Can Molecular Biomarkers Help Reduce the Overtreatment of DCIS?

 ,
, 
Abstract
:1. Introduction
2. Clinicopathological Factors to Identify Cases at Low Risk of Local Recurrence after BCS Where the Omission of RT Can Be Considered
3. Adjuvant Endocrine Therapy
4. Can Molecular Biomarkers Help De-Escalate the Treatment of DCIS?
4.1. Oncotype DX DCIS Score (Exact Sciences)
4.2. DCISionRT Decision Score (PreludeDx)
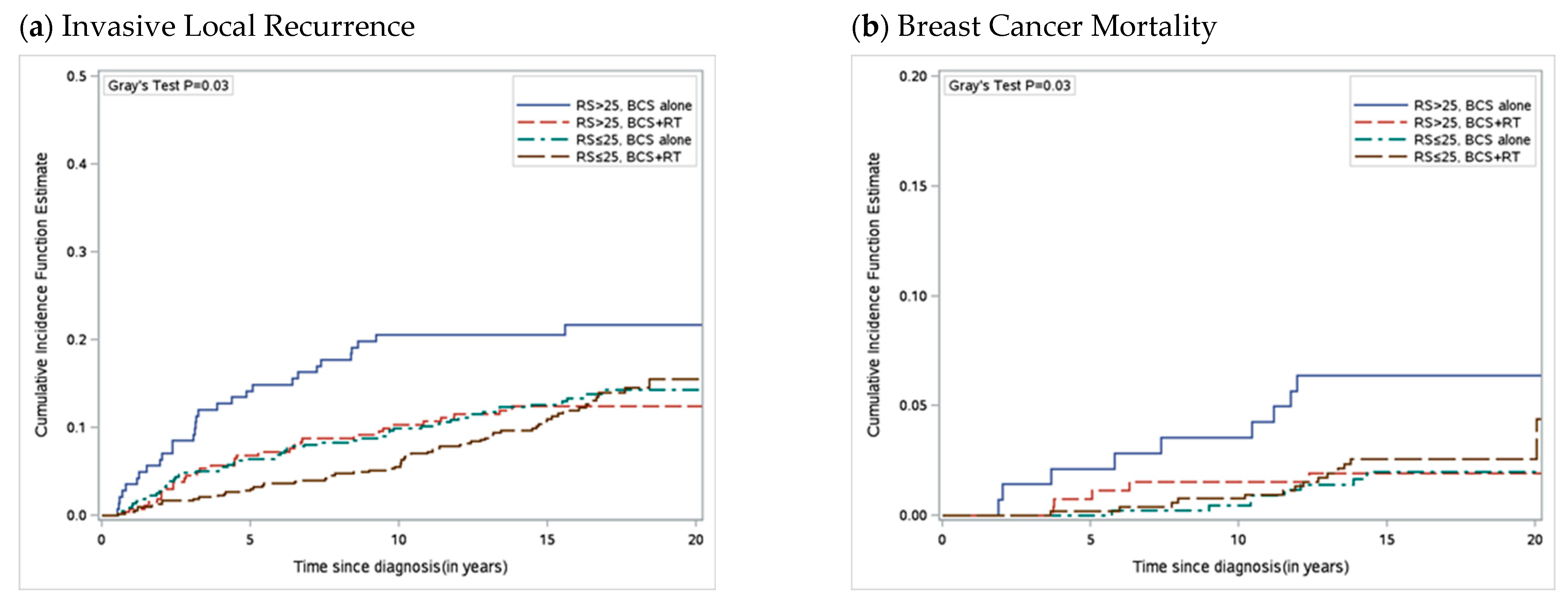
4.3. Oncotype 21-Gene Recurrence Score (Exact Sciences)
5. Predictive Modeling
6. Future Clinical Trials
7. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Ernster, V.L. Mammography screening for women aged 40 through 49—A guidelines saga and a clarion call for informed decision making. Am. J. Public Health 1997, 87, 1103–1106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ballard-Barbash, R.; Taplin, S.H.; Yankaskas, B.C.; Ernster, V.L.; Rosenberg, R.D.; Carney, P.A.; Barlow, W.E.; Geller, B.M.; Kerlikowske, K.; Edwards, B.K.; et al. Breast Cancer Surveillance Consortium: A national mammography screening and outcomes database. AJR Am. J. Roentgenol. 1997, 169, 1001–1008. [Google Scholar] [CrossRef]
- Ernster, V.L.; Ballard-Barbash, R.; Barlow, W.E.; Zheng, Y.; Weaver, D.L.; Cutter, G.; Yankaskas, B.C.; Rosenberg, R.; Carney, P.A.; Kerlikowske, K.; et al. Detection of Ductal Carcinoma In Situ in Women Undergoing Screening Mammography. J. Natl. Cancer Inst. 2002, 94, 1546–1554. [Google Scholar] [CrossRef] [Green Version]
- NCCN Clinical Practice Guidelines Breast. Version 5. 2020. Available online: https://www2.tri-kobe.org/nccn/guideline/breast/english/breast.pdf (accessed on 1 April 2023).
- Olivotto, I.; Levine, M.; Steering Committee on Clinical Practice Guidelines for the Care and Treatment of Breast Cancer. Clinical practice guidelines for the care and treatment of breast cancer: The management of ductal carcinoma in situ (summary of the 2001 update). CMAJ Can. Med. Assoc. J. 2001, 165, 912–913. [Google Scholar]
- Morrow, M.; Strom, E.A.; Bassett, L.W.; Dershaw, D.D.; Fowble, B.; Harris, J.R.; O’Malley, F.; Schnitt, S.J.; Singletary, S.E.; Winchester, D.P. Standard for the Management of Ductal Carcinoma In Situ of the Breast (DCIS). CA Cancer J. Clin. 2002, 52, 256–276. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- EBCTCG; Correa, C.; McGale, P.; Taylor, C.; Wang, Y.; Clarke, M.; Davies, C.; Peto, R.; Bijker, N.; Solin, L.; et al. Overview of the randomized trials of radiotherapy in ductal carcinoma in situ of the breast. J. Natl. Cancer Inst. Monogr. 2010, 2010, 162–177. [Google Scholar]
- Paszat, L.; Sutradhar, R.; Zhou, L.; Nofech-Mozes, S.; Rakovitch, E. Including the Ductal Carcinoma-In-Situ (DCIS) Score in the Development of a Multivariable Prediction Model for Recurrence After Excision of DCIS. Clin. Breast Cancer 2019, 19, 35–46. [Google Scholar] [CrossRef] [Green Version]
- Wapnir, I.L.; Dignam, J.J.; Fisher, B.; Mamounas, E.P.; Anderson, S.J.; Julian, T.B.; Land, S.R.; Margolese, R.G.; Swain, S.M.; Costantino, J.P.; et al. Long-Term Outcomes of Invasive Ipsilateral Breast Tumor Recurrences After Lumpectomy in NSABP B-17 and B-24 Randomized Clinical Trials for DCIS. J. Natl. Cancer Inst. 2011, 103, 478–488. [Google Scholar]
- Donker, M.; Litiere, S.; Werutsky, G.; Julien, J.P.; Fentiman, I.S.; Agresti, R.; Rouanet, P.; de Lara, C.T.; Bartelink, H.; Duez, N.; et al. Breast-Conserving Treatment with or without Radiotherapy in Ductal Carcinoma In Situ: 15-Year Recurrence Rates and Outcome after a Recurrence, from the EORTC 10853 Randomized Phase III Trial. J. Clin. Oncol. 2013, 31, 4054–4059. [Google Scholar] [CrossRef]
- Thompson, A.M.; Clements, K.; Cheung, S.; Pinder, S.E.; Lawrence, G.; Sawyer, E.; Kearins, O.; Ball, G.R.; Tomlinson, I.; Hanby, A.; et al. Management and 5-year outcomes in 9938 women with screen-detected ductal carcinoma in situ: The UK Sloane Project. Eur. J. Cancer 2018, 101, 210–219. [Google Scholar] [CrossRef] [Green Version]
- Fisher, B.; Dignam, J.; Wolmark, N.; Mamounas, E.; Costantino, J.; Poller, W.; Fisher, E.R.; Wickerham, D.L.; Deutsch, M.; Margolese, R.; et al. Lumpectomy and radiation therapy for the treatment of intraductal breast cancer: Findings from National Surgical Adjuvant Breast and Bowel Project B-17. J. Clin. Oncol. 1998, 16, 441–452. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Julien, J.P.; Bijker, N.; Fentiman, I.S.; Peterse, J.L.; Delledonne, V.; Rouanet, P.; Avril, A.; Sylvester, R.; Mignolet, F.; Bartelink, H.; et al. Radiotherapy in breast-conserving treatment for ductal carcinoma in situ: First results of the EORTC randomised phase III trial 10853. Lancet 2000, 355, 528–533. [Google Scholar] [CrossRef] [PubMed]
- Houghton, J.; UK Coordinating Committee on Cancer Research (UKCCCR) Ductal Carcinoma In Situ (DCIS) Working Party on Behalf of DCIS Trialists in the UK, Australia, and New Zealand. Radiotherapy and tamoxifen in women with completely excised ductal carcinoma in situ of the breast in the UK, Australia, and New Zealand: Randomised controlled trial. Lancet 2003, 362, 95–102. [Google Scholar]
- Warnberg, F.; Garmo, H.; Emdin, S.; Hedberg, V.; Adwall, L.; Sandelin, K.; Ringberg, A.; Karlsson, P.; Arnesson, L.G.; Anderson, H.; et al. Effect of radiotherapy after breast-conserving surgery for ductal carcinoma in situ: 20 years follow-up in the randomized SweDCIS Trial. J. Clin. Oncol. 2014, 32, 3613–3618. [Google Scholar] [CrossRef] [PubMed]
- Fisher, B.; Redmond, C.; Poisson, R.; Margolese, R.; Wolmark, N.; Wickerham, L.; Fisher, E.; Deutsch, M.; Caplan, R.; Pilch, Y. Eight-year results of a randomized clinical trial comparing total mastectomy and lumpectomy with or without irradiation in the treatment of breast cancer. N. Engl. J. Med. 1989, 320, 822–828, Erratum in N. Engl. J. Med. 1994, 330, 1467. [Google Scholar] [CrossRef]
- Cuzick, J.; Sestak, I.; Pinder, S.E.; Ellis, I.O.; Forsyth, S.; Bundred, N.J.; Forbes, J.F.; Bishop, H.; Fentiman, I.S.; George, W.D. Effect of tamoxifen and radiotherapy in women with locally excised ductal carcinoma in situ: Long-term results from the UK/ANZ DCIS trial. Lancet Oncol. 2011, 12, 21–29. [Google Scholar] [CrossRef]
- Rakovitch, E.; Nofech-Mozes, S.; Hanna, W.; Sutradhar, R.; Gu, S.; Fong, C.; Tuck, A.; Youngson, B.; Miller, N.; Done, S.J.; et al. Omitting radiation therapy after lumpectomy for pure DCIS does not reduce the risk of salvage mastectomy. Breast 2018, 37, 181–186. [Google Scholar] [CrossRef] [Green Version]
- Withrow, D.R.; Morton, L.M.; Curtis, R.E.; Schonfeld, S.J.; Berrington de Gonzalez, A. Radiotherapy for ductal carcinoma in situ and risk of second non-breast cancers. Breast Cancer Res. Treat. 2017, 166, 299–306. [Google Scholar] [CrossRef]
- Taylor, C.W.; Kirby, A.M. Cardiac Side-effects From Breast Cancer Radiotherapy. Clin. Oncol. 2015, 27, 621–629. [Google Scholar] [CrossRef]
- Whelan, T.J.; Levine, M.; Julian, J.; Kirkbride, P.; Skingley, P. The effects of radiation therapy on quality of life of women with breast carcinoma: Results of a randomized trial. Ontario Clinical Oncology Group. Cancer 2000, 88, 2260–2266. [Google Scholar]
- Longo, C.J.; Fitch, M.I.; Banfield, L.; Hanly, P.; Yabroff, K.R.; Sharp, L. Financial toxicity associated with a cancer diagnosis in publicly funded healthcare countries: A systematic review. Support. Care Cancer 2020, 28, 4645–4665. [Google Scholar] [CrossRef] [PubMed]
- Jagsi, R.; Ward, K.C.; Abrahamse, P.H.; Wallner, L.P.; Kurian, A.W.; Hamilton, A.S.; Katz, S.J.; Hawley, S.T. Unmet need for clinician engagement regarding financial toxicity after diagnosis of breast cancer. Cancer 2018, 124, 3668–3676. [Google Scholar] [CrossRef] [PubMed]
- Hwang, E.S.; Hyslop, T.; Lynch, T.; Frank, E.; Pinto, D.; Basila, D.; Collyar, D.; Bennett, A.; Kaplan, C.; Rosenberg, S.; et al. The COMET (Comparison of Operative versus Monitoring and Endocrine Therapy) trial: A phase III randomised controlled clinical trial for low-risk ductal carcinoma in situ (DCIS). BMJ Open 2019, 9, e026797. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Francis, A.; Fallowfield, L.; Rea, D. The LORIS Trial: Addressing overtreatment of ductal carcinoma in situ. Clin. Oncol. 2015, 27, 6–8. [Google Scholar] [CrossRef] [PubMed]
- Elshof, L.E.; Tryfonidis, K.; Slaets, L.; van Leeuwen-Stok, A.E.; Skinner, V.P.; Dif, N.; Pijnappel, R.M.; Bijker, N.; Rutgers, E.J.; Wesseling, J. Feasibility of a prospective, randomised, open-label, international multicentre, phase III, non-inferiority trial to assess the safety of active surveillance for low risk ductal carcinoma in situ—The LORD study. Eur. J. Cancer 2015, 51, 1497–1510. [Google Scholar] [CrossRef] [Green Version]
- Holmberg, L.; Garmo, H.; Granstrand, B.; Ringberg, A.; Arnesson, L.G.; Sandelin, K.; Karlsson, P.; Anderson, H.; Emdin, S. Absolute Risk Reductions for Local Recurrence After Postoperative Radiotherapy After Sector Resection for Ductal Carcinoma In Situ of the Breast. J. Clin. Oncol. 2008, 26, 1247–1252. [Google Scholar] [CrossRef]
- Vicini, F.A.; Kestin, L.L.; Goldstein, N.S.; Chen, P.Y.; Pettinga, J.; Frazier, R.C.; Martinez, A.A. Impact of Young Age on Outcome in Patients With Ductal Carcinoma-In-Situ Treated With Breast-Conserving Therapy. J. Clin. Oncol. 2000, 18, 296. [Google Scholar] [CrossRef]
- Kerlikowske, K.; Molinaro, A.; Cha, I.; Ljung, B.M.; Ernster, V.L.; Stewart, K.; Chew, K.; Moore, H.; Waldman, F. Characteristics Associated with Recurrence among Women with Ductal Carcinoma In Situ Treated by Lumpectomy. JNCI Cancer Spectr. 2003, 95, 1692–1702. [Google Scholar] [CrossRef] [Green Version]
- Wang, S.Y.; Shamliyan, T.; Virnig, B.A.; Kane, R. Tumor characteristics as predictors of local recurrence after treatment of ductal carcinoma in situ: A meta-analysis. Breast Cancer Res. Treat. 2011, 127, 1–14. [Google Scholar] [CrossRef]
- Pinder, S.E.; Duggan, C.; Ellis, I.O.; Cuzick, J.; Forbes, J.F.; Bishop, H.; Fentiman, I.S.; George, W.D.; on Behalf of the UK Coordinating Committee on Cancer Research (UKCCCR) Ductal Carcinoma In Situ (DCIS) Working Party. A new pathological system for grading DCIS with improved prediction of local recurrence: Results from the UKCCCR/ANZ DCIS trial. Br. J. Cancer 2010, 103, 94–100. [Google Scholar] [CrossRef] [Green Version]
- Nofech-Mozes, S.; Spayne, J.; Rakovitch, E.; Hanna, W.; Nofech-Mozes, S.; Spayne, J.; Rakovitch, E.; Hanna, W. Prognostic and predictive molecular markers in DCIS: A review. Adv. Anat. Pathol. 2005, 12, 256–264. [Google Scholar] [PubMed]
- Rakovitch, E.; Nofech-Mozes, S.; Narod, S.A.; Hanna, W.; Thiruchelvam, D.; Saskin, R.; Taylor, C.; Tuck, A.; Sengupta, S.; Elavathil, L.; et al. Can we select individuals with low risk ductal carcinoma in situ (DCIS)? A population-based outcomes analysis. Breast Cancer Res. Treat. 2013, 138, 581–590. [Google Scholar] [CrossRef] [PubMed]
- Cutuli, B.; Cohen-Solal-le Nir, C.; de Lafontan, B.; Mignotte, H.; Fichet, V.; Fay, R.; Servent, V.; Giard, S.; Charra-Brunaud, C.; Lemanski, C.; et al. Breast-conserving therapy for ductal carcinoma in situ of the breast: The French Cancer Centers’ experience. Int. J. Radiat Oncol. Biol. Phys. 2002, 53, 868–879. [Google Scholar] [CrossRef] [PubMed]
- Solin, L.J.; Fourquet, A.; Vicini, F.A.; Taylor, M.; Olivotto, I.A.; Haffty, B.; Strom, E.A.; Pierce, L.J.; Marks, L.B.; Bartelink, H.; et al. Long-term outcome after breast-conservation treatment with radiation for mammographically detected ductal carcinoma in situ of the breast. Cancer 2005, 103, 1137–1146. [Google Scholar] [CrossRef] [PubMed]
- Solin, L.J.; Gray, R.; Hughes, L.L.; Wood, W.C.; Lowen, M.A.; Badve, S.S.; Baehner, F.L.; Ingle, J.N.; Perez, E.A.; Recht, A.; et al. Surgical Excision without Radiation for Ductal Carcinoma in Situ of the Breast: 12-Year Results from the ECOG-ACRIN E5194 Study. J. Clin. Oncol. 2015, 33, 3938–3944. [Google Scholar] [CrossRef] [Green Version]
- Wong, J.S.; Kaelin, C.M.; Troyan, S.L.; Gadd, M.A.; Gelman, R.; Lester, S.C.; Schnitt, S.J.; Sgroi, D.C.; Silver, B.J.; Harris, J.R.; et al. Prospective Study of Wide Excision Alone for Ductal Carcinoma in Situ of the Breast. J. Clin. Oncol. 2006, 24, 1031–1036. [Google Scholar] [CrossRef] [Green Version]
- McCormick, B. RTOG 9804: A prospective randomized trial for “good risk” ductal carcinoma in situ (DCIS), comparing radiation (RT) to observation (OBS). J. Clin. Oncol. 2012, 30, 1004. [Google Scholar] [CrossRef]
- McCormick, B.; Winter, K.A.; Woodward, W.; Kuerer, H.M.; Sneige, N.; Rakovitch, E.; Smith, B.L.; Germain, I.; Hartford, A.C.; O’Rourke, M.A.; et al. Randomized Phase III Trial Evaluating Radiation Following Surgical Excision for Good-Risk Ductal Carcinoma In Situ: Long-Term Report from NRG Oncology/RTOG 9804. J. Clin. Oncol. 2021, 39, 3574–3582. [Google Scholar] [CrossRef] [PubMed]
- Gradishar, W.J.; Anderson, B.O.; Balassanian, R.; Blair, S.L.; Burstein, H.J.; Cyr, A.; Elias, A.D.; Farrar, W.B.; Forero, A.; Giordano, S.H.; et al. Breast Cancer, Version 4.2017, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Canc. Netw. 2018, 16, 310–320. [Google Scholar] [CrossRef]
- Worni, M.; Akushevich, I.; Greenup, R.; Sarma, D.; Ryser, M.D.; Myers, E.R.; Hwang, E.S. Trends in Treatment Patterns and Outcomes for Ductal Carcinoma In Situ. J. Natl. Cancer Inst. 2015, 107, djv263. [Google Scholar] [CrossRef] [Green Version]
- Rakovitch, E.; Pignol, J.P.; Hanna, W.; Kahn, H.J.; Wong, J.; Mai, V.; Paszat, L. The management of ductal carcinoma in situ of the breast: A screened population-based analysis. Breast Cancer Res. Treat. 2007, 101, 335–347. [Google Scholar] [CrossRef] [PubMed]
- Sagara, Y.; Freedman, R.A.; Wong, S.M.; Aydogan, F.; Nguyen, A.; Barry, W.T.; Golshan, M. Trends in adjuvant therapies after breast-conserving surgery for hormone receptor-positive ductal carcinoma in situ: Findings from the National Cancer Database, 2004–2013. Breast Cancer Res. Treat. 2017, 166, 583–592. [Google Scholar] [CrossRef] [PubMed]
- McCormick, B.; Winter, K.; Hudis, C.; Kuerer, H.M.; Rakovitch, E.; Smith, B.L.; Sneige, N.; Moughan, J.; Shah, A.; Germain, I.; et al. RTOG 9804: A prospective randomized trial for good-risk ductal carcinoma in situ comparing radiotherapy with observation. J. Clin. Oncol. 2015, 33, 709–715. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Allred, D.C.; Anderson, S.J.; Paik, S.; Wickerham, D.L.; Nagtegaal, I.D.; Swain, S.M.; Mamounas, E.P.; Julian, T.B.; Geyer, C.E., Jr.; Costantino, J.P.; et al. Adjuvant tamoxifen reduces subsequent breast cancer in women with estrogen receptor-positive ductal carcinoma in situ: A study based on NSABP protocol B-24. J. Clin. Oncol. 2012, 30, 1268–1273. [Google Scholar] [CrossRef] [Green Version]
- Fisher, B.; Dignam, J.; Wolmark, N.; Wickerham, D.L.; Fisher, E.R.; Mamounas, E.; Smith, R.; Begovic, M.; Dimitrov, N.V.; Margolese, R.G.; et al. Tamoxifen in treatment of intraductal breast cancer: National Surgical Adjuvant Breast and Bowel Project B-24 randomised controlled trial. Lancet 1999, 353, 1993–2000. [Google Scholar] [CrossRef]
- Staley, H.; McCallum, I.; Bruce, J. Postoperative tamoxifen for ductal carcinoma in situ. Cochrane Database Syst. Rev. 2012, 10, CD007847. [Google Scholar] [CrossRef]
- Amir, E.; Seruga, B.; Niraula, S.; Carlsson, L.; Ocana, A. Toxicity of adjuvant endocrine therapy in postmenopausal breast cancer patients: A systematic review and meta-analysis. J. Natl. Cancer Inst. 2011, 103, 1299–1309. [Google Scholar] [CrossRef] [Green Version]
- Solin, L.J.; Gray, R.; Baehner, F.L.; Butler, S.M.; Hughes, L.L.; Yoshizawa, C.; Cherbavaz, D.B.; Shak, S.; Page, D.L.; Sledge, G.W.; et al. A Multigene Expression Assay to Predict Local Recurrence Risk for Ductal Carcinoma In Situ of the Breast. J. Natl. Cancer Inst. 2013, 105, 701–710. [Google Scholar] [CrossRef] [Green Version]
- Rakovitch, E.; Nofech-Mozes, S.; Hanna, W.; Sutradhar, R.; Baehner, F.L.; Miller, D.P.; Fong, C.; Gu, S.; Tuck, A.; Sengupta, S.; et al. Multigene Expression Assay and Benefit of Radiotherapy After Breast Conservation in Ductal Carcinoma In Situ. J. Natl. Cancer Inst. 2017, 109, djw256. [Google Scholar] [CrossRef] [Green Version]
- Rakovitch, E.; Nofech-Mozes, S.; Hanna, W.; Baehner, F.L.; Saskin, R.; Butler, S.M.; Tuck, A.; Sengupta, S.; Elavathil, L.; Jani, P.A.; et al. A population-based validation study of the DCIS Score predicting recurrence risk in individuals treated by breast-conserving surgery alone. Breast Cancer Res. Treat. 2015, 152, 389–398. [Google Scholar] [CrossRef] [Green Version]
- Bremer, T.; Whitworth, P.; Patel, R.; Savala, J.; Barry, T.; Lyle, S.; Leesman, G.; Linke, S.P.; Jirstrom, K.; Zhou, W.; et al. A biologic signature for breast ductal carcinoma in situ to predict radiation therapy (RT) benefit and assess recurrence risk. Clin. Cancer Res. 2018, 24, 5895–5901. [Google Scholar] [CrossRef] [Green Version]
- Paik, S.; Shak, S.; Tang, G.; Kim, C.; Baker, J.; Cronin, M.; Baehner, F.L.; Walker, M.G.; Watson, D.; Park, T.; et al. A multigene assay to predict recurrence of tamoxifen-treated, node-negative breast cancer. N. Engl. J. Med. 2004, 351, 2817–2826. [Google Scholar] [CrossRef] [Green Version]
- Vicini, F.A.; Mann, G.B.; Shah, C.; Weinmann, S.; Leo, M.C.; Whitworth, P.; Rabinovitch, R.; Torres, M.A.; Margenthaler, J.A.; Dabbs, D.; et al. A Novel Biosignature Identifies Patients with DCIS with High Risk of Local Recurrence after Breast Conserving Surgery and Radiation Therapy. Int. J. Radiat Oncol. Biol. Phys. 2022, 115, 93–102. [Google Scholar] [CrossRef]
- Rakovitch, E.; Gray, R.; Baehner, F.L.; Sutradhar, R.; Crager, M.; Gu, S.; Nofech-Mozes, S.; Badve, S.S.; Hanna, W.; Hughes, L.L.; et al. Refined estimates of local recurrence risks by DCIS score adjusting for clinicopathological features: A combined analysis of ECOG-ACRIN E5194 and Ontario DCIS cohort studies. Breast Cancer Res. Treat. 2018, 169, 359–369. [Google Scholar] [CrossRef] [Green Version]
- Weinmann, S.; Leo, M.C.; Francisco, M.; Jenkins, C.L.; Barry, T.; Leesman, G.; Linke, S.P.; Whitworth, P.W.; Patel, R.; Pellicane, J.; et al. Validation of a Ductal Carcinoma In Situ Biomarker Profile for Risk of Recurrence after Breast-Conserving Surgery with and without Radiotherapy. Clin. Cancer Res. 2020, 26, 4054–4063. [Google Scholar] [CrossRef]
- Warnberg, F.; Karlsson, P.; Holmberg, E.; Sandelin, K.; Whitworth, P.W.; Savala, J.; Barry, T.; Leesman, G.; Linke, S.P.; Shivers, S.C.; et al. Prognostic Risk Assessment and Prediction of Radiotherapy Benefit for Women with Ductal Carcinoma In Situ (DCIS) of the Breast, in a Randomized Clinical Trial (SweDCIS). Cancers 2021, 13, 6103. [Google Scholar] [CrossRef]
- Sparano, J.A.; Gray, R.J.; Makower, D.F.; Pritchard, K.I.; Albain, K.S.; Hayes, D.F.; Geyer, C.E., Jr.; Dees, E.C.; Goetz, M.P.; Olson, J.A., Jr.; et al. Adjuvant Chemotherapy Guided by a 21-Gene Expression Assay in Breast Cancer. N. Engl. J. Med. 2018, 379, 111–121. [Google Scholar] [CrossRef] [Green Version]
- Sparano, J.A.; Gray, R.J.; Ravdin, P.M.; Makower, D.F.; Pritchard, K.I.; Albain, K.S.; Hayes, D.F.; Geyer, C.E., Jr.; Dees, E.C.; Goetz, M.P.; et al. Clinical and Genomic Risk to Guide the Use of Adjuvant Therapy for Breast Cancer. N. Engl. J. Med. 2019, 380, 2395–2405. [Google Scholar] [CrossRef] [PubMed]
- Rakovitch, E.; Sutradhar, R.; Nofech-Mozes, S.; Gu, S.; Fong, C.; Hanna, W.; Paszat, L. 21-Gene Assay and Breast Cancer Mortality in Ductal Carcinoma In Situ. J. Natl. Cancer Inst. 2021, 113, 572–579. [Google Scholar] [CrossRef] [PubMed]
- Iwamoto, N.; Nara, M.; Horiguchi, S.I.; Aruga, T. Surgical upstaging rates in patients meeting the eligibility for active surveillance trials. Jpn. J. Clin. Oncol. 2021, 51, 1219–1224. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Study | Design | N | Eligibility | 12 Year LR Risk | 12 Year Invasive LR Risk |
|---|---|---|---|---|---|
| ECOG-ACRIN 5194 | Prospective single arm cohort study of BCS alone | 627 | Cohort 1 (≤2.5 cm, grade 1 or 2) Cohort 2 (≤1 cm, grade 3) Resection margins > 3 mm | Cohort 1: 14.4% Cohort 2: 24.6% | Cohort 1: 7.4% Cohort 2: 13.4% |
| Boston Cohort | Prospective single arm cohort study of BCS alone | 158 | Low/intermediate grade DCIS Margins > 1 cm | 15.6% | |
| RTOG/NRG 9804 | Randomized clinical trial | 636 | Tumor size < 2.5 cm Nuclear grade 1 or 2 Margins > 3 mm 60% received tamoxifen | 15-yr risk: BCS alone: 15.1% BCS + RT: 7.1% | BCS alone: 9.5% BCS + RT: 5.4% |
| Genes | Risk Groups | Multivariable Hazard Ratio (HR) | Comments | |
|---|---|---|---|---|
| Oncotype DCIS Score [49,50,51] (Exact Sciences) | Ki67, STK15, Survivin, cyclin B1, MYBL2, PR, GSTM1 + reference genes (b-actin, GAPDH, RPLPO, GUS, TFRC) Scaled from 0–10 | Low: <39 Intermediate: 39–54 High: >55 | DS/50 = 2.1 (1.4, 3.1) Age < 50 yrs = 1.83 (1.2, 2.7) Tumor size > 10 mm = 1.7 (1.0, 2.9) Multifocality = 1.98 (1.3, 2.9) Pos. margins = 1.5 (1.0, 2.1) | Validated in E5194 and Ontario DCIS cohorts; Integration of DS improves prediction of 10 yr LR risk after BCS compared to clinical factors alone or with ER, PR, HER2 status [8]; Clinical factors contribute to LR risk prediction. |
| Decision Score [52] (Prelude DX) | Her2, Ki-67, Cox-2, SIAH2, FOXA1, p16, age, tumor size, palpability of DCIS lesion, margin status (DCISionRT) Scaled from 0–10 to produce the Decision Score | Low: ≤3 Elevated: >3 | HR for effect of RT as a function of the DS: Low Risk DS = 0.7 (0.3–1.6) High Risk DS = 0.3 (0.1–0.5) | RT benefit prediction; Clinicopathologic factors did not maintain significance; Not validated in SweDCIS randomized trial; significant interaction found with RT using threshold of 2.8. |
| Decision Score and Residual Risk subtype [53] (RRt) (Prelude DX) | Decision Score (threshold 2.8) combined with EGFR/HER2/KRAS expression | Low Risk: (DS ≤ 2.8 without RRt) Elevated Risk: (DS > 2.8 without RRt) Residual Risk: (DS > 2.8 with RRt). | 10-yr LR after BCS alone by groups: Low risk = 5.1% Elevated risk = 21% Residual risk = 42% | No benefit with RT in low-risk group; 10 yr LR risk after BCS + RT: Elevated risk = 4.9% Residual risk = 14.7% |
| 10-Year Risk of Local Recurrence (%) a (Range b) by DCIS Score Group | ||||
|---|---|---|---|---|
| Tumor Size (cm) | Age (yr) | Low DCIS Score (0–38) | Intermediate DCIS Score (39–54) | High DCIS Score (55–100) |
| ≤1 | ≥50 | 7.2 (5.3–10.0) | 11.3 (10.2–12.7) | 14.6 (12.9–23.1) |
| <50 | 10.2 (7.4–13.9) | 15.8 (14.1–17.4) | 19.6 (17.7–30.7) | |
| 1.1–2.5 | ≥50 | 10.1 (7.3–12.6) | 13.9 (12.8–15.6) | 19.5 (15.8–28.7) |
| <50 | 14.5 (10.1–17.2) | 18.9 (17.4–21.1) | 23.2 (21.4–37.2) | |
| >2.5 | ≥50 | 20.4 (14.9–27.0) | 29.1 (27.4–33.3) | 41.1 (33.8–54.4) |
| <50 | 30.2 (20.6–36.1) | 39.5 (36.6–43.6) | 48.6 (44.1–66.5) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hahn, E.; Rodin, D.; Sutradhar, R.; Nofech-Mozes, S.; Trebinjac, S.; Paszat, L.F.; Rakovitch, E. Can Molecular Biomarkers Help Reduce the Overtreatment of DCIS? Curr. Oncol. 2023, 30, 5795-5806. https://doi.org/10.3390/curroncol30060433
Hahn E, Rodin D, Sutradhar R, Nofech-Mozes S, Trebinjac S, Paszat LF, Rakovitch E. Can Molecular Biomarkers Help Reduce the Overtreatment of DCIS? Current Oncology. 2023; 30(6):5795-5806. https://doi.org/10.3390/curroncol30060433
Chicago/Turabian StyleHahn, Ezra, Danielle Rodin, Rinku Sutradhar, Sharon Nofech-Mozes, Sabina Trebinjac, Lawrence Frank Paszat, and Eileen Rakovitch. 2023. "Can Molecular Biomarkers Help Reduce the Overtreatment of DCIS?" Current Oncology 30, no. 6: 5795-5806. https://doi.org/10.3390/curroncol30060433
APA StyleHahn, E., Rodin, D., Sutradhar, R., Nofech-Mozes, S., Trebinjac, S., Paszat, L. F., & Rakovitch, E. (2023). Can Molecular Biomarkers Help Reduce the Overtreatment of DCIS? Current Oncology, 30(6), 5795-5806. https://doi.org/10.3390/curroncol30060433