Personalized Prehabilitation Improves Tolerance to Chemotherapy in Patients with Oesophageal Cancer


 ,
,
Abstract
:1. Introduction
2. Materials and Methods
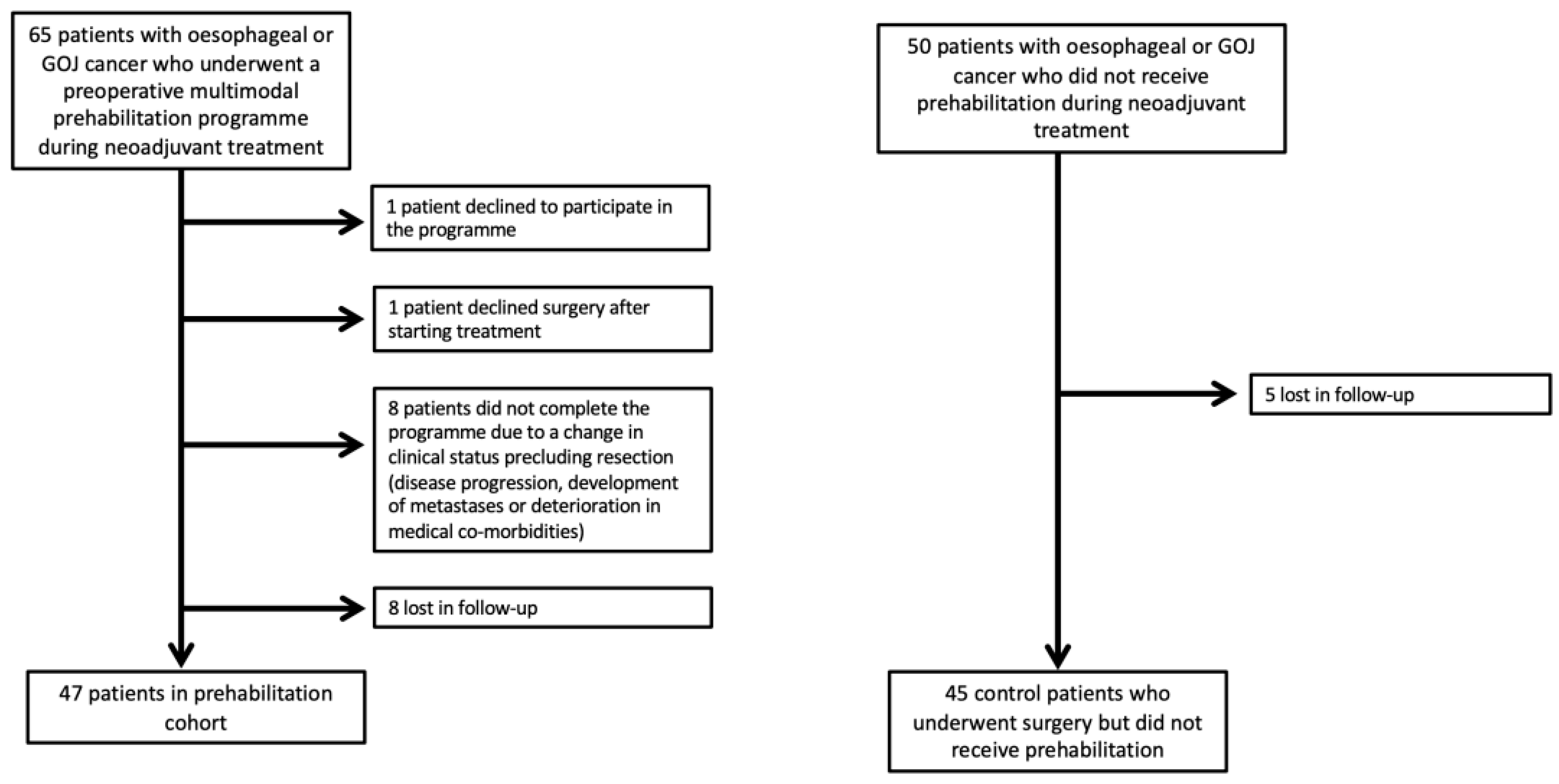
2.1. Study Participants
Details of the Prehabilitation Programme at Centre A
2.2. Primary and Secondary Endpoints
2.3. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Chemotherapy Completion and Multivariate Analysis
4. Discussion
Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cunningham, D.; Allum, W.H.; Stenning, S.P.; Thompson, J.N.; Van de Velde, C.J.; Nicolson, M.; Scarffe, J.H.; Lofts, F.J.; Falk, S.J.; Iveson, T.J.; et al. Perioperative chemotherapy versus surgery alone for resectable gastroesophageal cancer. N. Engl. J. Med. 2006, 355, 11–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Allum, W.H.; Stenning, S.P.; Bancewicz, J.; Clark, P.I.; Langley, R.E. Long-term results of a randomized trial of surgery with or without preoperative chemotherapy in esophageal cancer. J. Clin. Oncol. 2009, 27, 5062–5067. [Google Scholar] [CrossRef] [PubMed]
- Varagunam, M.; Hardwick, R.; Riley, S.; Chadwick, G.; Cromwell, D.A.; Groene, O. Changes in volume, clinical practice and outcome after reorganisation of oesophago-gastric cancer care in England: A longitudinal observational study. Eur. J. Surg. Oncol. 2018, 44, 524–531. [Google Scholar] [CrossRef]
- Sinclair, R.C.F.; Phillips, A.W.; Navidi, M.; Griffin, S.M.; Snowden, C.P. Pre-operative variables including fitness associated with complications after oesophagectomy. Anaesthesia 2017, 72, 1501–1507. [Google Scholar] [CrossRef] [Green Version]
- Moran, J.; Wilson, F.; Guinan, E.; McCormick, P.; Hussey, J.; Moriarty, J. Role of cardiopulmonary exercise testing as a risk-assessment method in patients undergoing intra-abdominal surgery: A systematic review. Br. J. Anaesth. 2016, 116, 177–191. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Doorakkers, E.; Konings, P.; Mattsson, F.; Lagergren, J.; Brusselaers, N. Early complications following oesophagectomy for cancer in relation to long-term healthcare utilisation: A prospective population-based cohort study. PLoS ONE 2015, 10, e0121080. [Google Scholar] [CrossRef] [PubMed]
- Rutegård, M.; Lagergren, P.; Rouvelas, I.; Mason, R.; Lagergren, J. Surgical complications and long-term survival after esophagectomy for cancer in a nationwide Swedish cohort study. Eur. J. Surg. Oncol. 2012, 38, 555–561. [Google Scholar] [CrossRef]
- Allum, W.H.; Blazeby, J.M.; Griffin, S.M.; Cunningham, D.; Jankowski, J.A.; Wong, R. Association of Upper Gastrointestinal Surgeons of Great Britain and Ireland, the British Society of Gastroenterology and the British Association of Surgical Oncology. Guidelines for the management of oesophageal and gastric cancer. Gut 2011, 60, 1449–1472. [Google Scholar] [CrossRef] [Green Version]
- Paul, S.; Altorki, N. Outcomes in the management of esophageal cancer. J. Surg. Oncol. 2014, 110, 599–610. [Google Scholar] [CrossRef]
- Backemar, L.; Lagergren, P.; Johar, A.; Lagergren, J. Impact of co-morbidity on mortality after oesophageal cancer surgery. Br. J. Surg. 2015, 102, 1097–1105. [Google Scholar] [CrossRef]
- West, M.A.; Loughney, L.; Barben, C.P.; Sripadam, R.; Kemp, G.J.; Grocott, M.P.; Jack, S. The effects of neoadjuvant chemoradiotherapy on physical fitness and morbidity in rectal cancer surgery patients. Eur. J. Surg. Oncol. 2014, 40, 1421–1428. [Google Scholar] [CrossRef] [PubMed]
- Nurgali, K.; Jagoe, R.T.; Abalo, R. Editorial: Adverse Effects of Cancer Chemotherapy: Anything New to Improve Tolerance and Reduce Sequelae? Front. Pharmacol. 2018, 9, 245. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahles, T.A. Brain vulnerability to chemotherapy toxicities. Psychooncology 2012, 21, 1141–1148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jack, S.; West, M.A.; Raw, D.; Marwood, S.; Ambler, G.; Cope, T.M.; Shrotri, M.; Sturgess, R.P.; Calverley, P.M.; Ottensmeier, C.H.; et al. The effect of neoadjuvant chemotherapy on physical fitness and survival in patients undergoing oesophagogastric cancer surgery. Eur. J. Surg. Oncol. 2014, 40, 1313–1320. [Google Scholar] [CrossRef] [PubMed]
- Wynter-Blyth, V.; Moorthy, K. Prehabilitation: Preparing patients for surgery. BMJ 2017, 358, j3702. [Google Scholar] [CrossRef] [PubMed]
- Carli, F.; Silver, J.K.; Feldman, L.S.; McKee, A.; Gilman, S.; Gillis, C.; Scheede-Bergdahl, C.; Gamsa, A.; Stout, N.; Hirsch, B. Surgical Prehabilitation in Patients with Cancer: State-of-the-Science and Recommendations for Future Research from a Panel of Subject Matter Experts. Phys. Med. Rehabil. Clin. N. Am. 2017, 28, 49–64. [Google Scholar] [CrossRef]
- Halliday, L.J.; Doganay, E.; Wynter-Blyth, V.A.; Hanna, G.B.; Moorthy, K. The Impact of Prehabilitation on Post-operative Outcomes in Oesophageal Cancer Surgery: A Propensity Score Matched Comparison. J. Gastrointest. Surg. 2021, 25, 2733–2741. [Google Scholar] [CrossRef]
- Allen, S.K.; Brown, V.; White, D.; King, D.; Hunt, J.; Wainwright, J.; Emery, A.; Hodge, E.; Kehinde, A.; Prabhu, P.; et al. Multimodal Prehabilitation During Neoadjuvant Therapy Prior to Esophagogastric Cancer Resection: Effect on Cardiopulmonary Exercise Test Performance, Muscle Mass and Quality of Life—A Pilot Randomized Clinical Trial. Ann. Surg. Oncol. 2022, 29, 1839–1850. [Google Scholar] [CrossRef]
- Vermillion, S.A.; James, A.; Dorrell, R.D.; Brubaker, P.; Mihalko, S.L.; Hill, A.R.; Clark, C.J. Preoperative exercise therapy for gastrointestinal cancer patients: A systematic review. Syst. Rev. 2018, 7, 103. [Google Scholar] [CrossRef]
- Minnella, E.M.; Carli, F. Prehabilitation and functional recovery for colorectal cancer patients. Eur. J. Surg. Oncol. 2018, 44, 919–926. [Google Scholar] [CrossRef]
- Karnofsky, D.A.; Abelmann, W.H.; Craver, L.F.; Burchenal, J.H. The Use of the Nitrogen Mustards in the Palliative Treatment of Carcinoma–with Particular Reference to Bronchogenic Carcinoma. Cancer 1948, 1, 634–656. [Google Scholar] [CrossRef]
- Daabiss, M. American Society of Anaesthesiologists physical status classification. Indian J. Anaesth. 2011, 55, 111–115. [Google Scholar] [CrossRef] [PubMed]
- Eyck, B.M.; van Lanschot, J.J.B.; Hulshof, M.C.C.M.; van der Wilk, B.J.; Shapiro, J.; van Hagen, P.; van Berge Henegouwen, M.I.; Wijnhoven, B.P.L.; van Laarhoven, H.W.M.; Nieuwenhuijzen, G.A.P.; et al. Ten-Year Outcome of Neoadjuvant Chemoradiotherapy Plus Surgery for Esophageal Cancer: The Randomized Controlled CROSS Trial. J. Clin. Oncol. 2021, 39, 1995–2004. [Google Scholar] [CrossRef] [PubMed]
- West, M.A.; Astin, R.; Moyses, H.E.; Cave, J.; White, D.; Levett, D.Z.H.; Bates, A.; Brown, G.; Grocott, M.P.W.; Jack, S. Exercise prehabilitation may lead to augmented tumor regression following neoadjuvant chemoradiotherapy in locally advanced rectal cancer. Acta Oncol. 2019, 58, 588–595. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Florez Bedoya, C.A.; Cardoso, A.C.F.; Parker, N.; Ngo-Huang, A.; Petzel, M.Q.; Kim, M.P.; Fogelman, D.; Romero, S.G.; Wang, H.; Park, M.; et al. Exercise during preoperative therapy increases tumor vascularity in pancreatic tumor patients. Sci. Rep. 2019, 9, 13966. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Demographics | Prehabilitation Group, n = 47 | Non-Prehabilitation Group (Control), n = 45 | p-Value |
|---|---|---|---|
| Female, n (%) | 9 (19%) | 7 (16%) | 0.649 |
| Age, years | 67.6 ± 10.2 | 65.8 ± 10.2 | 0.379 |
| BMI, kg/m2 | 26.5 ± 2.0 | 27.0 ± 5.4 | 0.82 |
| ASA Class, n (%) | 0.898 | ||
| I-II | 39 (83%) | 38 (84.5%) | |
| III-IV | 8 (17%) | 7 (15.5%) | |
| Karnofsky Score | 93.9 ± 10.0 | 99.3 ± 3.3 | 0.002 |
| Cardiac Disease, n (%) | 23 (49%) | 17 (37%) | 0.28 |
| Respiratory Disease, n (%) | 10 (21%) | 6 (13%) | 0.314 |
| Chemotherapy regime, n (%) | 0.834 | ||
| EOX | 18 (38%) | 20 (45%) | |
| ECX | 13 (28%) | 11 (24%) | |
| Other | 16 (34%) | 14 (31%) |
| Adverse Event | Prehabilitation (n = 3) | Control (n = 10) |
|---|---|---|
| Nausea and vomiting | 2 | 4 |
| Renal failure | 0 | 2 |
| Neurological | 1 | 3 |
| Cardiovascular | 0 | 1 |
| Variables | Univariate Analysis | Multiple Logistic Regression Analysis | ||
|---|---|---|---|---|
| p-Value | Odds Ratio (OR) | 95% C.I. | p-Value | |
| Age | 0.02 | 0.11 | (0.0123, 1.0278) | 0.101 |
| Histologic Type | 0.368 | 1.03 | (0.6725, 1.571) | 0.449 |
| ASA score | 0.036 | 1.03 | (0.745, 1.428) | 0.203 |
| Radiotherapy | 0.756 | 0.43 | (0.1310, 1.397) | 0.764 |
| Karnofsky score | 0.017 | 0.98 | (0.863, 1.110) | 0.501 |
| Prehabilitation | 0.003 | 10.93 | (1.044, 114.460) | 0.046 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Christodoulidis, G.; Halliday, L.J.; Samara, A.; Bhuva, N.; Park, W.-H.E.; Moorthy, K. Personalized Prehabilitation Improves Tolerance to Chemotherapy in Patients with Oesophageal Cancer. Curr. Oncol. 2023, 30, 1538-1545. https://doi.org/10.3390/curroncol30020118
Christodoulidis G, Halliday LJ, Samara A, Bhuva N, Park W-HE, Moorthy K. Personalized Prehabilitation Improves Tolerance to Chemotherapy in Patients with Oesophageal Cancer. Current Oncology. 2023; 30(2):1538-1545. https://doi.org/10.3390/curroncol30020118
Chicago/Turabian StyleChristodoulidis, Grigorios, Laura J. Halliday, Athina Samara, Neel Bhuva, Won-Ho Edward Park, and Krishna Moorthy. 2023. "Personalized Prehabilitation Improves Tolerance to Chemotherapy in Patients with Oesophageal Cancer" Current Oncology 30, no. 2: 1538-1545. https://doi.org/10.3390/curroncol30020118
APA StyleChristodoulidis, G., Halliday, L. J., Samara, A., Bhuva, N., Park, W. -H. E., & Moorthy, K. (2023). Personalized Prehabilitation Improves Tolerance to Chemotherapy in Patients with Oesophageal Cancer. Current Oncology, 30(2), 1538-1545. https://doi.org/10.3390/curroncol30020118