Prognostic Impact of Histologic Subtype and Divergent Differentiation in Patients with Metastatic Urothelial Carcinoma Treated with Enfortumab Vedotin: A Multicenter Retrospective Study

Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Population
2.2. Patient Management
2.3. Evaluation
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
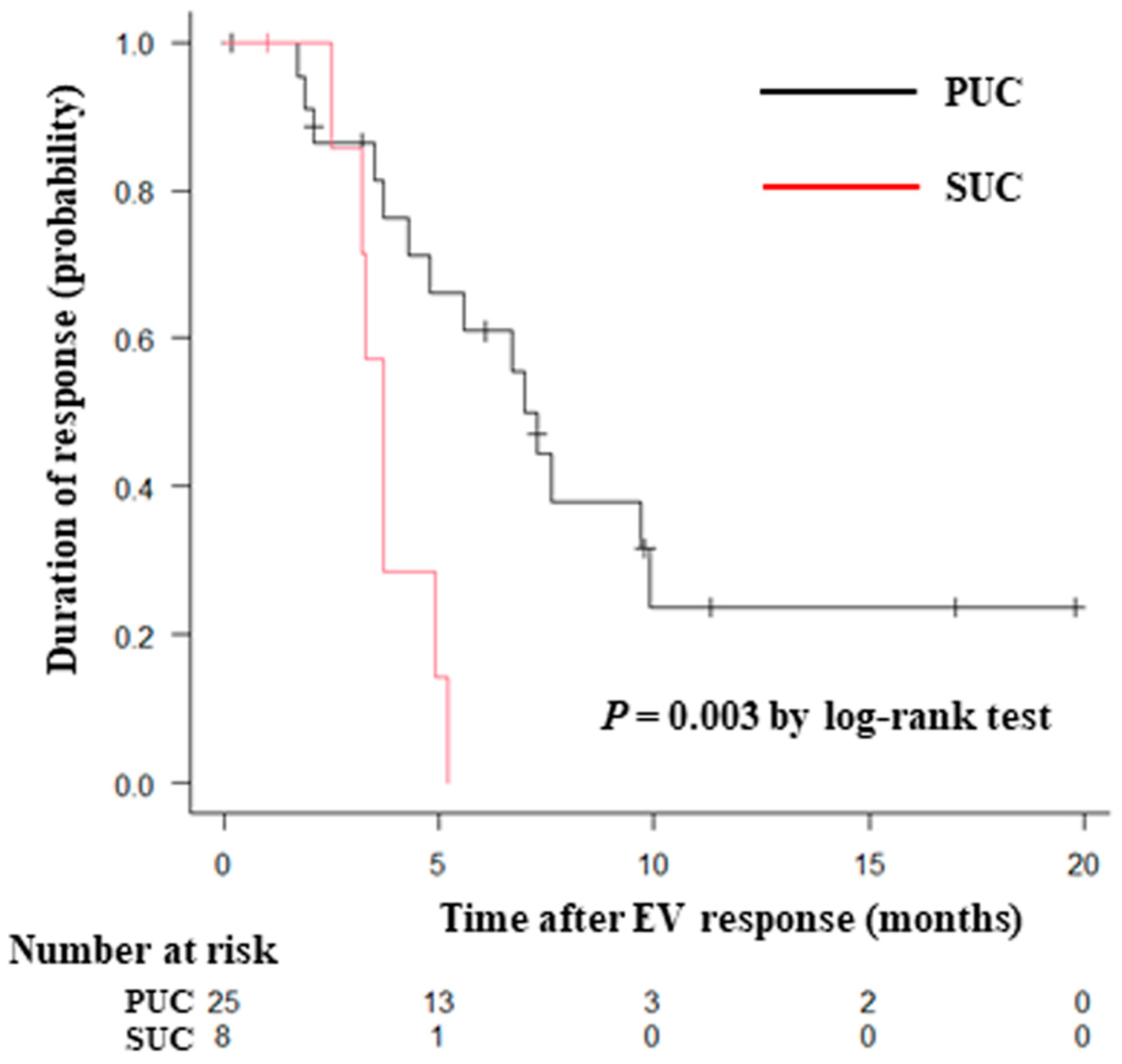
3.2. Response
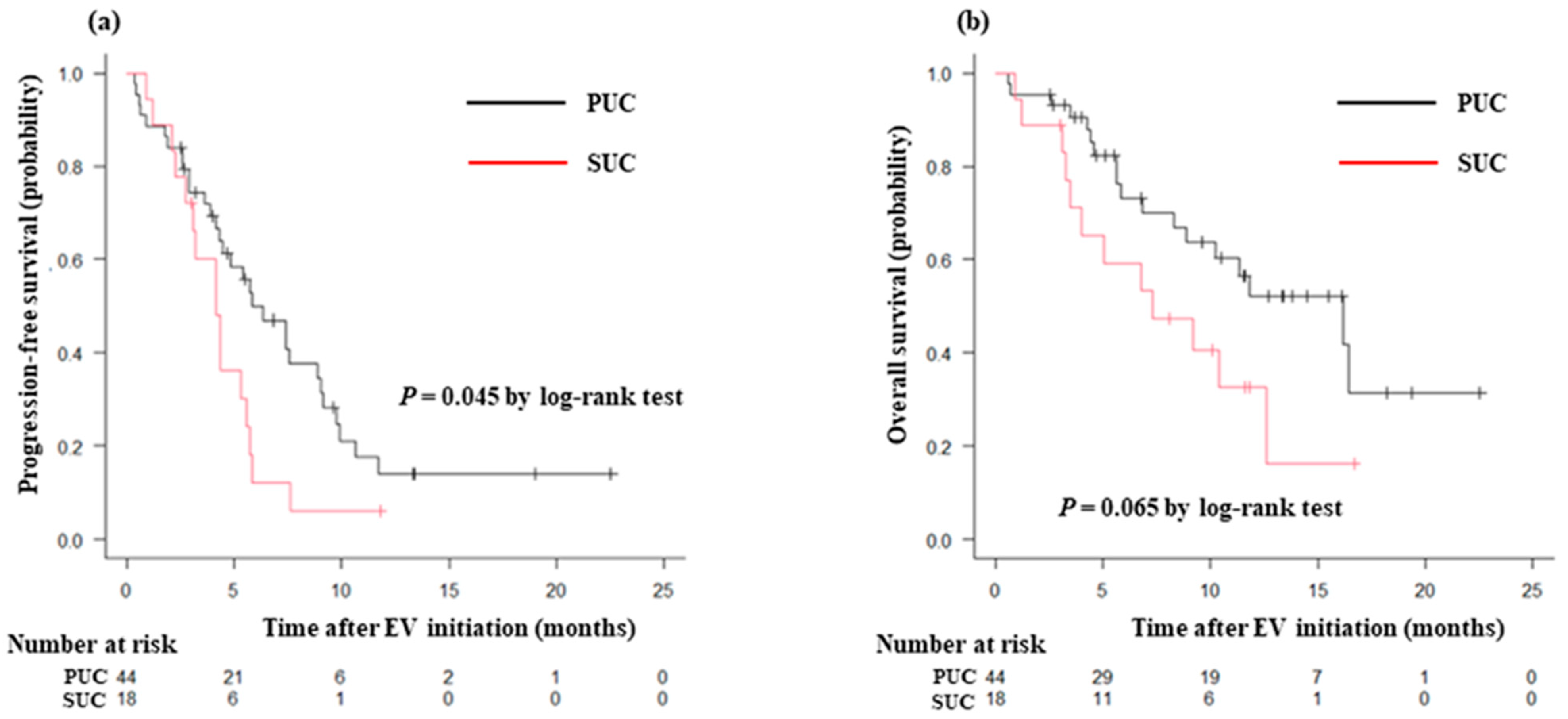
3.3. Survival
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Bajorin, D.F.; Witjes, J.A.; Gschwend, J.E.; Schenker, M.; Valderrama, B.P.; Tomita, Y.; Bamias, A.; Lebret, T.; Shariat, S.F.; Park, S.H.; et al. Adjuvant nivolumab versus placebo in muscle-invasive urothelial carcinoma. N. Engl. J. Med. 2021, 384, 2102–2114. [Google Scholar] [CrossRef]
- Powles, T.; Park, S.H.; Voog, E.; Caserta, C.; Valderrama, B.P.; Gurney, H.; Kalofonos, H.; Radulović, S.; Demey, W.; Ullén, A.; et al. Avelumab maintenance therapy for advanced or metastatic urothelial carcinoma. N. Engl. J. Med. 2020, 383, 1218–1230. [Google Scholar] [CrossRef] [PubMed]
- Bellmunt, J.; de Wit, R.; Vaughn, D.J.; Fradet, Y.; Lee, J.L.; Fong, L.; Vogelzang, N.J.; Climent, M.A.; Petrylak, D.P.; Choueiri, T.K.; et al. Pembrolizumab as second-line therapy for advanced urothelial carcinoma. N. Engl. J. Med. 2017, 376, 1015–1026. [Google Scholar] [CrossRef]
- Powles, T.; Rosenberg, J.E.; Sonpavde, G.P.; Loriot, Y.; Durán, I.; Lee, J.L.; Matsubara, N.; Vulsteke, C.; Castellano, D.; Wu, C.; et al. Enfortumab vedotin in previously treated advanced urothelial carcinoma. N. Engl. J. Med. 2021, 384, 1125–1135. [Google Scholar] [CrossRef] [PubMed]
- Minato, A.; Kimuro, R.; Ohno, D.; Tanigawa, K.; Kuretake, K.; Matsukawa, T.; Takaba, T.; Jojima, K.; Harada, M.; Higashijima, K.; et al. Efficacy and tolerability of enfortumab vedotin for metastatic urothelial carcinoma: Early experience in the real world. Anticancer Res. 2023, 43, 4055–4060. [Google Scholar] [CrossRef]
- Mantica, G.; Simonato, A.; Du Plessis, D.E.; Maffezzini, M.; De Rose, A.F.; van der Merwe, A.; Terrone, C. The pathologist’s role in the detection of rare variants of bladder cancer and analysis of the impact on incidence and type detection. Minerva Urol. Nefrol. 2018, 70, 594–597. [Google Scholar] [CrossRef] [PubMed]
- Netto, G.J.; Amin, M.B.; Berney, D.M.; Compérat, E.M.; Gill, A.J.; Hartmann, A.; Menon, S.; Raspollini, M.R.; Rubin, M.A.; Srigley, J.R.; et al. The 2022 World Health Organization classification of tumors of the urinary system and male genital organs-part B: Prostate and urinary tract tumors. Eur. Urol. 2022, 82, 469–482. [Google Scholar] [CrossRef]
- Minato, A.; Murooka, K.; Okumura, Y.; Takaba, T.; Higashijima, K.; Nagata, Y.; Tomisaki, I.; Harada, K.; Fujimoto, N. Efficacy of platinum-based chemotherapy in patients with metastatic urothelial carcinoma with variant histology. In Vivo, 2024, in press.
- Lobo, N.; Shariat, S.F.; Guo, C.C.; Fernandez, M.I.; Kassouf, W.; Choudhury, A.; Gao, J.; Williams, S.B.; Galsky, M.D.; Taylor, J.A.; et al. What is the significance of variant histology in urothelial carcinoma? Eur. Urol. Focus 2020, 6, 653–663. [Google Scholar] [CrossRef]
- Mori, K.; Abufaraj, M.; Mostafaei, H.; Quhal, F.; Karakiewicz, P.I.; Briganti, A.; Kimura, S.; Egawa, S.; Shariat, S.F. A systematic review and meta-analysis of variant histology in urothelial carcinoma of the bladder treated with radical cystectomy. J. Urol. 2020, 204, 1129–1140. [Google Scholar] [CrossRef] [PubMed]
- Mori, K.; Janisch, F.; Parizi, M.K.; Mostafaei, H.; Lysenko, I.; Kimura, S.; Enikeev, D.V.; Egawa, S.; Shariat, S.F. Prognostic value of variant histology in upper tract urothelial carcinoma treated with nephroureterectomy: A systematic review and meta-analysis. J. Urol. 2020, 203, 1075–1084. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, M.C.; Sung, M.T.; Chiang, P.H.; Huang, C.H.; Tang, Y.; Su, Y.L. The prognostic impact of histopathological variants in patients with advanced urothelial carcinoma. PLoS ONE 2015, 10, e0129268. [Google Scholar] [CrossRef] [PubMed]
- Minato, A.; Furubayashi, N.; Harada, M.; Negishi, T.; Sakamoto, N.; Song, Y.; Hori, Y.; Tomoda, T.; Tamura, S.; Kuroiwa, K.; et al. Efficacy of pembrolizumab in patients with variant urothelial carcinoma: A multicenter retrospective study. Clin. Genitourin. Cancer 2022, 20, 499.e1–499.e8. [Google Scholar] [CrossRef] [PubMed]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline, version 1.1. Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef] [PubMed]
- Kanda, Y. Investigation of the freely available easy-to-use software “EZR” for medical statistics. Bone Marrow Transpl. 2013, 48, 452–458. [Google Scholar] [CrossRef] [PubMed]
- Swami, U.; Grivas, P.; Pal, S.K.; Agarwal, N. Utilization of systemic therapy for treatment of advanced urothelial carcinoma: Lessons from real world experience. Cancer Treat. Res. Commun. 2021, 27, 100325. [Google Scholar] [CrossRef]
- Koshkin, V.S.; Henderson, N.; James, M.; Natesan, D.; Freeman, D.; Nizam, A.; Su, C.T.; Khaki, A.R.; Osterman, C.K.; Glover, M.J.; et al. Efficacy of enfortumab vedotin in advanced urothelial cancer: Analysis from the urothelial cancer network to investigate therapeutic experiences (UNITE) study. Cancer 2022, 128, 1194–1205. [Google Scholar] [CrossRef]
- Rosenberg, J.E.; O’Donnell, P.H.; Balar, A.V.; McGregor, B.A.; Heath, E.I.; Yu, E.Y.; Galsky, M.D.; Hahn, N.M.; Gartner, E.M.; Pinelli, J.M.; et al. Pivotal trial of enfortumab vedotin in urothelial carcinoma after platinum and anti-programmed death 1/programmed death ligand 1 therapy. J. Clin. Oncol. 2019, 37, 2592–2600. [Google Scholar] [CrossRef]
- Zschäbitz, S.; Biernath, N.; Hilser, T.; Höllein, A.; Zengerling, F.; Cascucelli, J.; Paffenholz, P.; Seidl, D.; Lutz, C.; Schlack, K.; et al. Enfortumab vedotin in metastatic urothelial carcinoma: Survival and safety in a European multicenter real-world patient cohort. Eur. Urol. Open Sci. 2023, 53, 31–37. [Google Scholar] [CrossRef] [PubMed]
- Hoffman-Censits, J.H.; Lombardo, K.A.; Parimi, V.; Kamanda, S.; Choi, W.; Hahn, N.M.; McConkey, D.J.; McGuire, B.M.; Bivalacqua, T.J.; Kates, M.; et al. Expression of Nectin-4 in bladder urothelial carcinoma, in morphologic variants, and nonurothelial histotypes. Appl. Immunohistochem. Mol. Morphol. 2021, 29, 619–625. [Google Scholar] [CrossRef]
- Chu, C.E.; Sjöström, M.; Egusa, E.A.; Gibb, E.A.; Badura, M.L.; Zhu, J.; Koshkin, V.S.; Stohr, B.A.; Meng, M.V.; Pruthi, R.S.; et al. Heterogeneity in NECTIN4 expression across molecular subtypes of urothelial cancer mediates sensitivity to enfortumab vedotin. Clin. Cancer Res. 2021, 27, 5123–5130. [Google Scholar] [CrossRef] [PubMed]
- Klümper, N.; Ralser, D.J.; Ellinger, J.; Roghmann, F.; Albrecht, J.; Below, E.; Alajati, A.; Sikic, D.; Breyer, J.; Bolenz, C.; et al. Membranous NECTIN-4 expression frequently decreases during metastatic spread of urothelial carcinoma and is associated with enfortumab vedotin resistance. Clin. Cancer Res. 2023, 29, 1496–1505. [Google Scholar] [CrossRef] [PubMed]
- Fan, Y.; Li, Q.; Shen, Q.; Liu, Z.; Zhang, Z.; Hu, S.; Yu, W.; He, Z.; He, Q.; Zhang, Q. Head-to-head comparison of the expression differences of nectin-4, TROP-2, and HER2 in urothelial carcinoma and its histologic variants. Front. Oncol. 2022, 12, 858865. [Google Scholar] [CrossRef] [PubMed]
- Rodler, S.; Eismann, L.; Schlenker, B.; Casuscelli, J.; Brinkmann, I.; Sendelhofert, A.; Waidelich, R.; Buchner, A.; Stief, C.; Schulz, G.B.; et al. Expression of nectin-4 in variant histologies of bladder cancer and its prognostic value-need for biomarker testing in high-risk patients? Cancers 2022, 14, 4411. [Google Scholar] [CrossRef] [PubMed]
- Ghali, F.; Vakar-Lopez, F.; Roudier, M.P.; Garcia, J.; Arora, S.; Cheng, H.H.; Schweizer, M.T.; Haffner, M.C.; Lee, J.K.; Yu, E.Y.; et al. Metastatic bladder cancer expression and subcellular localization of Nectin-4 and Trop-2 in variant histology: A rapid autopsy study. Clin. Genitourin. Cancer 2023, 21, 669–678. [Google Scholar] [CrossRef] [PubMed]
- Rosenberg, J.E.; Powles, T.; Sonpavde, G.P.; Loriot, Y.; Duran, I.; Lee, J.L.; Matsubara, N.; Vulsteke, C.; Castellano, D.; Mamtani, R.; et al. EV-301 long-term outcomes: 24-month findings from the phase III trial of enfortumab vedotin versus chemotherapy in patients with previously treated advanced urothelial carcinoma. Ann. Oncol. 2023, 34, 1047–1054. [Google Scholar] [CrossRef] [PubMed]
- Paciotti, M.; Nguyen, D.D.; Modonutti, D.; Haeuser, L.; Lipsitz, S.; Mossanen, M.; Kibel, A.S.; Lughezzani, G.; Trinh, Q.D.; Cole, A.P. Impact of high-intensity local treatment on overall survival in stage IV upper tract urothelial carcinoma. Urol. Oncol. 2021, 39, 436.e1–436.e10. [Google Scholar] [CrossRef]
- Seisen, T.; Sun, M.; Leow, J.J.; Preston, M.A.; Cole, A.P.; Gelpi-Hammerschmidt, F.; Hanna, N.; Meyer, C.P.; Kibel, A.S.; Lipsitz, S.R.; et al. Efficacy of high-intensity local treatment for metastatic urothelial carcinoma of the bladder: A propensity score-weighted analysis from the national cancer data base. J. Clin. Oncol. 2016, 34, 3529–3536. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Histologic Type | Number of Patients (%) | Primary Tumor Site Lower/Upper Urinary Tract |
|---|---|---|
| PUC | 44 (71) | 20/24 |
| SUC | 18 (29) | 12/6 |
| SUC subgroup | ||
| Squamous differentiation | 10 (16.1) | 6/4 |
| Glandular differentiation | 4 (6.5) | 4/0 |
| Sarcomatoid subtype | 2 (3.2) | 0/2 |
| Plasmacytoid subtype | 1 (1.6) | 1/0 |
| Neuroendocrine differentiation | 1 (1.6) | 1/0 |
| PUC (n = 44) | SUC (n = 18) | p Value | |
|---|---|---|---|
| Age, median (IQR) | 73 (68–76) | 73 (71–79) | 0.415 |
| Sex, n (%) | 0.355 | ||
| Male | 31 (70.5) | 15 (83.3) | |
| Female | 13 (29.5) | 3 (16.7) | |
| ECOG-PS score, n (%) | 0.667 | ||
| 0 | 19 (43.2) | 7 (38.9) | |
| 1 | 18 (40.9) | 8 (44.4) | |
| 2 | 4 (9.1) | 3 (16.7) | |
| 3 | 3 (6.8) | 0 (0) | |
| Primary tumor site, n (%) | 0.166 | ||
| Lower urinary tract | 20 (45.5) | 12 (66.7) | |
| Upper urinary tract | 24 (54.5) | 6 (33.3) | |
| Histologic diagnosis, n (%) | 0.412 | ||
| Prior radical surgery | 24 (54.5) | 12 (66.7) | |
| Biopsy | 20 (45.5) | 6 (33.3) | |
| Anemia (Hb < 10 g/dL), n (%) | 14 (31.8) | 7 (38.9) | 0.768 |
| Liver metastasis, n (%) | 9 (20.5) | 4 (22.2) | 1.00 |
| Number of prior lines of therapy, n (%) | 0.842 | ||
| 2 | 32 (72.7) | 13 (72.2) | |
| ≥3 | 12 (27.3) | 5 (27.8) | |
| Prior immune checkpoint blockade, n (%) | 1.00 | ||
| Anti-PD-1 | 28 (63.6) | 11 (61.1) | |
| Anti-PD-L1 | 16 (36.4) | 7 (38.9) | |
| EV cycles, median (IQR) | 4 (3–7) | 4 (2–7) | 0.365 |
| PUC (n = 44) | SUC (n = 18) | p Value | |
|---|---|---|---|
| Response, n (%) | 0.475 | ||
| CR | 3 (6.8) | 0 (0) | |
| PR | 22 (50.0) | 8 (44.4) | |
| SD | 10 (22.7) | 3 (16.7) | |
| PD | 9 (20.5) | 7 (38.9) | |
| Objective response rate (CR + PR), n (%) | 25 (56.8) | 8 (44.4) | 0.413 |
| Disease control rate (CR + PR + SD), n (%) | 35 (79.5) | 11 (61.1) | 0.20 |
| Variable | Univariate | Multivariate | ||
|---|---|---|---|---|
| HR (95% CI) | p Value | HR (95% CI) | p Value | |
| Age, years | ||||
| <73 | 1 | |||
| ≥73 | 1.21 (0.67–2.16) | 0.529 | ||
| Sex | ||||
| Male | 1 | |||
| Female | 0.97 (0.49–1.91) | 0.932 | ||
| ECOG-PS score | ||||
| 0 | 1 | 1 | ||
| 1 | 1.35 (0.71–2.59) | 0.361 | 1.27 (0.66–2.45) | 0.467 |
| 2 | 2.01 (0.83–4.86) | 0.123 | 1.73 (0.70–4.25) | 0.233 |
| 3 | 3.77 (1.08–13.2) | 0.038 | 4.54 (1.27–16.2) | 0.019 |
| Primary tumor site | ||||
| Lower urinary tract | 1 | |||
| Upper urinary tract | 0.83 (0.47–1.48) | 0.527 | ||
| Prior radical surgery | ||||
| No | 1 | |||
| Yes | 0.69 (0.38–1.22) | 0.201 | ||
| Anemia | ||||
| No | 1 | |||
| Yes | 1.54 (0.83–2.84) | 0.169 | ||
| Liver metastasis | ||||
| No | 1 | |||
| Yes | 1.50 (0.75–2.99) | 0.252 | ||
| Prior immune checkpoint blockade | ||||
| Anti-PD-1 | 1 | |||
| Anti-PD-L1 | 0.67 (0.36–1.23) | 0.193 | ||
| Histologic type | ||||
| PUC | 1 | 1 | ||
| SUC | 1.86 (1.01–3.45) | 0.049 | 1.90 (1.01–3.61) | 0.048 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Minato, A.; Furubayashi, N.; Nagata, Y.; Tomoda, T.; Masaoka, H.; Song, Y.; Hori, Y.; Kiyoshima, K.; Negishi, T.; Kuroiwa, K.; et al. Prognostic Impact of Histologic Subtype and Divergent Differentiation in Patients with Metastatic Urothelial Carcinoma Treated with Enfortumab Vedotin: A Multicenter Retrospective Study. Curr. Oncol. 2024, 31, 862-871. https://doi.org/10.3390/curroncol31020064
Minato A, Furubayashi N, Nagata Y, Tomoda T, Masaoka H, Song Y, Hori Y, Kiyoshima K, Negishi T, Kuroiwa K, et al. Prognostic Impact of Histologic Subtype and Divergent Differentiation in Patients with Metastatic Urothelial Carcinoma Treated with Enfortumab Vedotin: A Multicenter Retrospective Study. Current Oncology. 2024; 31(2):862-871. https://doi.org/10.3390/curroncol31020064
Chicago/Turabian StyleMinato, Akinori, Nobuki Furubayashi, Yujiro Nagata, Toshihisa Tomoda, Hiroyuki Masaoka, Yoohyun Song, Yoshifumi Hori, Keijiro Kiyoshima, Takahito Negishi, Kentaro Kuroiwa, and et al. 2024. "Prognostic Impact of Histologic Subtype and Divergent Differentiation in Patients with Metastatic Urothelial Carcinoma Treated with Enfortumab Vedotin: A Multicenter Retrospective Study" Current Oncology 31, no. 2: 862-871. https://doi.org/10.3390/curroncol31020064
APA StyleMinato, A., Furubayashi, N., Nagata, Y., Tomoda, T., Masaoka, H., Song, Y., Hori, Y., Kiyoshima, K., Negishi, T., Kuroiwa, K., Seki, N., Tomisaki, I., Harada, K., Nakamura, M., & Fujimoto, N. (2024). Prognostic Impact of Histologic Subtype and Divergent Differentiation in Patients with Metastatic Urothelial Carcinoma Treated with Enfortumab Vedotin: A Multicenter Retrospective Study. Current Oncology, 31(2), 862-871. https://doi.org/10.3390/curroncol31020064