
Cerebral Circulation and Brain Temperature during an Ultra-Short Session of Dry Immersion in Young Subjects

 ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. The DI Session
2.3. Outcome Measures
2.4. Statistical Analysis
3. Results
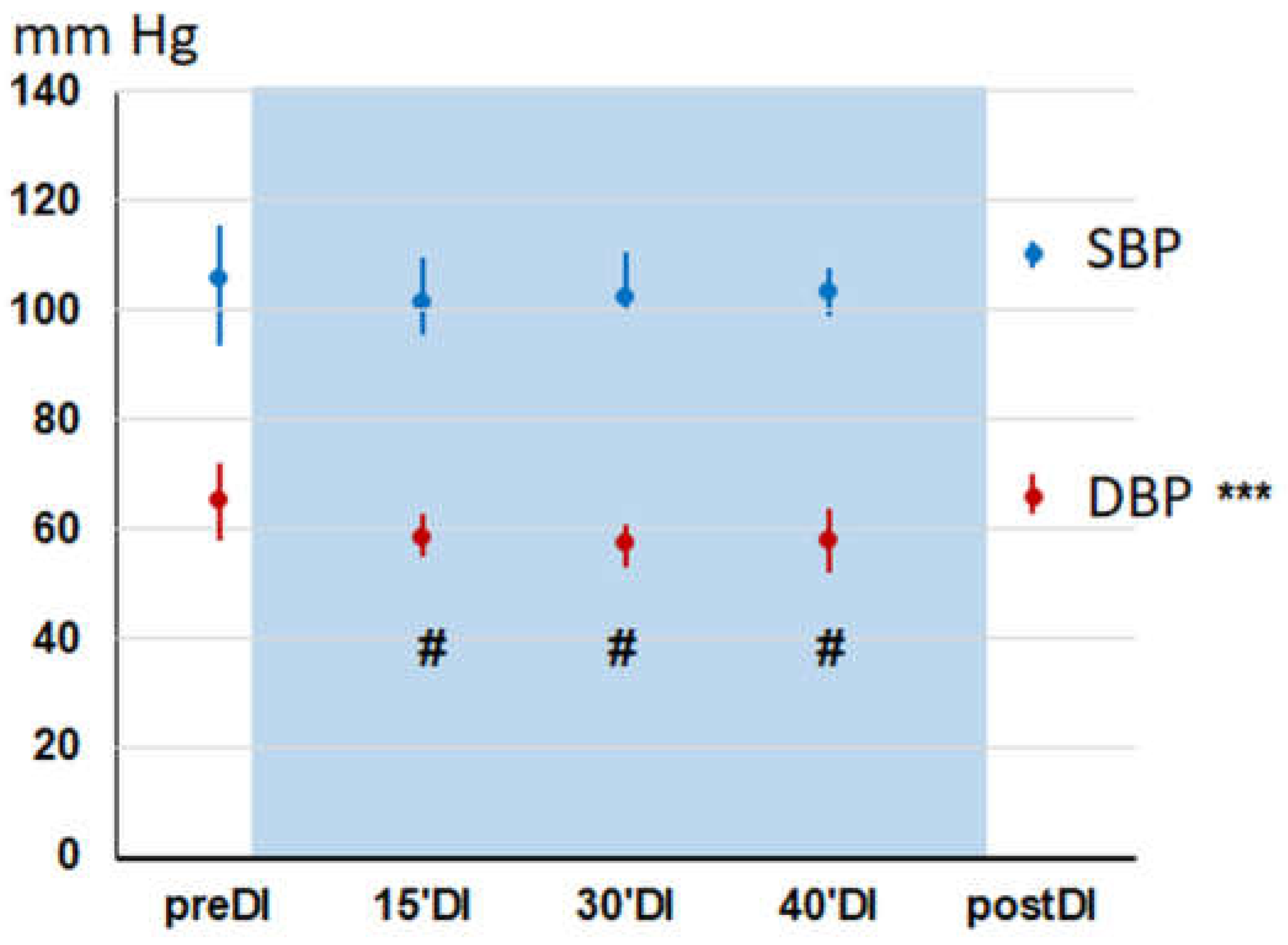
3.1. Hemodynamics during a DI Session
3.2. LDF Measurements in the Forehead Supraorbital Area during a DI Session
3.3. LDF Measurements in the Forearm Area during a DI Session
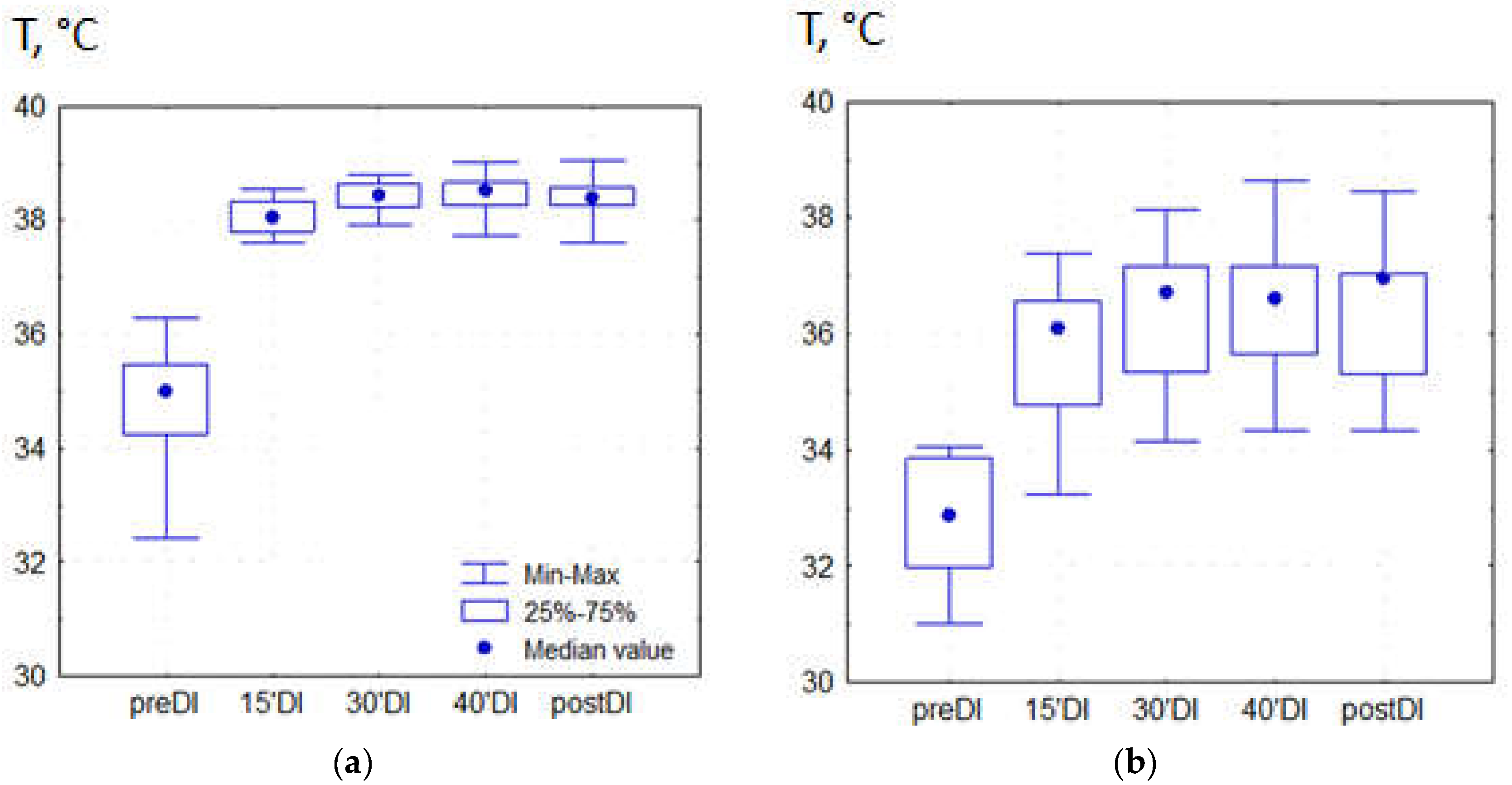
3.4. Temperature Measurements during a DI Session
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kermorgant, M.; Nasr, N.; Czosnyka, M.; Arvanitis, D.N.; Hélissen, O.; Senard, J.M.; Pavy-Le Traon, A. Impacts of Microgravity Analogs to Spaceflight on Cerebral Autoregulation. Front. Physiol. 2020, 11, 778. [Google Scholar] [CrossRef] [PubMed]
- Pandiarajan, M.; Hargens, A.R. Ground-Based Analogs for Human Spaceflight. Front. Physiol. 2020, 11, 716. [Google Scholar] [CrossRef] [PubMed]
- Watenpaugh, D.E. Analogs of microgravity: Head-down tilt and water immersion. J. Appl. Physiol. 2016, 120, 904–914. [Google Scholar] [CrossRef] [PubMed]
- Tomilovskaya, E.; Shigueva, T.; Sayenko, D.; Rukavishnikov, I.; Kozlovskaya, I. Dry Immersion as a Ground-Based Model of Microgravity Physiological Effects. Front. Physiol. 2019, 10, 284. [Google Scholar] [CrossRef] [PubMed]
- Demontis, G.C.; Germani, M.M.; Caiani, E.G.; Barravecchia, I.; Passino, C.; Angeloni, D. Human Pathophysiological Adaptations to the Space Environment. Front. Physiol. 2017, 8, 547. [Google Scholar] [CrossRef]
- Jirak, P.; Mirna, M.; Rezar, R.; Motloch, L.J.; Lichtenauer, M.; Jordan, J.; Binneboessel, S.; Tank, J.; Limper, U.; Jung, C. How spaceflight challenges human cardiovascular health. Eur. J. Prev. Cardiol. 2022, 29, 1399–1411. [Google Scholar] [CrossRef] [PubMed]
- Liphardt, A.M.; Fernandez-Gonzalo, R.; Albracht, K.; Rittweger, J.; Vico, L. Musculoskeletal research in human space flight—unmet needs for the success of crewed deep space exploration. NPJ Microgravity 2023, 9, 9. [Google Scholar] [CrossRef]
- Navasiolava, N.M.; Custaud, M.A.; Tomilovskaya, E.S.; Larina, I.M.; Mano, T.; Gauquelin-Koch, G.; Gharib, C.; Kozlovskaya, I.B. Long-term dry immersion: Review and prospects. Eur. J. Appl. Physiol. 2011, 111, 1235–1260. [Google Scholar] [CrossRef]
- Demangel, R.; Treffel, L.; Py, G.; Brioche, T.; Pagano, A.F.; Bareille, M.-P.; Beck, A.; Pessemesse, L.; Candau, R.; Gharib, C.; et al. Early structural and functional signature of 3-day human skeletal muscle disuse using the dry immersion model. J. Physiol. 2017, 595, 4301–4315. [Google Scholar] [CrossRef]
- Treffel, L.; Dmitrieva, L.; Gauquelin-Koch, G.; Custaud, M.A.; Blanc, S.; Gharib, C.; Millet, C. Craniomandibular System and Postural Balance after 3-Day Dry Immersion. PLoS ONE 2016, 11, e0150052. [Google Scholar] [CrossRef]
- Genin, A.M.; Modin, A.; Shashkov, V.S. Status of human hemodynamics during water immersion in different postures of immersion. Kosm. Biol. Aviakosm. Med. 1988, 22, 7–10. [Google Scholar] [PubMed]
- Arbeille, P.; Avan, P.; Treffel, L.; Zuj, K.; Normand, H.; Denise, P. Jugular and Portal Vein Volume, Middle Cerebral Vein Velocity, and Intracranial Pressure in Dry Immersion. Aerosp. Med. Hum. Perform. 2017, 88, 457–462. [Google Scholar] [CrossRef] [PubMed]
- Gerasimova-Meigal, L.; Meigal, A.; Sireneva, N.; Saenko, I. Autonomic Function in Parkinson’s Disease Subjects across Repeated Short-Term Dry Immersion: Evidence from Linear and Non-linear HRV Parameters. Front. Physiol. 2021, 12, 712365. [Google Scholar] [CrossRef] [PubMed]
- Gerasimova-Meigal, L.; Meigal, A.; Sireneva, N.; Gerasimova, M.; Sklyarova, A. Heart Rate Variability Parameters to Evaluate Autonomic Functions in Healthy Young Subjects during Short-Term “Dry” Immersion. Physiologia 2023, 3, 119–128. [Google Scholar] [CrossRef]
- Meigal, A.Y.; Tretjakova, O.G.; Gerasimova-Meigal, L.I.; Sayenko, I.V. Program of seven 45-min dry immersion sessions improves choice reaction time in Parkinson’s disease. Front. Physiol. 2021, 11, 621198. [Google Scholar] [CrossRef]
- Ogoh, S.; Hirasawa, A.; de Abreu, S.; Denise, P.; Normand, H. Internal carotid, external carotid and vertebral artery blood flow responses to 3 days of head-out dry immersion. Exp. Physiol. 2017, 102, 1278–1287. [Google Scholar] [CrossRef]
- Ogoh, S.; Sato, K.; de Abreu, S.; Denise, P.; Normand, H. Arterial and venous cerebral blood flow responses to long-term head-down bed rest in male volunteers. Exp. Physiol. 2020, 105, 44–52. [Google Scholar] [CrossRef]
- Du, J.; Cui, J.; Yang, J.; Wang, P.; Zhang, L.; Luo, B.; Han, B. Alterations in Cerebral Hemodynamics During Microgravity: A Literature Review. Med. Sci. Monit. 2021, 27, e928108. [Google Scholar] [CrossRef]
- Guillon, L.; Kermorgant, M.; Charvolin, T.; Bonneville, F.; Bareille, M.-P.; Cassol, E.; Beck, A.; Beaurain, M.; Péran, P.; Lotterie, J.-A.; et al. Reduced Regional Cerebral Blood Flow Measured by 99mTc-Hexamethyl Propylene Amine Oxime Single-Photon Emission Computed Tomography in Microgravity Simulated by 5-Day Dry Immersion. Front. Physiol. 2021, 12, 789298. [Google Scholar] [CrossRef]
- Yulug, B.; Velioglu, H.A.; Sayman, D.; Cankaya, S.; Hanoglu, L. Brain temperature in healthy and diseased conditions: A review on the special implications of MRS for monitoring brain temperature. Biomed. Pharmacother. 2023, 160, 114287. [Google Scholar] [CrossRef]
- Ball, D. Contrasting effects of heat stress on neuromuscular performance. Exp. Physiol. 2021, 106, 2328–2334. [Google Scholar] [CrossRef] [PubMed]
- Nybo, L. Hyperthermia and fatigue. J. Appl. Physiol. 2008, 104, 871–878. [Google Scholar] [CrossRef] [PubMed]
- Périard, J.D. Hyperthermia and supraspinal fatigue. Exp. Physiol. 2016, 101, 1323–1324. [Google Scholar] [CrossRef] [PubMed]
- Todd, G.; Butler, J.E.; Taylor, J.L.; Gandevia, S.C. Hyperthermia: A failure of the motor cortex and the muscle. J. Physiol. 2005, 563 Pt 2, 621–631. [Google Scholar] [CrossRef]
- Tucker, R.; Rauch, L.; Harley, Y.X.; Noakes, T.D. Impaired exercise performance in the heat is associated with an anticipatory reduction in skeletal muscle recruitment. Pflugers Arch. 2004, 448, 422–430. [Google Scholar] [CrossRef]
- Meigal, A.; Gerasimova-Meigal, L. Cold for gravity, heat for microgravity: A critical analysis of the “Baby Astronaut” concept. Front. Space Technol. 2022, 3, 981668. [Google Scholar] [CrossRef]
- Mauritzon, S.; Ginstman, F.; Hillman, J.; Wårdell, K. Analysis of laser Doppler flowmetry long-term recordings for investigation of cerebral microcirculation during neurointensive care. Front. Neurosci. 2022, 16, 1030805. [Google Scholar] [CrossRef]
- Gerasimova-Meigal, L.I.; Sireneva, N.V.; Meigal, A.Y. Estimation of the effect of the course of short-term sessions “dry” immersion on autonomic regulation in patients with parkinsonism. Hum. Physiol. 2021, 47, 51–57. [Google Scholar] [CrossRef]
- Sidorov, V.V.; Rybakov, Y.L.; Gukasov, V.M.; Evtushenko, G.S. A Device for Comprehensive Noninvasive Diagnostics of the Tissue Microcirculation System of Human Skin. Biomed. Eng. 2021, 4, 232–235. [Google Scholar] [CrossRef]
- Fedorovich, A.A.; Loktionova, Y.I.; Zharkikh, E.V.; Gorshkov, A.Y.; Korolev, A.I.; Dadaeva, V.A.; Drapkina, O.M.; Zherebtsov, E.A. Skin microcirculation in middle-aged men with newly diagnosed arterial hypertension according to remote laser Doppler flowmetry data. Microvasc. Res. 2022, 144, 104419. [Google Scholar] [CrossRef]
- Anisimova, A.V.; Krupatkin, A.I.; Sidorov, V.V.; Zacharkina, M.V.; Yutskova, E.V.; Galkin, S.S. Laser Doppler flowmetry in the assessment of the microcirculation in patients with acute and chronic cerebrovascular insufficiency. Reg. Krovoobrashhenie I Mikrocirk. 2014, 3, 31–37. [Google Scholar]
- Goltsov, A.; Anisimova, A.V.; Zakharkina, M.; Krupatkin, A.I.; Sidorov, V.V.; Sokolovski, S.G.; Rafailov, E. Bifurcation in Blood Oscillatory Rhythms for Patients with Ischemic Stroke: A Small Scale Clinical Trial using Laser Doppler Flowmetry and Computational Modeling of Vasomotion. Front. Physiol. 2017, 8, 160. [Google Scholar] [CrossRef] [PubMed]
- Seiyama, A.; Miura, T.; Sasaki, Y.; Okahashi, S.; Konishi, N.; Cassim, M. Characterization of forehead blood flow bias on NIRS signals during neural activation with a verbal fluency task. Neurosci. Res. 2023, 186, 43–50. [Google Scholar] [CrossRef] [PubMed]
- Krupatkin, A.I. Evaluation of the parameters of total, nutritive, and shunt blood flows in the skin microvasculature using laser Doppler flowmetry. Hum. Physiol. 2005, 31, 98–102. [Google Scholar] [CrossRef]
- Krupatkin, A.I.; Sidorov, V.V. Laser Doppler Flowmetry of Blood Microcirculation: A Guide for Doctors; Medicina: Moscow, Russia, 2005; p. 256. [Google Scholar]
- Saha, M.; Dremin, V.; Rafailov, I.; Dunaev, A.; Sokolovski, S.; Rafailov, E. Wearable Laser Doppler Flowmetry Sensor: A Feasibility Study with Smoker and Non-Smoker Volunteers. Biosensors 2020, 10, 201. [Google Scholar] [CrossRef] [PubMed]
- Navasiolava, N.; Yuan, M.; Murphy, R.; Robin, A.; Coupé, M.; Wang, L.; Alameddine, A.; Gauquelin-Koch, G.; Gharib, C.; Li, Y.; et al. Vascular and microvascular dysfunction induced by microgravity and its analogs in humans: Mechanisms and countermeasures. Front. Physiol. 2020, 11, 952. [Google Scholar] [CrossRef] [PubMed]
- Bernjak, A.; Stefanovska, A. Importance of wavelet analysis in laser Doppler flowmetry time series. Annu. Int. Conf. IEEE Eng. Med. Biol. Soc. 2007, 2007, 4064–4067. [Google Scholar] [CrossRef]
- Kralj, L.; Lenasi, H. Wavelet analysis of laser Doppler microcirculatory signals: Current applications and limitations. Front. Physiol. 2023, 13, 1076445. [Google Scholar] [CrossRef]
- Tansey, E.A.; Johnson, C.D. Recent advances in thermoregulation. Adv. Physiol. Educ. 2015, 39, 139–148. [Google Scholar] [CrossRef]
- Rzechorzek, N.M.; Thrippleton, M.J.; Chappell, F.M.; Mair, G.; Ercole, A.; Cabeleira, M.; Rhodes, J.; Marshall, I.; O’neill, J.S. A daily temperature rhythm in the human brain predicts survival after brain injury. Brain 2022, 145, 2031–2048. [Google Scholar] [CrossRef]
- Schwenke, M.; Strehlow, J.; Demedts, D.; Haase, S.; Romero, D.B.; Rothlübbers, S.; von Dresky, C.; Zidowitz, S.; Georgii, J.; Mihcin, S.; et al. A focused ultrasound treatment system for moving targets (part I): Generic system design and in-silico first-stage evaluation. J. Ther. Ultrasound. 2017, 5, 20. [Google Scholar] [CrossRef] [PubMed]
- Gulias-Cañizo, R.; Rodríguez-Malagón, M.E.; Botello-González, L.; Belden-Reyes, V.; Amparo, F.; Garza-Leon, M. Applications of Infrared Thermography in Ophthalmology. Life 2023, 13, 723. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Parameter | Men (n = 4) | Women (n = 7) |
|---|---|---|
| Body Mass, kg | 72.3 ± 3.4 | 57.9 ± 6.4 |
| Height, m | 1.81 ± 0.03 | 1.67 ± 0.05 |
| BMI 1 | 22.1 ± 0.7 | 20.7 ± 2.7 |
| Parameter | PreDI | 15′DI | 30′DI | 30′DI | PostDI | Significance 1 |
|---|---|---|---|---|---|---|
| M, p.u. | 15.14 ± 4.58 | 18.48 ± 4.22 | 18.45 ± 3.95 * | 19.01 ± 4.68 | 18.45 ± 4.59 * | 0.064 |
| MNUTR, p.u. | 6.66 ± 3.31 | 8.66 ± 3.67 | 7.74 ± 3.67 | 9.07 ± 3.28 | 9.48 ± 4.33 | 0.153 |
| MSHUNT, p.u. | 8.48 ± 3.95 | 9.81 ± 4.30 | 10.71 ± 3.42 | 9.95 ± 2.85 | 9.00 ± 4.64 | 0.440 |
| σ, p.u. | 1.55 ± 0.455 | 1.59 ± 0.42 | 1.69 ± 0.32 | 1.53 ± 0.28 | 1.61 ± 0.42 | 0.703 |
| KV | 10.68 ± 3.23 | 8.87 ± 2.61 | 9.47 ± 2.14 | 8.55 ± 2.76 | 8.96 ± 2.12 | 0.117 |
| AE, W2 | 0.43 ± 0.17 | 0.36 ± 0.30 | 0.41 ± 0.18 | 0.31 ± 0.14 | 0.37 ± 0.21 | 0.475 |
| AN, W2 | 0.47 ± 0.15 | 0.40 ± 0.22 | 0.59 ± 0.23 | 0.47 ± 0.18 | 0.48 ± 0.18 | 0.048 |
| AM, W2 | 0.54 ± 0.22 | 0.66 ± 0.31 | 0.65 ± 0.22 | 0.69 ± 0.21 | 0.76 ± 0.32 | 0.177 |
| AR, W2 | 0.34 ± 0.11 | 0.48 ± 0.17 * | 0.48 ± 0.13 * | 0.47 ± 0.14 ** | 0.51 ± 0.19 ** | 0.008 |
| AC, W2 | 0.82 ± 0.30 | 1.023 ± 0.29 | 1.06 ± 0.26 | 1.02 ± 0.25 | 1.06 ± 0.36 | 0.075 |
| T, °C | 34.84 ± 1.04 | 38.05 ± 0.31 *** | 38.40 ± 0.26 *** | 38.45 ± 0.32 *** | 38.36 ± 0.35 *** | 0.000 |
| Parameter | PreDI | 15′DI | 30′DI | 30′DI | PostDI | Significance 1 |
|---|---|---|---|---|---|---|
| M, p.u. | 4.46 ± 1.08 | 6.94 ± 2.71 | 8.56 ± 4.48 ** | 9.50 ± 5.33 ** | 8.69 ± 3.35 * | 0.005 |
| MNUTR, p.u. | 2.39 ± 1.71 | 3.47 ± 1.69 | 5.10 ± 4.30 * | 5.41 ± 3.84 | 5.23 ± 2.71 | 0.038 |
| MSHUNT, p.u. | 1.31 ± 0.83 | 2.68 ± 0.94 | 3.01 ± 1.91 | 3.38 ± 1.97 | 3.04 ± 1.57 | 0.241 |
| σ, p.u. | 0.43 ± 0.10 | 0.59 ± 0.36 | 0.84 ± 0.57 * | 0.76 ± 0.46 | 0.70 ± 0.36 | 0.067 |
| KV | 9.78 ± 2.13 | 8.32 ± 1.66 | 9.71 ± 3.21 | 8.24 ± 3.49 | 8.07 ± 2.00 | 0.205 |
| AE, W2 | 0.16 ± 0.15 | 0.14 ± 0.11 | 0.19 ± 0.12 | 0.15 ± 0.14 | 0.17 ± 0.09 | 0.789 |
| AN, W2 | 0.18 ± 0.11 | 0.22 ± 0.17 | 0.25 ± 0.18 | 0.26 ± 0.22 | 0.19 ± 0.09 | 0.593 |
| AM, W2 | 0.20 ± 0.09 | 0.26 ± 0.13 | 0.39 ± 0.38 | 0.36 ± 0.26 | 0.34 ± 0.19 | 0.178 |
| AR, W2 | 0.13 ± 0.06 | 0.17 ± 0.08 | 0.22 ± 0.12 * | 0.23 ± 0.12 | 0.22 ± 0.10 | 0.047 |
| AC, W2 | 0.20 ± 0.05 | 0.34 ± 0.20 | 0.40 ± 0.26 | 0.38 ± 0.21 * | 0.39 ± 0.25 | 0.067 |
| T, °C | 32.74 ± 1.12 | 35.75 ± 1.25 *** | 36.36 ± 1.18 *** | 36.44 ± 1.17 *** | 36.42 ± 1.18 *** | 0.000 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gerasimova-Meigal, L.; Meigal, A.; Gerasimova, M.; Sklyarova, A.; Sirotinina, E. Cerebral Circulation and Brain Temperature during an Ultra-Short Session of Dry Immersion in Young Subjects. Pathophysiology 2023, 30, 209-218. https://doi.org/10.3390/pathophysiology30020018
Gerasimova-Meigal L, Meigal A, Gerasimova M, Sklyarova A, Sirotinina E. Cerebral Circulation and Brain Temperature during an Ultra-Short Session of Dry Immersion in Young Subjects. Pathophysiology. 2023; 30(2):209-218. https://doi.org/10.3390/pathophysiology30020018
Chicago/Turabian StyleGerasimova-Meigal, Liudmila, Alexander Meigal, Maria Gerasimova, Anna Sklyarova, and Ekaterina Sirotinina. 2023. "Cerebral Circulation and Brain Temperature during an Ultra-Short Session of Dry Immersion in Young Subjects" Pathophysiology 30, no. 2: 209-218. https://doi.org/10.3390/pathophysiology30020018
APA StyleGerasimova-Meigal, L., Meigal, A., Gerasimova, M., Sklyarova, A., & Sirotinina, E. (2023). Cerebral Circulation and Brain Temperature during an Ultra-Short Session of Dry Immersion in Young Subjects. Pathophysiology, 30(2), 209-218. https://doi.org/10.3390/pathophysiology30020018