||
| Blue collar | 8 | 15.7 | 3 | 7.0 | ||
| Self-employed/director | 4 | 7.8 | 10 | 23.3 | ||
| Smokers | Non-Smokers | t (df) | p | |
|---|---|---|---|---|
| IES-Intrusion | 17.43 (4.96) | 18.83 (5.98) | −1.20 (86) | 0.232 |
| IES-Avoidance | 7.38 (2.13) | 7.47 (2.74) | −0.160 (88) | 0.874 |
| Effect (β) | SE | 95% CI | |
|---|---|---|---|
| IES-Intrusion | |||
| Appraisal of own emotions | −0.003 | 0.017 | [−0.04; 0.03] |
| Appraisal of others’ emotions | −0.001 | 0.013 | [−0.03; 0.03] |
| Regulation of own emotions | 0.018 | 0.019 | [−0.01; 0.06] |
| Regulation of others’ emotions | 0.007 | 0.014 | [−0.04; 0.02] |
| Utilization of emotions | 0.032 | 0.029 | [0.00; 0.10] |
| IES-Avoidance | |||
| Appraisal of own emotions | −0.006 | 0.048 | [−0.11; 0.09] |
| Appraisal of others’ emotions | −0.012 | 0.047 | [−0.12; 0.08] |
| Regulation of own emotions | 0.015 | 0.040 | [−0.06; 0.11] |
| Regulation of others’ emotions | −0.019 | 0.029 | [−0.09; 0.03] |
| Utilization of emotions | 0.082 | 0.058 | [0.00; 0.22] |
| IES-Intrusion | |||
| Openness to Experience | 0.003 | 0.011 | [−0.02; 0.03] |
| Conscientiousness | 0.008 | 0.018 | [−0.02; 0.05] |
| Extraversion | 0.004 | 0.013 | [−0.03; 0.03] |
| Agreeableness | 0.001 | 0.009 | [−0.02; 0.02] |
| Neuroticism | 0.039 | 0.030 | [0.00; 0.11] |
| IES-Avoidance | |||
| Openness to Experience | 0.003 | 0.034 | [−0.07; 0.08] |
| Conscientiousness | −0.013 | 0.041 | [−0.10; 0.07] |
| Extraversion | 0.038 | 0.041 | [−0.02; 0.14] |
| Agreeableness | 0.004 | 0.025 | [−0.04; 0.07] |
| Neuroticism | 0.053 | 0.050 | [0.00; 0.18] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Durosini, I.; Masiero, M.; Casini, C.; Pravettoni, G. Tobacco Smoking Behaviors in Cancer Survivors: The Mediation Effect of Personality and Emotional Intelligence. Curr. Oncol. 2022, 29, 9437-9451. https://doi.org/10.3390/curroncol29120742
Durosini I, Masiero M, Casini C, Pravettoni G. Tobacco Smoking Behaviors in Cancer Survivors: The Mediation Effect of Personality and Emotional Intelligence. Current Oncology. 2022; 29(12):9437-9451. https://doi.org/10.3390/curroncol29120742
Chicago/Turabian StyleDurosini, Ilaria, Marianna Masiero, Chiara Casini, and Gabriella Pravettoni. 2022. "Tobacco Smoking Behaviors in Cancer Survivors: The Mediation Effect of Personality and Emotional Intelligence" Current Oncology 29, no. 12: 9437-9451. https://doi.org/10.3390/curroncol29120742
APA StyleDurosini, I., Masiero, M., Casini, C., & Pravettoni, G. (2022). Tobacco Smoking Behaviors in Cancer Survivors: The Mediation Effect of Personality and Emotional Intelligence. Current Oncology, 29(12), 9437-9451. https://doi.org/10.3390/curroncol29120742