Novel Harmonization Method for Multi-Centric Radiomic Studies in Non-Small Cell Lung Cancer

 , , , , , , , , and
, , , , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.1.1. Patient Cohort
2.1.2. SBRT Details
2.2. Image Acquisition
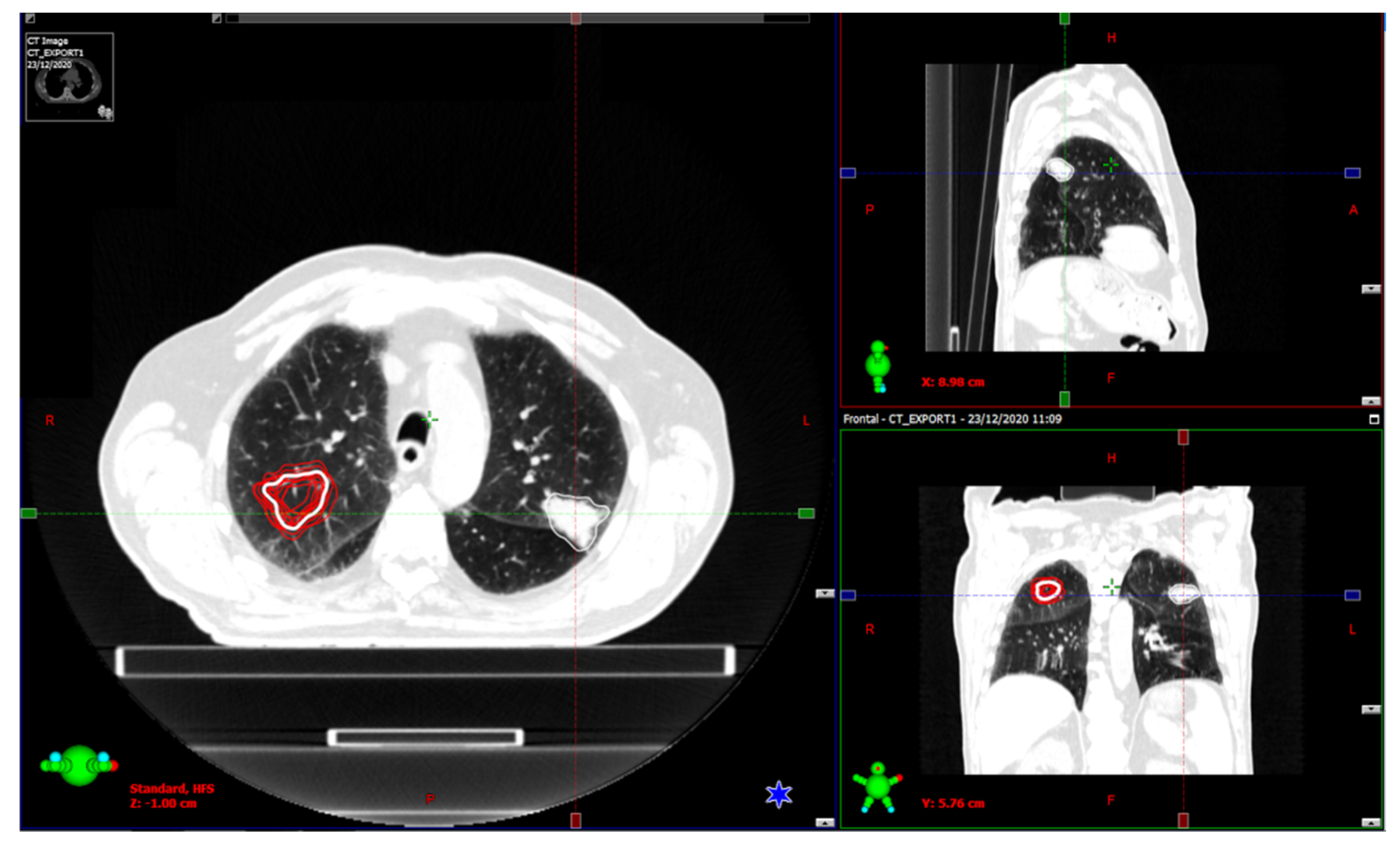
2.3. Image Segmentation
2.4. Outcome
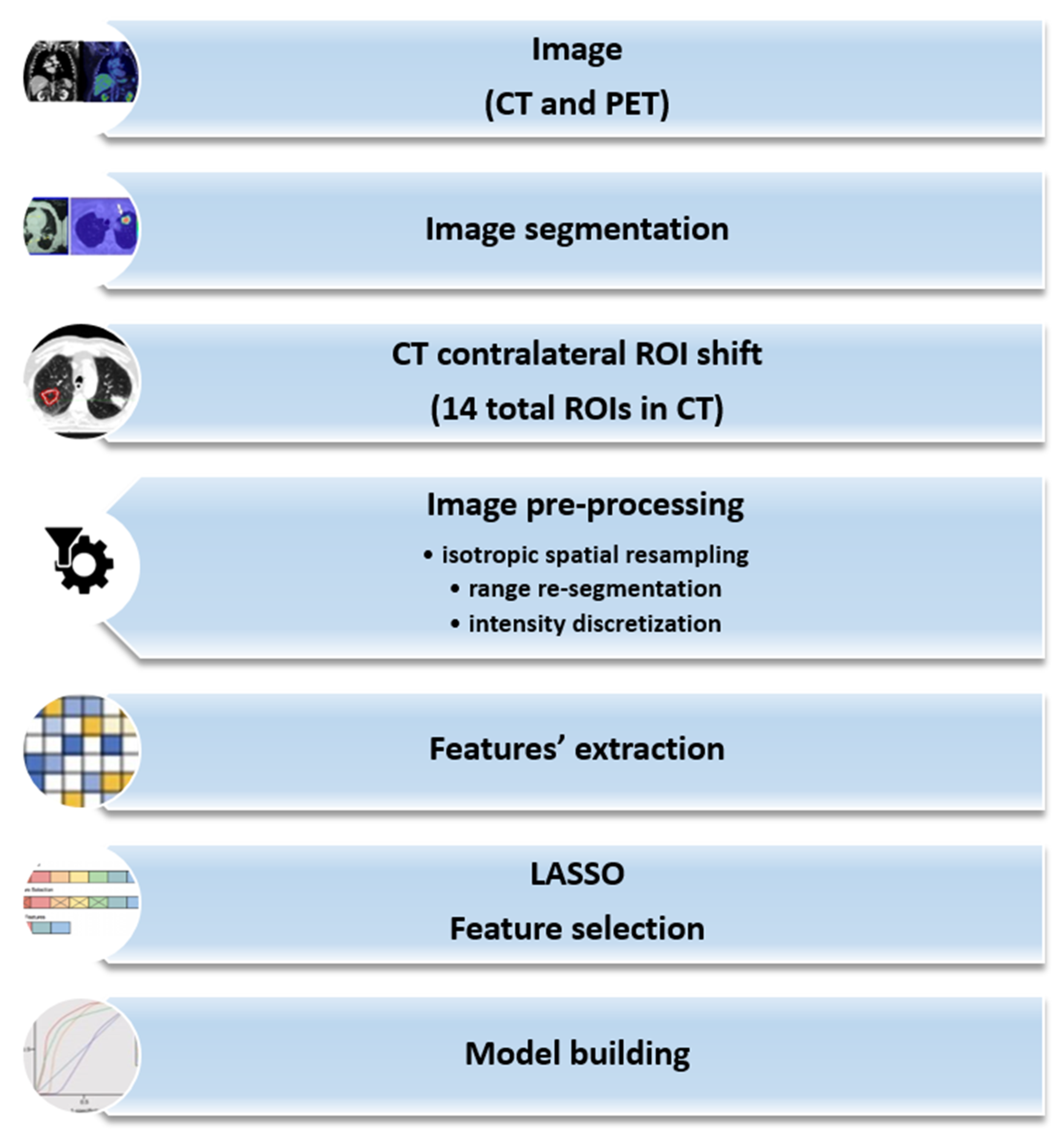
2.5. Radiomics Analysis
2.5.1. Feature Extraction
2.5.2. Harmonization Process
2.5.3. Feature Selection
2.5.4. Model Building
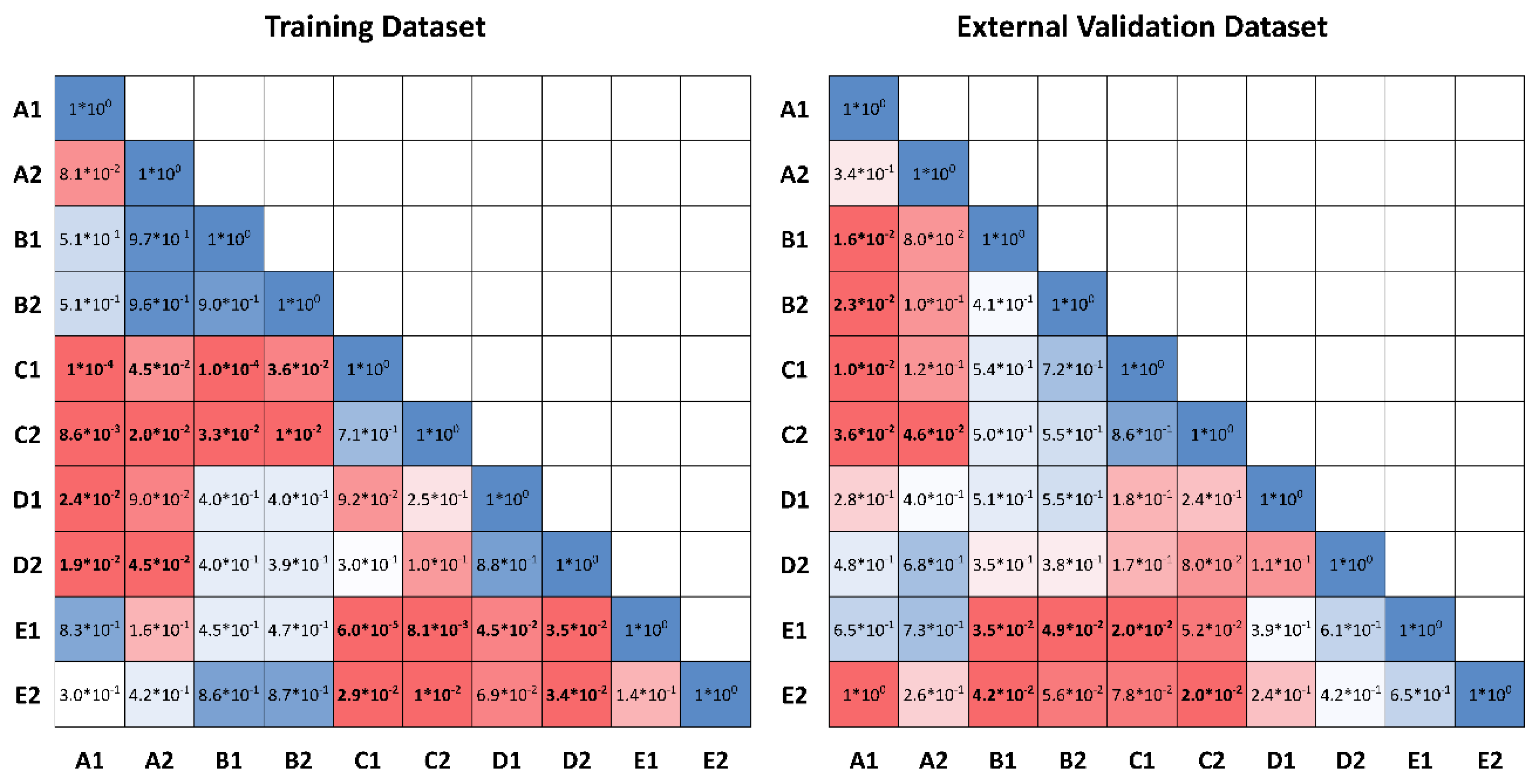
2.5.5. Statistical Analysis
3. Results
3.1. Clinical Results
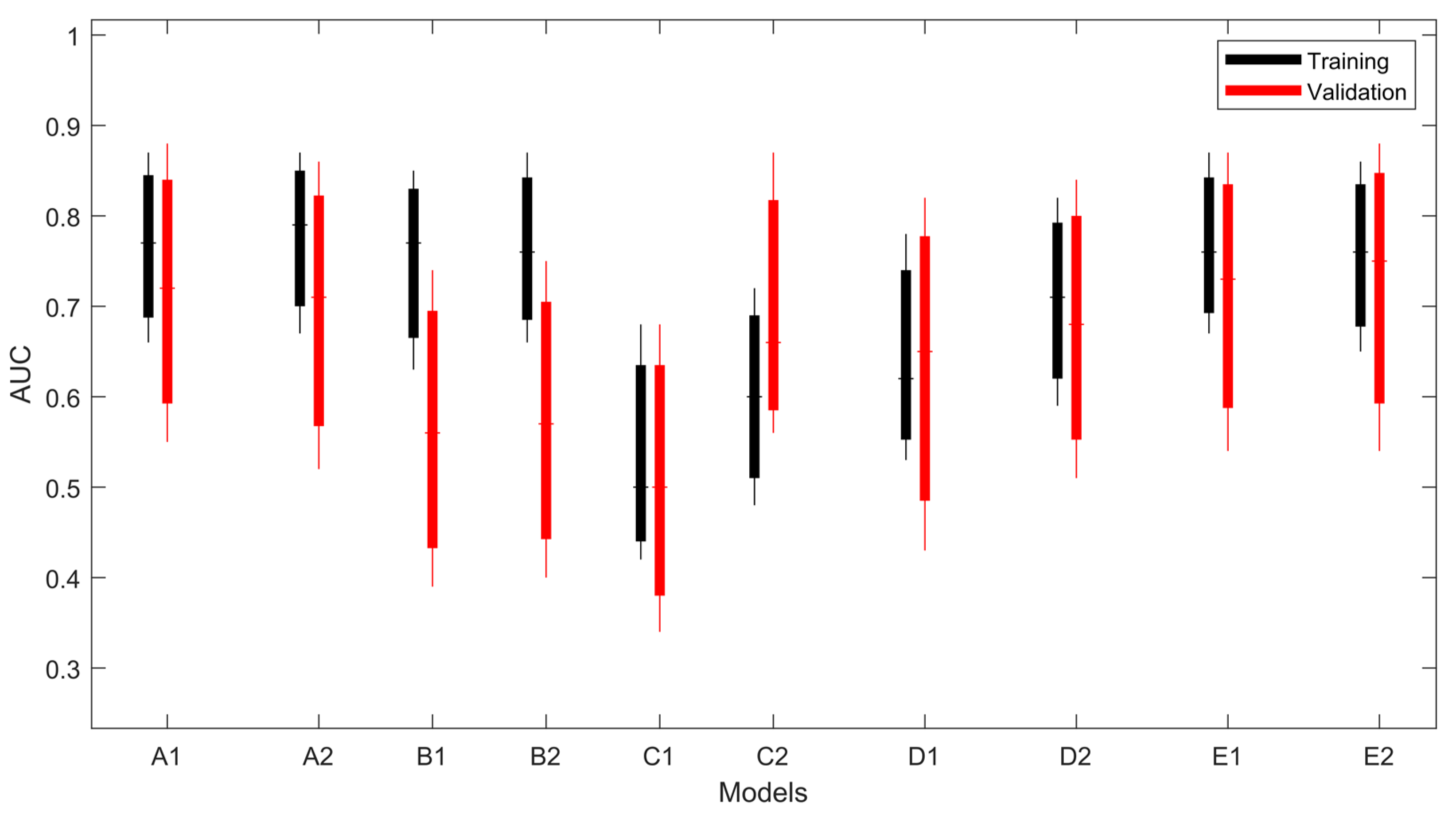
3.2. PFS Models
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Siegel, R.; Naishadham, D.; Jemal, A. Cancer statistics, 2013. CA Cancer J. Clin. 2013, 63, 11–30. [Google Scholar] [CrossRef] [Green Version]
- Edge, S.B.; Byrd, D.R.; Compton, C.C.; Fritz, A.G.; Greene, F.L.; Trotti, A. AJCC Cancer Staging Manual, 7th ed.; Springer: New York, NY, USA, 2010; pp. 253–264. [Google Scholar]
- Ginsberg, R.J.; Rubinstein, L.V. Randomized trial of lobectomy versus limited resection for T1 N0 non-small cell lung cancer. Lung Cancer Study Group. Ann. Thorac. Surg. 1995, 60, 615–622. [Google Scholar] [CrossRef]
- Bogart, J.A. Fractionated radiotherapy for high-risk patients with early-stage non-small cell lung cancer. Semin. Thorac. Cardiovasc. Surg. 2010, 22, 44–52. [Google Scholar] [CrossRef]
- Hayman, J.A.; Martel, M.K.; Ten Haken, R.K.; Normolle, D.P.; Todd, R.F., III; Littles, J.F.; Sullivan, M.A.; Possert, P.W.; Turrisi, A.T.; Lichter, A.S. Dose escalation in non-small-cell lung cancer using three-dimensional conformal radiation therapy: Update of a phase I trial. J. Clin. Oncol. 2001, 19, 127–136. [Google Scholar] [CrossRef]
- Qiao, X.; Tullgren, O.; Lax, I.; Sirzén, F.; Lewensohn, R. The role of radiotherapy in the treatment of stage I non-small cell lung cancer. Lung Cancer 2003, 41, 1–11. [Google Scholar] [CrossRef]
- Papiez, L.; Timmerman, R.; DesRosiers, C.; Randall, M. Extracranial stereotactic radioablation: Physical principles. Acta Oncol. 2003, 42, 882–894. [Google Scholar] [CrossRef] [Green Version]
- Timmerman, R.; Papiez, L.; McGarry, R.; Likes, L.; DesRosiers, C.; Frost, S.; Williams, M. Extracranial stereotactic radioablation: Results of a phase I study in medically inoperable stage I non-small cell lung cancer. Chest 2003, 124, 1946–1955. [Google Scholar] [CrossRef]
- Timmerman, R.; Paulus, R.; Galvin, J.; Michalski, J.; Straube, W.; Bradley, J.; Fakiris, A.; Bezjak, A.; Videtic, G.; Johnstone, D.; et al. Stereotactic body radiation therapy for inoperable early-stage lung cancer. JAMA 2010, 303, 1070–1076. [Google Scholar] [CrossRef] [Green Version]
- Timmerman, R.D.; Herman, J.; Cho, L.C. Emergence of stereotactic body radiation therapy and its impact on current and future clinical practice. J. Clin. Oncol. 2014, 32, 2847–2854. [Google Scholar] [CrossRef]
- Videtic, G.M.; Stephans, K.L.; Woody, N.M.; Reddy, C.A.; Zhuang, T.; Magnelli, A.; Djemil, T. 30 Gy or 34 Gy? Comparing 2 single-fraction SBRT dose schedules for stage I medically inoperable non-small cell lung cancer. Int. J. Radiat. Oncol. Biol. Phys. 2014, 90, 203–208. [Google Scholar] [CrossRef]
- Simone, C.B., 2nd; Wildt, B.; Haas, A.R.; Pope, G.; Rengan, R.; Hahn, S.M. Stereotactic body radiation therapy for lung cancer. Chest 2013, 143, 1784–1790. [Google Scholar] [CrossRef] [Green Version]
- Ackerson, B.G.; Tong, B.C.; Hong, J.C.; Gu, L.; Chino, J.; Trotter, J.W.; D’Amico, T.A.; Torok, J.A.; Lafata, K.; Chang, C.; et al. Stereotactic body radiation therapy versus sublobar resection for stage I NSCLC. Lung Cancer 2018, 125, 185–191. [Google Scholar] [CrossRef]
- Li, C.; Wang, L.; Wu, Q.; Zhao, J.; Yi, F.; Xu, J.; Wei, Y.; Zhang, W. A meta-analysis comparing stereotactic body radiotherapy vs. conventional radiotherapy in inoperable stage I non-small cell lung cancer. Medicine 2020, 99, e21715. [Google Scholar] [CrossRef]
- Fakiris, A.J.; McGarry, R.C.; Yiannoutsos, C.T.; Papiez, L.; Williams, M.; Henderson, M.A.; Timmerman, R. Stereotactic body radiation therapy for early-stage non-small-cell lung carcinoma: Four-year results of a prospective phase II study. Int. J. Radiat. Oncol. Biol. Phys. 2009, 75, 677. [Google Scholar] [CrossRef]
- Koshy, M.; Malik, R.; Mahmood, U.; Husain, Z.; Sher, D.J. Stereotactic body radiotherapy and treatment at a high volume facility is associated with improved survival in patients with inoperable stage I non-small cell lung cancer. Radiother. Oncol. 2015, 114, 148–154. [Google Scholar] [CrossRef]
- Olsen, J.R.; Robinson, C.G.; El Naqa, I.; Creach, K.M.; Drzymala, R.E.; Bloch, C.; Parikh, P.J.; Bradley, J.D. Dose Response for stereotactic body radiotherapy in early-stage nonsmall-cell lung cancer. Int. J. Radiat. Oncol. Biol. Phys. 2013, 81, e299–e303. [Google Scholar] [CrossRef]
- Onishi, H.; Shirato, H.; Nagata, Y.; Hiraoka, M.; Fujino, M.; Gomi, K.; Niibe, Y.; Karasawa, K.; Hayakawa, K.; Takai, Y.; et al. Hypofractionated Stereotactic Radiotherapy (HypoFXSRT) for stage I non-small cell lung cancer: Updated results of 257 patients in a Japanese multi-institutional study. J. Thorac. Oncol. 2011, 2, S94–S100. [Google Scholar] [CrossRef] [Green Version]
- Lee, P.; Loo, B.W., Jr.; Biswas, T.; Ding, G.X.; El Naqa, I.M.; Jackson, A.; Kong, F.M.; LaCouture, T.; Miften, M.; Solberg, T.; et al. Local Control After Stereotactic Body Radiation Therapy for Stage I Non-Small Cell Lung Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2021, 110, 160–171. [Google Scholar] [CrossRef]
- Haralick, R.M.; Shanmugam, K.; Dinstein, I. Textural Features for Image Classification. IEEE Trans. Syst. Man. Cybern. 1973, SMC-3, 610–621. [Google Scholar] [CrossRef] [Green Version]
- Castellano, G.; Bonilha, L.; Li, L.M.; Cendes, F. Texture analysis of medical images. Clin. Radiol. 2004, 59, 1061–1069. [Google Scholar] [CrossRef]
- Tourassi, G.D. Journey toward computer-aided diagnosis: Role of image texture analysis. Radiology 1999, 213, 317–320. [Google Scholar] [CrossRef] [PubMed]
- Yip, S.S.; Aerts, H.J. Applications and limitations of radiomics. Phys. Med. Biol. 2016, 61, R150–R166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lambin, P.; Rios-Velazquez, E.; Leijenaar, R.; Carvalho, S.; van Stiphout, R.G.; Granton, P.; Zegers, C.M.; Gillies, R.; Boellard, R.; Dekker, A.; et al. Radiomics: Extracting more information from medical images using advanced feature analysis. Eur. J. Cancer 2012, 48, 441–446. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lambin, P.; Leijenaar, R.T.-H.; Deist, T.M.; Peerlings, J.; de Jong, E.E.C.; van Timmeren, J.; Sanduleanu, S.; Larue, R.T.H.M.; Even, A.J.G.; Jochems, A.; et al. Radiomics: The bridge between medical imaging and personalized medicine. Nat. Rev. Clin. Oncol. 2017, 14, 749–762. [Google Scholar] [CrossRef]
- Drucker, E.; Krapfenbauer, K. Pitfalls and limitations in translation from biomarker discovery to clinical utility in predictive and personalised medicine. EPMA J. 2013, 4, 7. [Google Scholar] [CrossRef] [Green Version]
- Limkin, E.J.; Sun, R.; Dercle, L.; Zacharaki, E.I.; Robert, C.; Reuzé, S.; Schernberg, A.; Paragios, N.; Deutsch, E.; Ferté, C. Promises and challenges for the implementation of computational medical imaging (radiomics) in oncology. Ann. Oncol. 2017, 28, 1191–1206. [Google Scholar] [CrossRef]
- Chu, L.C.; Park, S.; Kawamoto, S.; Fouladi, D.F.; Shayesteh, S.; Zinreich, E.S.; Graves, J.S.; Horton, K.M.; Hruban, R.H.; Yuille, A.L.; et al. Utility of CT Radiomics Features in Differentiation of Pancreatic Ductal Adenocarcinoma from Normal Pancreatic Tissue. Am. J. Roentgenol. 2019, 213, 349–357. [Google Scholar] [CrossRef]
- Markel, D.; Caldwell, C.; Alasti, H.; Soliman, H.; Ung, Y.; Lee, J.; Sun, A. Automatic Segmentation of Lung Carcinoma Using 3D Texture Features in 18-FDG PET/CT. Int. J. Mol. Imaging. 2013, 2013, 980769. [Google Scholar] [CrossRef] [Green Version]
- Avanzo, M.; Gagliardi, V.; Stancanello, J.; Blanck, O.; Pirrone, G.; El Naqa, I.; Revelant, A.; Sartor, G. Combining computed tomography and biologically effective dose in radiomics and deep learning improves prediction of tumor response to robotic lung stereotactic body radiation therapy. Med. Phys. 2021, 48, 6257–6269. [Google Scholar] [CrossRef]
- De Ruysscher, D.; Faivre-Finn, C.; Moeller, D.; Nestle, U.; Hurkmans, C.W.; le Péchoux, C.; Belderbos, J.; Guckenberger, M.; Senan, S. Lung Group and the Radiation Oncology Group of the European Organization for Research and Treatment of Cancer (EORTC). European Organization for Research and Treatment of Cancer (EORTC) recommendations for planning and delivery of high-dose, high precision radiotherapy for lung cancer. Radiother. Oncol. 2017, 124, 1–10. [Google Scholar]
- Van Loon, J.; Siedschlag, C.; Stroom, J.; Blauwgeers, H.; van Suylen, R.J.; Knegjens, J.; Rossi, M.; van Baardwijk, A.; Boersma, L.; Klomp, H.; et al. Microscopic disease extension in three dimensions for non–small-cell lung cancer: Development of a prediction model using pathology-validated positron emission tomography and computed tomography features. Int. J. Radiat. Oncol. Biol. Phys. 2012, 82, 448–456. [Google Scholar] [CrossRef] [PubMed]
- Reuzé, S.; Orlhac, F.; Chargari, C.; Nioche, C.; Limkin, E.; Riet, F.; Escande, A.; Haie-Meder, C.; Dercle, L.; Gouy, S.; et al. Prediction of cervical cancer recurrence using textural features extracted from 18F-FDG PET images acquired with different scanners. Oncotarget 2017, 8, 43169–43179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Orlhac, F.; Soussan, M.; Chouahnia, K.; Martinod, E.; Buvat, I. 18F-FDG PET-Derived Textural Indices Reflect Tissue-Specific Uptake Pattern in Non-Small Cell Lung Cancer. PLoS ONE 2015, 10, e0145063. [Google Scholar] [CrossRef]
- Van Griethuysen, J.J.M.; Fedorov, A.; Parmar, C.; Hosny, A.; Aucoin, N.; Narayan, V.; Beets-Tan, R.G.H.; Fillon-Robin, J.C.; Pieper, S.; Aerts, H.J.W.L. Computational Radiomics System to Decode the Radiographic Phenotype. Cancer Res. 2017, 77, e104–e107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haga, A.; Takahashi, W.; Aoki, S.; Nawa, K.; Yamashita, H.; Abe, O.; Nakagawa, K. Standardization of imaging features for radiomics analysis. J. Med. Investig. 2019, 66, 35–37. [Google Scholar] [CrossRef]
- James, G.; Witten, D.; Hastie, T.; Tibshirani, R. Support vector machines. In An Introduction to Statistical Learning: Applications in R; Springer: New York, NY, USA, 2013; p. 359. [Google Scholar]
- Cortes, C.; Vapnik, V. Support-vector networks. Mach. Learn. 1995, 20, 273–297. [Google Scholar] [CrossRef]
- Polikar, R. Ensemble based systems in decision making. IEEE Circuits Syst. Mag. 2006, 6, 21–45. [Google Scholar] [CrossRef]
- Kothari, G.; Korte, J.; Lehrer, E.J.; Zaorsky, N.G.; Lazarakis, S.; Kron, T.; Hardcastle, N.; Siva, S. A systematic review and meta-analysis of the prognostic value of radiomics based models in non-small cell lung cancer treated with curative radiotherapy. Radiother. Oncol. 2021, 155, 188–203. [Google Scholar] [CrossRef]
- Mali, S.A.; Ibrahim, A.; Woodruff, H.C.; Andrearczyk, V.; Müller, H.; Primakov, S.; Salahuddin, Z.; Chatterjee, A.; Lambin, P. Making Radiomics More Reproducible across Scanner and Imaging Protocol Variations: A Review of Harmonization Methods. J. Pers. Med. 2021, 11, 842. [Google Scholar] [CrossRef]
- Da-ano, R.; Masson, I.; Lucia, F.; Doré, M.; Robin, P.; Alfieri, J.; Rousseau, C.; Mervoyer, A.; Reinhold, C.; Castelli, J.; et al. Performance comparison of modified ComBat for harmonization of radiomic features for multicenter studies. Sci. Rep. 2020, 10, 10248. [Google Scholar] [CrossRef]
- Fave, X.; Zhang, L.; Yang, J.; Mackin, D.; Balter, P.; Gomez, D.; Followill, D.; Jones, A.K.; Stingo, F.; Liao, Z.; et al. Delta-radiomics features for the prediction of patient outcomes in non-small cell lung cancer. Sci. Rep. 2017, 7, 588. [Google Scholar] [CrossRef] [PubMed]
- Alahmari, S.S.; Cherezov, D.; Goldgof, D.B.; Hall, L.O.; Gillies, R.J.; Schabath, M.B. Delta Radiomics Improves Pulmonary Nodule Malignancy Prediction in Lung Cancer Screening. IEEE Access 2018, 6, 77796–77806. [Google Scholar] [CrossRef] [PubMed]
- Nardone, V.; Reginelli, A.; Guida, C.; Belfiore, M.P.; Biondi, M.; Mormile, M.; Banci Buonamici, F.; di Giorgio, E.; Spadafora, M.; Tini, P.; et al. Delta-radiomics increases multicentre reproducibility: A phantom study. Med. Oncol. 2020, 37, 38. [Google Scholar] [CrossRef] [PubMed]
- Pinto, J.A.; Vallejos, C.S.; Raez, L.E.; Mas, L.A.; Ruiz, R.; Torres-Roman, J.S.; Morante, Z.; Araujo, J.M.; Gómez, H.L.; Aguilar, A.; et al. Gender and outcomes in non-small cell lung cancer: An old prognostic variable comes back for targeted therapy and immunotherapy? ESMO Open 2018, 3, e000344. [Google Scholar] [CrossRef] [Green Version]
- De Perrot, M.; Licker, M.; Bouchardy, C.; Usel, M.; Robert, J.; Spiliopoulos, A. Sex differences in presentation, management, and prognosis of patients with non-small cell lung carcinoma. J. Thorac. Cardiovasc. Surg. 2000, 119, 21–26. [Google Scholar] [CrossRef] [Green Version]
- Hsu, L.H.; Chu, N.M.; Liu, C.C.; Tsai, S.Y.; You, D.L.; Ko, J.S.; Lu, M.C.; Feng, A.C. Sex-associated differences in non-small cell lung cancer in the new era: Is gender an independent prognostic factor? Lung Cancer 2009, 66, 262–267. [Google Scholar] [CrossRef]
- Louie, A.V.; Haasbeek, C.J.; Mokhles, S.; Rodrigues, G.B.; Stephans, K.L.; Lagerwaard, F.J.; Palma, D.A.; Videtic, G.M.; Warner, A.; Takkenberg, J.J.; et al. Predicting Overall Survival After Stereotactic Ablative Radiation Therapy in Early-Stage Lung Cancer: Development and External Validation of the Amsterdam Prognostic Model. Int. J. Radiat. Oncol. Biol. Phys. 2015, 93, 82–90. [Google Scholar] [CrossRef]
- Ye, L.; Shi, S.; Zeng, Z.; Huang, Y.; Hu, Y.; He, J. Nomograms for predicting disease progression in patients of Stage I non-small cell lung cancer treated with stereotactic body radiotherapy. Jpn. J. Clin. Oncol. 2018, 48, 160–166. [Google Scholar] [CrossRef]
- Kang, J.; Ning, M.S.; Feng, H.; Li, H.; Bahig, H.; Brooks, E.D.; Welsh, J.W.; Ye, R.; Miao, H.; Chang, J.Y. Predicting 5-Year Progression and Survival Outcomes for Early Stage Non-small Cell Lung Cancer Treated with Stereotactic Ablative Radiation Therapy: Development and Validation of Robust Prognostic Nomograms. Int. J. Radiat. Oncol. Biol. Phys. 2020, 106, 90–99. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| CT | |||||||
|---|---|---|---|---|---|---|---|
| Center | kV | mAs (Min–Max) | Slice Thickness (mm) | Manufacturer (s) | Convolution Kernel | Recon Diameter | |
| TRAIN | BS | 120 | 191–401 | 3.0 | PHILIPS | B | 500 |
| RE | 120 | 83–355 | 3.0 | GE | STD + | 500 | |
| PD | 120 | 70–363 | 2.5 | GE | BODY FILTER | 500 | |
| EXT VAL | AV | 120 | 108–138 | 2.5 | PHILIPS | B | 500 |
| NE | 120 | 40–73 | 3.0 | SIEMENS | B30f | 500 | |
| PI | 120 | 27–236 | 2.0 | SIEMENS | B30f–B31s | 500 | |
| PG | 120 | 80–200 | 2.5–3 | GE | STD + | 500 | |
| PET | |||||||
| Center | Slice thickness (mm) | Manufacturer (s) | Recon diameter | Recon method | |||
| TRAIN | BS | 3.27 | GE | 700–815 | 3D IR/VPFXS | ||
| RE | 3.27 | GE | 700–700 | 3D IR/VPFXS | |||
| PD | 2–4 | PHILIPS|SIEMENS | 576–815 | 3D-RAMLA/BLOB-OS-TF(PHILIPS)|PSF 3i21s/(SIEMENS) | |||
| EXT VAL | AV | 4 | PHILIPS|GE | 500–700 | BLOB-OS-TF/VPFXS | ||
| NE | 2–5 | SIEMENS | 576–700 | PSF+TOF 3i21s | |||
| PI | 3.27 | GE|PHILIPS | 576–700 | 3D IR (GE)|BLOB-OS-TF(PHILIPS) | |||
| PG | 3.27 | GE|SIEMENS | 600–700 | OSEM|OSEM 2i8s | |||
| Characteristics | Training Cohort (N = 76) | External Validation Co#Hort (N = 41) | p |
|---|---|---|---|
| Gender | |||
| Male | 61 | 24 | 0.04 |
| Female | 15 | 17 | |
| Age (years) | 78 [51–87] | 79 [57–88] | 0.72 |
| Smoking Status | |||
| Yes | 50 | 27 | 0.22 |
| No | 26 | 14 | |
| Performance Status | |||
| 0 | 37 | 18 | 0.75 |
| 1 | 35 | 15 | |
| 2 | 4 | 7 | |
| BMI | 25.2 [16.4–37.1] | 24.8 [18.3–44.7] | 0.17 |
| Diabetes mellitus | |||
| Yes | 16 | 12 | 0.58 |
| No | 60 | 29 | |
| BPCO | |||
| Yes | 43 | 17 | 0.54 |
| No | 19 | 24 | |
| Charlson Comorbidity Index (CCI) | |||
| Median | 6.5 | 6 | 0.55 |
| Range | [3–13] | [4–10] | |
| T diameter | |||
| Median | 2.35 | 2.3 | 0.58 |
| Range | [0.6–5.5] | [0.72–27] | |
| Lesion type | |||
| Subsolid | 5 | 4 | 0.42 |
| Solid | 71 | 37 | |
| Lung Side | |||
| Lung right | 42 | 22 | 0.006 |
| Lung left | 34 | 19 | |
| Lobe Site | |||
| Upper Lobe | 44 | 23 | 0.89 |
| Lower Lobe | 30 | 15 | |
| Middle Lobe | 2 | 1 | |
| Lesion Site | |||
| Peripheral | 55 | 34 | 0.92 |
| Central | 21 | 7 | |
| BED10 | |||
| Median | 115.5 | 100 | 0.64 |
| Range | [100–180] | [100–132] | |
| Harmo CT + Original PET Features (A) | |||||
|---|---|---|---|---|---|
| Linear SVM (A1) | |||||
| AUC * | Accuracy | Precision ** | Recall ** | p *** | |
| Training dataset | 0.77 [0.66–0.87] | 0.72 ± 0.02 | 0.67 | 0.83 | 1.0 × 10–4 |
| External validation dataset | 0.75 [0.55–0.88] | 0.66 ± 0.01 | 0.68 | 0.65 | 0.01 |
| Subspace Discriminant (A2) | |||||
| AUC * | Accuracy | Precision ** | Recall ** | p *** | |
| Training dataset | 0.79 [0.67–0.87] | 0.71 ± 0.01 | 0.69 | 0.83 | 0.02 |
| External validation dataset | 0.71 [0.52–0.86] | 0.63 ± 0.02 | 0.68 | 0.65 | 0.046 |
| Harmo CT features (B) | |||||
| Linear SVM (B1) | |||||
| AUC | Accuracy | Precision ** | Recall ** | p *** | |
| Training dataset | 0.77 [0.63–0.85] | 0.67 ± 0.02 | 0.74 | 0.58 | 1.0 × 10−4 |
| External validation dataset | 0.56 [0.39–0.74] | 0.58 ± 0.01 | 0.67 | 0.52 | 0.5 |
| Subspace Discriminant (B2) | |||||
| AUC | Accuracy | Precision ** | Recall ** | p *** | |
| Training dataset | 0.76 [0.66–0.87] | 0.71 ± 0.02 | 0.73 | 0.6 | 0.01 |
| External validation dataset | 0.57 [0.4–0.75] | 0.58 ± 0.01 | 0.67 | 0.52 | 0.50 |
| Original CT features (C) | |||||
| Linear SVM (C1) | |||||
| AUC | Accuracy | Precision ** | Recall ** | ||
| Training dataset | 0.56 [0.42–0.68] | 0.52 ± 0.03 | 0.49 | 0.45 | |
| External validation dataset | 0.50 [0.34–0.68] | 0.43 ± 0.02 | 0.54 | 0.65 | |
| Subspace Discriminant (C2) | |||||
| AUC | Accuracy | Precision ** | Recall ** | ||
| Training dataset | 0.63 [0.48–0.72] | 0.56 ± 0.03 | 0.58 | 0.56 | |
| External validation dataset | 0.51 [0.39–0.74] | 0.54 ± 0.01 | 0.58 | 0.65 | |
| PET features only (D) | |||||
| Linear SVM (D1) | |||||
| AUC | Accuracy | Precision ** | Recall ** | p *** | |
| Training dataset | 0.68 [0.53-0.78] | 0.64 ± 0.03 | 0.64 | 0.80 | 0.09 |
| External validation dataset | 0.65 [0.43-0.82] | 0.64 ± 0.01 | 0.67 | 0.78 | 0.18 |
| Subspace Discriminant (D2) | |||||
| AUC | Accuracy | Precision ** | Recall ** | p *** | |
| Training dataset | 0.71 [0.59–0.82] | 0.69 ± 0.01 | 0.67 | 0.8 | 0.10 |
| External validation dataset | 0.68 [0.51–0.84] | 0.60 ± 0.01 | 0.67 | 0.61 | 0.08 |
| Harmo CT + Original PET + Clinical features (E) | |||||
| Linear SVM (E1) | |||||
| AUC * | Accuracy | Precision ** | Recall ** | p *** | |
| Training dataset | 0.79 [0.67–0.87] | 0.73 ± 0.02 | 0.72 | 0.83 | 6.0 × 10−5 |
| External validation dataset | 0.73 [0.54–0.87] | 0.73 ± 0.01 | 0.77 | 0.74 | 0.02 |
| Subspace Discriminant (E2) | |||||
| AUC * | Accuracy | Precision ** | Recall ** | p *** | |
| Training dataset | 0.76 [0.65–0.86] | 0.74 ± 0.01 | 0.72 | 0.83 | 0.01 |
| External validation dataset | 0.75 [0.54–0.88] | 0.68 ± 0.02 | 0.73 | 0.70 | 0.02 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bertolini, M.; Trojani, V.; Botti, A.; Cucurachi, N.; Galaverni, M.; Cozzi, S.; Borghetti, P.; La Mattina, S.; Pastorello, E.; Avanzo, M.; et al. Novel Harmonization Method for Multi-Centric Radiomic Studies in Non-Small Cell Lung Cancer. Curr. Oncol. 2022, 29, 5179-5194. https://doi.org/10.3390/curroncol29080410
Bertolini M, Trojani V, Botti A, Cucurachi N, Galaverni M, Cozzi S, Borghetti P, La Mattina S, Pastorello E, Avanzo M, et al. Novel Harmonization Method for Multi-Centric Radiomic Studies in Non-Small Cell Lung Cancer. Current Oncology. 2022; 29(8):5179-5194. https://doi.org/10.3390/curroncol29080410
Chicago/Turabian StyleBertolini, Marco, Valeria Trojani, Andrea Botti, Noemi Cucurachi, Marco Galaverni, Salvatore Cozzi, Paolo Borghetti, Salvatore La Mattina, Edoardo Pastorello, Michele Avanzo, and et al. 2022. "Novel Harmonization Method for Multi-Centric Radiomic Studies in Non-Small Cell Lung Cancer" Current Oncology 29, no. 8: 5179-5194. https://doi.org/10.3390/curroncol29080410
APA StyleBertolini, M., Trojani, V., Botti, A., Cucurachi, N., Galaverni, M., Cozzi, S., Borghetti, P., La Mattina, S., Pastorello, E., Avanzo, M., Revelant, A., Sepulcri, M., Paronetto, C., Ursino, S., Malfatti, G., Giaj-Levra, N., Falcinelli, L., Iotti, C., Iori, M., & Ciammella, P. (2022). Novel Harmonization Method for Multi-Centric Radiomic Studies in Non-Small Cell Lung Cancer. Current Oncology, 29(8), 5179-5194. https://doi.org/10.3390/curroncol29080410