
The Learning Curve and Inter-Observer Variability in Contouring the Hippocampus under the Hippocampal Sparing Guidelines of Radiation Therapy Oncology Group 0933

 , , ,
, , , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
Aim of Study
2. Material and Methods
3. Results
3.1. Size and Volume of the Hippocampus
3.2. Overlapping Contours
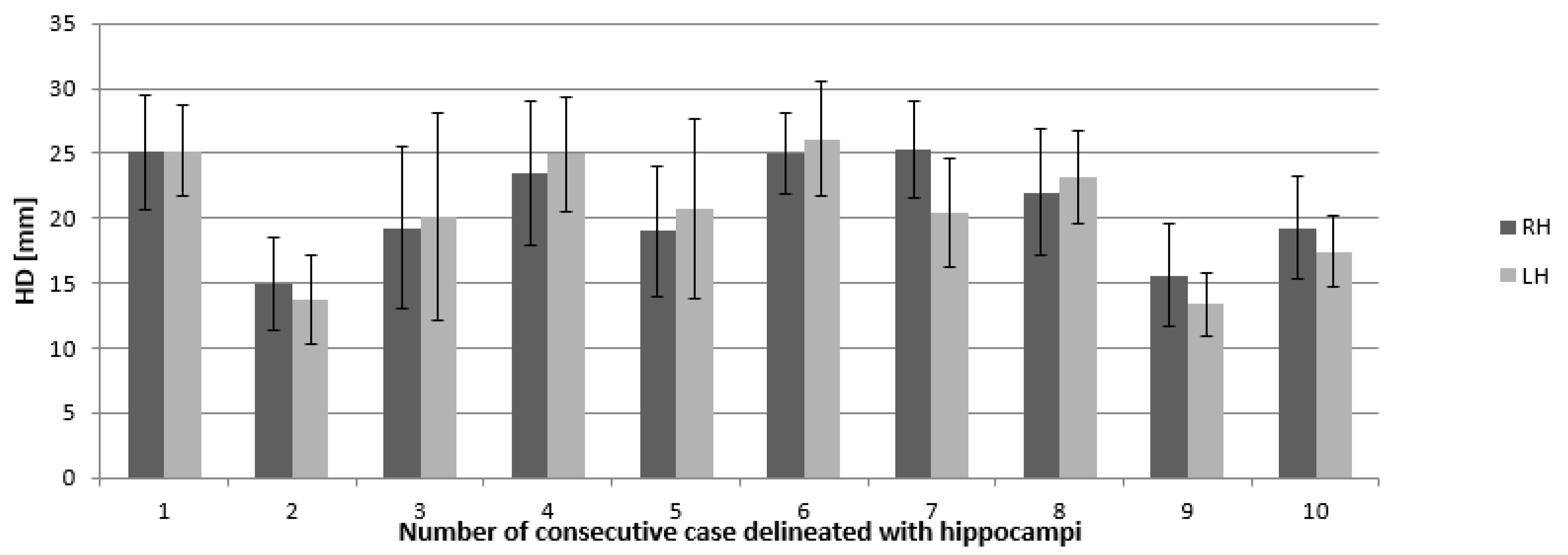
3.3. Hausdorf Distance and Dice Coefficient
3.4. Discrepancies in Axis and Location
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Aoyama, H.; Shirato, H.; Tago, M.; Nakagawa, K.; Toyoda, T.; Hatano, K.; Kenjyo, M.; Oya, N.; Hirota, S.; Shioura, H.; et al. Stereotactic radiosurgery plus whole-brain radiation therapy vs stereotactic radiosurgery alone for treatment of brain metastases: A randomized controlled trial. JAMA 2006, 295, 2483–2491. [Google Scholar] [CrossRef] [PubMed]
- Patchell, R.A.; Tibbs, P.A.; Regine, W.F.; Dempsey, R.J.; Mohiuddin, M.; Kryscio, R.J.; Markesbery, W.R.; Foon, K.A.; Young, B. Postoperative radiotherapy in the treatment of single metastases to the brain: A randomized trial. JAMA 1998, 280, 1485–1489. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Bentzen, S.M.; Renschler, M.; Mehta, M.P. Regression after whole-brain radiation therapy for brain metastases correlates with survival and improved neurocognitive function. J. Clin. Oncol. 2007, 25, 1260–1266. [Google Scholar] [CrossRef] [PubMed]
- Tallet, A.V.; Azria, D.; Barlesi, F.; Spano, J.P.; Carpentier, A.F.; Gonçalves, A.; Metellus, P. Neurocognitive function impairment after whole brain radiotherapy for brain metastases: Actual assessment. Radiat. Oncol. 2012, 7, 77. [Google Scholar] [CrossRef] [Green Version]
- Barani, I.J.; Benedict, S.H.; Lin, P.S. Neural stem cells: Implication for the conventional radiotherapy of central nervous malignancies. Int. J. Radiat. Oncol. Biol. Phys. 2007, 68, 324–333. [Google Scholar] [CrossRef]
- Konopka-Filippow, M.; Sierko, E.; Wojtukiewicz, M.Z. Hippocampal sparing in brain radiotherapy. Nowotw. J. Oncol. 2016, 66, 301–310. [Google Scholar] [CrossRef]
- Meyers, C.A.; Smith, J.A.; Bezjak, A.; Mehta, M.P.; Liebmann, J.; Illidge, T.; Kunkler, I.; Caudrelier, J.M.; Eisenberg, P.D.; Meerwaldt, J.; et al. Neurocognitive function and progression in patients with brain metastases treated with whole-brain radiation and motexafin gadolinium: Results of a randomized phase III trial. J. Clin. Oncol. 2004, 22, 157–165. [Google Scholar] [CrossRef] [Green Version]
- Gondi, V.; Tome, W.A.; Metha, M.P. Why avoid the hippocampus? A comprehensive review. Radiother. Oncol. 2010, 97, 370–376. [Google Scholar] [CrossRef] [Green Version]
- Gondi, V.; Tolakanahalli, R.; Mehta, M.P.; Tewatia, D.; Rowley, H.; Kuo, J.S.; Khuntia, D.; Tomé, W.A. Hippocampal-sparing whole-brain radiotherapy: A “how-to” technique using helical tomotherapy and linear accelerator-based intensity-modulated radiotherapy. Int. J. Radiat. Oncol. Biol. Phys. 2010, 78, 1244–1252. [Google Scholar] [CrossRef] [Green Version]
- Bartel, F.; van Herk, M.; Vrenken, H.; Vandaele, F.; Sunaert, S.; de Jaeger, K.; Dollekamp, N.J.; Carbaat, C.; Lamers, E.; Dieleman, E.M.T.; et al. Inter-observer variation of hippocampus delineation in hippocampal avoidance prophylactic cranial irradiation. Clin. Transl. Oncol. 2019, 21, 178–186. [Google Scholar] [CrossRef]
- Tofilon, P.J.; Fike, J.R. The radioresponse of the central nervous system: A dynamic process. Radiat. Res. 2000, 154, 357–370. [Google Scholar] [CrossRef]
- Cameron, H.A.; Wolley, C.S.; Mc Ewen, B.S.; Gould, E. Differentiation of newly born neurons and glia in the dentate gyrus of the adult rat. Neuroscience 1993, 56, 337–344. [Google Scholar] [CrossRef]
- Mizumatsu, S.; Monje, M.L.; Morhardt, D.R.; Rola, R.; Palmer, T.D.; Fike, J.R. Extreme sensitivity of adult neurogenesis to low doses of X-irradiation. Cancer Res. 2003, 63, 4021–4027. [Google Scholar] [PubMed]
- Kazda, T.; Jancalek, R.; Pospisil, P.; Sevela, O.; Prochazka, T.; Vrzal, M.; Burkon, P.; Slavik, M.; Hynkova, L.; Slampa, P.; et al. Why and how to spare the hippo campus during brain radiotherapy: The developing role of hippocampal avoidance in cranial radiotherapy. Radiat. Oncol. 2014, 9, 139. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gondi, V.; Pugh, S.L.; Tome, W.A.; Caine, C.; Corn, B.; Kanner, A.; Rowley, H.; Kundapur, V.; DeNittis, A.; Greenspoon, J.N.; et al. Memory preservation with conformal avoidance of the hippocampus during whole brain radiation therapy for patients with brain metastases: Primary endpoint results of RTOG 0933. Int. J. Radiat. Oncol. Biol. Phys. 2013, 87, 1186. [Google Scholar] [CrossRef]
- Nevelsky, A.; Ieumwananonthachai, N.; Kaidar-Person, O.; Bar-Deroma, R.; Nasrallah, H.; Ben-Yosef, R.; Kuten, A. Hippocampal-sparing whole brain radiotherapy using Elekta equipment. J. Appl. Clin. Med. Phys. 2013, 14, 4205. [Google Scholar] [CrossRef] [Green Version]
- Gondi, V.; Tome, W.A.; Rowley, H.A.; Mehta, M.P. Hippocampal contouring: A Contouring Atlas for RTOG 0933; The Radiation Therapy Oncology Group: Philadelphia, PA, USA, 2010. [Google Scholar]
- Holmes, C.J.; Hoge, R.; Collins, L.; Woods, R.; Toga, A.W.; Evans, A.C. MR Images courtesy of: Enhancement of MR images using registration for signal averaging. J. Comput. Assist. Tomogr. 1998, 22, 324–333. [Google Scholar] [CrossRef]
- Heung-Yeung, S.; Hebert, M.; Ikeuchi, K. On 3D shape similarity. In Proceedings of the CVPR IEEE Computer Society Conference on Computer Vision and Pattern Recognition, San Francisco, CA, USA, 18–20 June 1996. [Google Scholar]
- Chiappiniello, A.; Tarducci, R.; Muscio, C.; Bruzzone, M.G.; Bozzali, M.; Tiraboschi, P.; Nigri, A.; Ambrosi, C.; Chipi, E.; Ferraro, S.; et al. Automatic multispectral MRI segmentation of human hippocampal subfields: An evaluation of multicentric test-retest reproducibility. Brain Struct. Funct. 2021, 226, 137–150. [Google Scholar] [CrossRef]
- Cootes, T.F.; Taylor, C.J.; Cooper, D.H.; Graham, J. Active shape models-their training and applications. Comput. Vis. Image Underst. 1995, 61, 38–59. [Google Scholar] [CrossRef] [Green Version]
- Van Kesteren, Z.; Belderbos, J.; van Herk, M.; Olszewska, A.; Lamers, E.; de Ruysscher, D.; Damen, E.; van Vliet-Vroegindeweij, C. A practical technique to avoid the hippocampus in prophylactic cranial irradiation for lung cancer. Radiother. Oncol. 2012, 102, 225–227. [Google Scholar] [CrossRef]
- Truc, G.; Martin, E.; Mirjolet, C. What place for the whole brain radiotherapy with hippocampal-sparing? Cancer Radioth. 2013, 17, 419–423. [Google Scholar] [CrossRef] [PubMed]
- Van Paesschen, W.; Connelly, A.; King, M.D.; Jackson, G.D.; Duncan, J.S. The spectrum of hippocampal sclerosis: A quantitative magnetic resonance imaging study. Ann. Neurol. 1997, 41, 41–51. [Google Scholar] [CrossRef] [PubMed]
- Briellmann, R.S.B.; Kalnins, R.M.; Berkovic, S.F.; Jackson, G.D. Hippocampal pathology in refractory temporal lobe epilepsy: T2-weighted signal change reflects dentate gliosis. Neurology 2002, 58, 265–271. [Google Scholar] [CrossRef] [PubMed]
- Bender, E.T.; Metha, M.P.; Tome, W.A. On the estimation of the location of the hippocampus in the context of hippocampal avoidance whole brain radiotherapy treatment planning. Technol. Cancer Res. Treat. 2009, 8, 425–432. [Google Scholar] [CrossRef] [Green Version]
- Mehta, P.; Janssen, S.; Fahlbusch, F.B.; Schmid, S.M.; Gebauer, J.; Cremers, F.; Ziemann, C.; Tartz, M.; Rades, D. Sparing the hippocampus and the hypothalamic- pituitary region during whole brain radiotherapy: A volumetric modulated arc therapy planning study. BMC Cancer 2020, 20, 610. [Google Scholar] [CrossRef]
- Khodayari, B.; Michaud, A.L.; Stanic, S.; Wooten, O.H.; Dublin, A.; Purdy, J.A.; Chen, A.M. Evaluation of hippocampus dose for patients undergoing intensity-modulated radiotherapy for nasopharyngeal carcinoma. Br. J. Radiol. 2014, 87, 20130474. [Google Scholar] [CrossRef] [Green Version]
- Gondi, V.; Cui, Y.; Mehta, M.P.; Manfredi, D.; Xiao, Y.; Galvin, J.M.; Rowley, H.; Tome, W.A. Real-time pre-treatment review limits unacceptable deviations on a cooperative group radiotherapy technique trial: Quality assurance results of RTOG 0933. Int. J. Radiat. Oncol. Biol. Phys. 2015, 91, 564–570. [Google Scholar] [CrossRef] [Green Version]
- Pan, K.; Zhao, L.; Gu, S.; Tang, Y.; Wang, J.; Yu, W.; Zhu, L.; Feng, Q.; Su, R.; Xu, Z.; et al. Deep learning-based automatic delineation of the hippocampus by MRI: Geometric and dosimetric evaluation. Radiat. Oncol. 2021, 16, 12. [Google Scholar] [CrossRef]
- Winston, G.P.; Cardoso, M.J.; Williams, E.J.; Burdett, J.L.; Bartlett, P.A.; Espak, M.; Behr, C.; Duncan, J.S.; Ourselin, S. Automated hippocampal segmentation in patients with epilepsy: Available free online. Epilepsia 2013, 54, 2166–2173. [Google Scholar] [CrossRef] [Green Version]
- Winston, G.P.; Vos, S.B.; Burdett, J.L.; Cardoso, M.J.; Ourselin, S.; Duncan, J.S. Automated T2 relaxometry of the hippocampus for temporal lobe epilepsy. Epilepsia 2017, 58, 1645–1652. [Google Scholar] [CrossRef] [Green Version]
- Dekeyzer, S.; De Kock, I.; Nikoubashman, O.; Vanden Bossche, S.; Van Eetvelde, R.; De Groote, J.; Acou, M.; Wiesmann, M.; Deblaere, K.; Achten, E. “Unforgettable”—a pictorial essay on anatomy and pathology of the hippocampus. Insights Imaging 2017, 8, 199–212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chera, B.S.; Amdur, R.J.; Patel, P.; Mendenhall, W.M. A radiation oncologist’s guide to contouring the hippocampus. Am. J. Clin. Oncol. 2009, 32, 20–22. [Google Scholar] [CrossRef] [PubMed]
- Feng, C.H.; Cornell, M.; Moore, K.L.; Karunamuni, R.; Seibert, T.M. Automated contouring and planning pipeline for hippocampal-avoidant whole-brain radiotherapy. Radiat. Oncol. 2020, 15, 251. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Zheng, D.; Zhang, C.; Ma, R.; Bennion, N.R.; Lei, Y.; Zhu, X.; Enke, C.A.; Zhou, S. Automatic planning on hippocampal avoidance whole brain radiotherapy. Med. Dosim. 2017, 42, 63–68. [Google Scholar] [CrossRef]
- Artaechevarria, X.; Munoz-Barrutia, A.; Ortiz-de-Solorzano, C. Combination strategies in multiatlas image segmentation: Application to brain MR data. IEEE Trans. Med. Imaging 2009, 28, 1266–1277. [Google Scholar] [CrossRef]
- Porter, E.; Fuentes, P.; Siddiqui, Z.; Thompson, A.; Levitin, R.; Solis, D.; Myziuk, N.; Guerrero, T. Hippocampus segmentation on noncontrast CT using deep learning. Med. Phys. 2020, 47, 2950–2961. [Google Scholar] [CrossRef]
- Di Biase, S.; Trignani, M.; Caravatta, L.; Voicu, P.I.; Di Carlo, C.; Vinciguerra, A.; Augurio, A.; Perrotti, F.; Panara, V.; Genovesi, D. Development of a contouring guide in three different head set-ups for hippocampal sparing radiotherapy: A practical approach. Radiol. Med. 2017, 122, 683–689. [Google Scholar] [CrossRef]







Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Konopka-Filippow, M.; Sierko, E.; Hempel, D.; Maksim, R.; Samołyk-Kogaczewska, N.; Filipowski, T.; Rożkowska, E.; Jelski, S.; Kasprowicz, B.; Karbowska, E.; et al. The Learning Curve and Inter-Observer Variability in Contouring the Hippocampus under the Hippocampal Sparing Guidelines of Radiation Therapy Oncology Group 0933. Curr. Oncol. 2022, 29, 2564-2574. https://doi.org/10.3390/curroncol29040210
Konopka-Filippow M, Sierko E, Hempel D, Maksim R, Samołyk-Kogaczewska N, Filipowski T, Rożkowska E, Jelski S, Kasprowicz B, Karbowska E, et al. The Learning Curve and Inter-Observer Variability in Contouring the Hippocampus under the Hippocampal Sparing Guidelines of Radiation Therapy Oncology Group 0933. Current Oncology. 2022; 29(4):2564-2574. https://doi.org/10.3390/curroncol29040210
Chicago/Turabian StyleKonopka-Filippow, Monika, Ewa Sierko, Dominika Hempel, Rafał Maksim, Natalia Samołyk-Kogaczewska, Tomasz Filipowski, Ewa Rożkowska, Stefan Jelski, Beata Kasprowicz, Eryka Karbowska, and et al. 2022. "The Learning Curve and Inter-Observer Variability in Contouring the Hippocampus under the Hippocampal Sparing Guidelines of Radiation Therapy Oncology Group 0933" Current Oncology 29, no. 4: 2564-2574. https://doi.org/10.3390/curroncol29040210
APA StyleKonopka-Filippow, M., Sierko, E., Hempel, D., Maksim, R., Samołyk-Kogaczewska, N., Filipowski, T., Rożkowska, E., Jelski, S., Kasprowicz, B., Karbowska, E., Szymański, K., & Szczecina, K. (2022). The Learning Curve and Inter-Observer Variability in Contouring the Hippocampus under the Hippocampal Sparing Guidelines of Radiation Therapy Oncology Group 0933. Current Oncology, 29(4), 2564-2574. https://doi.org/10.3390/curroncol29040210