Open Surgery including Lymphadenectomy without Adjuvant Therapy for Uterine-Confined Intermediate- and High-Risk Endometrioid Endometrial Carcinoma


Abstract
:1. Introduction
2. Patients and Methods
3. Results
3.1. Surgical Staging
3.2. Patient Demographics
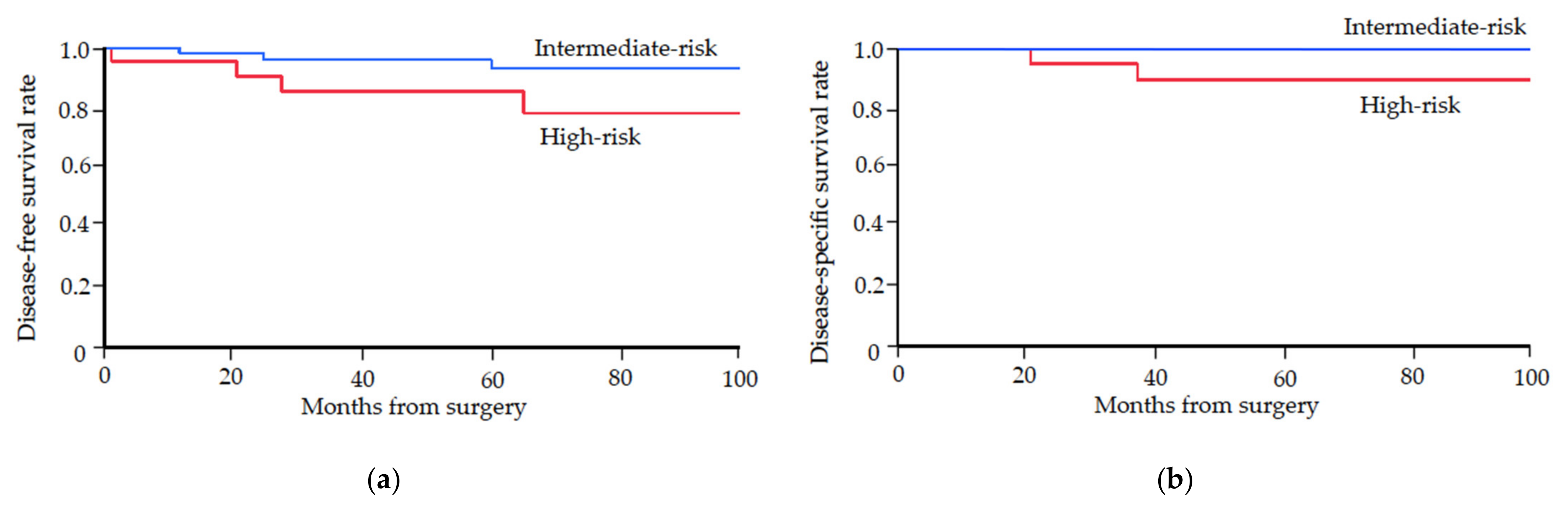
3.3. Patterns of Recurrence and Long-Term Survivals
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Walker, J.L.; Piedmonte, M.R.; Spirtos, N.M.; Eisenkop, S.M.; Schalaerth, J.B.; Mannel, R.S.; Barakat, R.; Pearl, M.L.; Sharma, S.K. Recurrence and survival after random assignment to laparoscopy versus laparotomy for comprehensive surgical staging of uterine cancer: Gynecologic Oncology Group LAP2 Study. J. Clin. Oncol. 2012, 30, 695–700. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Janda, M.V.; Gebski, L.C.; Davies, P.; Forder, A.; Brand, R.; Hogg, T.W.; Land, R.; Manolitsas, T.; Nascimento, M.; Neesham, D.; et al. Effect of total laparoscopic hysterectomy vs total abdominal hysterectomy on disease-free survival among women with stage I endometrial cancer: A randomized clinical trial. JAMA 2017, 317, 1224–1233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kitchener, H.; Swart, A.M.C.; Qian, Q.; Amos, C.; Parmar, M.K.B. Efficacy of systematic pelvic lymphadenectomy in endometrial cancer (MRC ASTEC trial): A randomised study. Lancet 2009, 373, 125–136. [Google Scholar] [PubMed] [Green Version]
- Benedetti Panici, P.; Basile, S.; Maneschi, F.; Lissoni, A.A.; Signorelli, M.; Scambia, G.; Angioli, R.; Tateo, S.; Mangili, G.; Katsaros, D.; et al. Systematic pelvic lymphadenectomy vs no lymphadenectomy in early-stage endometrial carcinoma: Randomized clinical trial. J. Natl. Cancer Inst. 2008, 100, 1707–1716. [Google Scholar] [CrossRef] [Green Version]
- Song, J.; Le, T.; Hopkins, L.; Fung-Kee-Fung, M.; Lupe, K.; Gaudet, M.; Rajiv Samant, C.E. A comparison of disease recurrence between robotic versus laparotomy approach in patients with intermediate-risk endometrial cancer. Int. J. Gynecol Cancer 2020, 30, 160–166. [Google Scholar] [CrossRef]
- Philp, I.; Tannenbaum, S.; Haber, H.; Saini, A.; St Laurent, J.; James, K.; Feltmate, C.; Russo, A.; Growdon, W. Effect of surgical approach on risk of recurrence after vaginal brachytherapy in early-stage high-intermediate risk endometrial cancer. Gynecol Oncol 2021, 160, 389–395. [Google Scholar] [CrossRef]
- Feigenberg, T.; Cormier, B.; Gotlieb, W.H.; Jegatheeswaran, K.; Helpman, L.; Kim, S.R.; Lau, S.; May, T.; Saab, D.; Plante, M.; et al. Factors associated with an increased risk of recurrence in patients diagnosed with high-grade endometrial cancer undergoing minimally invasive surgery: A study of the society of gynecologic oncology of Canada (GOC) community of practice (CoP). Gynecol. Oncol. 2021, 162, 606–612. [Google Scholar] [CrossRef]
- Kim, S.I.; Park, D.C.; Lee, S.J.; Song, M.J.; Kim, C.J.; Lee, H.N.; Yoon, J.H. Survival rates of patients who undergo minimally invasive surgery for endometrial cancer with cervical involvement. Int. J. Med. Sci. 2021, 18, 2204–2208. [Google Scholar] [CrossRef]
- Dai, Y.; Wang, Z.; Wang, J. Survival of microsatellite-stable endometrioid endometrial cancer patients after minimally invasive surgery: An analysis of the Cancer Genome Atlas data. Gynecol. Oncol. 2020, 158, 92–98. [Google Scholar] [CrossRef]
- Dai, Y.; Wang, J.; Zhao, L.; Wang, Z.; Wang, J. Tumor Molecular Features Predict Endometrial Cancer Patients’ Survival After Open or Minimally Invasive Surgeries. Front. Oncol. 2021, 11, 634857. [Google Scholar] [CrossRef]
- Todo, Y.; Kato, H.; Kaneuchi, M.; Watari, H.; Takeda, M.; Sakuragi, N. Survival effect of para-aortic lymphadenectomy in endometrial cancer (SEPAL study): A retrospective cohort analysis. Lancet 2010, 375, 1165–1172. [Google Scholar] [CrossRef]
- Chen, S.S. Operative treatment in stage I endometrial carcinoma with deep myometrial invasion and/or grade 3 tumor surgically limited to the corpus uteri. No recurrence with only primary surgery. Cancer 1989, 63, 1843–1845. [Google Scholar] [CrossRef]
- Ayhan, A.; Taskiran, C.; Celik, C.; Guney, I.; Yuce, K.; Ozyar, E.; Atahan, L.; Kucukali, T. Is there a survival benefit to adjuvant radiotherapy in high-risk surgical stage I endometrial cancer? Gynecol. Oncol. 2002, 86, 259–263. [Google Scholar] [CrossRef]
- Straughn, J.M.; Huh, W.K.; Orr, J.W.; Kelly, F.J.; Roland, P.Y.; Gold, M.A.; Powell, M.; Mutch, D.G.; Partridge, E.E.; Kilgore, L.C.; et al. Stage IC adenocarcinoma of the endometrium: Survival comparisons of surgically staged patients with and without adjuvant radiotherapy. Gynecol. Oncol. 2003, 89, 295–300. [Google Scholar] [CrossRef]
- Otsuka, I.; Kubota, T.; Aso, T. Lymphadenectomy and adjuvant therapy in endometrial carcinoma: Role of adjuvant chemotherapy. Br. J. Cancer 2002, 87, 377–380. [Google Scholar] [CrossRef] [Green Version]
- Orr, J.W., Jr.; Holimon, J.L.; Orr, P.F. Stage I corpus cancer: Is teletherapy necessary? Am. J. Obstet. Gynecol. 1997, 176, 777–789. [Google Scholar] [CrossRef]
- Fanning, J. Long-term survival of intermediate risk endometrial cancer (stage IG3, IC, II) treated with full lymphadenectomy and brachytherapy without teletherapy. Gynecol. Oncol. 2001, 82, 371–374. [Google Scholar] [CrossRef]
- Ebina, Y.; Katabuchi, H.; Mikami, M.; Nagase, S.; Yaegashi, N.; Udagawa, Y.; Kato, H.; Kubushiro, K.; Takamatsu, K.; Ino, K.; et al. Japan Society of Gynecologic Oncology guidelines 2013 for the treatment of uterine body neoplasms. Int. J. Clin. Oncol. 2016, 21, 419–434. [Google Scholar] [CrossRef]
- Morrow, C.P.; Bundy, B.N.; Kurman, R.J.; Creasman, W.T.; Heller, P.; Homesley, H.D.; Graham, J.E. Relationship between surgical-pathological risk factors and outcome in clinical stage I and II carcinoma of the endometrium: A Gynecologic Oncology Group Study. Gynecol. Oncol. 1991, 40, 55–65. [Google Scholar] [CrossRef]
- Wright, J.D.; Burke, W.M.; Tergas, A.I.; Hou, J.Y.; Huang, Y.; Hu, J.C.; Hillyer, G.C.; Ananth, C.V.; Neugut, A.I.; Hershman, D.L. Comparative Effectiveness of Minimally Invasive Hysterectomy for Endometrial Cancer. J. Clin. Oncol. 2016, 34, 1087–1096. [Google Scholar] [CrossRef] [Green Version]
- Gunderson, C.C.; Java, J.; Moore, K.N.; Walker, J.L. The impact of obesity on surgical staging, complications, and survival with uterine cancer: A Gynecologic Oncology Group LAP2 ancillary data study. Gynecol. Oncol. 2014, 133, 23–27. [Google Scholar] [CrossRef]
- Mauland, K.K.; Trovik, J.; Wik, E.; Raeder, M.B.; Njolstad, T.S.; Stefansson, I.M.; Oyan, A.M.; Kalland, K.H.; Bjorge, T.; Akslen, L.A.; et al. High BMI is significantly associated with positive progesterone receptor status and clinico-pathological markers for non-aggressive disease in endometrial cancer. Br. J. Cancer 2011, 104, 921–926. [Google Scholar] [CrossRef]
- Uccella, S.; Bonzini, M.; Malzoni, M.; Fanfani, F.; Palomba, S.; Aletti, G.; Corrado, G.; Ceccaroni, M.; Seracchioli, R.; Shakir, F.; et al. The effect of a uterine manipulator on the recurrence and mortality of endometrial cancer: A multi-centric study by the Italian Society of Gynecological Endoscopy. Am. J. Obstet. Gynecol. 2017, 216, 592.e1–11. [Google Scholar] [CrossRef]
- Padilla-Iserte, P.; Lago, V.; Tauste, C.; Diaz-Feijoo, B.; Gil-Moreno, A.; Oliver, R.; Coronado, P.; Salamanca, M.B.M.; Pantoja-Garrido, M.; Marcos-Sanmartin, J.; et al. Impact of uterine manipulator on oncological outcome in endometrial cancer surgery. Am. J. Obstet. Gynecol. 2021, 224, 65.e1–65.e11. [Google Scholar] [CrossRef]
- Chan, J.K.; Cheung, M.K.; Huh, W.K.; Osann, K.; Husain, A.; Teng, N.N.; Kapp, D.S. Therapeutic role of lymph node resection in endometrioid corpus cancer. A study of 12,333 patients. Cancer 2006, 107, 1823–1830. [Google Scholar] [CrossRef]
- Abu-Rustum, N.R.; Iasonos, A.; Zhou, Q.; Oke, E.; Soslow, R.A.; Alektiar, K.M.; Chi, D.S.; Barakat, R.R. Is there a therapeutic impact to regional lymphadenectomy in the surgical treatment of endometrial carcinoma? Am. J. Obstet. Gynecol. 2008, 198, 457.e1–457.e6. [Google Scholar] [CrossRef]
- Chan, J.K.; Kapp, D.S. Role of complete lymphadenectomy in endometrioid uterine cancer. Lancet Oncol. 2007, 8, 831–841. [Google Scholar] [CrossRef]
- Huang, C.Y.; Ho, C.M.; Chen, Y.L.; You, S.L.; Chen, C.A.; Cheng, W.F. Impact of lymphadenectomy in uterine endometrioid carcinoma. Eur. J. Surg. Oncol. 2013, 39, 350–357. [Google Scholar] [CrossRef]
- Otsuka, I.; Kadooka, M.; Matsuura, T. Long-term survival of a patient with stage IIIC2 grade 3 endometrioid endometrial carcinoma treated with surgery alone. Gynecol. Oncol. Rep. 2021, 38, 100869. [Google Scholar] [CrossRef]
- Ballester, M.; Dubernard, G.; Lecuru, F.; Heitz, D.; Mathevet, P.; Marret, H.; Querleu, D.; Golfier, F.; Leblanc, E.; Rouzier, R.; et al. Detection rate and diagnostic accuracy of sentinel-node biopsy in early stage endometrial cancer: A prospective multicentre study (SENTI-ENDO). Lancet Oncol. 2011, 12, 469–476. [Google Scholar] [CrossRef]
- Rossi, E.C.; Kowalski, L.D.; Scalici, J.; Cantrell, L.; Schuler, K.; Hanna, R.K.; Method, M.; Ade, M.; Ivanova, A.; Boggess, J.F.; et al. A comparison of sentinel lymph node biopsy to lymphadenectomy for endometrial cancer staging (FIRES trial): A multicentre, prospective, cohort study. Lancet Oncol. 2017, 18, 384–392. [Google Scholar] [CrossRef]
- Schlappe, B.A.; Weaver, A.L.; Ducie, J.A.; Eriksson, A.G.Z.; Dowdy, S.C.; Cliby, W.A.; Glaser, G.E.; Soslow, R.A.; Alektiar, K.M.; Makker, V.; et al. Multicenter study comparing oncologic outcomes between two nodal assessment methods in patients with deeply invasive endometrioid endometrial carcinoma: A sentinel lymph node algorithm versus a comprehensive pelvic and paraaortic lymphadenectomy. Gynecol. Oncol. 2018, 151, 235–242. [Google Scholar] [CrossRef] [PubMed]
- Daraï, E.; Dubernard, G.; Bats, A.S.; Heitz, D.; Mathevet, P.; Marret, H.; Querleu, D.; Golfier, F.; Leblanc, E.; Rouzier, R.; et al. Sentinel node biopsy for the management of early stage endometrial cancer: Long-term results of the SENTI-ENDO study. Gynecol. Oncol. 2015, 136, 54–59. [Google Scholar] [CrossRef] [PubMed]
- Otsuka, I.; Uno, M.; Wakabayashi, A.; Kameda, S.; Udagawa, H.; Kubota, T. Predictive factors for prolonged survival in recurrent endometrial carcinoma: Implications for follow-up protocol. Gynecol. Oncol. 2010, 119, 506–510. [Google Scholar] [CrossRef]
- Creutzberg, C.L.; van Putten, W.L.J.; Koper, P.C.M.; Lybeert, M.L.M.; Jobsen, J.J.; Warlam-Rodenhuis, C.C.; De Winter, K.A.; Lutgens, L.C.; van den Bergh, A.C.; van de Steen-Banasik, E.; et al. Surgery and postoperative radiotherapy versus surgery alone for patients with stage-1 endometrial carcinoma: Multicentre random trial. Lancet 2000, 355, 1404–1411. [Google Scholar] [CrossRef]
- Keys, H.M.; Roberts, J.A.; Brunetto, V.L.; Zaino, R.J.; Spirtos, N.M.; Bloss, J.D.; Pearlman, A.; Maiman, M.A.; Bell, J.G. A phase III trial of surgery with or without adjunctive external pelvic radiation therapy in intermediate risk endometrial adenocarcinoma: A Gynecologic Oncology Group study. Gynecol. Oncol. 2004, 92, 744–751. [Google Scholar] [CrossRef]
- Randall, M.E.; Filiaci, V.L.; Muss, H.; Spirtos, N.M.; Mannel, R.S.; Fowler, J.; Thigpen, J.T.; Benda, J.A. Randomized phase III trial of whole-abdominal irradiation versus doxorubicin and cisplatin chemotherapy in advanced endometrial carcinoma: A Gynecologic Oncology Group study. J. Clin. Oncol. 2006, 24, 36–44. [Google Scholar] [CrossRef]
- Susumu, N.; Sagae, S.; Udagawa, Y.; Niwa, K.; Kuramoto, H.; Satoh, S.; Kudo, R. Randomized phase III trial of pelvic radiotherapy versus cisplatin-based combined chemotherapy in patients with intermediate- and high-risk endometrial cancer: A Japanese Gynecologic Oncology Group study. Gynecol. Oncol. 2008, 108, 226–233. [Google Scholar] [CrossRef]
- Fujimoto, T.; Nanjyo, H.; Fukuda, J.; Nakamura, A.; Mizunuma, H.; Yaegashi, N.; Sugiyama, T.; Kurachi, H.; Satoh, A.; Tanaka, T. Endometrioid uterine cancer: Histopathological risk factors of local and distant recurrence. Gynecol. Oncol. 2009, 112, 342–347. [Google Scholar] [CrossRef]
- Bakkum-Gamez, J.N.; Mariani, A.; Dowdy, S.C.; Weaver, A.L.; McGree, M.E.; Martin, J.R.; Keeney, G.L.; Jatoi, A.; Gostout, B.S.; Podratz, K.C. Efficacy of contemporary chemotherapy in stage IIIC endometrial cancer: A histologic dichotomy. Gynecol. Oncol. 2014, 132, 578–584. [Google Scholar] [CrossRef] [Green Version]
- Boronow, R.C.; Morrow, C.P.; Creasman, W.T.; DiSaia, P.J.; Silverberg, S.G.; Miller, A.; Blessing, J.A. Surgical staging in endometrial cancer: Clinical-pathologic findings of a prospective study. Obstet. Gynecol. 1984, 63, 825–832. [Google Scholar]
- The Cancer Genome Atlas Research Network. Integrated genomic characterization of endometrial carcinoma. Nature 2013, 497, 67–73. [Google Scholar] [CrossRef] [Green Version]
- Kommoss, S.; McConechy, M.K.; Kommoss, F.; Leung, S.; Bunz, A.; Magrill, J.; Britton, H.; Kommoss, F.; Grevenkamp, F.; Karnezis, A.; et al. Final validation of the ProMisE molecular classifier for endometrial carcinoma in a large population-based case series. Ann. Oncol. 2018, 29, 1180–1188. [Google Scholar] [CrossRef]
- Cosgrove, C.M.; Tritchler, D.L.; Cohn, D.E.; Mutch, D.G.; Rush, C.M.; Lankes, H.A.; Creasman, W.T.; Miller, D.; Ramirez, N.C.; Geller, M.A.; et al. An NRG Oncology/GOG study of molecular classification for risk prediction in endometrioid endometrial cancer. Gynecol. Oncol. 2018, 148, 174–180. [Google Scholar] [CrossRef] [Green Version]
- Backes, F.J.; Haag, J.; Cosgrove, C.M.; Suarez, A.; Cohn, D.E.; Goodfellow, P.J. Mismatch repair deficiency identifies patients with high-intermediate-risk (HIR) endometrioid endometrial cancer at the highest risk of recurrence: A prognostic biomarker. Cancer 2019, 125, 398–405. [Google Scholar] [CrossRef] [Green Version]
- Forsse, D.; Barbero, M.L.; Werner, H.M.J.; Woie, K.; Nordskar, N.; Nielsen, E.B.; Engh, M.E.; Vistad, I.; Rege, A.; Sævik-Lode, M.; et al. Longitudinal effects of adjuvant chemotherapy and lymph node staging on patient-reported outcomes in endometrial cancer survivors: A prospective cohort study. Am. J. Obstet. Gynecol. 2022, 226, 90.e1–90.e20. [Google Scholar] [CrossRef]


{kind=link}
| No. of Patients | Lymph Node Metastasis | ||||
|---|---|---|---|---|---|
| (n = 292) | Total (n = 27) | Pelvic (n = 24) | Para-Aortic (n = 8) | Para-Aortic Alone (n = 3) | |
| pT classification | |||||
| pT1A | 200 | 7 (3.5%) | 7 (3.5%) | 0 | 0 |
| pT1B | 62 | 12 (19.4%) | 11 (17.7%) | 3 (4.8%) | 1 (1.6%) |
| pT2 | 17 | 2 (11.8%) | 2 (11.8%) | 0 | 0 |
| pT3 | 13 | 6 (46.2%) | 4 (30.8%) | 5 (38.5%) | 2 (15.4%) |
| Tumor Grade | |||||
| G1 | 155 | 8 (5.2%) | 7 (4.5%) | 1 (0.6%) | 1 (0.6%) |
| G2 | 94 | 10 (10.6%) | 10 (10.6%) | 4 (4.3%) | 0 |
| G3 | 43 | 9 (20.9%) | 7 (16.3%) | 3 (7.0%) | 2 (4.7%) |
| Myometrial invasion | |||||
| <1/2 | 214 | 9 (4.2%) | 9 (4.2%) | 1 (0.5%) | 0 |
| ≥1/2 | 78 | 18 (23.1%) | 15 (19.2%) | 7 (9.0%) | 3 (3.8%) |
| Cervical stromal invasion | |||||
| No | 268 | 22 (8.2%) | 20 (7.5%) | 5 (1.9%) | 2 (0.7%) |
| Yes | 24 | 5 (20.8%) | 4 (16.7%) | 3 (12.5%) | 1 (4.2%) |
| Lymphovascular space invasion | |||||
| Negative/Undetermined | 246 | 11 (4.5%) | 9 (3.7%) | 3 (1.2%) | 2 (0.8%) |
| Positive | 46 | 16 (34.8%) | 15 (32.6%) | 5 (10.9%) | 1 (2.2%) |
| Risk group † | |||||
| Low-risk | 175 | 5 (2.9%) | 5 (2.9%) | 0 | 0 |
| Intermediate-risk | 72 | 11 (15.3%) | 10 (13.9%) | 3 (4.2%) | 1 (1.4%) |
| High-risk | 45 | 11 (24.4%) | 9 (20.0%) | 5 (11.1%) | 2 (4.4%) |
| Case | Age | Risk | G, MI, Cx, LVSI | LA | Site of Rec | Time to Rec | Salvage Treatment | Status | Survival after Rec |
|---|---|---|---|---|---|---|---|---|---|
| 1 | 58 | Intermediate | G1, ≥1/2, No, No | P | Lung | 61 mo | Chemo, Surgery | NED | 37+ mo |
| 2 | 70 | Intermediate | G1, ≥1/2, No, No | P | Vaginal apex | 25 mo | RT (EBRT + VB) | NED | 81+ mo |
| 3 | 64 | Intermediate | G2, ≥1/2, No, Yes | P + PA | Pelvic LN † | 12 mo | RT (EBRT) | NED | 125+ mo |
| 4 | 67 | High | G3, ≤1/2, Yes, Yes | P | Vaginal apex | 21 mo | RT (EBRT + VB) | NED | 58+ mo |
| 5 | 57 | High | G3, ≥1/2, No, Yes | P | Vaginal sidewall | 1 mo | RT (EBRT + VB), Chemo | DOD | 20 mo |
| 6 | 71 | High | G3, ≥1/2, No, Yes | P + PA | Lung | 66 mo | RT | NED | 11+ mo |
| 7 | 70 | High | G2, ≥1/2, Yes, Yes | P | Para-aortic—supraclavicular LN | 28 mo | None | DOD | 10 mo |
| Authors (Year) | Cases (No.) | Stage, Grade; Histology | Lymphadenectomy (LA) | 5-Year Survival Rate | Median Follow-Up |
|---|---|---|---|---|---|
| Chen (1989) | 18 | IAG3, IB | Selective biopsy of pelvic and para-aortic lymph nodes | 100% (DFS) | 5–13 years |
| Ayhan (2002) | 25 | IAG3, IB; endometrioid | Pelvic and para-aortic LA | 92% (OS) | 96 months |
| Straughn (2003) | 121 | IB; serous and clear cell were excluded | Pelvic and para-aortic LA | 90% (OS) | 41 months |
| Present study | 77 | IAG3, IB, II; endometrioid | Pelvic LA in all patients and para-aortic LA in selected patients | 97% (DSS) | 75 months |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Otsuka, I.; Matsuura, T.; Mitani, T.; Otsuka, K.; Kanamoto, Y. Open Surgery including Lymphadenectomy without Adjuvant Therapy for Uterine-Confined Intermediate- and High-Risk Endometrioid Endometrial Carcinoma. Curr. Oncol. 2022, 29, 3728-3737. https://doi.org/10.3390/curroncol29050298
Otsuka I, Matsuura T, Mitani T, Otsuka K, Kanamoto Y. Open Surgery including Lymphadenectomy without Adjuvant Therapy for Uterine-Confined Intermediate- and High-Risk Endometrioid Endometrial Carcinoma. Current Oncology. 2022; 29(5):3728-3737. https://doi.org/10.3390/curroncol29050298
Chicago/Turabian StyleOtsuka, Isao, Takuto Matsuura, Takahiro Mitani, Koji Otsuka, and Yoshihisa Kanamoto. 2022. "Open Surgery including Lymphadenectomy without Adjuvant Therapy for Uterine-Confined Intermediate- and High-Risk Endometrioid Endometrial Carcinoma" Current Oncology 29, no. 5: 3728-3737. https://doi.org/10.3390/curroncol29050298
APA StyleOtsuka, I., Matsuura, T., Mitani, T., Otsuka, K., & Kanamoto, Y. (2022). Open Surgery including Lymphadenectomy without Adjuvant Therapy for Uterine-Confined Intermediate- and High-Risk Endometrioid Endometrial Carcinoma. Current Oncology, 29(5), 3728-3737. https://doi.org/10.3390/curroncol29050298