Gadoxetic Acid-Based MRI for Decision-Making in Hepatocellular Carcinoma Employing Perfusion Criteria Only—A Post Hoc Analysis from the SORAMIC Trial Diagnostic Cohort

 , ,
, ,  , , , and
, , , and
Abstract
:
1. Introduction
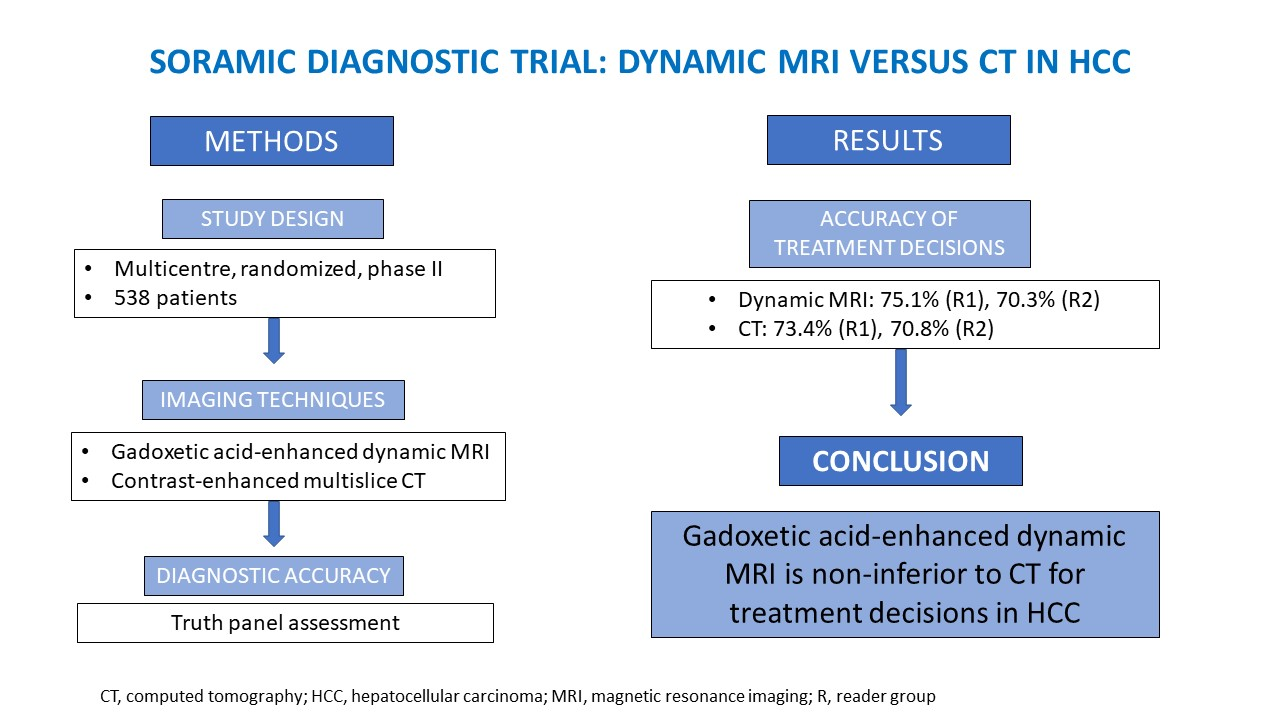
2. Materials and Methods
3. Results
3.1. Accuracy of Treatment Decisions
3.2. Diagnostic Confidence
3.3. Detection Rate of Lesions
3.4. Artefacts
3.5. Portal Vein Thrombosis and Portal Vein or Other Macrovascular Invasion
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Perz, J.F.; Armstrong, G.L.; Farrington, L.A.; Hutin, Y.J.; Bell, B.P. The Contributions of Hepatitis B Virus and Hepatitis C Virus Infections to Cirrhosis and Primary Liver Cancer Worldwide. J. Hepatol. 2006, 45, 529–538. [Google Scholar] [CrossRef] [PubMed]
- Recio-Boiles, A.; Hoilat, G.J.; Smith, M.; Babiker, H.M. Hepatobiliary Tract Cancer; StatPearls Publishing: Treasure Island, FL, USA, 2020. [Google Scholar]
- Omata, M.; Cheng, A.L.; Kokudo, N.; Kudo, M.; Lee, J.M.; Jia, J.; Tateishi, R.; Han, K.H.; Chawla, Y.K.; Shiina, S.; et al. Asia-Pacific Clinical Practice Guidelines on the Management of Hepatocellular Carcinoma: A 2017 Update. Hepatol. Int. 2017, 11, 317–370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- LI-RADS. CT/MRI LI-RADS v2018. Available online: https://www.acr.org/Clinical-Resources/Reporting-and-Data-Systems/LI-RADS/CT-MRI-LI-RADS-v2018 (accessed on 5 August 2021).
- European Association for the Study of the Liver EASL Clinical Practice Guidelines: Management of Hepatocellular Carcinoma. J. Hepatol. 2018, 69, 182–236. [CrossRef] [PubMed] [Green Version]
- Ricke, J.; Klümpen, H.J.; Amthauer, H.; Bargellini, I.; Bartenstein, P.; de Toni, E.N.; Gasbarrini, A.; Pech, M.; Peck-Radosavljevic, M.; Popovič, P.; et al. Impact of Combined Selective Internal Radiation Therapy and Sorafenib on Survival in Advanced Hepatocellular Carcinoma. J. Hepatol. 2019, 71, 1164–1174. [Google Scholar] [CrossRef] [PubMed]
- Ricke, J.; Steffen, I.G.; Bargellini, I.; Berg, T.; Bilbao Jaureguizar, J.I.; Gebauer, B.; Iezzi, R.; Loewe, C.; Karçaaltincaba, M.; Pech, M.; et al. Gadoxetic Acid-Based Hepatobiliary MRI in Hepatocellular Carcinoma. JHEP Rep. Innov. Hepatol. 2020, 2, 100173. [Google Scholar] [CrossRef] [PubMed]
- Heimbach, J.K.; Kulik, L.M.; Finn, R.S.; Sirlin, C.B.; Abecassis, M.M.; Roberts, L.R.; Zhu, A.X.; Murad, M.H.; Marrero, J.A. AASLD Guidelines for the Treatment of Hepatocellular Carcinoma. Hepatology 2018, 67, 358–380. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fowler, K.J.; Sirlin, C.B. Is It Time to Expand the Definition of Washout Appearance in LI-RADS? Radiology 2019, 291, 658–659. [Google Scholar] [CrossRef] [PubMed]
- Joo, I.; Lee, J.M.; Lee, D.H.; Jeon, J.H.; Han, J.K.; Choi, B.I. Noninvasive Diagnosis of Hepatocellular Carcinoma on Gadoxetic Acid-Enhanced MRI: Can Hypointensity on the Hepatobiliary Phase Be Used as an Alternative to Washout? Eur. Radiol. 2015, 25, 2859–2868. [Google Scholar] [CrossRef] [PubMed]
- Kim, R.; Lee, J.M.; Shin, C.I.; Lee, E.S.; Yoon, J.H.; Joo, I.; Kim, S.H.; Hwang, I.; Han, J.K.; Choi, B.I. Differentiation of Intrahepatic Mass-Forming Cholangiocarcinoma from Hepatocellular Carcinoma on Gadoxetic Acid-Enhanced Liver MR Imaging. Eur. Radiol. 2016, 26, 1808–1817. [Google Scholar] [CrossRef] [PubMed]
- Choi, S.H.; Lee, S.S.; Kim, S.Y.; Park, S.H.; Park, S.H.; Kim, K.M.; Hong, S.M.; Yu, E.; Lee, M.G. Intrahepatic Cholangiocarcinoma in Patients with Cirrhosis: Differentiation from Hepatocellular Carcinoma by Using Gadoxetic Acid-Enhanced MR Imaging and Dynamic CT. Radiology 2017, 282, 771–781. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.H.; Choi, S.H.; Kim, S.Y.; Kim, M.J.; Lee, S.S.; Byun, J.H. Gadoxetic Acid-Enhanced MRI of Hepatocellular Carcinoma: Value of Washout in Transitional and Hepatobiliary Phases. Radiology 2019, 292, 270. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baek, K.A.; Kim, S.S.; Shin, H.C.; Hwang, J.A.; Choi, S.Y.; Lee, W.H.; Park, C.H.; Lee, H.N.; Heo, N.H. Gadoxetic Acid-Enhanced MRI for Diagnosis of Hepatocellular Carcinoma in Patients with Chronic Liver Disease: Can Hypointensity on the Late Portal Venous Phase Be Used as an Alternative to Washout? Abdom. Radiol. N. Y. 2020, 45, 2705–2716. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.J.; Lee, J.M.; Lee, J.S.; Lee, H.Y.; Park, B.H.; Kim, Y.H.; Han, J.K.; Choi, B.I. Hepatocellular Carcinoma: Diagnostic Performance of Multidetector CT and MR Imaging-a Systematic Review and Meta-Analysis. Radiology 2015, 275, 97–109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, X.; Zou, L.; Liu, F.; Zhou, Y.; Song, B. Gadoxetic Acid Disodium-Enhanced Magnetic Resonance Imaging for the Detection of Hepatocellular Carcinoma: A Meta-Analysis. PLoS ONE 2013, 8, e70896. [Google Scholar] [CrossRef] [Green Version]
- Haradome, H.; Grazioli, L.; Tinti, R.; Morone, M.; Motosugi, U.; Sano, K.; Ichikawa, T.; Kwee, T.C.; Colagrande, S. Additional Value of Gadoxetic Acid-DTPA-Enhanced Hepatobiliary Phase MR Imaging in the Diagnosis of Early-Stage Hepatocellular Carcinoma: Comparison with Dynamic Triple-Phase Multidetector CT Imaging. J. Magn. Reson. Imaging 2011, 34, 69–78. [Google Scholar] [CrossRef] [PubMed]
- Di Martino, M.; Marin, D.; Guerrisi, A.; Baski, M.; Galati, F.; Rossi, M.; Brozzetti, S.; Masciangelo, R.; Passariello, R.; Catalano, C. Intraindividual Comparison of Gadoxetate Disodium-Enhanced MR Imaging and 64-Section Multidetector CT in the Detection of Hepatocellular Carcinoma in Patients with Cirrhosis. Radiology 2010, 256, 806–816. [Google Scholar] [CrossRef] [PubMed]
- Semaan, S.; Vietti Violi, N.; Lewis, S.; Chatterji, M.; Song, C.; Besa, C.; Babb, J.S.; Fiel, M.I.; Schwartz, M.; Thung, S.; et al. Hepatocellular Carcinoma Detection in Liver Cirrhosis: Diagnostic Performance of Contrast-Enhanced CT vs. MRI with Extracellular Contrast vs. Gadoxetic Acid. Eur. Radiol. 2020, 30, 1020–1030. [Google Scholar] [CrossRef] [PubMed]
- Erra, P.; Puglia, M.; Ragozzino, A.; Maurea, S.; Liuzzi, R.; Sabino, G.; Barbuto, L.; Cuocolo, A.; Imbriaco, M. Appearance of Hepatocellular Carcinoma on Gadoxetic Acid-enhanced Hepato-biliary Phase MR Imaging: A Systematic Review. Radiol. Med. 2015, 120, 1002–1011. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davenport, M.S.; Caoili, E.M.; Kaza, R.K.; Hussain, H.K. Matched Within-Patient Cohort Study of Transient Arterial Phase Respiratory Motion-Related Artifact in MR Imaging of the Liver: Gadoxetate Disodium versus Gadobenate Dimeglumine. Radiology 2014, 272, 123–131. [Google Scholar] [CrossRef] [PubMed]
- Well, L.; Weinrich, J.M.; Adam, G.; Bannas, P. Transient Severe Respiratory Motion Artifacts After Application of Gadoxetate Disodium: What We Currently Know. Rofo 2018, 190, 20–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
{kind=link}
| Parameter | Median | IQR | n | Valid% | |
|---|---|---|---|---|---|
| Sex (17 a) | Women | 69 | 13.2 | ||
| Men | 452 | 86.8 | |||
| Age (y) (17 a) | 66 | 59–73 | |||
| ≤65 | 249 | 47.8 | |||
| >65 | 272 | 52.2 | |||
| Race (38 a) | Caucasian | 468 | 93.6 | ||
| Other | 32 | 6.4 | |||
| Previous HCC treatment (19 a) | Yes | 150 | 28.9 | ||
| No | 369 | 71.1 | |||
| Previous HCC treatments in detail | TACE or TAE | 102 | 19.7 | ||
| Resection | 44 | 8.5 | |||
| PVE, no resection | 4 | 0.8 | |||
| Local ablation | 51 | 9.8 | |||
| Liver cirrhosis (23 a) | Yes | 418 | 81.2 | ||
| No | 97 | 18.8 | |||
| ECOG (31 a) | 0 | 375 | 74 | ||
| 1 | 123 | 24.3 | |||
| ≥2 | 9 | 1.8 | |||
| HCC diagnosis by (19 a) | Histology | 223 | 43 | ||
| Imaging criteria | 291 | 56.1 | |||
| Other | 5 | 0.9 | |||
| Cause of disease b | Alcohol abuse | 225 | 41.8 | ||
| Hepatitis B | 57 | 10.6 | |||
| Hepatitis C | 128 | 23.8 | |||
| NASH | 49 | 9.1 | |||
| NAFLD | 27 | 5 | |||
| Hemochromatosis | 15 | 2.8 | |||
| Cryptogenic | 50 | 9.3 | |||
| Other | 6 | 1.1 | |||
| Alcohol abuse only | 182 | 33.8 | |||
| Hepatitis B or C only | 149 | 27.7 | |||
| No hepatitis B or C, no alcohol abuse | 125 | 23.2 | |||
| Hepatitis B or C and alcohol abuse | 25 | 4.6 | |||
| Child-Pugh points (24 a) | 5 (A) | 330 | 64.2 | ||
| 6 (A) | 127 | 24.7 | |||
| 7 (B) | 47 | 9.1 | |||
| 8 (B) | 6 | 1.2 | |||
| 10 I | 2 | 0.4 | |||
| BCLC stage (25 a) | 0 | 6 | 1.2 | ||
| A | 93 | 18.1 | |||
| B | 144 | 28.1 | |||
| C | 269 | 52.4 | |||
| D | 1 | 0.2 | |||
| Metastases (21 a) | y | 90 | 17.4 | ||
| n | 427 | 82.6 | |||
| Specified | Lymph node | 49 | 9.5 | ||
| Bone | 10 | 1.9 | |||
| Other | 31 | 6 | |||
| Study arm c | Curative arm | 95 | 17.7 | ||
| Palliative arm | 354 | 65.8 | |||
| Screen failure | 89 | 16.5 | |||
| No. of patients by country (No. of centres) | Germany (10) | 226 | 42.0 | ||
| Switzerland (1) | 3 | 0.6 | |||
| Austria (2) | 25 | 4.7 | |||
| The Netherlands (1) | 54 | 10 | |||
| Poland (3) | 32 | 5.9 | |||
| Belgium (1) | 10 | 1.9 | |||
| Spain (1) | 28 | 5.2 | |||
| Turkey (1) | 10 | 1.9 | |||
| Great Britain (4) | 24 | 4.5 | |||
| France (5) | 70 | 13.0 | |||
| Italy (3) | 40 | 7.4 | |||
| Slovenia (1) | 16 | 3.0 |
| (a) Accuracy of Treatment Recommendation a | ||||
| CT | Gadoxetic acid-enhanced dynamic MRI | |||
| Reader 1 | Reader 2 | Reader 1 | Reader 2 | |
| Accuracy of treatment recommendation ITT (n = 538) a | 73.4% | 70.8% | 75.1% | 70.3% |
| Accuracy of treatment recommendation per protocol (n = 363) a | 76.6% | 71.6% | 79.1% | 72.2% |
| Accuracy of treatment recommendation histological verified cases only (n = 223) a | 78.5% | 74.0% | 76.2% | 75.3% |
| (b) OR by Modality and Reader Group | ||||
| CT | ||||
| Reader group 1 | Reader group 2 | |||
| OR | CI (LCI-UCI) | OR | CI (LCI-UCI) | |
| ITT | ||||
| Gadoxetic acid-enhanced dynamic MRI as compared to | 1.09 | 0.83–1.43 | 0.97 | 0.75–1.27 |
| Per Protocol | ||||
| Gadoxetic acid-enhanced dynamic MRI as compared to | 1.15 | 0.81–1.64 | 1.03 | 0.74–1.42 |
| ITT histological verified cases only | ||||
| Gadoxetic acid-enhanced dynamic MRI as compared to | 0.88 | 0.56–1.37 | 1.07 | 0.70–1.65 |
| (c) OR by Modality (Based on GEE with Independent Working Correlation Matrix) | ||||
| CT | ||||
| OR | CI (LCI-UCI) | |||
| ITT | ||||
| Gadoxetic acid-enhanced dynamic MRI as compared to | 1.01 | 0.97–1.05 | ||
| Per Protocol | ||||
| Gadoxetic acid-enhanced dynamic MRI as compared to | 1.02 | 0.98–1.07 | ||
| ITT histological verified cases only | ||||
| Gadoxetic acid-enhanced dynamic MRI as compared to | 0.99 | 0.94–1.05 | ||
| Lesion Detection CT and MRI Imaging | ||||
|---|---|---|---|---|
| CT | Gadoxetic Acid-Enhanced Dynamic MRI | |||
| R1 (n/%) | R2 (n/%) | R1 (n/%) | R2 (n/%) | |
| Patients with lesions > 1 cm with arterial enhancement/wash-out (n/%) | ||||
| Lesion number n = 1 | 194/36.1 | 181/33.6 | 202/37.6 | 173/32.2 |
| Lesion number n = 2–4 | 138/25.7 | 118/21.9 | 128/23.8 | 145/27.0 |
| Lesion number n = 5–20 | 113/21.0 | 140/26.0 | 112/20.8 | 135/25.1 |
| Lesion number n > 20 | 71/13.2 | 61/11.4 | 55/10.2 | 45/8.4 |
| Longest hypervascularized diameter lesions (cm, mean/SD) | 6.1/4.1 | 5.1/3.6 | 7.0/4.4 | 5.4/3.7 |
| Rate of lesion number 0–4 | 354/65.8 | 337/62.6 | 363/67.7 | 358/66.5 |
| Rate of lesion number > 4 | 184/34.2 | 201/37.4 | 174/32.3 | 180/33.5 |
| Image Quality and Artefacts, Frequencies | |||||
| CT | Gadoxetic Acid-Enhanced Dynamic MRI | ||||
| n | Valid % | n | Valid% | ||
| Image quality (R1/R2) | Good or average | 537/535 | 99.8/99.4 | 480/489 | 89.2/91.9 |
| poor | 1/3 | 0.2/0.6 | 58/49 | 10.8/9.1 | |
| Artefacts present a (R1/R2) | Yes | 1/1 | 0.2/0.2 | 26/52 | 4.9/9.7 |
| Correct timing contrast dynamics (R1/R2) | Yes | 520/458 | 96.7/85.1 | 496/394 | 92.2/73.2 |
| Evaluation of hypervascularity compromised (R1/R2) | Yes | 10/42 | 1.9/7.8 | 32/108 | 5.9/20.1 |
| Combined artefacts (according to per protocol) b (R1/R2) | Yes | 10/43 | 1.9/8.0 | 41/119 | 7.6/22.1 |
| Image quality and artefacts, comparison of modalities | |||||
| CT | |||||
| Reader 1 | Reader 2 | ||||
| OR | CI (LCI/UCI) | OR | CI (LCI/UCI) | ||
| Image quality good/average vs. poor | Gadoxetic acid-enhanced dynamic MRI as compared to | 0.1 | 0.1/0.1 | 0.1 | 0.1/0.1 |
| Artefacts present a, yes vs. no | Gadoxetic acid-enhanced dynamic MRI as compared to | 27.3 | 3.7/201.7 | 57.5 | 7.9/417.2 |
| Correct timing contrast dynamics, yes vs. no | Gadoxetic acid-enhanced dynamic MRI as compared to | 0.4 | 0.2/0.8 | 0.5 | 0.4/0.7 |
| Evaluation of hypervascularity compromised, yes vs. no | Gadoxetic acid-enhanced dynamic MRI as compared to | 0.3 | 0.2/0.6 | 0.3 | 0.2/0.5 |
| Combined artefacts (according to per protocol) b, yes vs. no | Gadoxetic acid-enhanced dynamic MRI as compared to | 4.4 | 2.2/8.8 | 3.3 | 2.3/4.7 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Seidensticker, M.; Steffen, I.G.; Bargellini, I.; Berg, T.; Benito, A.; Gebauer, B.; Iezzi, R.; Loewe, C.; Karçaaltincaba, M.; Pech, M.; et al. Gadoxetic Acid-Based MRI for Decision-Making in Hepatocellular Carcinoma Employing Perfusion Criteria Only—A Post Hoc Analysis from the SORAMIC Trial Diagnostic Cohort. Curr. Oncol. 2022, 29, 565-577. https://doi.org/10.3390/curroncol29020051
Seidensticker M, Steffen IG, Bargellini I, Berg T, Benito A, Gebauer B, Iezzi R, Loewe C, Karçaaltincaba M, Pech M, et al. Gadoxetic Acid-Based MRI for Decision-Making in Hepatocellular Carcinoma Employing Perfusion Criteria Only—A Post Hoc Analysis from the SORAMIC Trial Diagnostic Cohort. Current Oncology. 2022; 29(2):565-577. https://doi.org/10.3390/curroncol29020051
Chicago/Turabian StyleSeidensticker, Max, Ingo G. Steffen, Irene Bargellini, Thomas Berg, Alberto Benito, Bernhard Gebauer, Roberto Iezzi, Christian Loewe, Musturay Karçaaltincaba, Maciej Pech, and et al. 2022. "Gadoxetic Acid-Based MRI for Decision-Making in Hepatocellular Carcinoma Employing Perfusion Criteria Only—A Post Hoc Analysis from the SORAMIC Trial Diagnostic Cohort" Current Oncology 29, no. 2: 565-577. https://doi.org/10.3390/curroncol29020051
APA StyleSeidensticker, M., Steffen, I. G., Bargellini, I., Berg, T., Benito, A., Gebauer, B., Iezzi, R., Loewe, C., Karçaaltincaba, M., Pech, M., Sengel, C., van Delden, O., Vandecaveye, V., Zech, C. J., & Ricke, J. (2022). Gadoxetic Acid-Based MRI for Decision-Making in Hepatocellular Carcinoma Employing Perfusion Criteria Only—A Post Hoc Analysis from the SORAMIC Trial Diagnostic Cohort. Current Oncology, 29(2), 565-577. https://doi.org/10.3390/curroncol29020051