Alcoholic Liver Disease-Related Hepatocellular Carcinoma: Characteristics and Comparison to General Slovak Hepatocellular Cancer Population

 ,
,  , , and
, , and 
Abstract
:1. Introduction
2. Methods
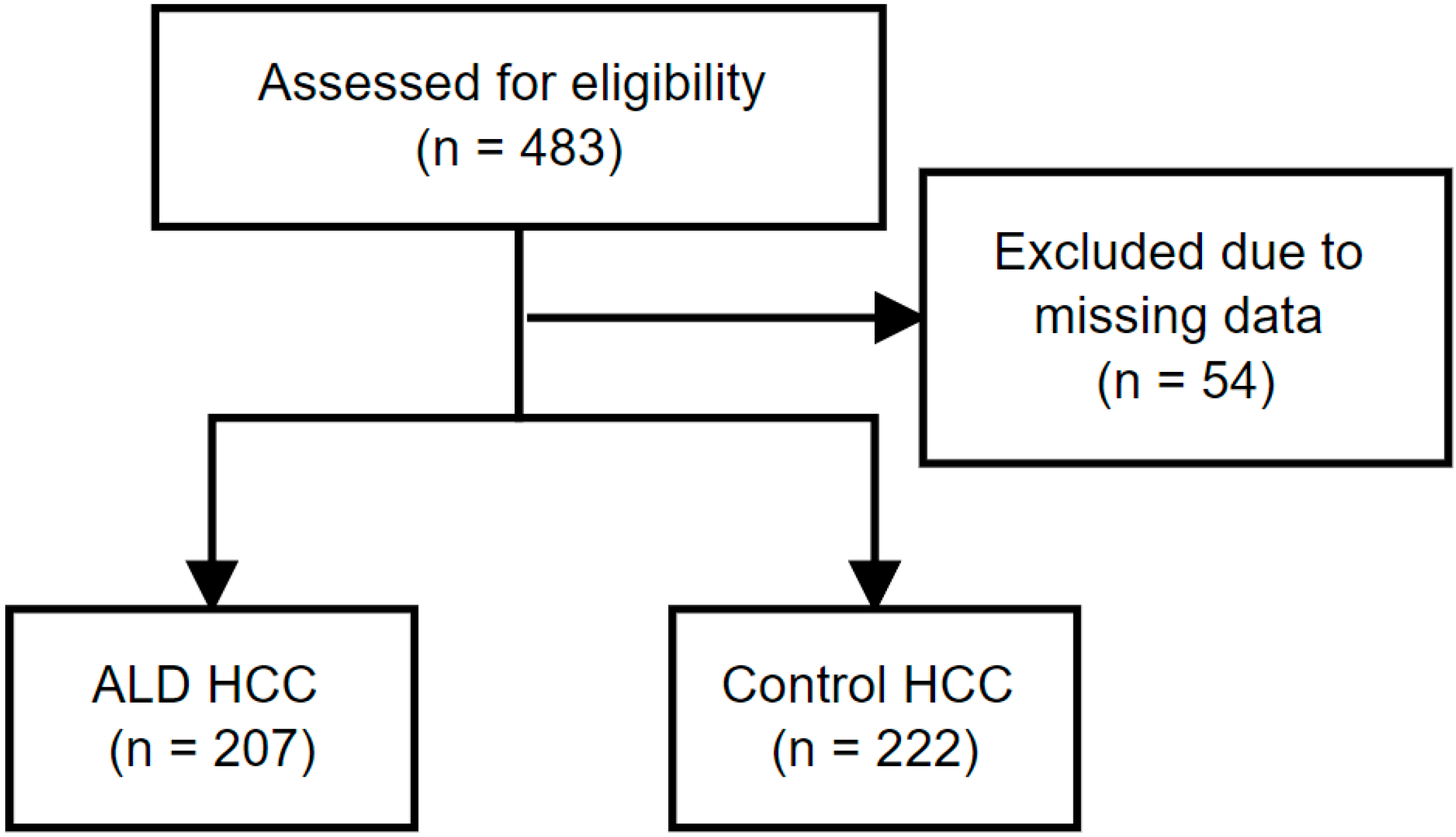
2.1. Patient Selection
2.2. Data Collection
2.3. Inflammatory Indexes Were Calculated as:
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Huang, D.Q.; El-Serag, H.B.; Loomba, R. Global epidemiology of NAFLD-related HCC: Trends, predictions, risk factors and prevention. Nat. Rev. Gastroenterol. Hepatol. 2020, 18, 223–238. [Google Scholar] [CrossRef] [PubMed]
- Llovet, J.M.; Kelley, R.K.; Villanueva, A.; Singal, A.G.; Pikarsky, E.; Roayaie, S.; Lencioni, R.; Koike, K.; Zucman-Rossi, J.; Finn, R.S. Hepatocellular carcinoma. Nat. Rev. Dis. Prim. 2021, 7, 6. [Google Scholar] [CrossRef]
- Llovet, J.M.; Zucman-Rossi, J.; Pikarsky, E.; Sangro, B.; Schwartz, M.; Sherman, M.; Gores, G. Hepatocellular carcinoma. Nat. Rev. Dis. Prim. 2016, 2, 16018. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Templeton, A.J.; Mcnamara, M.G.; Šeruga, B.; Vera-Badillo, F.E.; Aneja, P.; Ocaña, A.; Leibowitz-Amit, R.; Sonpavde, G.; Knox, J.J.; Tran, B.; et al. Prognostic Role of Neutrophil-to-Lymphocyte Ratio in Solid Tumors: A Systematic Review and Me-ta-Analysis. J. Natl. Cancer Inst. 2014, 106, dju124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lai, Q.; Melandro, F.; Laureiro, Z.L.; Giovanardi, F.; Corradini, S.G.; Ferri, F.; Hassan, R.; Rossi, M.; Mennini, G. Plate-let-to-lymphocyte ratio in the setting of liver transplantation for hepatocellular cancer: A systematic review and meta-analysis. World J. Gastroenterol. 2018, 24, 1658–1665. [Google Scholar] [CrossRef] [PubMed]
- Hu, B.; Yang, X.-R.; Xu, Y.; Sun, Y.-F.; Sun, C.; Guo, W.; Zhang, X.; Wang, W.-M.; Qiu, S.-J.; Zhou, J.; et al. Systemic Im-mune-Inflammation Index Predicts Prognosis of Patients after Curative Resection for Hepatocellular Carcinoma. Clin. Cancer Res. 2014, 20, 6212–6222. [Google Scholar] [CrossRef] [Green Version]
- European Association for The Study of The Liver; European Organisation for Research and Treatment of Cancer. EASL–EORTC clinical practice guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2012, 56, 908–943. [Google Scholar] [CrossRef] [Green Version]
- Park, J.; Chen, M.; Colombo, M.; Roberts, L.; Schwartz, M.; Chen, P.-J.; Kudo, M.; Johnson, P.; Wagner, S.; Orsini, L.S.; et al. Global patterns of hepatocellular carcinoma management from diagnosis to death: The BRIDGE Study. Liver Int. 2015, 35, 2155–2166. [Google Scholar] [CrossRef] [Green Version]
- Ganne-Carrié, N.; Nahon, P. Hepatocellular carcinoma in the setting of alcohol-related liver disease. J. Hepatol. 2019, 70, 284–293. [Google Scholar] [CrossRef] [Green Version]
- Torisu, Y.; Ikeda, K.; Kobayashi, M.; Hosaka, T.; Sezaki, H.; Akuta, N.; Kawamura, Y.; Yatsuji, H.; Suzuki, F.; Suzuki, Y.; et al. Diabetes mellitus increases the risk of hepatocarcinogenesis in patients with alcoholic cirrhosis: A preliminary report. Hepatol. Res. 2007, 37, 517–523. [Google Scholar] [CrossRef]
- Kodama, K.; Tokushige, K.; Hashimoto, E.; Taniai, M.; Shiratori, K. Hepatic and Extrahepatic Malignancies in Cirrhosis Caused by Nonalcoholic Steatohepatitis and Alcoholic Liver Disease. Alcohol. Clin. Exp. Res. 2013, 37, E247–E252. [Google Scholar] [CrossRef] [PubMed]
- N’Kontchou, G.; Paries, J.; Htar, M.T.T.; Ganne-Carrié, N.; Costentin, L.; Grando–Lemaire, V.; Trinchet, J.; Beaugrand, M. Risk Factors for Hepatocellular Carcinoma in Patients with Alcoholic or Viral C Cirrhosis. Clin. Gastroenterol. Hepatol. 2006, 4, 1062–1068. [Google Scholar] [CrossRef] [PubMed]
- Loomba, R.; Yang, H.-I.; Su, J.; Brenner, D.; Barrett-Connor, E.; Iloeje, U.; Chen, C.-J. Synergism Between Obesity and Alcohol in Increasing the Risk of Hepatocellular Carcinoma: A Prospective Cohort Study. Am. J. Epidemiol. 2013, 177, 333–342. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Altamirano, J.; Bataller, R. Cigarette smoking and chronic liver diseases. Gut 2010, 59, 1159–1162. [Google Scholar] [CrossRef]
- Popova, S.; Rehm, J.; Patra, J.; Zatonski, W. Comparing alcohol consumption in central and eastern Europe to other European countries. Alcohol Alcohol. 2007, 42, 465–473. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control. Systematic Review on Hepatitis B and C Prevalence in the EU/EEA. LU: Publications Office. Available online: https://data.europa.eu/doi/10.2900/24396 (accessed on 1 July 2022).
- Baecker, A.; Liu, X.; La Vecchia, C.; Zhang, Z.-F. Worldwide incidence of hepatocellular carcinoma cases attributable to major risk factors. Eur. J. Cancer Prev. 2018, 27, 205–212. [Google Scholar] [CrossRef]
- Akinyemiju, T.; Abera, S.; Ahmed, M.; Alam, N.; Alemayohu, M.A.; Allen, C.; Al-Raddadi, R.; Alvis-Guzman, N.; Amoako, Y.; Artaman, A.; et al. The Burden of Primary Liver Cancer and Underlying Etiologies from 1990 to 2015 at the Global, Regional, and National Level: Results from the Global Burden of Disease Study. JAMA Oncol. 2017, 3, 1683–1691. [Google Scholar]
- Hester, C.A.; Rich, N.E.; Singal, A.G.; Yopp, A.C. Comparative Analysis of Nonalcoholic Steatohepatitis—Versus Viral Hep-atitis– and Alcohol-Related Liver Disease–Related Hepatocellular Carcinoma. J. Natl. Compr. Cancer Netw. 2019, 17, 322–329. [Google Scholar] [CrossRef] [Green Version]
- Costentin, C.E.; Mourad, A.; Lahmek, P.; Causse, X.; Pariente, A.; Hagège, H.; Dobrin, A.S.; Becker, C.; Marks, B.; Bader, R.; et al. Hepatocellular carcinoma is diagnosed at a later stage in alcoholic patients: Results of a prospective, nationwide study. Cancer 2018, 124, 1964–1972. [Google Scholar] [CrossRef]
- Delemos, A.; Patel, M.; Gawrieh, S.; Burney, H.; Dakhoul, L.; Miller, E.; Scanga, A.; Kettler, C.; Liu, H.; Roche, P.; et al. Dis-tinctive Features and Outcomes of Hepatocellular Carcinoma in Patients with Alcohol-Related Liver Disease: A US Multicenter Study. Clin. Transl. Gastroenterol. 2020, 11, e00139. [Google Scholar] [CrossRef]
- Schütte, K.; Bornschein, J.; Kahl, S.; Seidensticker, R.; Arend, J.; Ricke, J.; Malfertheiner, P. Delayed Diagnosis of HCC with Chronic Alcoholic Liver Disease. Liver Cancer 2012, 1, 257–266. [Google Scholar] [CrossRef] [PubMed]
- Bucci, L.; Garuti, F.; Camelli, V.; Lenzi, B.; Farinati, F.; Giannini, E.G.; Ciccarese, F.; Piscaglia, F.; Rapaccini, G.L.; Di Marco, M.; et al. Comparison between alcohol- and hepatitis C virus-related hepatocellular carcinoma: Clinical presentation, treatment and outcome. Aliment. Pharmacol. Ther. 2015, 43, 385–399. [Google Scholar] [CrossRef] [PubMed]
- Trevisani, F.; Magini, G.; Santi, V.; Morselli/labate, A.M.; Cantarini, M.C.; Di Nolfo, M.A.; Del Poggio, P.; Benvegnù, L.; Ra-paccini, G.; Farinati, F.; et al. Impact of Etiology of Cirrhosis on the Survival of Patients Diagnosed with Hepatocellular Car-cinoma During Surveillance. Am. J. Gastroenterol. 2007, 102, 1022–1031. [Google Scholar] [CrossRef] [PubMed]
- Facciorusso, A.; El Aziz, M.A.A.; Tartaglia, N.; Ramai, D.; Mohan, B.P.; Cotsoglou, C.; Pusceddu, S.; Giacomelli, L.; Ambrosi, A.; Sacco, R. Microwave Ablation Versus Radiofrequency Ablation for Treatment of Hepatocellular Carcinoma: A Me-ta-Analysis of Randomized Controlled Trials. Cancers 2020, 12, 3796. [Google Scholar] [CrossRef] [PubMed]
- Facciorusso, A.; Aziz, M.A.A.E.; Singh, S.; Pusceddu, S.; Milione, M.; Giacomelli, L.; Sacco, R. Statin Use Decreases the Inci-dence of Hepatocellular Carcinoma: An Updated Meta-Analysis. Cancers 2020, 12, 874. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zeng, R.W.; Yong, J.N.; Tan, D.J.H.; Fu, C.E.; Lim, W.H.; Xiao, J.; Chan, K.E.; Tan, C.; Goh, X.L.; Chee, D.; et al. Meta-analysis: Chemoprevention of hepatocellular carcinoma with statins, aspirin and metformin. Aliment. Pharmacol. Ther. 2023, 57, 600–609. [Google Scholar] [CrossRef]
- Zhou, Y.-Y.; Zhu, G.-Q.; Liu, T.; Zheng, J.-N.; Cheng, Z.; Zou, T.-T.; Braddock, M.; Fu, S.-W.; Zheng, M.-H. Systematic Review with Network Meta-Analysis: Antidiabetic Medication and Risk of Hepatocellular Carcinoma. Sci. Rep. 2016, 6, 33743. [Google Scholar] [CrossRef] [Green Version]
- Antwi, S.O.; Li, Z.; Mody, K.; Roberts, L.R.; Patel, T. Independent and Joint Use of Statins and Metformin by Elderly Patients with Diabetes and Overall Survival Following HCC Diagnosis. J. Clin. Gastroenterol. 2019, 54, 468–476. [Google Scholar] [CrossRef]
- Shen, G.-L.; Lu, Y.; Liang, L.; Lu, W.-F.; Diao, Y.-K.; Xiao, Z.-Q.; Zhang, K.-J.; Zhang, J.-G.; Zhang, C.-W.; Liu, J. Impact of diabetes mellitus on the long-term prognosis of patients with hepatocellular carcinoma after hepatectomy. Expert Rev. Gas-Troenterol. Hepatol. 2022, 16, 473–478. [Google Scholar] [CrossRef]
- Zhang, H.; Li, H.; Lan, X.; Liu, F.; Li, B.; Wei, Y. Diabetes mellitus affects long-term survival in hepatitis B virus-related hepatocellular carcinoma patients. Medicine 2021, 100, e24354. [Google Scholar] [CrossRef]
- Ringelhan, M.; Pfister, D.; O’Connor, T.; Pikarsky, E.; Heikenwalder, M. The immunology of hepatocellular carcinoma. Nat. Immunol. 2018, 19, 222–232. [Google Scholar] [CrossRef] [PubMed]
- Llovet, J.M.; Castet, F.; Heikenwalder, M.; Maini, M.K.; Mazzaferro, V.; Pinato, D.J.; Pikarsky, E.; Zhu, A.X.; Finn, R.S. Im-munotherapies for hepatocellular carcinoma. Nat. Rev. Clin. Oncol. 2021, 19, 151–172. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Etiology | N | % | 95% CI |
|---|---|---|---|
| Alcoholic liver disease | 207 | 48.3 | 43–53 |
| Chronic hepatitis C | 64 | 14.9 | 11.7–18.7 |
| NAFLD | 54 | 12.6 | 9.6–16.1 |
| Chronic hepatitis B | 43 | 10 | 7.4–13.3 |
| Alcohol in combination | 9 | 2.1 | 0.9–3.9 |
| HBV + HCV coinfection | 1 | 0.2 | 0.01–1.3 |
| Cryptogenic liver disease | 40 | 9.3 | 6.7–12.5 |
| Parameter | n | ALD | n | Control Group | P |
|---|---|---|---|---|---|
| Patients | 207 | 207 (48.3%) | 222 | 222 (51.7%) | N/A |
| Male sex | 207 | 153(73.9%) | 222 | 127(57.2%) | <0.0001 |
| Age at diagnosis (years) | 207 | 66.6 ± 0.5 | 222 | 65.0 ± 0.8 | 0.112 |
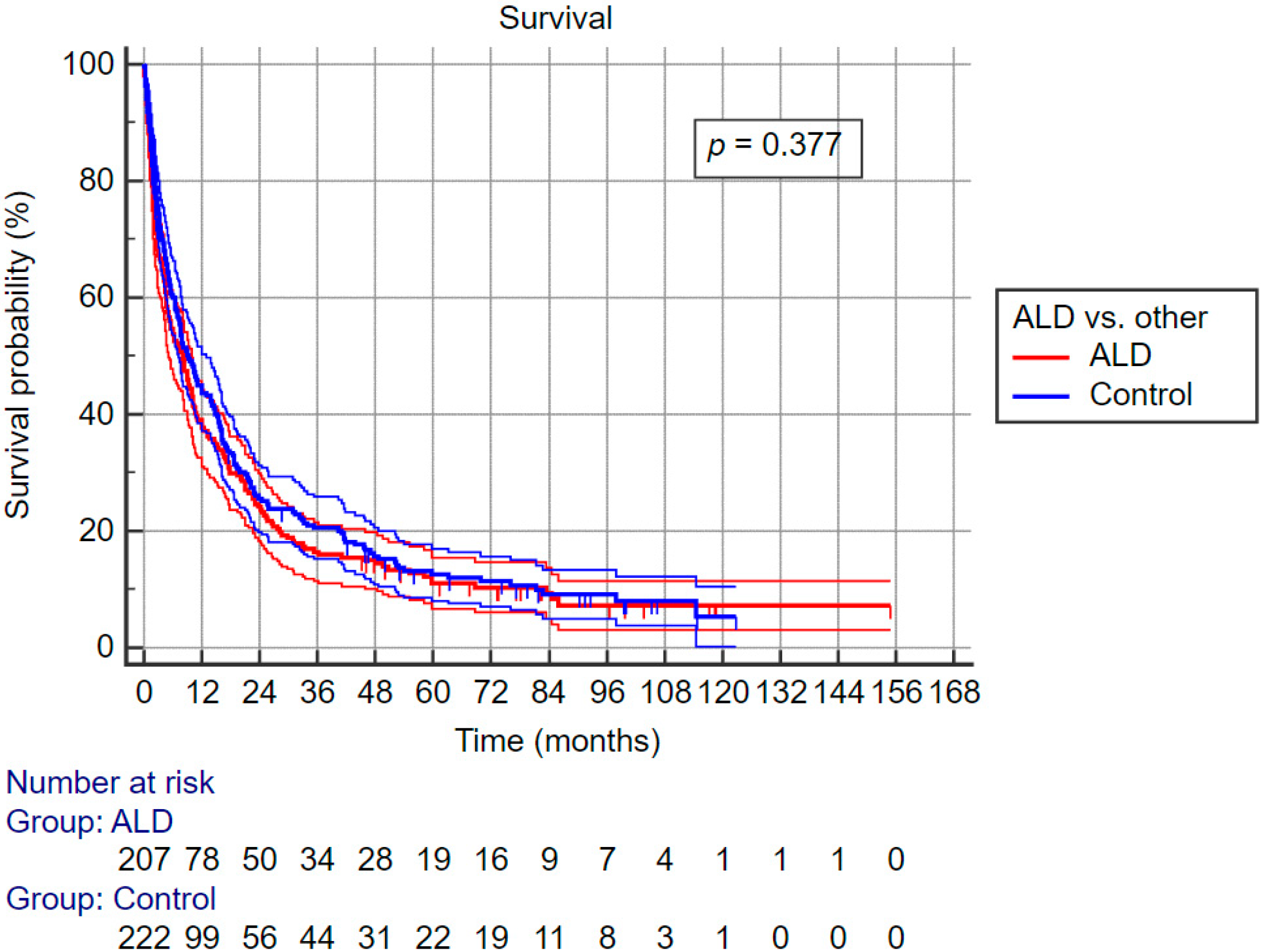
| Diabetes mellitus present | 207 | 72 (35%) | 220 | 86(39%) | 0.377 |
| Statin use at baseline | 207 | 10(4.8%) | 222 | 15(6.8%) | 0.395 |
| BCLC stage 0–A | 207 | 37(17.9%) | 221 | 33(14.9%) | 0.079 |
| BCLC stage B | 56(27.1%) | 70(31.5%) | |||
| BCLC stage C | 62(30.0%) | 83(37.4%) | |||
| BCLC stage D | 52(25.1%) | 36(16.2%) | |||
| Cirrhosis at diagnosis | 207 | 206(99.5%) | 221 | 206(93.2%) | <0.0001 |
| Child–Pugh points | 196 | 7.4 ± 0.14 | 209 | 6.7 ± 0.13 | <0.0001 |
| MELD score | 196 | 6.5 ± 0.41 | 213 | 6.2 ± 0.44 | <0.0001 |
| Performance status ECOG 0 | 207 | 2(1%) | 222 | 8(3.6%) | 0.009 |
| Performance status ECOG 1 | 151(72.9%) | 182(82%) | |||
| Performance status ECOG 2 | 52(25.1%) | 31(14.0%) | |||
| Performance status ECOG 3 | 2(1.0%) | 1(0.5%) | |||
| BMI (kg/m2) | 37 | 28.69 ± 0.57 | 42 | 29.62 ± 0.71 | 0.320 |
| CRP (mg/L) | 167 | 27.62 ± 2.35 | 174 | 25.69 ± 2.91 | 0.608 |
| AST (ukat/L) | 207 | 1.51 ± 0.1 | 221 | 2.58 ± 0.81 | 0.203 |
| ALT (ukat/L) | 207 | 0.88 ± 0.07 | 221 | 1.08 ± 0.06 | 0.031 |
| ALP (ukat/L) | 205 | 3.27 ± 0.21 | 219 | 3.3 ± 0.19 | 0.935 |
| GGT (ukat/L) | 207 | 4.07 ± 0.28 | 220 | 3.58 ± 0.25 | 0.194 |
| Total bilirubin (umol/L) | 207 | 44.31 ± 4.44 | 221 | 31.89 ± 2.72 | 0.016 |
| Direct bilirubin (umol/L) | 166 | 24.52 ± 3.47 | 158 | 18.67 ± 2.19 | 0.159 |
| Albumin (g/L) | 203 | 32.49 ± 0.53 | 216 | 33.64 ± 0.55 | 0.131 |
| INR | 199 | 1.27 ± 0.01 | 215 | 1.26 ± 0.02 | 0.873 |
| Neutrophiles (×109/L) | 181 | 4.99 ± 0.26 | 206 | 4.74 ± 0.24 | 0.466 |
| Lymphocytes (×109/L) | 152 | 1.28 ± 0.06 | 176 | 1.36 ± 0.05 | 0.316 |
| Platelets (×109/L) | 207 | 164.36 ± 7.59 | 219 | 192.93 ± 8.61 | 0.014 |
| Cholesterol (mmol/L) | 76 | 13.19 ± 8.81 | 98 | 4.15 ± 0.17 | 0.245 |
| HDL (mmol/L) | 53 | 0.99 ± 0.08 | 75 | 1.37 ± 0.19 | 0.104 |
| LDL (mmol/L) | 52 | 2.79 ± 0.19 | 73 | 3.38 ± 0.94 | 0.601 |
| Triglycerides (mmol/L) | 59 | 1.25 ± 0.08 | 93 | 1.26 ± 0.09 | 0.948 |
| Creatinine (μmol/L) | 204 | 98.96 ± 4.2 | 219 | 85.43 ± 2.4 | 0.005 |
| Urea (mmol/L) | 206 | 7.61 ± 0.59 | 219 | 6.91 ± 0.56 | 0.395 |
| Na (mmol/L) | 204 | 137.4 ± 1.58 | 218 | 137.6 ± 0.36 | 0.898 |
| AFP (kIU/L) | 180 | 28.1 (864.1) | 195 | 44 (666.7) | 0.094 |
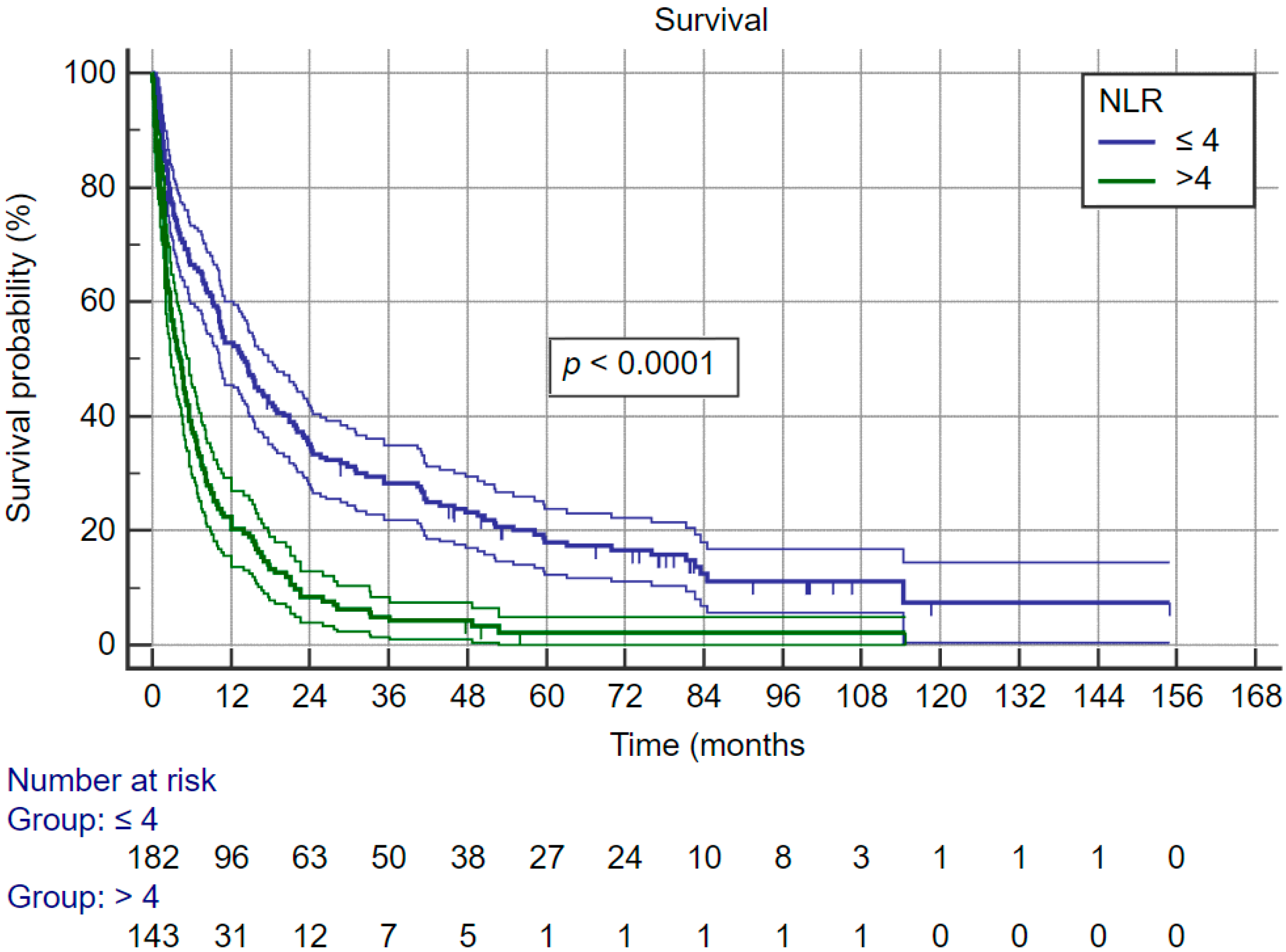
| NLR | 150 | 4 (3.51) | 174 | 3.42 (3.1) | 0.056 |
| TLR | 151 | 129.8 (136.7) | 175 | 141.2 (127.7) | 0.803 |
| APRI | 207 | 2 ± 0.15 | 219 | 3.01 ± 0.82 | 0.240 |
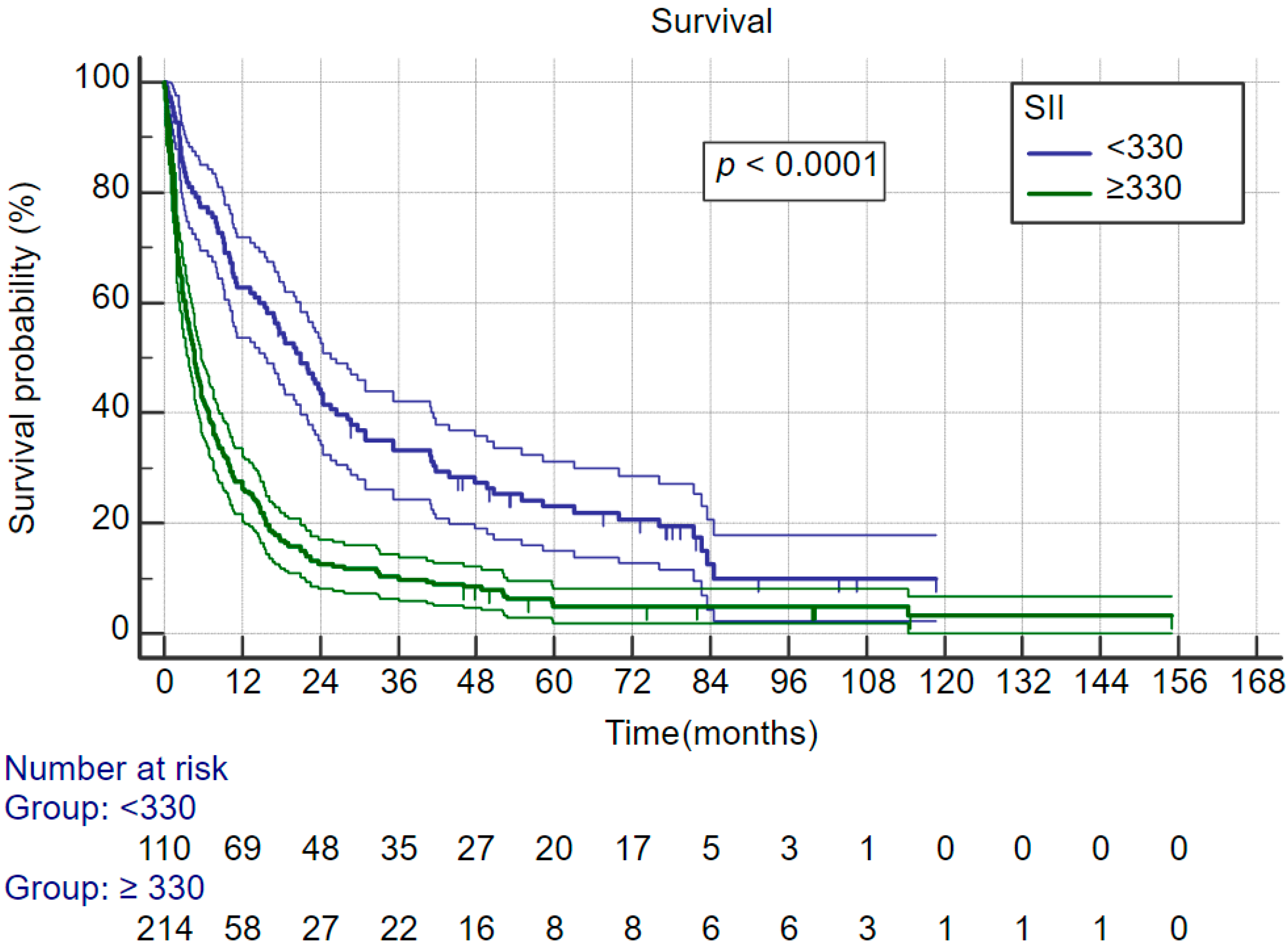
| SII (109 cells/L) | 150 | 563 (973.3) | 174 | 552.9 (972.2) | 0.773 |
| No. lesions | 192 | 2 (5) | 212 | 2 (4,8) | 0.629 |
| Max lesion size (mm) | 192 | 59.8 ± 3.4 | 212 | 63.7 ± 2.8 | 0.053 |
| MAVI—0 | 207 | 168(81.2%) | 222 | 169(76.1%) | 0.117 |
| MAVI—1 | 16(7.7%) | 31(14.0%) | |||
| MAVI—2 | 23(11.1%) | 22(9.9%) | |||
| MIVI—0 | 207 | 163(78.7%) | 222 | 163(73.4%) | 0.436 |
| MIVI—1 | 41(19.8%) | 55(24.8%) | |||
| MIVI—2 | 3(1.4%) | 4(1.8%) | |||
| DFS/PFS (months) | 207 | 4.9(0–154.9) | 222 | 5.7(0.1–114.7) | 0.528 |
| OS (months) | 207 | 8.1(0–154.9) | 222 | 8.5(0.1–122.9) | 0.315 |
| Treatment | ALD | Control | ||
|---|---|---|---|---|
| n | % | n | % | |
| Resection | 14 | 6.8% | 30 | 10.9% |
| RFA | 9 | 4.3% | 13 | 4.7% |
| TACE | 46 | 22.2% | 55 | 19.9% |
| Sorafenib | 49 | 23.7% | 93 | 33.7% |
| Supportive | 76 | 36.7% | 70 | 25.4% |
| Sorafenib + TACE | 1 | 0.5% | 0 | 0.0% |
| Second line chemo | 1 | 0.5% | 3 | 1.1% |
| LTx | 11 | 5.3% | 12 | 4.3% |
| Response | ALD | Control | ||
|---|---|---|---|---|
| n | % | n | % | |
| Complete response | 36 | 17.60 | 56 | 20.4 |
| Partial response | 27 | 13.20 | 25 | 9.1 |
| Stable disease | 23 | 11.30 | 48 | 17.5 |
| Progressive disease | 118 | 57.80 | 146 | 53.1 |
| Variable | ALD-Related HCC | Control Group HCC | ||
|---|---|---|---|---|
| Cox HR | P | Cox HR (95% CI) | P | |
| Age | 1.030 (1.011–1.050) | 0.002 | 1.009 (0.999–1.020) | 0.087 |
| Sex | 1.262 (0.911–1.748) | 0.161 | 1.2 (0.932–1.545) | 0.156 |
| DM present | 1.125 (0.834–1.517) | 0.441 | 1.052 (0.789–1.401) | 0.731 |
| BCLC—0–A (ref) | ||||
| BCLC—B | 1.751 (1.077–2.849) | <0.024 | 2.445 (1.496–3.994) | <0.0001 |
| BCLC—C | 4.884 (2.983–7.996) | <0.0001 | 7.733 (4.694–12.747) | <0.0001 |
| BCLC—D | 10.856 (6.485–18.173) | <0.0001 | 24.968 (14.173–43.983) | <0.0001 |
| CRP | 1.013 (1.008–1.017) | <0.0001 | 1.009 (1.006–1.012) | <0.0001 |
| PLR | 1.590 (1.211–2.087) | 0.001 | 1.760 (1.366–2.267) | <0.0001 |
| NLR | 2.037 (1.563–2.654) | <0.0001 | 2.015 (1.559–2.605) | <0.0001 |
| AFP | 1.134 (1.073–1.198) | <0.0001 | 1.073 (1.015–1.134) | 0.012 |
| SII | 1.736 (1.437–2.098) | <0.0001 | 1.662 (1.411–1.957) | <0.0001 |
| MELD | 2.076 (1.1545–2.788) | <0.0001 | 1.402 (1.119–1.758) | 0.003 |
| Child–Pugh | 1.222 (1.132–1.318) | <0.0001 | 1.139 (1.064–1.220) | <0.0001 |
| Max lesion size | 1.005 (1.002–1.009) | 0.002 | 1.006 (1.003–1.008) | <0.0001 |
| No. of lesions | 1.156 (1.104–1.202) | <0.0001 | 1.101 (1.072–1.12)1 | <0.0001 |
| ECOG—0 (ref) | <0.0001 | <0.0001 | ||
| ECOG—1 | 0.784 (0.194–3.176) | 0.733 | 0.659 (0.405–1.070) | 0.092 |
| ECOG—2 | 3.563 (0.862–14.727 | 0.079 | 2.543 (1.453–4.448) | 0.001 |
| ECOG—3 | 5.352 (0.737–38.856) | 0.097 | 4.420 (1.006–19.412) | 0.049 |
| Variable | ALD-HCC | Control Group HCC | ||||
|---|---|---|---|---|---|---|
| Sig. | Exp (B) | 95% CI | Sig. | Exp (B) | 95% CI | |
| Number of Tu | <0.0001 | 1.176 | 1.122–1.232 | <0.0001 | 1.117 | 1.07–1.166 |
| Max Tu size | <0.0001 | 1.007 | 1.003–1.011 | 0.001 | 1.007 | 1.003–1.011 |
| ECOG 0 | <0.0001 | <0.0001 | ||||
| ECOG 1 | 0.392 | 0.540 | 0.132–2.209 | 0.084 | 0.508 | 0.236–1.095 |
| ECOG 2 | 0.233 | 2.417 | 0.566–10.314 | 0.182 | 1.852 | 0.749–4.582 |
| ECOG 3 | 0.189 | 3.945 | 0.509–30.588 | 0.132 | 5.160 | 0.611–43.585 |
| MELD | 0.003 | 1.650 | 1.18–2.306 | 0.050 | 1.305 | 1–1.705 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Šafčák, D.; Dražilová, S.; Gazda, J.; Andrašina, I.; Adamcová-Selčanová, S.; Barila, R.; Mego, M.; Rác, M.; Skladaný, Ľ.; Žigrai, M.; et al. Alcoholic Liver Disease-Related Hepatocellular Carcinoma: Characteristics and Comparison to General Slovak Hepatocellular Cancer Population. Curr. Oncol. 2023, 30, 3557-3570. https://doi.org/10.3390/curroncol30030271
Šafčák D, Dražilová S, Gazda J, Andrašina I, Adamcová-Selčanová S, Barila R, Mego M, Rác M, Skladaný Ľ, Žigrai M, et al. Alcoholic Liver Disease-Related Hepatocellular Carcinoma: Characteristics and Comparison to General Slovak Hepatocellular Cancer Population. Current Oncology. 2023; 30(3):3557-3570. https://doi.org/10.3390/curroncol30030271
Chicago/Turabian StyleŠafčák, Dominik, Sylvia Dražilová, Jakub Gazda, Igor Andrašina, Svetlana Adamcová-Selčanová, Radovan Barila, Michal Mego, Marek Rác, Ľubomír Skladaný, Miroslav Žigrai, and et al. 2023. "Alcoholic Liver Disease-Related Hepatocellular Carcinoma: Characteristics and Comparison to General Slovak Hepatocellular Cancer Population" Current Oncology 30, no. 3: 3557-3570. https://doi.org/10.3390/curroncol30030271
APA StyleŠafčák, D., Dražilová, S., Gazda, J., Andrašina, I., Adamcová-Selčanová, S., Barila, R., Mego, M., Rác, M., Skladaný, Ľ., Žigrai, M., Janičko, M., & Jarčuška, P. (2023). Alcoholic Liver Disease-Related Hepatocellular Carcinoma: Characteristics and Comparison to General Slovak Hepatocellular Cancer Population. Current Oncology, 30(3), 3557-3570. https://doi.org/10.3390/curroncol30030271