An Unconventional Regimen of Carboplatin and Paclitaxel in Metastatic Colorectal Carcinosarcoma: A Case Report and Review of Literature

 ,
,
Abstract
:1. Introduction
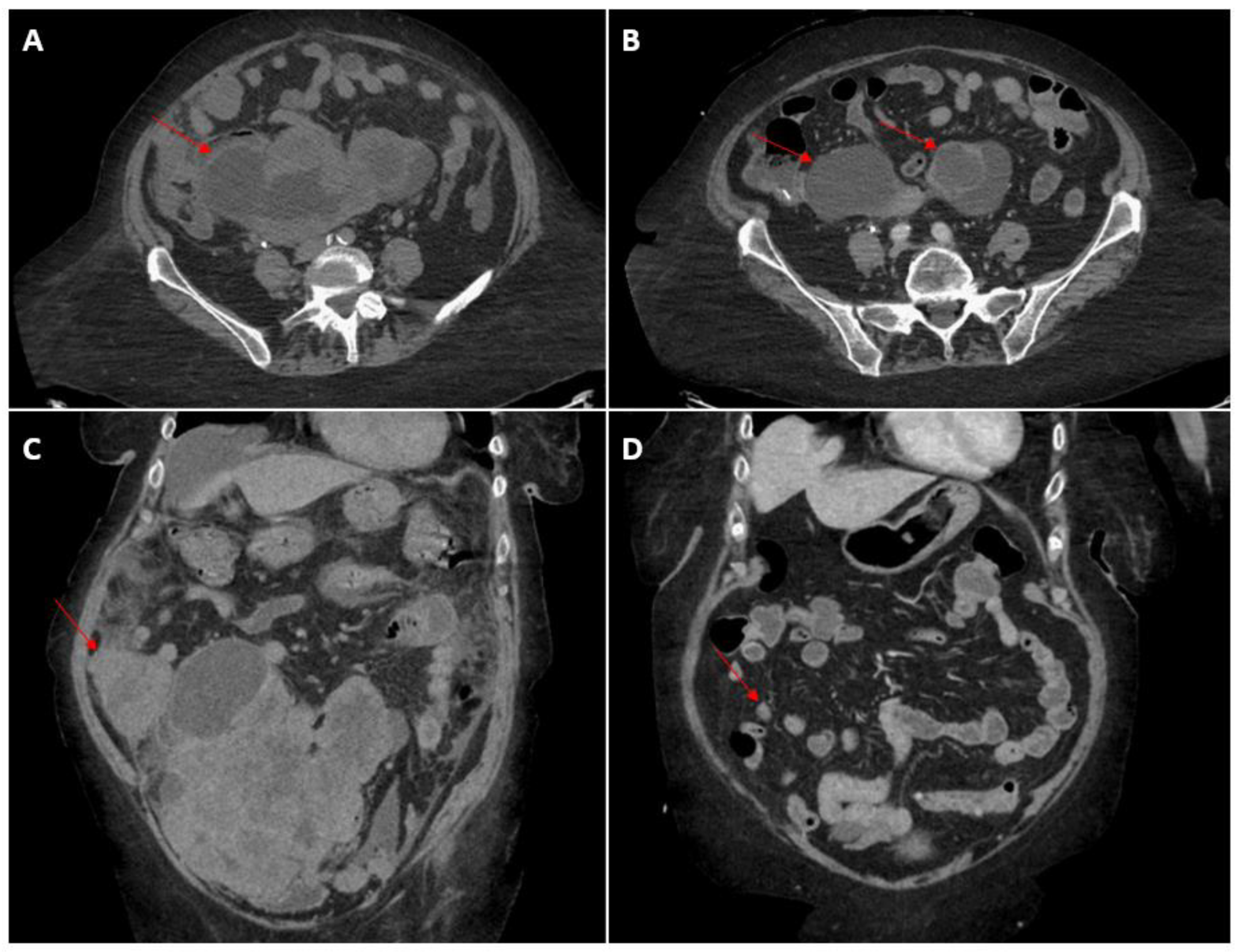
2. Case Presentation
3. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Feng, L.; Cai, D.; Muhetaer, A.; Yang, Y.-L.; Ren, F.; Yishake, M.; Zhang, H.; Fang, Y.; Wushou, A. Spindle cell carcinoma: The general demographics, basic clinico-pathologic characteristics, treatment, outcome and prognostic factors. Oncotarget 2017, 8, 43228–43236. [Google Scholar] [CrossRef] [PubMed]
- Zidar, N.; Gale, N. Carcinosarcoma and spindle cell carcinoma—Monoclonal neoplasms undergoing epithelial-mesenchymal transition. Virchows Arch. 2015, 466, 357–358. [Google Scholar] [CrossRef] [PubMed]
- Matsuzaki, S.; Klar, M.; Matsuzaki, S.; Roman, L.D.; Sood, A.K.; Matsuo, K. Uterine carcinosarcoma: Contemporary clinical summary, molecular updates, and future research opportunity. Gynecol. Oncol. 2021, 160, 586–601. [Google Scholar] [CrossRef] [PubMed]
- Ersek, J.L.; Symanowski, J.T.; Han, Y.; Howard, A.; Dumas, K.; Ahrens, W.; Kim, E.; Kim, E.S. Pulmonary Carcinosarcoma: A Surveillance, Epidemiology, and End Results (SEER) Analysis. Clin. Lung Cancer 2020, 21, 160–170. [Google Scholar] [CrossRef] [PubMed]
- He, H.-L.; Liu, Z.-L.; Ma, C.-Y.; Li, X.-G.; He, Y. Clinicopathological features of carcinosarcoma in oromaxillofacial head and neck region. Shanghai J. Stomatol. 2017, 26, 569–572. [Google Scholar] [PubMed]
- Rawla, P.; Sunkara, T.; Barsouk, A. Epidemiology of colorectal cancer: Incidence, mortality, survival, and risk factors. Przegla̜d Gastroenterol. 2019, 14, 89–103. [Google Scholar] [CrossRef] [PubMed]
- Saad, M.K.; Ghandour, F.; El Hajj, F.G.; El Hajj, I.; Saikaly, E. Colonic Carcinosarcoma: Report of a Rare Colorectal Malignancy and Review of Literature. Gastrointest. Tumors 2020, 8, 8–15. [Google Scholar] [CrossRef] [PubMed]
- Sudlow, A.; Liu, M.H.; Waters, G.; Velchuru, V.R. Carcinosarcoma of the Rectum: Report of a Rare Colorectal Malignancy and Review of the Literature. Case Rep. Surg. 2015, 2015, 412918. [Google Scholar] [CrossRef] [PubMed]
- Weidner, N.; Zekan, P. Carcinosarcoma of the colon. Report of a unique case with light and immunohistochemical studies. Cancer 1986, 58, 1126–1130. [Google Scholar] [CrossRef] [PubMed]
- Bertram, P.; Treutner, K.H.; Tietze, L.; Schumpelick, V. True carcinosarcoma of the colon. Case report. Langenbecks Arch. Chir. 1997, 382, 173–174. [Google Scholar] [PubMed]
- Kim, J.H.; Moon, W.S.; Kang, M.J.; Park, M.J.; Lee, D.G. Sarcomatoid carcinoma of the colon: A case report. J. Korean Med Sci. 2001, 16, 657–660. [Google Scholar] [CrossRef] [PubMed]
- Mori, Y.; Katsumata, K.; Suzuki, S.; Matsuda, D.; Hara, T.; Hayashida, Y.; Enomoto, M.; Wada, T.; Tsuchida, A.; Aoki, T.; et al. Carcinosarcoma of the Sigmoid Colon: Report of a Case. Case Rep. Gastroenterol. 2010, 4, 484–491. [Google Scholar] [CrossRef] [PubMed]
- Ambrosini-Spaltro, A.; Vaira, V.; Braidotti, P.; Rovati, M.P.L.; Ferrero, S.; Bosari, S. Carcinosarcoma of the colon: Report of a case with morphological, ultrastructural and molecular analysis. BMC Cancer 2006, 6, 185. [Google Scholar] [CrossRef] [PubMed]
- Macaigne, G.; Aouad, K.; Boivin, J.F.; Bellaïche, A.; Auriault, M.L.; Picard, D.; Deplus, R. Sarcomatoid carcinoma of the colon: Report of a case and review of the literature. Gastroenterol. Clin. Biol. 2004, 28 Pt 1, 600–604. [Google Scholar] [CrossRef] [PubMed]
- Patel, D.H.; Dang, S.; Bentley, F.R.; Julka, R.N.; Olden, K.W.; Aduli, F. Carcinosarcoma of the colon: A rare cause of colovesical fistula. Am. Surg. 2009, 75, 335–337. [Google Scholar] [CrossRef] [PubMed]
- Gong, J.; Cho, M.; Fakih, M. RAS and BRAF in metastatic colorectal cancer management. J. Gastrointest. Oncol. 2016, 7, 687–704. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Ref. | Metastatic Sites | Surgery? | Systemic Treatment | Best Response |
|---|---|---|---|---|
| [13] | Liver | Yes | Capecitabine | Stable disease sustained for 2 years |
| [14] | Liver, peritoneum | Yes | Doxorubicin | Disease progression |
| [15] | Liver | Yes | Gemcitabine + Docetaxel | Unknown |
| [9] | Peritoneum | Yes | 1: Mitomycin C + 5-FU 2: Cyclophosphamide + doxorubicin + carboplatin | Disease progression |
| [10] | Liver | Yes | 5-FU + Leucovorin | Disease progression |
| [11] | Liver, Lung, Brain | Yes | 5-FU + Leucovorin | Disease progression |
| [12] | Lung | Yes | FOLFIRI + Bevacizumab | Disease progression |
| * | Liver, peritoneum | No | Carboplatin + Paclitaxel | Partial response |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, C.L.; Rajadurai, C.V.; Ton Nu, T.N.; Mandilaras, V. An Unconventional Regimen of Carboplatin and Paclitaxel in Metastatic Colorectal Carcinosarcoma: A Case Report and Review of Literature. Curr. Oncol. 2023, 30, 4897-4903. https://doi.org/10.3390/curroncol30050369
Park CL, Rajadurai CV, Ton Nu TN, Mandilaras V. An Unconventional Regimen of Carboplatin and Paclitaxel in Metastatic Colorectal Carcinosarcoma: A Case Report and Review of Literature. Current Oncology. 2023; 30(5):4897-4903. https://doi.org/10.3390/curroncol30050369
Chicago/Turabian StylePark, Changsu Lawrence, Charles Vincent Rajadurai, Tuyet Nhung Ton Nu, and Victoria Mandilaras. 2023. "An Unconventional Regimen of Carboplatin and Paclitaxel in Metastatic Colorectal Carcinosarcoma: A Case Report and Review of Literature" Current Oncology 30, no. 5: 4897-4903. https://doi.org/10.3390/curroncol30050369
APA StylePark, C. L., Rajadurai, C. V., Ton Nu, T. N., & Mandilaras, V. (2023). An Unconventional Regimen of Carboplatin and Paclitaxel in Metastatic Colorectal Carcinosarcoma: A Case Report and Review of Literature. Current Oncology, 30(5), 4897-4903. https://doi.org/10.3390/curroncol30050369