Electromagnetic Transmitter-Based Prostate Gating for Dose-Escalated Linac-Based Stereotactic Body Radiation Therapy: An Evaluation of Intrafraction Motion

Abstract
:1. Introduction
2. Material and Methods
2.1. Patient Setup and Treatment Planning
- PTV1: Whole prostate +/− distal 1.5 cm of seminal vesicles (only in ISUP 3–5 patients [18]) +2 mm;
- PTV2: GTV(s) defined through MRI of +2 mm.
- Rectum—V27 Gy < 20 cc, V13.5 < 30%, V6.7 Gy < 60% and max dose 40.5 Gy;
- Bladder—V19 Gy < 15 cc, V10.6 Gy < 30%;
- Urethra—V39 Gy < 1 cc and V41 Gy < 0.1 cc;
- Femoral heads—30 Gy < 10 cc.
2.2. Intrafraction Motion Tracking and Intervention Protocol
2.3. Data Acquisition, Processing, and Analysis
2.4. Data about Treatment Duration
- Per-patient, realized including all the 5 delivered sessions of the total treatment;
- Per-fraction, including all the patients, in order to determine whether there is a possible influence of the session number on treatment duration;
- Per-session, including data on all the sessions and on all the patients.
3. Results
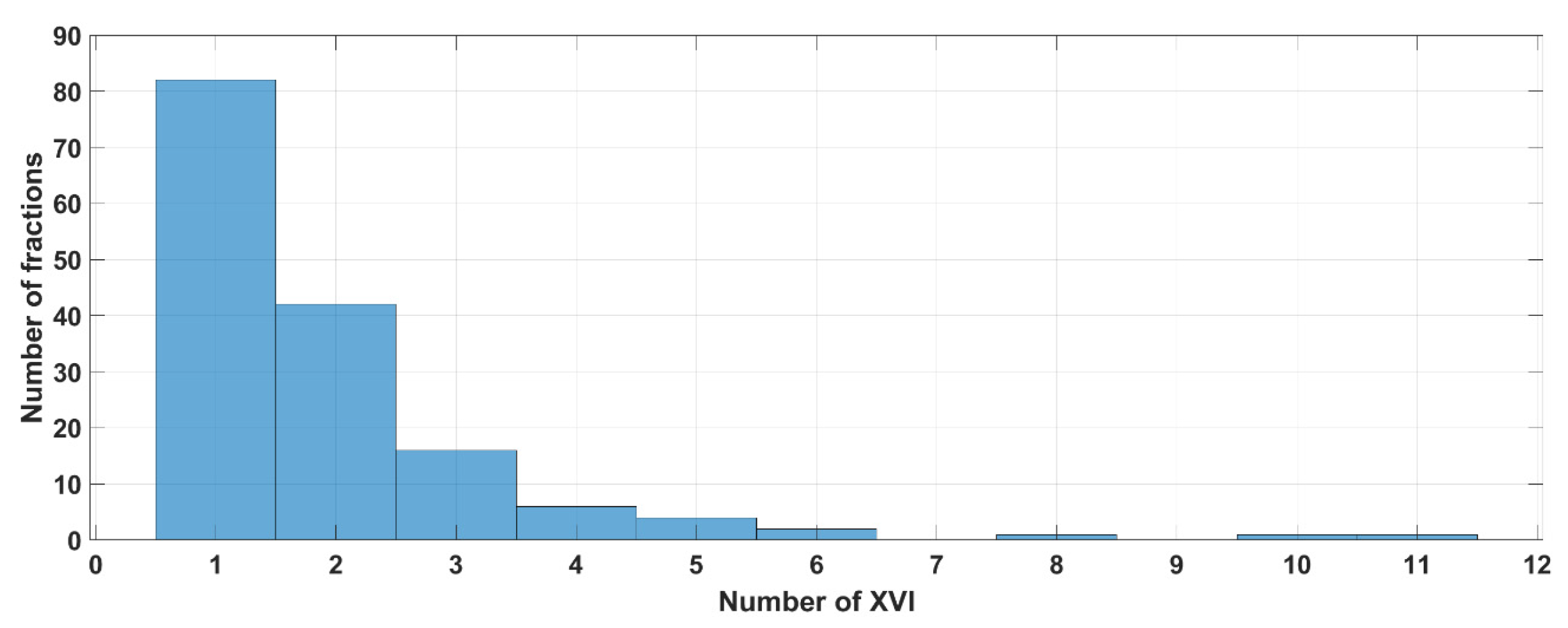
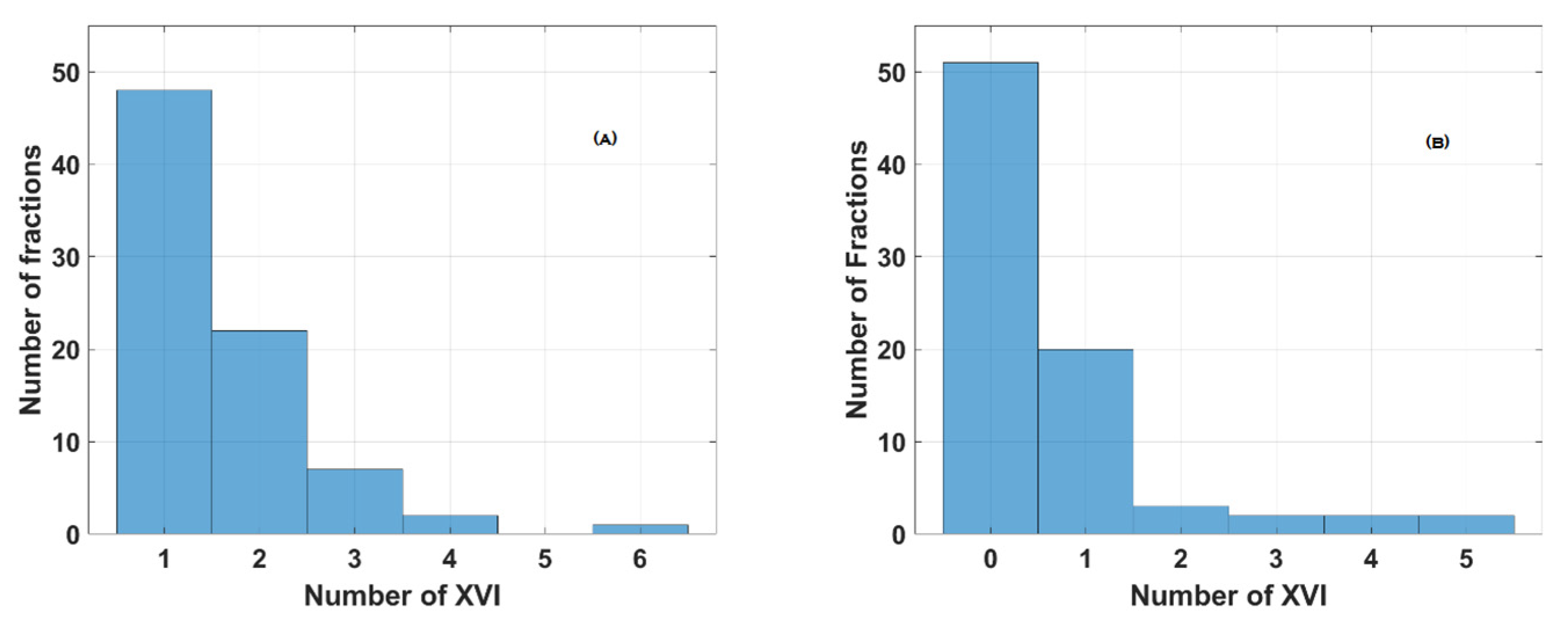
3.1. Data about XVI CBCT Acquisition
3.2. Results of the Per-Patient Analysis
- Group A (3 patients, 15 sessions)—only one setup control was performed and needed before the beginning of the treatment, without any other setup verification required during either the setup phase or the delivery phase.
- Group B (15 patients, 75 sessions)—at least one setup control was performed and needed before the beginning of the treatment. No other setup controls were needed during the delivery phase. This group encompasses Group A.
- Group C (16 patients, 80 sessions)—at least one supplementary setup control was performed and needed during the delivery of the treatment. No other setup controls were needed during the setup phase.
3.3. Results of the Per-Session Analysis
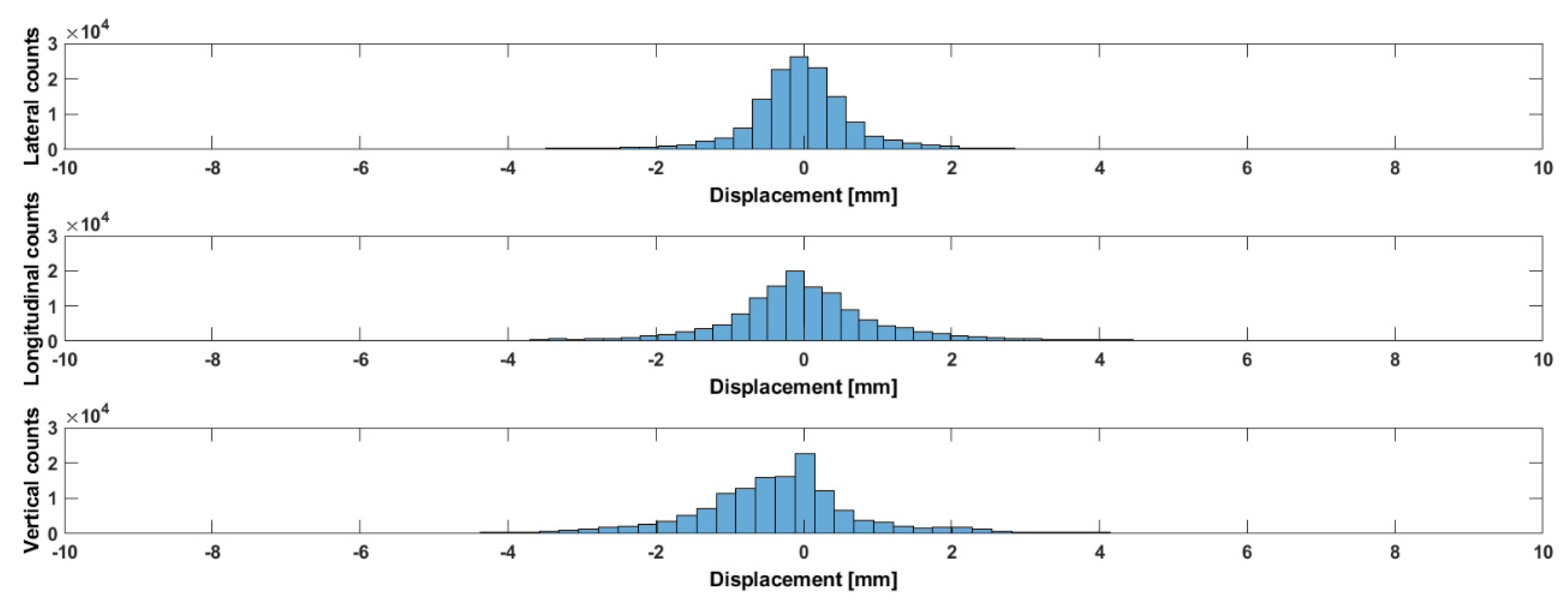
3.4. Prostate Displacements (% of Time Outside the CTV-to-PTV Margin of 2 mm)
3.5. Results of the Per-Fraction Analysis
3.6. Clinical Compliance
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Miralbell, R.; Roberts, S.A.; Zubizarreta, E.; Hendry, J.H. Dose-Fractionation Sensitivity of Prostate Cancer Deduced From Radiotherapy Outcomes of 5969 Patients in Seven International Institutional Datasets: A/b = 1.4 (0.9 − 2.2)Gy. Int. J. Radiat. Oncol. Biol. Phys. 2012, 82, e17–e24. [Google Scholar] [CrossRef] [PubMed]
- Dasu, A.; Toma-Dasu, I. Prostate a/b Revisited—An Analysis of Clinical Results from 14168 Patients. Acta Oncol. 2012, 51, 963–974. [Google Scholar] [CrossRef] [PubMed]
- Proust-Lima, C.; Taylor, J.M.; Sécher, S.; Sandler, H.; Kestin, L.; Pickles, T.; Bae, K.; Allison, R.; Williams, S. Confirmation of a Low a/b Ratio for Prostate Cancer Treated by External Beam Radiation Therapy Alone Using a Post-Treatment Repeated-Measures Model for PSA Dynamics. Int. J. Radiat. Oncol. Biol. Phys. 2011, 79, 195–201. [Google Scholar] [CrossRef] [PubMed]
- De Bari, B.; Arcangeli, S.; Ciardo, D.; Mazzola, R.; Alongi, F.; Russi, E.G.; Santoni, R.; Magrini, S.M.; Jereczek-Fossa, B.A.; on the behalf of the Italian Association of Radiation Oncology (AIRO). Extreme hypofractionation for early prostate cancer: Biology meets technology. Cancer Treat. Rev. 2016, 50, 48–60. [Google Scholar] [CrossRef] [PubMed]
- De Bari, B.; Fiorentino, A.; Arcangeli, S.; Franco, P.; D’Angelillo, R.M.; Alongi, F. From radiobiology to technology: What is changing in radiotherapy for prostate cancer. Expert Rev. Anticancer Ther. 2014, 14, 553–564. [Google Scholar] [CrossRef]
- Arcangeli, S.; Scorsetti, M.; Alongi, F. Will SBRT Replace Conventional Radiotherapy in Patients with Low-Intermediate Risk Prostate Cancer? A Review. Crit. Rev. Oncol. Hematol. 2012, 84, 101–108. [Google Scholar] [CrossRef] [PubMed]
- Morgan, S.C.; Hoffman, K.; Loblaw, D.A.; Buyyounouski, M.K.; Patton, C.; Barocas, D.; Bentzen, S.; Chang, M.; Efstathiou, J.; Greany, P.; et al. Hypofractionated Radiation Therapy for Localized Prostate Cancer: An ASTRO, ASCO, and AUA Evidence-Based Guideline. Pract. Radiat. Oncol. 2018, 8, 354–360. [Google Scholar] [CrossRef]
- Kishan, A.U.; Dang, A.; Katz, A.J.; Mantz, C.A.; Collins, S.P.; Aghdam, N.; Chu, F.I.; Kaplan, I.D.; Appelbaum, L.; Fuller, D.B.; et al. Long-Term Outcomes of Stereotactic Body Radiotherapy for Low-Risk and Intermediate-Risk Prostate Cancer. JAMA Netw. Open 2019, 2, e188006. [Google Scholar] [CrossRef]
- Jackson, W.C.; Silva, J.; Hartman, H.E.; Dess, R.T.; Kishan, A.U.; Beeler, W.H.; Gharzai, L.A.; Jaworski, E.M.; Mehra, R.; Hearn, J.W.D.; et al. Stereotactic Body Radiation Therapy for Localized Prostate Cancer: A Systematic Review and Meta-Analysis of Over 6000 Patients Treated On Prospective Studies. Int. J. Radiat. Oncol. Biol. Phys. 2019, 104, 778–789. [Google Scholar] [CrossRef]
- Widmark, A.; Gunnlaugsson, A.; Beckman, L.; Thellenberg-Karlsson, C.; Hoyer, M.; Lagerlund, M.; Kindblom, J.; Ginman, C.; Johansson, B.; Björnlinger, K.; et al. Ultra-Hypofractionated Versus Conventionally Fractionated Radiotherapy for Prostate Cancer: 5-Year Outcomes of the HYPO-RT-PC Randomised, Non-Inferiority, Phase 3 Trial. Lancet 2019, 394, 385–395. [Google Scholar] [CrossRef]
- Tree, A.C.; Ostler, P.; van der Voet, H.; Chu, W.; Loblaw, A.; Ford, D.; Tolan, S.; Jain, S.; Martin, A.; Staffurth, J.; et al. Intensity-modulated radiotherapy versus stereotactic body radiotherapy for prostate cancer (PACE-B): 2-year toxicity results from an open-label, randomised, phase 3, non-inferiority trial. Lancet Oncol. 2022, 23, 1308–1320. [Google Scholar] [CrossRef] [PubMed]
- Ballhausen, H.; Li, M.; Hegemann, N.S.; Ganswindt, U.; Belka, C. Intra-Fraction Motion of the Prostate Is a Random Walk. Phys. Med. Biol. 2015, 60, 549–563. [Google Scholar] [CrossRef]
- Udrescu, C.; Jalade, P.; De Bari, B.; Michel-Amadry, G.; Chapet, O. Evaluation of the respiratory prostate motion with four-dimensional computed tomography scan acquisitions using three implanted markers. Radiother. Oncol. 2012, 103, 266–269. [Google Scholar] [CrossRef]
- Legge, K.; Nguyen, D.; Ng, J.A.; Wilton, L.; Richardson, M.; Booth, J.; Keall, P.; O’Connor, D.J.; Greer, P.; Martin, J. Real-Time Intrafraction Prostate Motion During Linac Based Stereotactic Radiotherapy With Rectal Displacement. J. Appl. Clin. Med. Phys. 2017, 18, 130–136. [Google Scholar] [CrossRef] [PubMed]
- Lovelock, D.M.; Messineo, A.P.; Cox, B.W.; Kollmeier, M.A.; Zelefsky, M.J. Continuous Monitoring and Intrafraction Target Position Correction During Treatment Improves Target Coverage for Patients Undergoing SBRT Prostate Therapy. Int. J. Radiat. Oncol. Biol. Phys. 2015, 91, 588–594. [Google Scholar] [CrossRef] [PubMed]
- Panizza, D.; Faccenda, V.; Lucchini, R.; Daniotti, M.C.; Trivellato, S.; Caricato, P.; Pisoni, V.; De Ponti, E.; Arcangeli, S. Intrafraction Prostate Motion Management during Dose-Escalated Linac-Based Stereotactic Body Radiation Therapy. Front. Oncol. 2022, 7, 883725. [Google Scholar] [CrossRef]
- Herrera, F.G.; Valerio, M.; Berthold, D.; Tawadros, T.; Meuwly, J.Y.; Vallet, V.; Baumgartner, P.; Thierry, A.C.; De Bari, B.; Jichlinski, P.; et al. 50-Gy Stereotactic Body Radiation Therapy to the Dominant Intraprostatic Nodule: Results From a Phase 1a/b Trial. Int. J. Radiat. Oncol. Biol. Phys. 2019, 103, 320–334. [Google Scholar] [CrossRef] [PubMed]
- Scher, N.; Bauduceau, O.; Bollet, M.; Lamallem, H.; Charas, T.; Garaud, P.; Foster, D.; Fawzi, M.; Labidi, M.; Toledano, A. Stereotactic prostate focal reirradiation therapy for local recurrence: Preliminary results of Hartmann Oncology Radiotherapy Group. BJR Open 2019, 1, 20180027. [Google Scholar] [CrossRef]
- Lucchini, R.; Panizza, D.; Colciago, R.R.; Vernier, V.; Daniotti, M.C.; Faccenda, V.; Arcangeli, S. Treatment Outcome and Compliance to Dose-Intensified Linac-Based SBRT for Unfavorable Prostate Tumors Using a Novel Real-Time Organ- Motion Tracking. Radiat. Oncol. 2021, 16, 180. [Google Scholar] [CrossRef]
- Kindblom, J.; Ekelund-Olvenmark, A.M.; Syren, H.; Iustin, R.; Braide, K.; Frank- Lissbrant, I.; Lennernäs, B. High Precision Transponder Localization Using a Novel Electromagnetic Positioning System in Patients With Localized Prostate Cancer. Radiother. Oncol. 2009, 90, 307–311. [Google Scholar] [CrossRef]
- Epstein, J.I.; Egevad, L.; Amin, M.B.; Delahunt, B.; Srigley, J.R.; Humphrey, P.A.; Grading Committee. The 2014 International Society of Urological Pathology (ISUP) Consensus Conference on Gleason Grading of Prostatic Carcinoma: Definition of Grading Patterns and Proposal for a New Grading System. Am. J. Surg. Pathol. 2016, 40, 244. [Google Scholar] [CrossRef] [PubMed]
- de Crevoisier, R.; Bayar, M.A.; Pommier, P.; Muracciole, X.; Pêne, F.; Dudouet, P.; Latorzeff, I.; Beckendorf, V.; Bachaud, J.M.; Laplanche, A.; et al. Daily Versus Weekly Prostate Cancer Image Guided Radiation Therapy: Phase 3 Multicenter Randomized Trial. Int. J. Radiat. Oncol. Biol. Phys. 2018, 102, 1420–1429. [Google Scholar] [CrossRef] [PubMed]
- de Crevoisier, R.; Tucker, S.L.; Dong, L.; Mohan, R.; Cheung, R.; Cox, J.D.; Kuban, D.A. Increased Risk of Biochemical and Local Failure in Patients With Distended Rectum on the Planning CT for Prostate Cancer Radiotherapy. Int. J. Radiat. Oncol. Biol. Phys. 2005, 62, 965–973. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Tang, W.; Luo, H.; Jin, F.; Wang, Y. The role of image-guided radiotherapy in prostate cancer: A systematic review and meta-analysis. Clin. Transl. Radiat. Oncol. 2023, 38, 81–89. [Google Scholar] [CrossRef] [PubMed]
- Bertholet, J.; Knopf, A.; Eiben, B.; McClelland, J.; Grimwood, A.; Harris, E.; Menten, M.; Poulsen, P.; Nguyen, D.T.; Keall, P. Real-Time Intrafraction Motion Monitoring in External Beam Radiotherapy. Phys. Med. Biol. 2019, 64, 15TR01. [Google Scholar] [CrossRef]
- Kupelian, P.; Willoughby, T.; Mahadevan, A.; Djemil, T.; Weinstein, G.; Jani, S.; Enke, C.; Solberg, T.; Flores, N.; Liu, D.; et al. Multi-Institutional Clinical Experience With the Calypso System in Localization and Continuous, Real-Time Monitoring of the Prostate Gland During External Radiotherapy. Int. J. Radiat. Oncol. Biol. Phys. 2007, 67, 1088–1098. [Google Scholar] [CrossRef]
- Zhu, X.; Bourland, J.D.; Yuan, Y.; Zhuang, T.; O’Daniel, J.; Thongphiew, D.; Wu, Q.J.; Das, S.K.; Yoo, S.; Yin, F.F. Tradeoffs of Integrating Real-Time Tracking Into IGRT for Prostate Cancer Treatment. Phys. Med. Biol. 2009, 54, N393–N401. [Google Scholar] [CrossRef]
- Braide, K.; Lindencrona, U.; Welinder, K.; Götstedt, J.; Ståhl, I.; Pettersson, N.; Kindblom, J. Clinical Feasibility and Positional Stability of an Implanted Wired Transmitter in a Novel Electromagnetic Positioning System for Prostate Cancer Radiotherapy. Radiother. Oncol. 2018, 128, 336–342. [Google Scholar] [CrossRef]
- Vanhanen, A.; Syrén, H.; Kapanen, M. Localization Accuracy of Two Electromagnetic Tracking Systems in Prostate Cancer Radiotherapy: A Comparison with Fiducial Marker Based Kilovoltage Imaging. Phys. Med. 2018, 56, 10–18. [Google Scholar] [CrossRef]
- Mah, D.; Freedman, G.; Milestone, B.; Hanlon, A.; Palacio, E.; Richardson, T.; Movsas, B.; Mitra, R.; Horwitz, E.; Hanks, G.E. Measurement of Intrafractional Prostate Motion Using Magnetic Resonance Imaging. Int. J. Radiat. Oncol. Biol. Phys. 2002, 54, 568–575. [Google Scholar] [CrossRef]
- Quon, H.; Loblaw, D.A.; Cheung, P.C.; Holden, L.; Tang, C.; Pang, G.; Morton, G.; Mamedov, A.; Deabreu, A. Intra- Fraction Motion during Extreme Hypofractionated Radiotherapy of the Prostate Using Pre- and Post-Treatment Imaging. Clin. Oncol. 2012, 24, 640–645. [Google Scholar] [CrossRef] [PubMed]
- Koike, Y.; Sumida, I.; Mizuno, H.; Shiomi, H.; Kurosu, K.; Ota, S.; Yoshioka, Y.; Suzuki, O.; Tamari, K.; Ogawa, K. Dosimetric Impact of Intra-Fraction Prostate Motion Under a Tumour-Tracking System in hypofractionated robotic radiosurgery. PLoS ONE 2018, 13, e0195296. [Google Scholar] [CrossRef] [PubMed]
- Gorovets, D.; Burleson, S.; Jacobs, L.; Ravindranath, B.; Tierney, K.; Kollmeier, M.; McBride, S.; Happersett, L.; Hunt, M.; Zelefsky, M. Prostate SBRT With Intrafraction Motion Management Using a Novel Linear Accelerator-Based MV-kV Imaging Method. Pract. Radiat. Oncol. 2020, 10, e388–e396. [Google Scholar] [CrossRef] [PubMed]
- Levin-Epstein, R.; Qiao-Guan, G.; Juarez, J.E.; Shen, Z.; Steinberg, M.L.; Ruan, D.; Valle, L.; Nickols, N.G.; Kupelian, P.A.; King, C.; et al. Clinical Assessment of Prostate Displacement and Planning Target Volume Margins for Stereotactic Body Radiotherapy of Prostate Cancer. Front. Oncol. 2020, 10, 539. [Google Scholar] [CrossRef]
- Zelefsky, M.J.; Kollmeier, M.; Cox, B.; Fidaleo, A.; Sperling, D.; Pei, X.; Carver, B.; Coleman, J.; Lovelock, M.; Hunt, M. Improved Clinical Outcomes with High-Dose Image Guided Radiotherapy Compared With Non-IGRT for the Treatment of Clinically Localized Prostate Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2012, 84, 125–129. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Number of Cases | % | |
|---|---|---|
| Number of patients | 31 | 100 |
| Age at the moment of the diagnosis (years) | ||
| Mean | 73.6 | |
| Median | 73.8 | |
| Range (min–max) | (60.7–84.6) | |
| T stage (defined with pre-treatment MRI) | ||
| 1c | 1 | 3.2 |
| 2a | 15 | 48.3 |
| 2b | 3 | 9.7 |
| 2c | 5 | 16.1 |
| 3a | 3 | 9.7 |
| Relapsing pre-treated PCa | 4 | 13 |
| PSA at the moment of the diagnosis (ng/mL) * | ||
| Mean | 8.57 | |
| Median | 8.43 | |
| Range (min–max) | (3.05–20) | |
| ISUP category risk (as defined in [21]) | ||
| 1 | 5 | 16.1 |
| 2 | 13 | 42 |
| 3 | 7 | 22.6 |
| 4 | 2 | 6.4 |
| 5 | 0 | 0 |
| Relapsing pre-treated PCa | 4 | 12.9 |
| Total n. of XVI CBCT | Median | Min | Max | |
|---|---|---|---|---|
| Session 1 | 62 | 1 | 1 | 11 |
| Session 2 | 60 | 2 | 1 | 5 |
| Session 3 | 57 | 1 | 1 | 6 |
| Session 4 | 70 | 1 | 1 | 10 |
| Session 5 | 50 | 1 | 1 | 5 |
| Direction | Mean (mm) | SD (mm) | Mean Absolute (mm) |
|---|---|---|---|
| Lateral | −0.38 | 2.76 | 1.0969 |
| Longitudinal | −0.28 | 2.42 | 1.208 |
| Vertical | −0.38 | 1.92 | 1.0957 |
| Group | Setup Phase | Delivery Phase | Overall Time (Setup + Delivery) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| lat | Lng | Vrt | Lat | Lng | Vrt | Lat | Lng | Vrt | |
| Whole population | 12% | 20% | 22% | 4% | 9% | 11% | 10% | 17% | 19% |
| Group A | 4% | 2% | 4% | 0 | 0.2% | 18% | 2% | 1% | 7% |
| Group B | 17% | 25% | 26% | 2% | 5% | 9% | 13% | 19% | 21% |
| Group C | 9% | 17% | 19% | 5% | 12% | 13% | 8% | 15% | 17% |
| Mean | Median | Min | Max | |
|---|---|---|---|---|
| Fraction #1 | 14 min 33 s | 8 min 48 s | 5 min 49 s | 1 h 05 min 28 s |
| Fraction #2 | 12 min 54 | 11 min 49 | 5 min 23 s | 34 min 35 s |
| Fraction #3 | 12 min 36 | 10 min 53 | 5 min 31 s | 47 min 15 s |
| Fraction #4 | 12 min 00 | 8 min 40 | 5 min 18 s | 55 min |
| Fraction #5 | 11 min 32 | 8 min 39 | 5 min 21 s | 58 min 28 s |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Bari, B.; Guibert, G.; Slimani, S.; Bashar, Y.; Risse, T.; Guisolan, N.; Trouillot, J.; Abel, J.; Weber, P. Electromagnetic Transmitter-Based Prostate Gating for Dose-Escalated Linac-Based Stereotactic Body Radiation Therapy: An Evaluation of Intrafraction Motion. Curr. Oncol. 2024, 31, 962-974. https://doi.org/10.3390/curroncol31020072
De Bari B, Guibert G, Slimani S, Bashar Y, Risse T, Guisolan N, Trouillot J, Abel J, Weber P. Electromagnetic Transmitter-Based Prostate Gating for Dose-Escalated Linac-Based Stereotactic Body Radiation Therapy: An Evaluation of Intrafraction Motion. Current Oncology. 2024; 31(2):962-974. https://doi.org/10.3390/curroncol31020072
Chicago/Turabian StyleDe Bari, Berardino, Geoffroy Guibert, Sabrine Slimani, Yanes Bashar, Terence Risse, Nicole Guisolan, Juliane Trouillot, Jonathan Abel, and Patrick Weber. 2024. "Electromagnetic Transmitter-Based Prostate Gating for Dose-Escalated Linac-Based Stereotactic Body Radiation Therapy: An Evaluation of Intrafraction Motion" Current Oncology 31, no. 2: 962-974. https://doi.org/10.3390/curroncol31020072
APA StyleDe Bari, B., Guibert, G., Slimani, S., Bashar, Y., Risse, T., Guisolan, N., Trouillot, J., Abel, J., & Weber, P. (2024). Electromagnetic Transmitter-Based Prostate Gating for Dose-Escalated Linac-Based Stereotactic Body Radiation Therapy: An Evaluation of Intrafraction Motion. Current Oncology, 31(2), 962-974. https://doi.org/10.3390/curroncol31020072