Multimodal Approaches to Patient Selection for Pancreas Cancer Surgery


Abstract
:1. Introduction
2. Pathology Acquisition and Biliary Drainage
3. Complete Staging and Resectability Assessment
3.1. Structural Assessment
3.1.1. Computed Tomography
3.1.2. Magnetic Resonance Imaging
3.2. Biological Assessment
3.2.1. Blood Work
3.2.2. Positron Emission Tomography
3.3. Radiographically Occult Disease Assessment
Diagnostic Laparoscopy
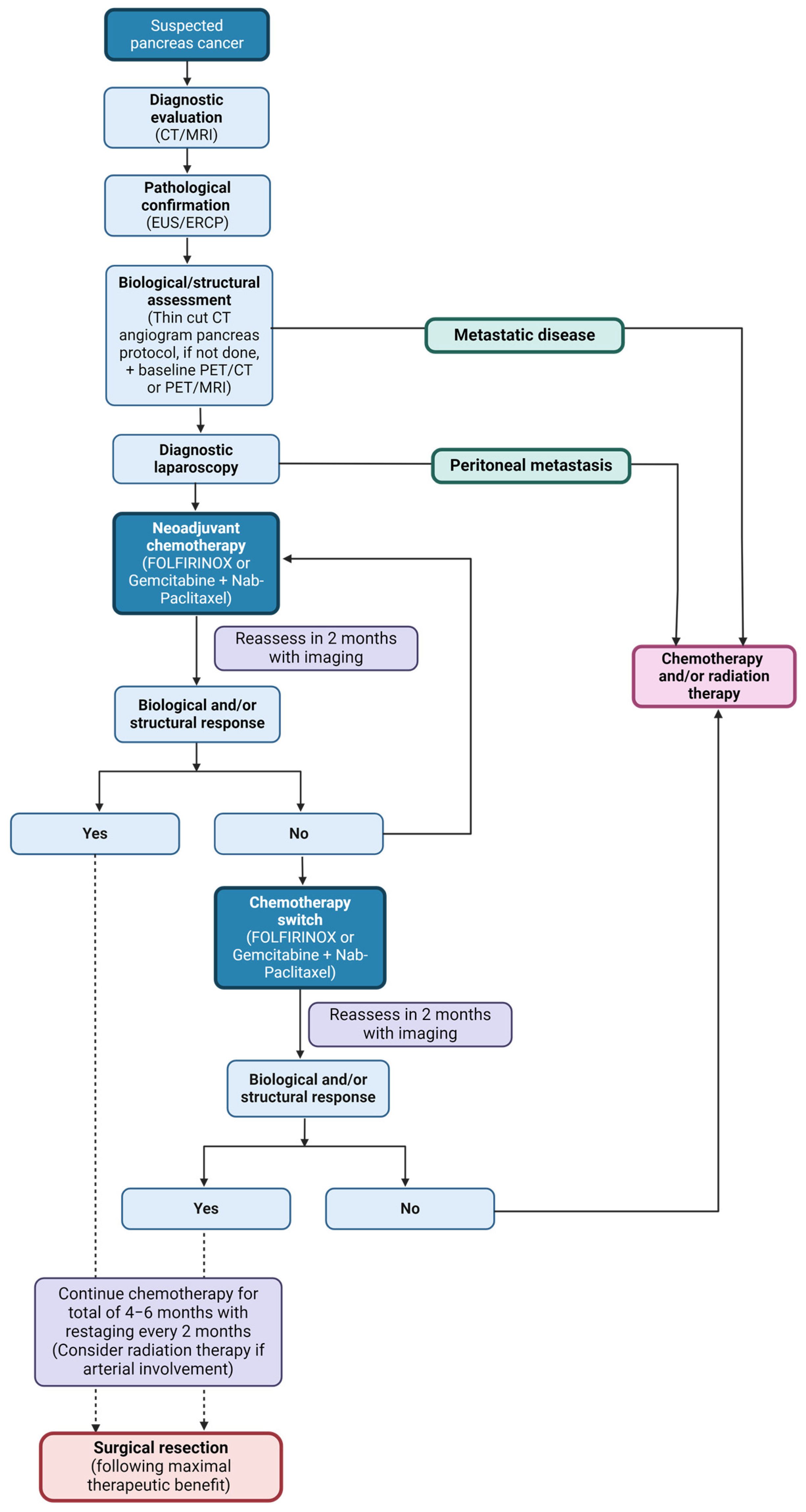
4. Neoadjuvant Treatment
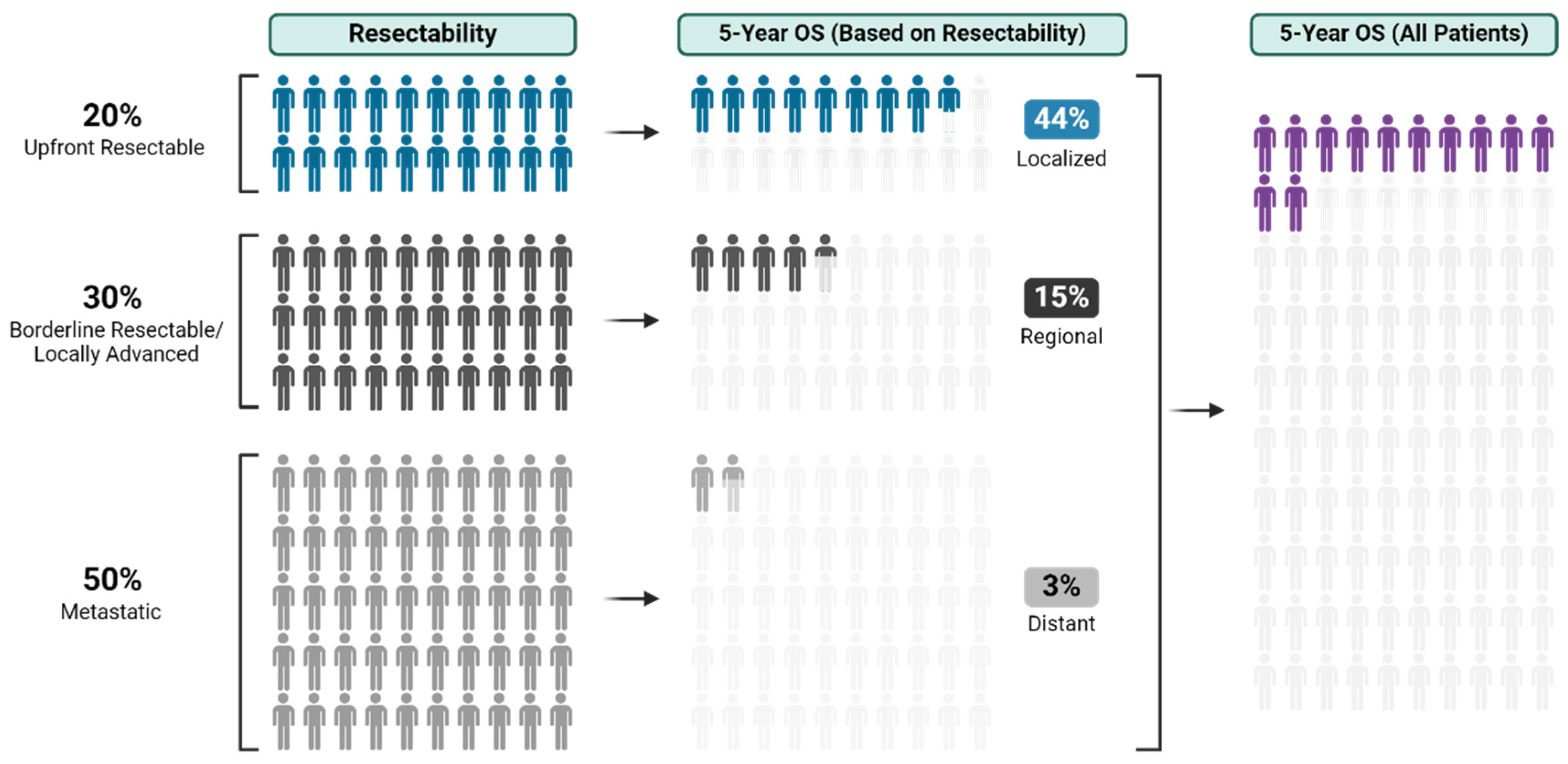
5. Resectability
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Siegel, R.L.; Giaquinto, A.N.; Jemal, A. Cancer statistics, 2024. CA Cancer J. Clin. 2024, 74, 12–49. [Google Scholar] [CrossRef] [PubMed]
- Grossberg, A.J.; Chu, L.C.; Deig, C.R.; Fishman, E.K.; Hwang, W.L.; Maitra, A.; Marks, D.L.; Mehta, A.; Nabavizadeh, N.; Simeone, D.M.; et al. Multidisciplinary standards of care and recent progress in pancreatic ductal adenocarcinoma. CA Cancer J. Clin. 2020, 70, 375–403. [Google Scholar] [CrossRef] [PubMed]
- Hall, B.R.; Cannon, A.; Atri, P.; Wichman, C.S.; Smith, L.M.; Ganti, A.K.; Are, C.; Sasson, A.R.; Kumar, S.; Batra, S.K. Advanced pancreatic cancer: A meta-analysis of clinical trials over thirty years. Oncotarget 2018, 9, 19396–19405. [Google Scholar] [CrossRef] [PubMed]
- Sohn, T.A.; Yeo, C.J.; Cameron, J.L.; Koniaris, L.; Kaushal, S.; Abrams, R.A.; Sauter, P.K.; Coleman, J.; Hruban, R.H.; Lillemoe, K.D. Resected adenocarcinoma of the pancreas-616 patients: Results, outcomes, and prognostic indicators. J. Gastrointest. Surg. 2000, 4, 567–579. [Google Scholar] [CrossRef] [PubMed]
- Neoptolemos, J.P.; Stocken, D.D.; Dunn, J.A.; Almond, J.; Beger, H.G.; Pederzoli, P.; Bassi, C.; Dervenis, C.; Fernandez-Cruz, L.; Lacaine, F.; et al. Influence of resection margins on survival for patients with pancreatic cancer treated by adjuvant chemoradiation and/or chemotherapy in the ESPAC-1 randomized controlled trial. Ann. Surg. 2001, 234, 758–768. [Google Scholar] [CrossRef] [PubMed]
- Mizrahi, J.D.; Surana, R.; Valle, J.W.; Shroff, R.T. Pancreatic cancer. Lancet 2020, 395, 2008–2020. [Google Scholar] [CrossRef]
- Katz, M.H.; Fleming, J.B.; Bhosale, P.; Varadhachary, G.; Lee, J.E.; Wolff, R.; Wang, H.; Abbruzzese, J.; Pisters, P.W.; Vauthey, J.N.; et al. Response of borderline resectable pancreatic cancer to neoadjuvant therapy is not reflected by radiographic indicators. Cancer 2012, 118, 5749–5756. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, S.A.; Duong, M.; Sohal, D.P.S.; Gandhi, N.S.; Beg, M.S.; Wang-Gillam, A.; Wade, J.L., 3rd; Chiorean, E.G.; Guthrie, K.A.; Lowy, A.M.; et al. Surgical Outcome Results from SWOG S1505: A Randomized Clinical Trial of mFOLFIRINOX versus Gemcitabine/Nab-paclitaxel for Perioperative Treatment of Resectable Pancreatic Ductal Adenocarcinoma. Ann. Surg. 2020, 272, 481–486. [Google Scholar] [CrossRef] [PubMed]
- Isaji, S.; Mizuno, S.; Windsor, J.A.; Bassi, C.; Fernandez-Del Castillo, C.; Hackert, T.; Hayasaki, A.; Katz, M.H.G.; Kim, S.W.; Kishiwada, M.; et al. International consensus on definition and criteria of borderline resectable pancreatic ductal adenocarcinoma 2017. Pancreatology 2018, 18, 2–11. [Google Scholar] [CrossRef]
- Katz, M.H.; Pisters, P.W.; Evans, D.B.; Sun, C.C.; Lee, J.E.; Fleming, J.B.; Vauthey, J.N.; Abdalla, E.K.; Crane, C.H.; Wolff, R.A.; et al. Borderline resectable pancreatic cancer: The importance of this emerging stage of disease. J. Am. Coll. Surg. 2008, 206, 833–846; discussion 846–848. [Google Scholar] [CrossRef]
- Varadhachary, G.R.; Tamm, E.P.; Abbruzzese, J.L.; Xiong, H.Q.; Crane, C.H.; Wang, H.; Lee, J.E.; Pisters, P.W.; Evans, D.B.; Wolff, R.A. Borderline resectable pancreatic cancer: Definitions, management, and role of preoperative therapy. Ann. Surg. Oncol. 2006, 13, 1035–1046. [Google Scholar] [CrossRef]
- Vauthey, J.N.; Dixon, E. AHPBA/SSO/SSAT Consensus Conference on Resectable and Borderline Resectable Pancreatic Cancer: Rationale and overview of the conference. Ann. Surg. Oncol. 2009, 16, 1725–1726. [Google Scholar] [CrossRef] [PubMed]
- Okusaka, T.; Nakamura, M.; Yoshida, M.; Kitano, M.; Uesaka, K.; Ito, Y.; Furuse, J.; Hanada, K.; Okazaki, K.; Committee for Revision of Clinical Guidelines for Pancreatic Cancer of the Japan Pancreas Society. Clinical Practice Guidelines for Pancreatic Cancer 2019 from the Japan Pancreas Society: A Synopsis. Pancreas 2020, 49, 326–335. [Google Scholar] [CrossRef] [PubMed]
- Truty, M.J.; Kendrick, M.L.; Nagorney, D.M.; Smoot, R.L.; Cleary, S.P.; Graham, R.P.; Goenka, A.H.; Hallemeier, C.L.; Haddock, M.G.; Harmsen, W.S.; et al. Factors Predicting Response, Perioperative Outcomes, and Survival Following Total Neoadjuvant Therapy for Borderline/Locally Advanced Pancreatic Cancer. Ann. Surg. 2021, 273, 341–349. [Google Scholar] [CrossRef]
- Maggino, L.; Malleo, G.; Marchegiani, G.; Viviani, E.; Nessi, C.; Ciprani, D.; Esposito, A.; Landoni, L.; Casetti, L.; Tuveri, M.; et al. Outcomes of Primary Chemotherapy for Borderline Resectable and Locally Advanced Pancreatic Ductal Adenocarcinoma. JAMA Surg. 2019, 154, 932–942. [Google Scholar] [CrossRef]
- Jolissaint, J.S.; Reyngold, M.; Bassmann, J.; Seier, K.P.; Gonen, M.; Varghese, A.M.; Yu, K.H.; Park, W.; O’Reilly, E.M.; Balachandran, V.P.; et al. Local Control and Survival after Induction Chemotherapy and Ablative Radiation Versus Resection for Pancreatic Ductal Adenocarcinoma with Vascular Involvement. Ann. Surg. 2021, 274, 894–901. [Google Scholar] [CrossRef] [PubMed]
- Truty, M.J.; Colglazier, J.J.; Mendes, B.C.; Nagorney, D.M.; Bower, T.C.; Smoot, R.L.; DeMartino, R.R.; Cleary, S.P.; Oderich, G.S.; Kendrick, M.L. En Bloc Celiac Axis Resection for Pancreatic Cancer: Classification of Anatomical Variants Based on Tumor Extent. J. Am. Coll. Surg. 2020, 231, 8–29. [Google Scholar] [CrossRef]
- Shi, C.; Klein, A.P.; Goggins, M.; Maitra, A.; Canto, M.; Ali, S.; Schulick, R.; Palmisano, E.; Hruban, R.H. Increased Prevalence of Precursor Lesions in Familial Pancreatic Cancer Patients. Clin. Cancer Res. 2009, 15, 7737–7743. [Google Scholar] [CrossRef]
- Lau, M.K.; Davila, J.A.; Shaib, Y.H. Incidence and survival of pancreatic head and body and tail cancers: A population-based study in the United States. Pancreas 2010, 39, 458–462. [Google Scholar] [CrossRef]
- Saad, A.M.; Turk, T.; Al-Husseini, M.J.; Abdel-Rahman, O. Trends in pancreatic adenocarcinoma incidence and mortality in the United States in the last four decades; a SEER-based study. BMC Cancer 2018, 18, 688. [Google Scholar] [CrossRef]
- Wong, J.C.; Lu, D.S. Staging of pancreatic adenocarcinoma by imaging studies. Clin. Gastroenterol. Hepatol. 2008, 6, 1301–1308. [Google Scholar] [CrossRef]
- Agarwal, B.; Abu-Hamda, E.; Molke, K.L.; Correa, A.M.; Ho, L. Endoscopic ultrasound-guided fine needle aspiration and multidetector spiral CT in the diagnosis of pancreatic cancer. Am. J. Gastroenterol. 2004, 99, 844–850. [Google Scholar] [CrossRef]
- Owens, D.J.; Savides, T.J. Endoscopic ultrasound staging and novel therapeutics for pancreatic cancer. Surg. Oncol. Clin. N. Am. 2010, 19, 255–266. [Google Scholar] [CrossRef] [PubMed]
- Cote, G.A.; Sherman, S. Endoscopic palliation of pancreatic cancer. Cancer J. 2012, 18, 584–590. [Google Scholar] [CrossRef] [PubMed]
- Ghazi, R.; AbiMansour, J.P.; Mahmoud, T.; Martin, J.A.; Law, R.J.; Levy, M.J.; Abu Dayyeh, B.K.; Storm, A.C.; Petersen, B.T.; Chandrasekhara, V. Uncovered versus fully covered self-expandable metal stents for the management of distal malignant biliary obstruction. Gastrointest. Endosc. 2023, 98, 577–584.e4. [Google Scholar] [CrossRef]
- Speer, A.G.; Cotton, P.B.; Russell, R.C.; Mason, R.R.; Hatfield, A.R.; Leung, J.W.; MacRae, K.D.; Houghton, J.; Lennon, C.A. Randomised trial of endoscopic versus percutaneous stent insertion in malignant obstructive jaundice. Lancet 1987, 2, 57–62. [Google Scholar] [CrossRef]
- Strom, T.J.; Klapman, J.B.; Springett, G.M.; Meredith, K.L.; Hoffe, S.E.; Choi, J.; Hodul, P.; Malafa, M.P.; Shridhar, R. Comparative long-term outcomes of upfront resected pancreatic cancer after preoperative biliary drainage. Surg. Endosc. 2015, 29, 3273–3281. [Google Scholar] [CrossRef]
- Dorcaratto, D.; Hogan, N.M.; Munoz, E.; Garces, M.; Limongelli, P.; Sabater, L.; Ortega, J. Is Percutaneous Transhepatic Biliary Drainage Better than Endoscopic Drainage in the Management of Jaundiced Patients Awaiting Pancreaticoduodenectomy? A Systematic Review and Meta-analysis. J. Vasc. Interv. Radiol. 2018, 29, 676–687. [Google Scholar] [CrossRef] [PubMed]
- Fletcher, J.G.; Wiersema, M.J.; Farrell, M.A.; Fidler, J.L.; Burgart, L.J.; Koyama, T.; Johnson, C.D.; Stephens, D.H.; Ward, E.M.; Harmsen, W.S. Pancreatic malignancy: Value of arterial, pancreatic, and hepatic phase imaging with multi-detector row CT. Radiology 2003, 229, 81–90. [Google Scholar] [CrossRef]
- Frisch, A.; Walter, T.C.; Hamm, B.; Denecke, T. Efficacy of oral contrast agents for upper gastrointestinal signal suppression in MRCP: A systematic review of the literature. Acta Radiol. Open 2017, 6, 2058460117727315. [Google Scholar] [CrossRef]
- Al-Hawary, M.M.; Francis, I.R.; Chari, S.T.; Fishman, E.K.; Hough, D.M.; Lu, D.S.; Macari, M.; Megibow, A.J.; Miller, F.H.; Mortele, K.J.; et al. Pancreatic ductal adenocarcinoma radiology reporting template: Consensus statement of the society of abdominal radiology and the american pancreatic association. Gastroenterology 2014, 146, 291–304.e1. [Google Scholar] [CrossRef] [PubMed]
- Chen, F.M.; Ni, J.M.; Zhang, Z.Y.; Zhang, L.; Li, B.; Jiang, C.J. Presurgical Evaluation of Pancreatic Cancer: A Comprehensive Imaging Comparison of CT versus MRI. AJR Am. J. Roentgenol. 2016, 206, 526–535. [Google Scholar] [CrossRef] [PubMed]
- Hartwig, W.; Strobel, O.; Hinz, U.; Fritz, S.; Hackert, T.; Roth, C.; Buchler, M.W.; Werner, J. CA19-9 in potentially resectable pancreatic cancer: Perspective to adjust surgical and perioperative therapy. Ann. Surg. Oncol. 2013, 20, 2188–2196. [Google Scholar] [CrossRef] [PubMed]
- Bergquist, J.R.; Ivanics, T.; Storlie, C.B.; Groeschl, R.T.; Tee, M.C.; Habermann, E.B.; Smoot, R.L.; Kendrick, M.L.; Farnell, M.B.; Roberts, L.R.; et al. Implications of CA19-9 elevation for survival, staging, and treatment sequencing in intrahepatic cholangiocarcinoma: A national cohort analysis. J. Surg. Oncol. 2016, 114, 475–482. [Google Scholar] [CrossRef] [PubMed]
- van Veldhuisen, E.; Vogel, J.A.; Klompmaker, S.; Busch, O.R.; van Laarhoven, H.W.M.; van Lienden, K.P.; Wilmink, J.W.; Marsman, H.A.; Besselink, M.G. Added value of CA19-9 response in predicting resectability of locally advanced pancreatic cancer following induction chemotherapy. HPB 2018, 20, 605–611. [Google Scholar] [CrossRef]
- Bergquist, J.R.; Puig, C.A.; Shubert, C.R.; Groeschl, R.T.; Habermann, E.B.; Kendrick, M.L.; Nagorney, D.M.; Smoot, R.L.; Farnell, M.B.; Truty, M.J. Carbohydrate Antigen 19-9 Elevation in Anatomically Resectable, Early Stage Pancreatic Cancer Is Independently Associated with Decreased Overall Survival and an Indication for Neoadjuvant Therapy: A National Cancer Database Study. J. Am. Coll. Surg. 2016, 223, 52–65. [Google Scholar] [CrossRef] [PubMed]
- Maisey, N.R.; Norman, A.R.; Hill, A.; Massey, A.; Oates, J.; Cunningham, D. CA19-9 as a prognostic factor in inoperable pancreatic cancer: The implication for clinical trials. Br. J. Cancer 2005, 93, 740–743. [Google Scholar] [CrossRef] [PubMed]
- Azizian, A.; Ruhlmann, F.; Krause, T.; Bernhardt, M.; Jo, P.; Konig, A.; Kleiss, M.; Leha, A.; Ghadimi, M.; Gaedcke, J. CA19-9 for detecting recurrence of pancreatic cancer. Sci. Rep. 2020, 10, 1332. [Google Scholar] [CrossRef] [PubMed]
- Abdel-Misih, S.R.; Hatzaras, I.; Schmidt, C.; Saab, T.B.; Klemanski, D.; Muscarella, P.; Melvin, W.S.; Ellison, E.C.; Bloomston, M. Failure of normalization of CA19-9 following resection for pancreatic cancer is tantamount to metastatic disease. Ann. Surg. Oncol. 2011, 18, 1116–1121. [Google Scholar] [CrossRef] [PubMed]
- Kondo, N.; Murakami, Y.; Uemura, K.; Hayashidani, Y.; Sudo, T.; Hashimoto, Y.; Nakashima, A.; Sakabe, R.; Shigemoto, N.; Kato, Y.; et al. Prognostic impact of perioperative serum CA 19-9 levels in patients with resectable pancreatic cancer. Ann. Surg. Oncol. 2010, 17, 2321–2329. [Google Scholar] [CrossRef]
- Macedo, F.I.; Ryon, E.; Maithel, S.K.; Lee, R.M.; Kooby, D.A.; Fields, R.C.; Hawkins, W.G.; Williams, G.; Maduekwe, U.; Kim, H.J.; et al. Survival Outcomes Associated with Clinical and Pathological Response Following Neoadjuvant FOLFIRINOX or Gemcitabine/Nab-Paclitaxel Chemotherapy in Resected Pancreatic Cancer. Ann. Surg. 2019, 270, 400–413. [Google Scholar] [CrossRef] [PubMed]
- Choi, M.; Heilbrun, L.K.; Venkatramanamoorthy, R.; Lawhorn-Crews, J.M.; Zalupski, M.M.; Shields, A.F. Using 18F-fluorodeoxyglucose positron emission tomography to monitor clinical outcomes in patients treated with neoadjuvant chemo-radiotherapy for locally advanced pancreatic cancer. Am. J. Clin. Oncol. 2010, 33, 257–261. [Google Scholar] [CrossRef] [PubMed]
- Diaz, C.L.; Cinar, P.; Hwang, J.; Ko, A.H.; Tempero, M.A. CA 19-9 Response: A Surrogate to Predict Survival in Patients with Metastatic Pancreatic Adenocarcinoma. Am. J. Clin. Oncol. 2019, 42, 898–902. [Google Scholar] [CrossRef] [PubMed]
- Barreto, S.G.; Loveday, B.; Windsor, J.A.; Pandanaboyana, S. Detecting tumour response and predicting resectability after neoadjuvant therapy for borderline resectable and locally advanced pancreatic cancer. ANZ J. Surg. 2019, 89, 481–487. [Google Scholar] [CrossRef] [PubMed]
- Higashi, T.; Sakahara, H.; Torizuka, T.; Nakamoto, Y.; Kanamori, S.; Hiraoka, M.; Imamura, M.; Nishimura, Y.; Tamaki, N.; Konishi, J. Evaluation of intraoperative radiation therapy for unresectable pancreatic cancer with FDG PET. J. Nucl. Med. 1999, 40, 1424–1433. [Google Scholar] [PubMed]
- Abdelrahman, A.M.; Goenka, A.H.; Alva-Ruiz, R.; Yonkus, J.A.; Leiting, J.L.; Graham, R.P.; Merrell, K.W.; Thiels, C.A.; Hallemeier, C.L.; Warner, S.G.; et al. FDG-PET Predicts Neoadjuvant Therapy Response and Survival in Borderline Resectable/Locally Advanced Pancreatic Adenocarcinoma. J. Natl. Compr. Canc Netw. 2022, 20, 1023–1032.e3. [Google Scholar] [CrossRef] [PubMed]
- Alva-Ruiz, R.; Yohanathan, L.; Yonkus, J.A.; Abdelrahman, A.M.; Gregory, L.A.; Halfdanarson, T.R.; Mahipal, A.; McWilliams, R.R.; Ma, W.W.; Hallemeier, C.L.; et al. Neoadjuvant Chemotherapy Switch in Borderline Resectable/Locally Advanced Pancreatic Cancer. Ann. Surg. Oncol. 2022, 29, 1579–1591. [Google Scholar] [CrossRef] [PubMed]
- Hue, J.J.; Dorth, J.; Sugumar, K.; Hardacre, J.M.; Ammori, J.B.; Rothermel, L.D.; Saltzman, J.; Mohamed, A.; Selfridge, J.E.; Bajor, D.; et al. Neoadjuvant Radiotherapy is Associated with Improved Pathologic Outcomes and Survival in Resected Stage II–III Pancreatic Adenocarcinoma Treated with Multiagent Neoadjuvant Chemotherapy in the Modern Era. Am. Surg. 2021, 87, 1386–1395. [Google Scholar] [CrossRef] [PubMed]
- Fong, Z.V.; Ferrone, C.R. Surgery After Response to Chemotherapy for Locally Advanced Pancreatic Ductal Adenocarcinoma: A Guide for Management. J. Natl. Compr. Cancer Netw. 2021, 19, 459–467. [Google Scholar] [CrossRef]
- Gudmundsdottir, H.; Yonkus, J.A.; Alva-Ruiz, R.; Kendrick, M.L.; Smoot, R.L.; Warner, S.G.; Starlinger, P.; Thiels, C.A.; Nagorney, D.M.; Cleary, S.P.; et al. Yield of Staging Laparoscopy for Pancreatic Cancer in the Modern Era: Analysis of More than 1000 Consecutive Patients. J. Am. Coll. Surg. 2023, 237, 49–57. [Google Scholar] [CrossRef]
- Sell, N.M.; Fong, Z.V.; Del Castillo, C.F.; Qadan, M.; Warshaw, A.L.; Chang, D.; Lillemoe, K.D.; Ferrone, C.R. Staging Laparoscopy Not Only Saves Patients an Incision, But May Also Help Them Live Longer. Ann. Surg. Oncol. 2018, 25, 1009–1016. [Google Scholar] [CrossRef] [PubMed]
- Allen, V.B.; Gurusamy, K.S.; Takwoingi, Y.; Kalia, A.; Davidson, B.R. Diagnostic accuracy of laparoscopy following computed tomography (CT) scanning for assessing the resectability with curative intent in pancreatic and periampullary cancer. Cochrane Database Syst. Rev. 2016, 7, CD009323. [Google Scholar] [CrossRef] [PubMed]
- Merkow, R.P.; Bilimoria, K.Y.; Tomlinson, J.S.; Paruch, J.L.; Fleming, J.B.; Talamonti, M.S.; Ko, C.Y.; Bentrem, D.J. Postoperative complications reduce adjuvant chemotherapy use in resectable pancreatic cancer. Ann. Surg. 2014, 260, 372–377. [Google Scholar] [CrossRef] [PubMed]
- Sugimoto, M.; Takahashi, N.; Farnell, M.B.; Smyrk, T.C.; Truty, M.J.; Nagorney, D.M.; Smoot, R.L.; Chari, S.T.; Carter, R.E.; Kendrick, M.L. Survival benefit of neoadjuvant therapy in patients with non-metastatic pancreatic ductal adenocarcinoma: A propensity matching and intention-to-treat analysis. J. Surg. Oncol. 2019, 120, 976–984. [Google Scholar] [CrossRef]
- Heestand, G.M.; Murphy, J.D.; Lowy, A.M. Approach to patients with pancreatic cancer without detectable metastases. J. Clin. Oncol. 2015, 33, 1770–1778. [Google Scholar] [CrossRef] [PubMed]
- Cloyd, J.M.; Heh, V.; Pawlik, T.M.; Ejaz, A.; Dillhoff, M.; Tsung, A.; Williams, T.; Abushahin, L.; Bridges, J.F.P.; Santry, H. Neoadjuvant Therapy for Resectable and Borderline Resectable Pancreatic Cancer: A Meta-Analysis of Randomized Controlled Trials. J. Clin. Med. 2020, 9, 1129. [Google Scholar] [CrossRef] [PubMed]
- Versteijne, E.; Suker, M.; Groothuis, K.; Akkermans-Vogelaar, J.M.; Besselink, M.G.; Bonsing, B.A.; Buijsen, J.; Busch, O.R.; Creemers, G.M.; van Dam, R.M.; et al. Preoperative Chemoradiotherapy Versus Immediate Surgery for Resectable and Borderline Resectable Pancreatic Cancer: Results of the Dutch Randomized Phase III PREOPANC Trial. J. Clin. Oncol. 2020, 38, 1763–1773. [Google Scholar] [CrossRef]
- O’Reilly, E.M.; Ferrone, C. Neoadjuvant or Adjuvant Therapy for Resectable or Borderline Resectable Pancreatic Cancer: Which Is Preferred? J. Clin. Oncol. 2020, 38, 1757–1759. [Google Scholar] [CrossRef] [PubMed]
- Labori, K.J.; Bratlie, S.O.; Andersson, B.; Angelsen, J.H.; Biorserud, C.; Bjornsson, B.; Bringeland, E.A.; Elander, N.; Garresori, H.; Gronbech, J.E.; et al. Neoadjuvant FOLFIRINOX versus upfront surgery for resectable pancreatic head cancer (NORPACT-1): A multicentre, randomised, phase 2 trial. Lancet Gastroenterol. Hepatol. 2024, 9, 205–217. [Google Scholar] [CrossRef]
- Janssen, Q.P.; van Dam, J.L.; Bonsing, B.A.; Bos, H.; Bosscha, K.P.; Coene, P.; van Eijck, C.H.J.; de Hingh, I.; Karsten, T.M.; van der Kolk, M.B.; et al. Total neoadjuvant FOLFIRINOX versus neoadjuvant gemcitabine-based chemoradiotherapy and adjuvant gemcitabine for resectable and borderline resectable pancreatic cancer (PREOPANC-2 trial): Study protocol for a nationwide multicenter randomized controlled trial. BMC Cancer 2021, 21, 300. [Google Scholar] [CrossRef]
- Motoi, F.; Kosuge, T.; Ueno, H.; Yamaue, H.; Satoi, S.; Sho, M.; Honda, G.; Matsumoto, I.; Wada, K.; Furuse, J.; et al. Randomized phase II/III trial of neoadjuvant chemotherapy with gemcitabine and S-1 versus upfront surgery for resectable pancreatic cancer (Prep-02/JSAP05). Jpn. J. Clin. Oncol. 2019, 49, 190–194. [Google Scholar] [CrossRef] [PubMed]
- Ettrich, T.J.; Berger, A.W.; Perkhofer, L.; Daum, S.; Konig, A.; Dickhut, A.; Wittel, U.; Wille, K.; Geissler, M.; Algul, H.; et al. Neoadjuvant plus adjuvant or only adjuvant nab-paclitaxel plus gemcitabine for resectable pancreatic cancer—The NEONAX trial (AIO-PAK-0313), a prospective, randomized, controlled, phase II study of the AIO pancreatic cancer group. BMC Cancer 2018, 18, 1298. [Google Scholar] [CrossRef] [PubMed]
- Katz, M.H.G.; Shi, Q.; Meyers, J.; Herman, J.M.; Chuong, M.; Wolpin, B.M.; Ahmad, S.; Marsh, R.; Schwartz, L.; Behr, S.; et al. Efficacy of Preoperative mFOLFIRINOX vs mFOLFIRINOX Plus Hypofractionated Radiotherapy for Borderline Resectable Adenocarcinoma of the Pancreas: The A021501 Phase 2 Randomized Clinical Trial. JAMA Oncol. 2022, 8, 1263–1270. [Google Scholar] [CrossRef] [PubMed]
- Jethwa, K.R.; Sannapaneni, S.; Mullikin, T.C.; Harmsen, W.S.; Petersen, M.M.; Antharam, P.; Laughlin, B.; Mahipal, A.; Halfdanarson, T.R.; Merrell, K.W.; et al. Chemoradiotherapy for patients with locally advanced or unresectable extra-hepatic biliary cancer. J. Gastrointest. Oncol. 2020, 11, 1408–1420. [Google Scholar] [CrossRef] [PubMed]
- Neoptolemos, J.P.; Palmer, D.H.; Ghaneh, P.; Psarelli, E.E.; Valle, J.W.; Halloran, C.M.; Faluyi, O.; O’Reilly, D.A.; Cunningham, D.; Wadsley, J.; et al. Comparison of adjuvant gemcitabine and capecitabine with gemcitabine monotherapy in patients with resected pancreatic cancer (ESPAC-4): A multicentre, open-label, randomised, phase 3 trial. Lancet 2017, 389, 1011–1024. [Google Scholar] [CrossRef] [PubMed]
- Klein-Brill, A.; Amar-Farkash, S.; Lawrence, G.; Collisson, E.A.; Aran, D. Comparison of FOLFIRINOX vs Gemcitabine Plus Nab-Paclitaxel as First-Line Chemotherapy for Metastatic Pancreatic Ductal Adenocarcinoma. JAMA Netw. Open 2022, 5, e2216199. [Google Scholar] [CrossRef] [PubMed]
- Bilimoria, K.Y.; Bentrem, D.J.; Ko, C.Y.; Ritchey, J.; Stewart, A.K.; Winchester, D.P.; Talamonti, M.S. Validation of the 6th edition AJCC Pancreatic Cancer Staging System: Report from the National Cancer Database. Cancer 2007, 110, 738–744. [Google Scholar] [CrossRef] [PubMed]
- Demir, I.E.; Jager, C.; Schlitter, A.M.; Konukiewitz, B.; Stecher, L.; Schorn, S.; Tieftrunk, E.; Scheufele, F.; Calavrezos, L.; Schirren, R.; et al. R0 Versus R1 Resection Matters after Pancreaticoduodenectomy, and Less after Distal or Total Pancreatectomy for Pancreatic Cancer. Ann. Surg. 2018, 268, 1058–1068. [Google Scholar] [CrossRef] [PubMed]
- Regine, W.F.; Winter, K.A.; Abrams, R.A.; Safran, H.; Hoffman, J.P.; Konski, A.; Benson, A.B.; Macdonald, J.S.; Kudrimoti, M.R.; Fromm, M.L.; et al. Fluorouracil vs gemcitabine chemotherapy before and after fluorouracil-based chemoradiation following resection of pancreatic adenocarcinoma: A randomized controlled trial. JAMA 2008, 299, 1019–1026. [Google Scholar] [CrossRef]
- Oettle, H.; Neuhaus, P.; Hochhaus, A.; Hartmann, J.T.; Gellert, K.; Ridwelski, K.; Niedergethmann, M.; Zulke, C.; Fahlke, J.; Arning, M.B.; et al. Adjuvant chemotherapy with gemcitabine and long-term outcomes among patients with resected pancreatic cancer: The CONKO-001 randomized trial. JAMA 2013, 310, 1473–1481. [Google Scholar] [CrossRef]
- Maeda, S.; Moore, A.M.; Yohanathan, L.; Hata, T.; Truty, M.J.; Smoot, R.L.; Cleary, S.P.; Nagorney, D.M.; Grotz, T.E.; Park, E.J.; et al. Impact of resection margin status on survival in pancreatic cancer patients after neoadjuvant treatment and pancreatoduodenectomy. Surgery 2020, 167, 803–811. [Google Scholar] [CrossRef] [PubMed]
- Neoptolemos, J.P.; Stocken, D.D.; Friess, H.; Bassi, C.; Dunn, J.A.; Hickey, H.; Beger, H.; Fernandez-Cruz, L.; Dervenis, C.; Lacaine, F.; et al. A randomized trial of chemoradiotherapy and chemotherapy after resection of pancreatic cancer. N. Engl. J. Med. 2004, 350, 1200–1210. [Google Scholar] [CrossRef] [PubMed]
- Gillen, S.; Schuster, T.; Meyer Zum Buschenfelde, C.; Friess, H.; Kleeff, J. Preoperative/neoadjuvant therapy in pancreatic cancer: A systematic review and meta-analysis of response and resection percentages. PLoS Med. 2010, 7, e1000267. [Google Scholar] [CrossRef] [PubMed]
- Khan, A.Z.; Smith, A.M.; Irving, G.R.; Cameron, I. Portal vein resection during pancreaticoduodenectomy for cancer. Ann. R. Coll. Surg. Engl. 2009, 91, 95–99. [Google Scholar] [CrossRef] [PubMed]
- Fuhrman, G.M.; Leach, S.D.; Staley, C.A.; Cusack, J.C.; Charnsangavej, C.; Cleary, K.R.; El-Naggar, A.K.; Fenoglio, C.J.; Lee, J.E.; Evans, D.B. Rationale for en bloc vein resection in the treatment of pancreatic adenocarcinoma adherent to the superior mesenteric-portal vein confluence. Pancreatic Tumor Study Group. Ann. Surg. 1996, 223, 154–162. [Google Scholar] [CrossRef] [PubMed]
- Yekebas, E.F.; Bogoevski, D.; Cataldegirmen, G.; Kunze, C.; Marx, A.; Vashist, Y.K.; Schurr, P.G.; Liebl, L.; Thieltges, S.; Gawad, K.A.; et al. En bloc vascular resection for locally advanced pancreatic malignancies infiltrating major blood vessels: Perioperative outcome and long-term survival in 136 patients. Ann. Surg. 2008, 247, 300–309. [Google Scholar] [CrossRef] [PubMed]
- Giovinazzo, F.; Turri, G.; Katz, M.H.; Heaton, N.; Ahmed, I. Meta-analysis of benefits of portal-superior mesenteric vein resection in pancreatic resection for ductal adenocarcinoma. Br. J. Surg. 2016, 103, 179–191. [Google Scholar] [CrossRef] [PubMed]
- Diener, M.K.; Mihaljevic, A.L.; Strobel, O.; Loos, M.; Schmidt, T.; Schneider, M.; Berchtold, C.; Mehrabi, A.; Muller-Stich, B.P.; Jiang, K.; et al. Periarterial divestment in pancreatic cancer surgery. Surgery 2021, 169, 1019–1025. [Google Scholar] [CrossRef] [PubMed]
- Cai, B.; Lu, Z.; Neoptolemos, J.P.; Diener, M.K.; Li, M.; Yin, L.; Gao, Y.; Wei, J.; Chen, J.; Guo, F.; et al. Sub-adventitial divestment technique for resecting artery-involved pancreatic cancer: A retrospective cohort study. Langenbecks Arch. Surg. 2021, 406, 691–701. [Google Scholar] [CrossRef]
- Evans, D.B.; Varadhachary, G.R.; Crane, C.H.; Sun, C.C.; Lee, J.E.; Pisters, P.W.; Vauthey, J.N.; Wang, H.; Cleary, K.R.; Staerkel, G.A.; et al. Preoperative gemcitabine-based chemoradiation for patients with resectable adenocarcinoma of the pancreatic head. J. Clin. Oncol. 2008, 26, 3496–3502. [Google Scholar] [CrossRef]
- Barnes, C.A.; Chavez, M.I.; Tsai, S.; Aldakkak, M.; George, B.; Ritch, P.S.; Dua, K.; Clarke, C.N.; Tolat, P.; Hagen, C.; et al. Survival of patients with borderline resectable pancreatic cancer who received neoadjuvant therapy and surgery. Surgery 2019, 166, 277–285. [Google Scholar] [CrossRef] [PubMed]
- Del Chiaro, M.; Rangelova, E.; Halimi, A.; Ateeb, Z.; Scandavini, C.; Valente, R.; Segersvard, R.; Arnelo, U.; Verbeke, C.S. Pancreatectomy with arterial resection is superior to palliation in patients with borderline resectable or locally advanced pancreatic cancer. HPB 2019, 21, 219–225. [Google Scholar] [CrossRef] [PubMed]
- Sonohara, F.; Yamada, S.; Takami, H.; Hayashi, M.; Kanda, M.; Tanaka, C.; Kobayashi, D.; Nakayama, G.; Koike, M.; Fujiwara, M.; et al. Novel implications of combined arterial resection for locally advanced pancreatic cancer in the era of newer chemo-regimens. Eur. J. Surg. Oncol. 2019, 45, 1895–1900. [Google Scholar] [CrossRef] [PubMed]
- Abrams, R.A.; Lowy, A.M.; O’Reilly, E.M.; Wolff, R.A.; Picozzi, V.J.; Pisters, P.W. Combined modality treatment of resectable and borderline resectable pancreas cancer: Expert consensus statement. Ann. Surg. Oncol. 2009, 16, 1751–1756. [Google Scholar] [CrossRef] [PubMed]
- Thalji, S.Z.; Aldakkak, M.; Christians, K.K.; Clarke, C.N.; George, B.; Kamgar, M.; Erickson, B.A.; Hall, W.A.; Chisholm, P.; Kulkarni, N.; et al. Neoadjuvant chemotherapy for pancreatic cancer: Quality over quantity. J. Surg. Oncol. 2023, 128, 41–50. [Google Scholar] [CrossRef]
- Hackert, T.; Sachsenmaier, M.; Hinz, U.; Schneider, L.; Michalski, C.W.; Springfeld, C.; Strobel, O.; Jager, D.; Ulrich, A.; Buchler, M.W. Locally Advanced Pancreatic Cancer: Neoadjuvant Therapy with Folfirinox Results in Resectability in 60% of the Patients. Ann. Surg. 2016, 264, 457–463. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Muaddi, H.; Kearse, L.; Warner, S. Multimodal Approaches to Patient Selection for Pancreas Cancer Surgery. Curr. Oncol. 2024, 31, 2260-2273. https://doi.org/10.3390/curroncol31040167
Muaddi H, Kearse L, Warner S. Multimodal Approaches to Patient Selection for Pancreas Cancer Surgery. Current Oncology. 2024; 31(4):2260-2273. https://doi.org/10.3390/curroncol31040167
Chicago/Turabian StyleMuaddi, Hala, LaDonna Kearse, and Susanne Warner. 2024. "Multimodal Approaches to Patient Selection for Pancreas Cancer Surgery" Current Oncology 31, no. 4: 2260-2273. https://doi.org/10.3390/curroncol31040167
APA StyleMuaddi, H., Kearse, L., & Warner, S. (2024). Multimodal Approaches to Patient Selection for Pancreas Cancer Surgery. Current Oncology, 31(4), 2260-2273. https://doi.org/10.3390/curroncol31040167