
Trends in Drug Tests among Children: A 22-Year Retrospective Analysis


 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Dataset
2.2. Data Sources and Analysis
3. Results
3.1. Demographic Characteristics
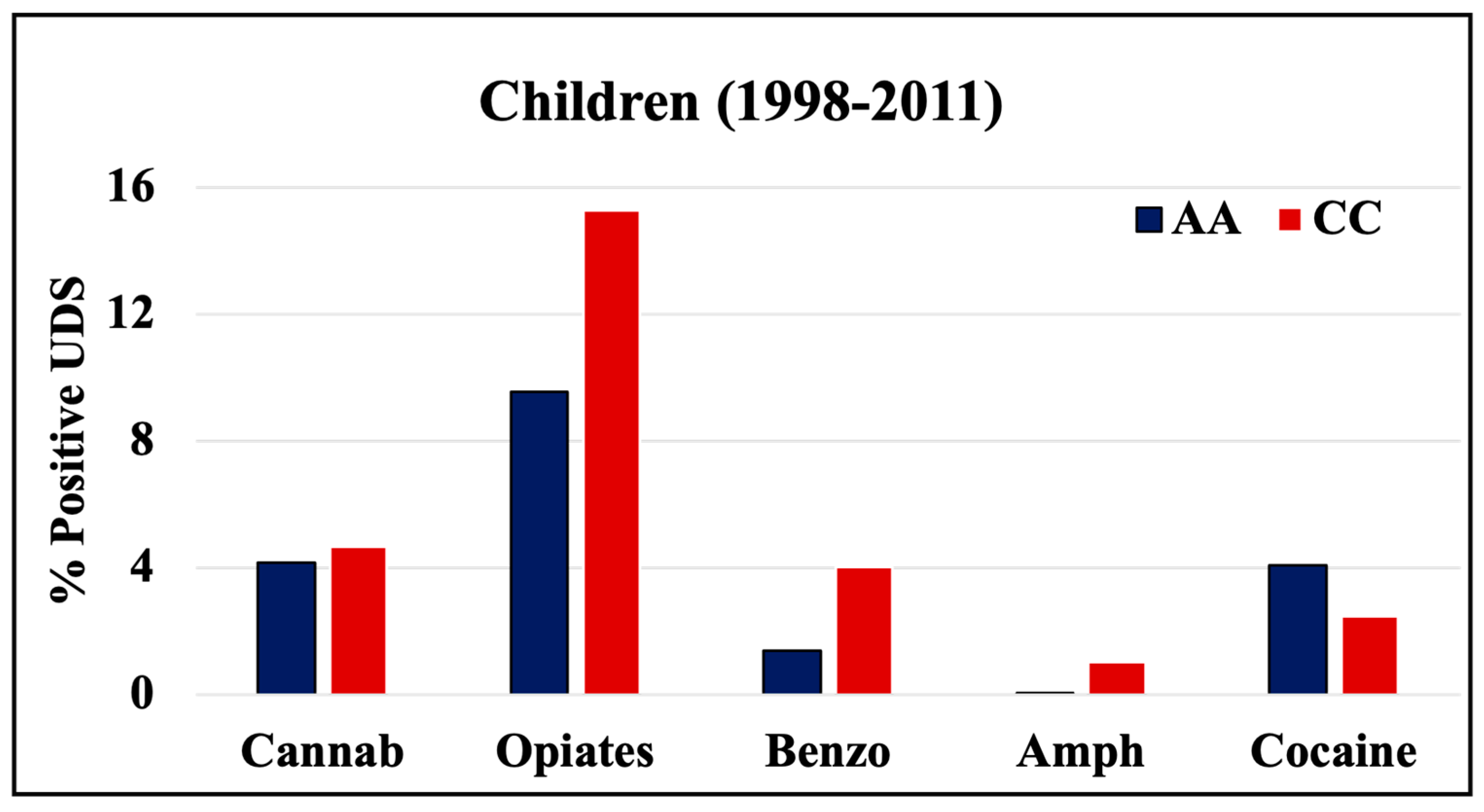
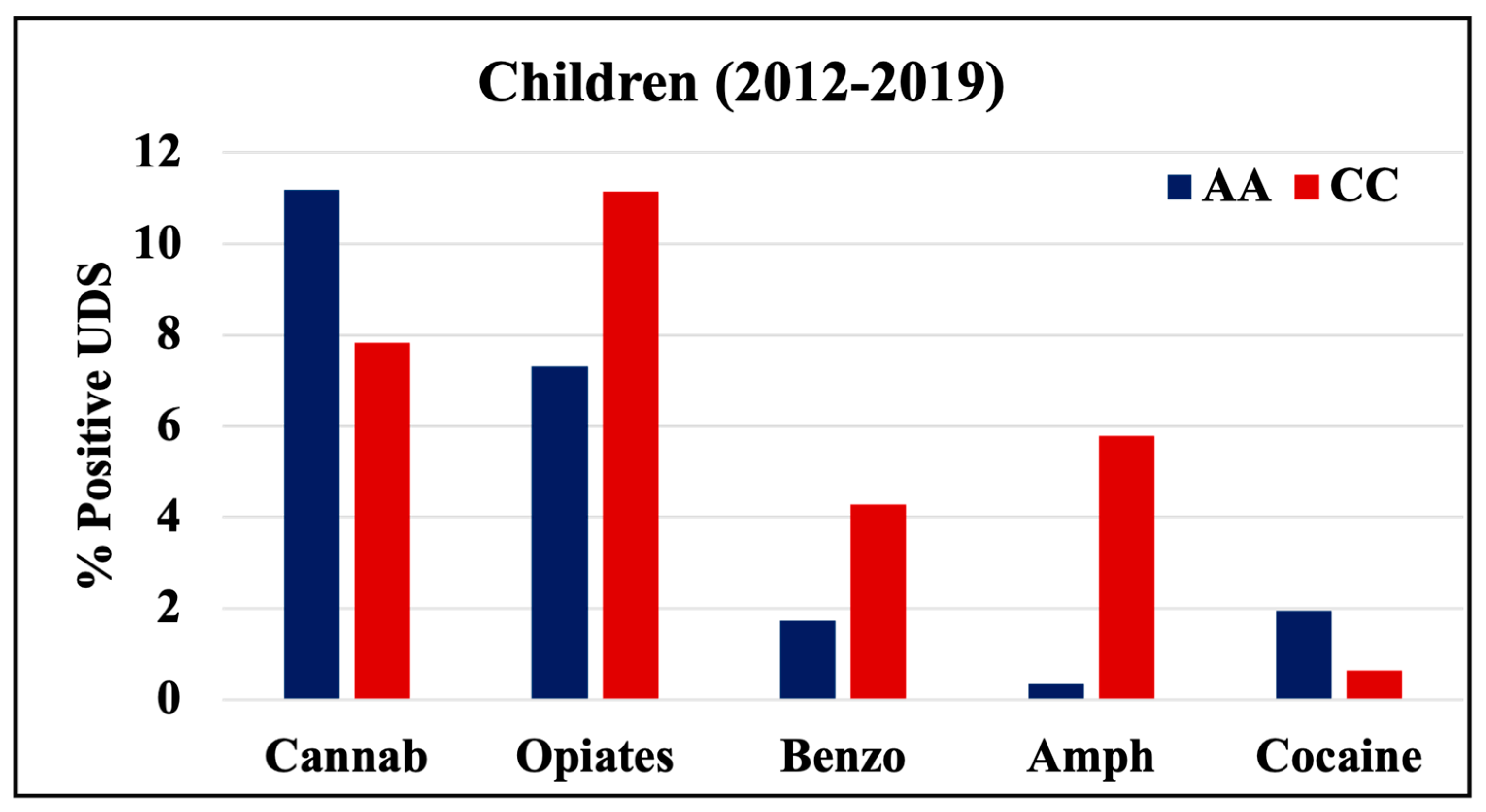
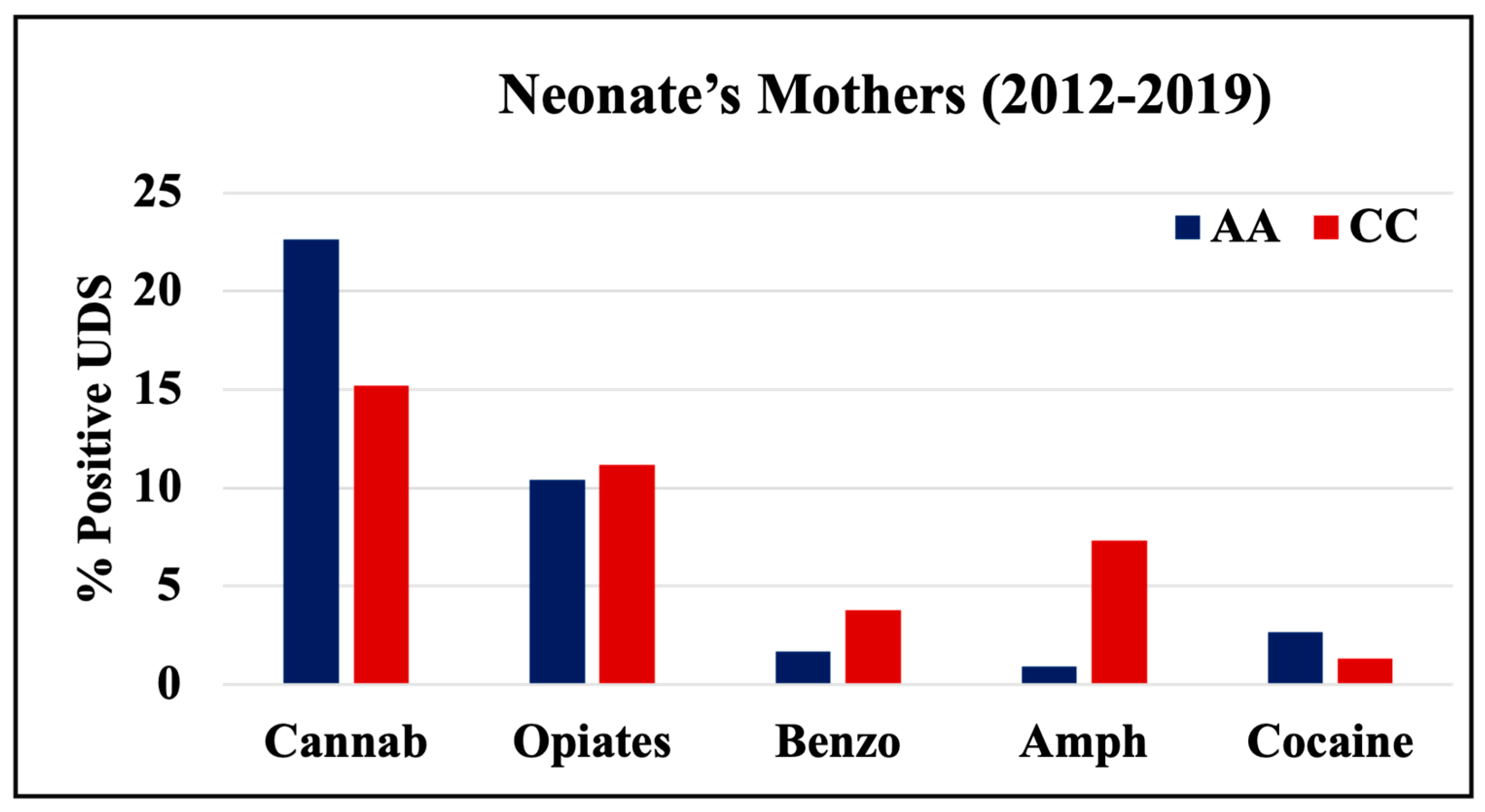
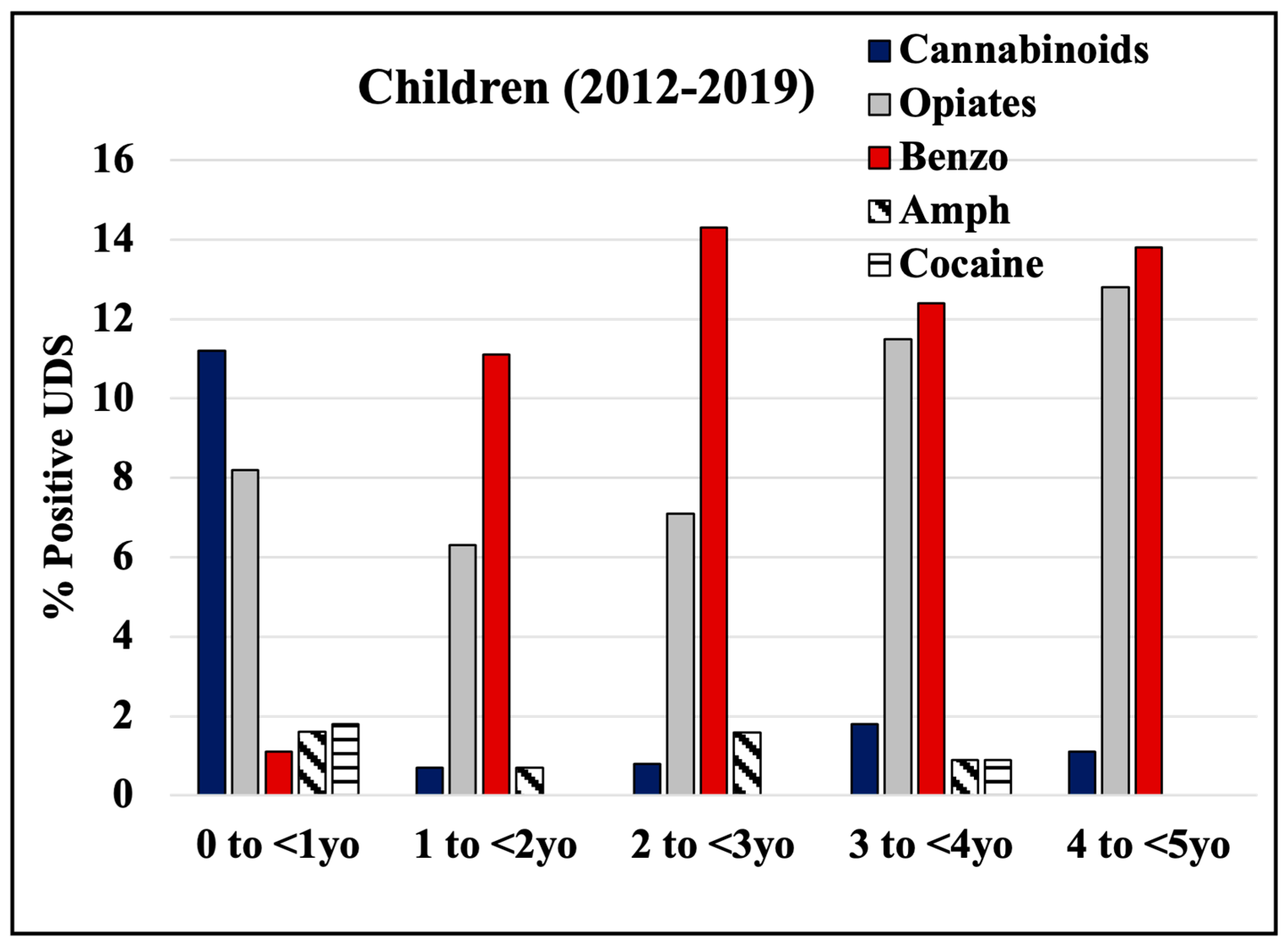
3.2. Drug Screen Results
3.3. Trends in Positive UDS Results
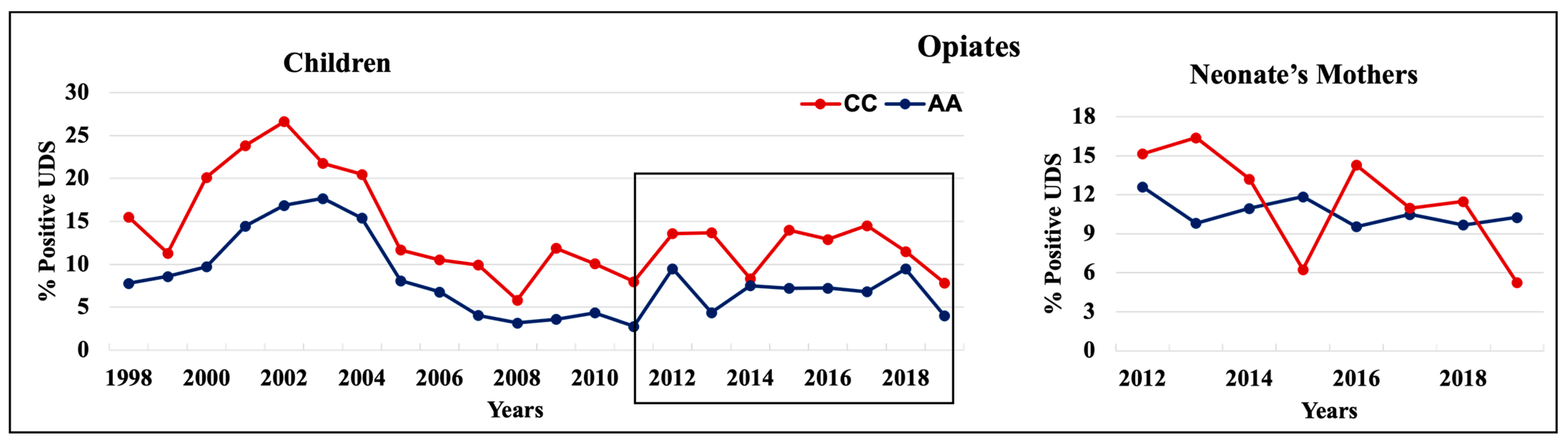
3.3.1. Opiates
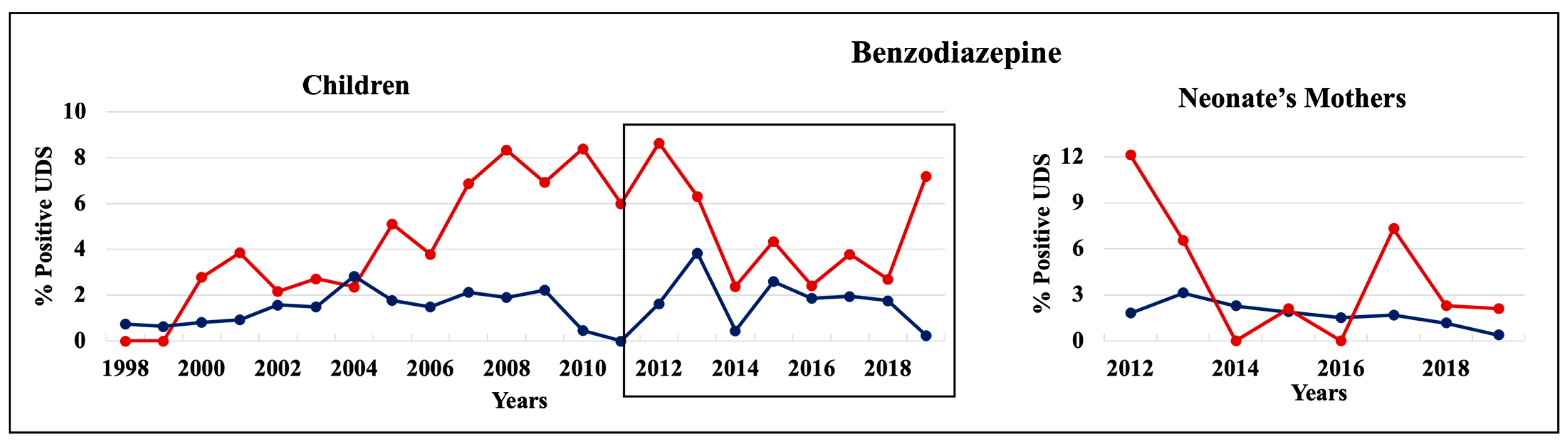
3.3.2. Benzodiazepine
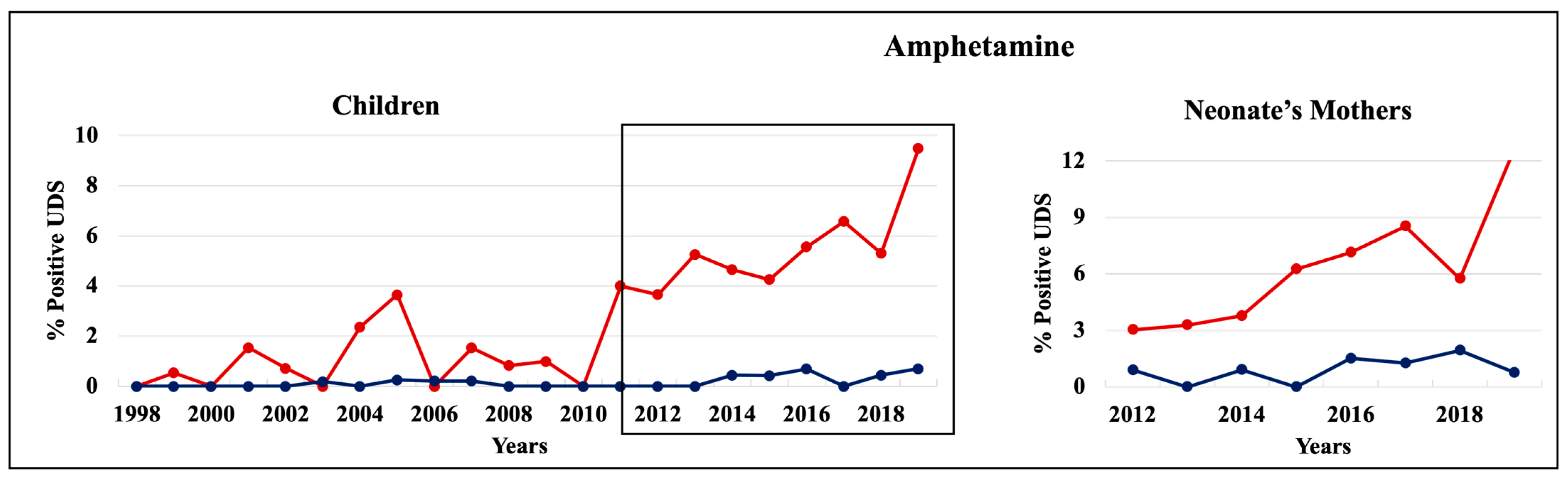
3.3.3. Amphetamine
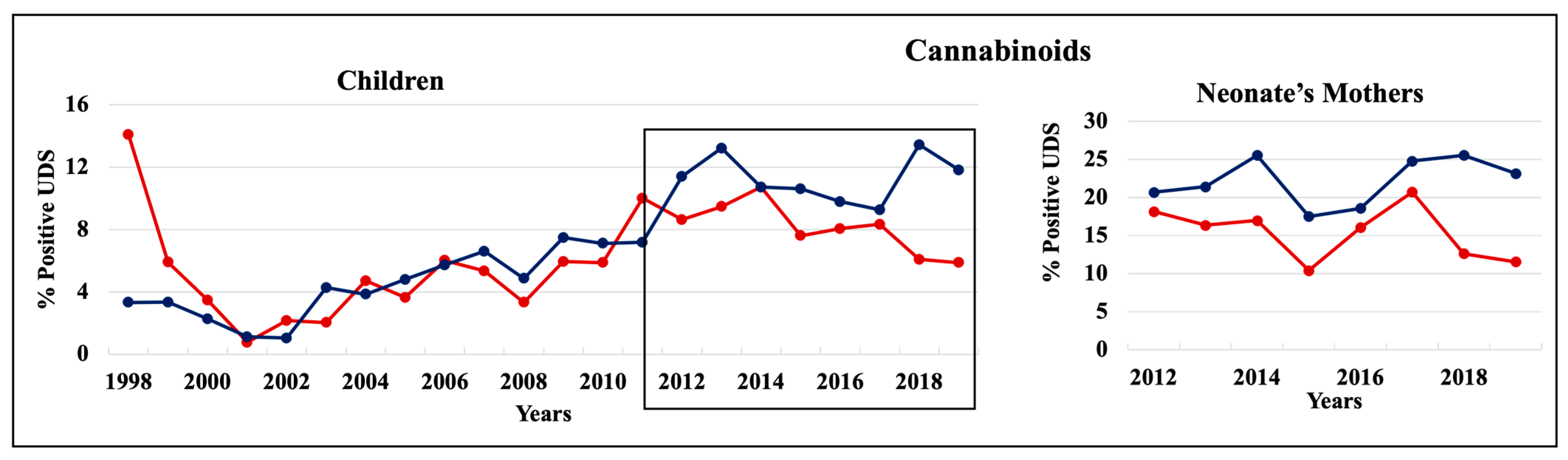
3.3.4. Cannabinoid
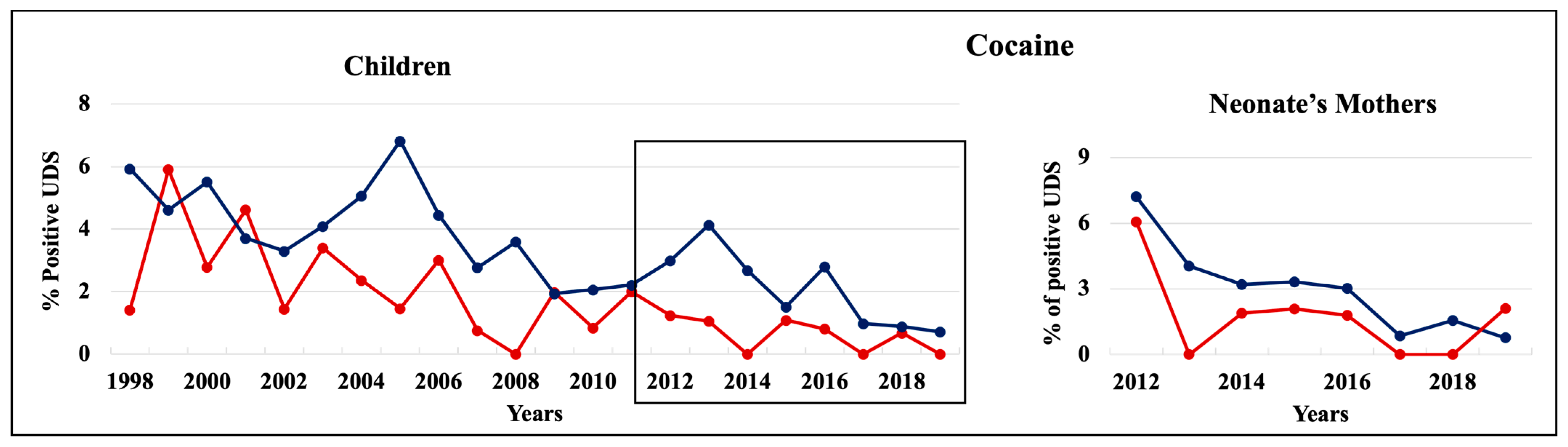
3.3.5. Cocaine
3.3.6. Trends in Drug Use among 18 Years Old Females Later in Their Life
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Schiavone, S.; Neri, M.; Harvey, B. Pathological Consequences of Drug Abuse: Implication of Redox Imbalance. Oxidative Med. Cell. Longev. 2019, 2019, 4780852–4780853. [Google Scholar] [CrossRef] [PubMed]
- Bachhuber, M.A.; Hennessy, S.; Cunningham, C.O.; Starrels, J.L. Increasing Benzodiazepine Prescriptions and Overdose Mortality in the United States, 1996–2013. Am. J. Public Health 2016, 106, 686–688. [Google Scholar] [CrossRef] [PubMed]
- NIDA. Benzodiazepines and Opioids; NIH Advancing Addiction Science; NIDA: Washington, DC, USA, 2021. Available online: https://nida.nih.gov/research-topics/opioids/benzodiazepines-opioids (accessed on 7 September 2022).
- Tetro, N.; Moushaev, S.; Rubinchik-Stern, M.; Eyal, S. The Placental Barrier: The Gate and the Fate in Drug Distribution. Pharm. Res. 2018, 35, 71. [Google Scholar] [CrossRef] [PubMed]
- Syme, M.R.; Paxton, J.W.; Keelan, J.A. Drug Transfer and Metabolism by the Human Placenta. Clin. Pharmacokinet. 2004, 43, 487–514. [Google Scholar] [CrossRef] [PubMed]
- NIDA. Substance Use in Women Drug Facts; NIDA: Washington, DC, USA, 2020. Available online: https://nida.nih.gov/publications/drugfacts/substance-use-in-women (accessed on 7 September 2022).
- Calvigioni, D.; Hurd, Y.L.; Harkany, T.; Keimpema, E. Neuronal substrates and functional consequences of prenatal cannabis exposure. Eur. Child Adolesc. Psychiatry 2014, 23, 931–941. [Google Scholar] [CrossRef]
- Perez, F.A.; Blythe, S.; Wouldes, T.; McNamara, K.; Black, K.I.; Oei, J.L. Prenatal methamphetamine—Impact on the mother and child—A review. Addiction 2022, 117, 250–260. [Google Scholar] [CrossRef]
- Chin, E.M.; Kitase, Y.; Madurai, N.K.; Robinson, S.; Jantzie, L.L. In utero methadone exposure permanently alters anatomical and functional connectivity: A preclinical evaluation. Front. Pediatr. 2023, 11, 1139378. [Google Scholar] [CrossRef]
- Belcher, A.M.; Rorabaugh, B.R. Maternal Use of Methamphetamine Alters Cardiovascular Function in the Adult Offspring. Biochem. Cell Biol. 2023. [Google Scholar] [CrossRef]
- NIDA. Substance Use While Pregnant and Breastfeeding; NIDA: Washington, DC, USA, 2022. Available online: https://nida.nih.gov/publications/research-reports/substance-use-in-women/substance-use-while-pregnant-breastfeeding (accessed on 7 September 2022).
- Barry, J.M.B.; Birnbaum, A.K.; Jasin, L.R.; Sherwin, C.M. Maternal Exposure and Neonatal Effects of Drugs of Abuse. J. Clin. Pharmacol. 2021, 61 (Suppl. S2), S142–S155. [Google Scholar] [CrossRef]
- Kocherlakota, P. Neonatal Abstinence Syndrome. Pediatrics 2014, 134, e547–e561. [Google Scholar] [CrossRef]
- Raffaeli, G.; Cavallaro, G.; Allegaert, K.; Wildschut, E.D.; Fumagalli, M.; Agosti, M.; Tibboel, D.; Mosca, F. Neonatal Abstinence Syndrome: Update on Diagnostic and Therapeutic Strategies. Pharmacother. J. Hum. Pharmacol. Drug Ther. 2017, 37, 814–823. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Zhang, T.; Ekheden, I.; Chang, Z.; Hellner, C.; Hasselström, J.; Jayaram-Lindström, N.; Onofrio, B.M.D.; Larsson, H.; Mataix-Cols, D.; et al. Prenatal exposure to benzodiazepines and Z-drugs in humans and risk of adverse neurodevelopmental outcomes in offspring: A systematic review. Neurosci. Biobehav. Rev. 2022, 137, 104647. [Google Scholar] [CrossRef] [PubMed]
- Behnke, M.; Smith, V.C.; Committee on Substance Abuse; Committee on Fetus and Newborn. Prenatal Substance Abuse: Short- and Long-term Effects on the Exposed Fetus. Pediatrics 2013, 131, e1009–e1024. [Google Scholar] [CrossRef]
- Clifford, E.; Kilgore, P.C.S.R.; Cvek, U.; Trutschl, M.; Baker, S.; Conrad, S.A.; Arnold, T.; Korneeva, N. Trends in drug use among young adult females: A 22-year retrospective analysis. Toxicol. Commun. 2022, 6, 85–96. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing. Available online: https://www.R-project.org/ (accessed on 2 February 2022).
- U.S. Census Bureau. Quick Facts; Shreveport City, LA, USA. 2019. Available online: https://www.census.gov/quickfacts/shreveportcitylouisiana (accessed on 22 September 2022).
- Leyenaar, J.K.; Schaefer, A.P.; Wasserman, J.R.; Moen, E.L.; O’malley, A.J.; Goodman, D.C. Infant Mortality Associated with Prenatal Opioid Exposure. JAMA Pediatr. 2021, 175, 706–714. [Google Scholar] [CrossRef]
- Creanga, A.A.; Sabel, J.C.; Ko, J.Y.; Wasserman, C.R.; Shapiro-Mendoza, C.K.; Taylor, P.; Barfield, W.; Cawthon, L.; Paulozzi, L.J. Maternal Drug Use and Its Effect on Neonates. Obstet. Gynecol. 2012, 119, 924–933. [Google Scholar] [CrossRef]
- Wen, X.; Belviso, N.; Murray, E.; Lewkowitz, A.K.; Ward, K.E.; Meador, K.J. Association of Gestational Opioid Exposure and Risk of Major and Minor Congenital Malformations. JAMA Netw. Open 2021, 4, e215708. [Google Scholar] [CrossRef]
- Lind, J.N.; Interrante, J.D.; Ailes, E.C.; Gilboa, S.M.; Khan, S.; Frey, M.T.; Dawson, A.L.; Honein, M.A.; Dowling, N.F.; Razzaghi, H.; et al. Maternal Use of Opioids During Pregnancy and Congenital Malformations: A Systematic Review. Pediatrics 2017, 139. [Google Scholar] [CrossRef]
- Radhakrishnan, R.; Vishnubhotla, R.V.; Guckien, Z.; Zhao, Y.; Sokol, G.M.; Haas, D.M.; Sadhasivam, S. Thalamocortical functional connectivity in infants with prenatal opioid exposure correlates with severity of neonatal opioid withdrawal syndrome. Neuroradiology 2022, 64, 1649–1659. [Google Scholar] [CrossRef]
- Grecco, G.G.; E Mork, B.; Huang, J.-Y.; E Metzger, C.; Haggerty, D.L.; Reeves, K.C.; Gao, Y.; Hoffman, H.; Katner, S.N.; Masters, A.R.; et al. Prenatal methadone exposure disrupts behavioral development and alters motor neuron intrinsic properties and local circuitry. Elife 2021, 10, e66230. [Google Scholar] [CrossRef]
- Huitfeldt, A.; Sundbakk, L.M.; Skurtveit, S.; Handal, M.; Nordeng, H. Associations of Maternal Use of Benzodiazepines or Benzodiazepine-like Hypnotics During Pregnancy with Immediate Pregnancy Outcomes in Norway. JAMA Netw. Open 2020, 3, e205860. [Google Scholar] [CrossRef] [PubMed]
- Wikner, B.N.; Stiller, C.-O.; Bergman, U.; Asker, C.; Källén, B. Use of benzodiazepines and benzodiazepine receptor agonists during pregnancy: Neonatal outcome and congenital malformations. Pharmacoepidemiol. Drug Saf. 2007, 16, 1203–1210. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.; Koh, J.-W.; Kim, Y.-A.; Chun, K.-C.; Han, J.Y.; Hwang, J.H.; Choi, J.-S.; Joo, S.H.; Kwon, H.-Y. Pregnancy and Neonatal Outcomes After Exposure to Alprazolam in Pregnancy. Front. Pharmacol. 2022, 13. [Google Scholar] [CrossRef] [PubMed]
- Noh, Y.; Lee, H.; Choi, A.; Kwon, J.S.; Choe, S.-A.; Chae, J.; Kim, D.-S.; Shin, J.-Y. First-trimester exposure to benzodiazepines and risk of congenital malformations in offspring: A population-based cohort study in South Korea. PLoS Med. 2022, 19, e1003945. [Google Scholar] [CrossRef] [PubMed]
- Convertino, I.; Sansone, A.C.; Marino, A.; Galiulo, M.T.; Mantarro, S.; Antonioli, L.; Fornai, M.; Blandizzi, C.; Tuccori, M. Neonatal Adaptation Issues After Maternal Exposure to Prescription Drugs: Withdrawal Syndromes and Residual Pharmacological Effects. Drug Saf. 2016, 39, 903–924. [Google Scholar] [CrossRef] [PubMed]
- Brandlistuen, R.E.; Ystrom, E.; Hernandez-Diaz, S.; Skurtveit, S.; Selmer, R.; Handal, M.; Nordeng, H. Association of prenatal exposure to benzodiazepines and child internalizing problems: A sibling-controlled cohort study. PLoS ONE 2017, 12, e0181042. [Google Scholar] [CrossRef]
- Sundbakk, L.M.; Wood, M.; Gran, J.M.; Nordeng, H. Impact of prenatal exposure to benzodiazepines and z-hypnotics on behavioral problems at 5 years of age: A study from the Norwegian Mother and Child Cohort Study. PLoS ONE 2019, 14, e0217830. [Google Scholar] [CrossRef]
- Jensen, A.G.; Knudsen, S.S.; Bech, B.H. Prenatal exposure to benzodiazepines and the development of the offspring–a systematic review. Neurotoxicol. Teratol. 2022, 91, 107078. [Google Scholar] [CrossRef]
- Votaw, V.R.; Geyer, R.; Rieselbach, M.M.; McHugh, R.K. The epidemiology of benzodiazepine misuse: A systematic review. Drug Alcohol Depend. 2019, 200, 95–114. [Google Scholar] [CrossRef]
- McHugh, R.K.; Geyer, R.; Bs, S.K.; Griffin, M.L.; Weiss, R.D. Nonmedical benzodiazepine use in adults with alcohol use disorder: The role of anxiety sensitivity and polysubstance use. Am. J. Addict. 2018, 27, 485–490. [Google Scholar] [CrossRef]
- Hurd, Y.; Wang, X.; Anderson, V.; Beck, O.; Minkoff, H.; Dow-Edwards, D. Marijuana impairs growth in mid-gestation fetuses. Neurotoxicol. Teratol. 2005, 27, 221–229. [Google Scholar] [CrossRef]
- Gray, T.R.; Eiden, R.D.; E Leonard, K.; Connors, G.J.; Shisler, S.; A Huestis, M. Identifying Prenatal Cannabis Exposure and Effects of Concurrent Tobacco Exposure on Neonatal Growth. Clin. Chem. 2010, 56, 1442–1450. [Google Scholar] [CrossRef]
- Gunn, J.K.L.; Rosales, C.B.; Center, K.E.; Nuñez, A.; Gibson, S.J.; Christ, C.; Ehiri, J.E. Prenatal exposure to cannabis and maternal and child health outcomes: A systematic review and meta-analysis. BMJ Open 2016, 6, e009986. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.-S.; Jew, C.P.; Lu, H.-C. Lasting impacts of prenatal cannabis exposure and the role of endogenous cannabinoids in the developing brain. Future Neurol. 2011, 6, 459–480. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Dow-Edwards, D.; Anderson, V.; Minkoff, H.; Hurd, Y.L. In utero marijuana exposure associated with abnormal amygdala dopamine D2 gene expression in the human fetus. Biol. Psychiatry 2004, 56, 909–915. [Google Scholar] [CrossRef] [PubMed]
- Bara, A.; Ferland, J.-M.N.; Rompala, G.; Szutorisz, H.; Hurd, Y.L. Cannabis and synaptic reprogramming of the developing brain. Nat. Rev. Neurosci. 2021, 22, 423–438. [Google Scholar] [CrossRef]
- Paul, S.E.; Hatoum, A.S.; Fine, J.D.; Johnson, E.C.; Hansen, I.; Karcher, N.R.; Moreau, A.L.; Bondy, E.; Qu, Y.; Carter, E.B.; et al. Associations Between Prenatal Cannabis Exposure and Childhood Outcomes: Results from the ABCD Study. JAMA Psychiatry 2021, 78, 64. [Google Scholar] [CrossRef]
- Day, N.L.; Goldschmidt, L.; Thomas, C.A. Prenatal marijuana exposure contributes to the prediction of marijuana use at age 14. Addiction 2006, 101, 1313–1322. [Google Scholar] [CrossRef]
- Roncero, C.; Valriberas-Herrero, I.; Mezzatesta-Gava, M.; Villegas, J.L.; Aguilar, L.; Grau-López, L. Cannabis use during pregnancy and its relationship with fetal developmental outcomes and psychiatric disorders. A systematic review. Reprod. Health 2020, 17, 25. [Google Scholar] [CrossRef]
- Oei, J.L.; Kingsbury, A.; Dhawan, A.; Burns, L.; Feller, J.M.; Clews, S.; Falconer, J.; Abdel-Latif, M.E. Amphetamines, the pregnant woman and her children: A review. J. Perinatol. 2012, 32, 737–747. [Google Scholar] [CrossRef]
- Ross, E.J.; Graham, D.L.; Money, K.M.; Stanwood, G.D. Developmental Consequences of Fetal Exposure to Drugs: What We Know and What We Still Must Learn. Neuropsychopharmacology 2015, 40, 61–87. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Gong, F.; Liu, P.; He, Y.; Wang, H. Effects of Prenatal Methamphetamine Exposure on Birth Outcomes, Brain Structure, and Neurodevelopmental Outcomes. Dev. Neurosci. 2021, 43, 271–280. [Google Scholar] [CrossRef] [PubMed]
- Shah, R.; Diaz, S.D.; Arria, A.; LaGasse, L.L.; Derauf, C.; Newman, E.; Smith, L.M.; Huestis, M.A.; Haning, W.; Strauss, A.; et al. Prenatal Methamphetamine Exposure and Short-Term Maternal and Infant Medical Outcomes. Am. J. Perinatol. 2012, 29, 391–400. [Google Scholar] [CrossRef] [PubMed]
- Watson, R.E.; DeSesso, J.M.; Hurtt, M.E.; Cappon, G.D. Postnatal growth and morphological development of the brain: A species comparison. Birth Defects Res. Part B Dev. Reprod. Toxicol. 2006, 77, 471–484. [Google Scholar] [CrossRef]
- Cunningham, J.K.; Callaghan, R.C.; Liu, L. US federal cocaine essential (‘precursor’) chemical regulation impacts on US cocaine availability: An intervention time–series analysis with temporal replication. Addiction 2015, 110, 805–820. [Google Scholar] [CrossRef]
- National Center for Biotechnology Information. PubChem Compound Summary for CID 446220, Cocaine. 2004. Available online: https://pubchem.ncbi.nlm.nih.gov/compound/Cocaine (accessed on 20 April 2022).
- Rizk, B.; Atterbury, J.L.; Groome, L.J. Reproductive risks of cocaine. Hum. Reprod. Update 1996, 2, 43–55. [Google Scholar] [CrossRef]
- Church, M.W.; Crossland, W.J.; Holmes, P.A.; Overbeck, G.W.; Tilak, J.P. Effects of Prenatal Cocaine on Hearing, Vision, Growth, and Behavior(a). Ann. N. Y. Acad. Sci. 1998, 846, 12–28. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 0–4-Year-Old Children | Neonates’ Mothers | ||
|---|---|---|---|
| Self-Identified Race | 1998–2011 | 2012–2019 | 2012–2019 |
| Black or African American | 6453 | 3530 | 1758 |
| White or Caucasian | 1735 | 932 | 606 |
| American Indian/Alaska Native | 10 | 5 | 4 |
| Asian | 28 | 9 | 2 |
| Native Hawaiian and Other Pacific Islander | 242 | 9 | 4 |
| Other | 39 | 3 | 51 |
| Unknown | 0 | 155 | 17 |
| Total | 8507 | 4769 | 2442 |
| Drug at 19 | Cannabinoid | Opiate | Benzodiazepine | Amphetamine | Cocaine | |
|---|---|---|---|---|---|---|
| Drug at 18 | ||||||
| Cannabinoid | 86 | 11 | 7 | 35 | 14 | |
| Opiate | 39 | 43 | 19 | 16 | 0 | |
| Benzodiazepine | 67 | 12 | 21 | 67 | 9 | |
| Amphetamine | 76 | 18 | 26 | 71 | 45 | |
| Cocaine | 65 | 0 | 0 | 50 | 30 | |
| All 18-35 y.o. females | 31 | 18 | 7 | 8 | 5 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ochoa, C.; Kilgore, P.C.S.R.; Korneeva, N.; Clifford, E.; Conrad, S.A.; Trutschl, M.; Bowers, J.M.; Arnold, T.; Cvek, U. Trends in Drug Tests among Children: A 22-Year Retrospective Analysis. Pathophysiology 2023, 30, 219-232. https://doi.org/10.3390/pathophysiology30020019
Ochoa C, Kilgore PCSR, Korneeva N, Clifford E, Conrad SA, Trutschl M, Bowers JM, Arnold T, Cvek U. Trends in Drug Tests among Children: A 22-Year Retrospective Analysis. Pathophysiology. 2023; 30(2):219-232. https://doi.org/10.3390/pathophysiology30020019
Chicago/Turabian StyleOchoa, Carolina, Phillip C. S. R. Kilgore, Nadejda Korneeva, Eric Clifford, Steven A. Conrad, Marjan Trutschl, Jacquelyn M. Bowers, Thomas Arnold, and Urska Cvek. 2023. "Trends in Drug Tests among Children: A 22-Year Retrospective Analysis" Pathophysiology 30, no. 2: 219-232. https://doi.org/10.3390/pathophysiology30020019
APA StyleOchoa, C., Kilgore, P. C. S. R., Korneeva, N., Clifford, E., Conrad, S. A., Trutschl, M., Bowers, J. M., Arnold, T., & Cvek, U. (2023). Trends in Drug Tests among Children: A 22-Year Retrospective Analysis. Pathophysiology, 30(2), 219-232. https://doi.org/10.3390/pathophysiology30020019