Efficacy of Octacalcium Phosphate Collagen Composite for Titanium Dental Implants in Dogs

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Animals
2.2. Preparation of OCP/Col and Autologous Bone
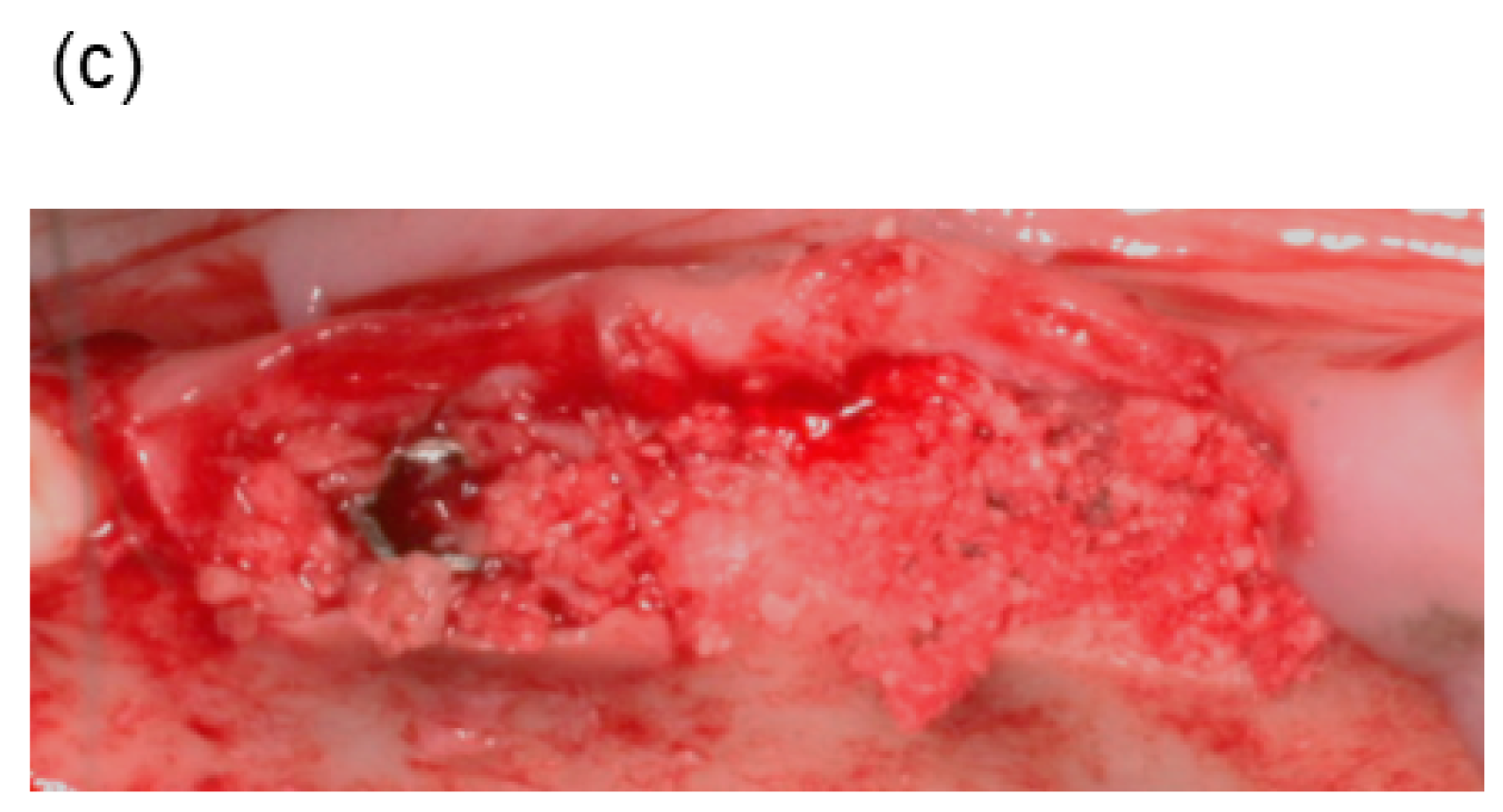
2.3. Surgical Procedure
2.4. Radiographic Analysis
2.5. Contact Microradiography, Histological, and Histomorphometric Analyses
2.6. Statistical Analysis
3. Results
3.1. Clinical Observation
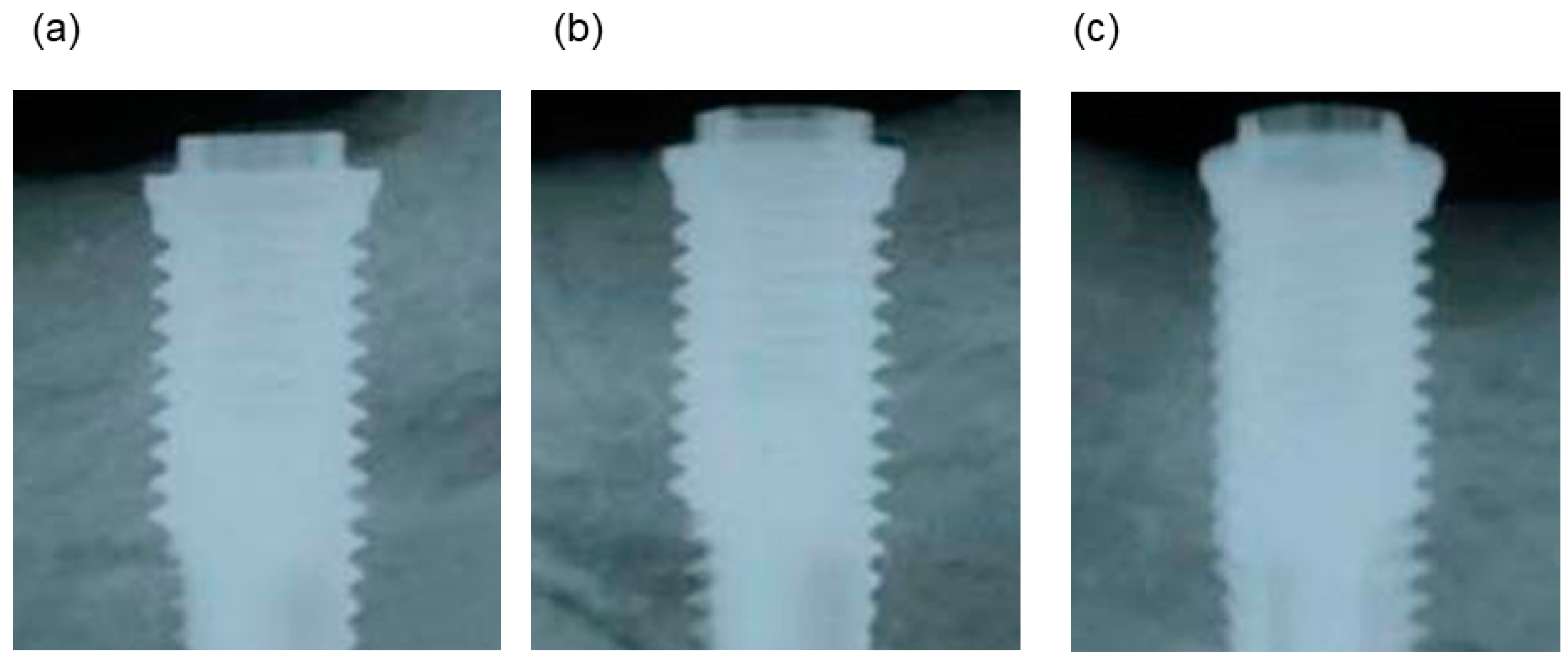
3.2. Radiographic Observations
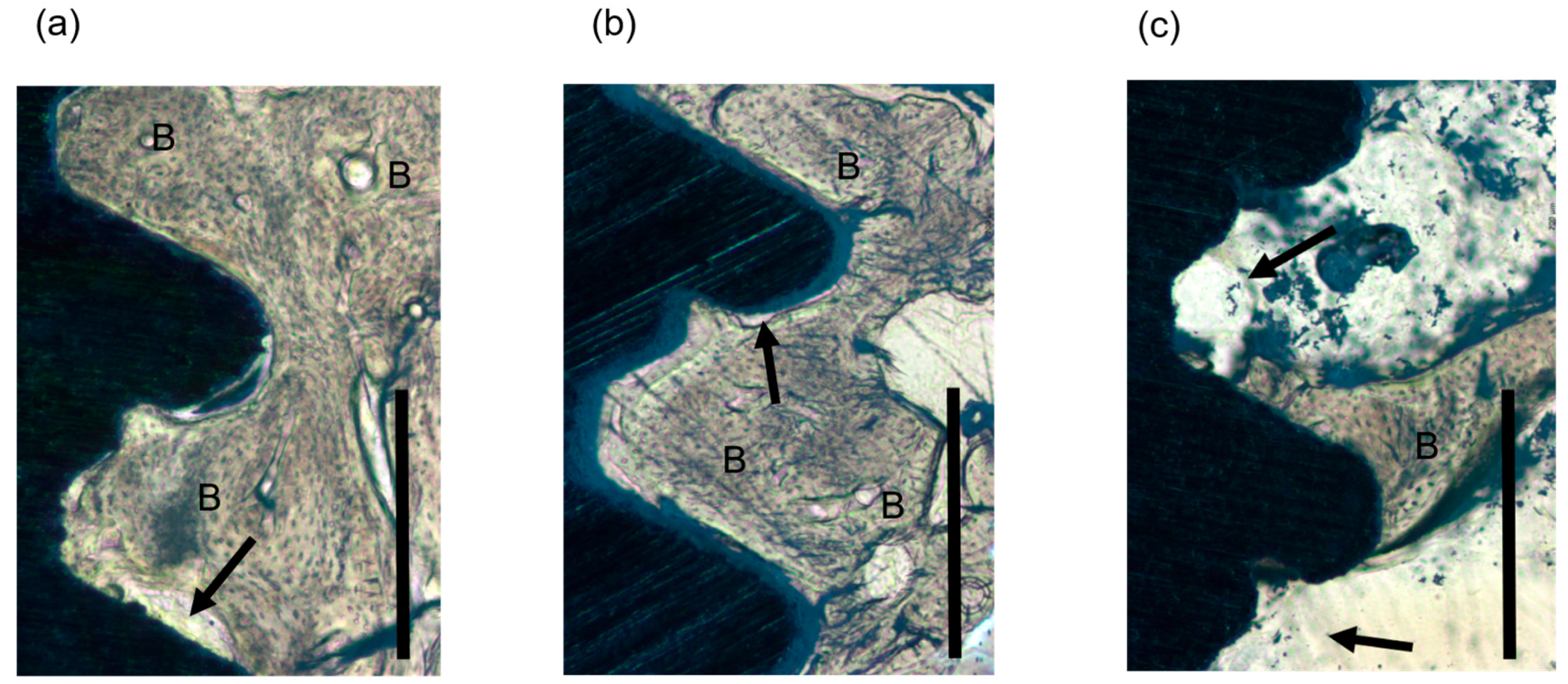
3.3. Contact Microradiography and Histological Observations
3.4. Histomorphometric Findings
4. Discussion
5. Conclusions
6. Patents
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Boyne, P.J.; James, R.A. Grafting of the maxillary sinus floor with autogenous marrow and bone. J. Oral Surg. 1980, 38, 613–616. [Google Scholar] [PubMed]
- Tatum, H., Jr. Maxillary and sinus implant reconstructions. Dent. Clin. N. Am. 1986, 30, 207–229. [Google Scholar] [PubMed]
- Bruschi, G.B.; Scipioni, A.; Calesini, G.; Bruschi, E. Localized management of sinus floor with simultaneous implant placement: A clinical report. Int. J. Oral Maxillofac. Implants 1998, 13, 219–226. [Google Scholar] [PubMed]
- Mestas, G.; Alarcon, M.; Chambrone, L. Long-term survival rates of titanium implants placed in expanded alveolar ridges using split crest procedures: A systematic review. Int. J. Oral Maxillofac. Implants 2016, 31, 591–599. [Google Scholar] [CrossRef] [PubMed]
- Hurzeler, M.B.; Quinones, C.R.; Schupbach, P. Guided bone regeneration around dental implants in the atrophic alveolar ridge using a bioresorbable barrier. An experimental study in the monkey. Clin. Oral Implants Res. 1997, 8, 323–331. [Google Scholar] [CrossRef] [PubMed]
- Buser, D.; Dula, K.; Hirt, H.P.; Schenk, R.K. Lateral ridge augmentation using autografts and barrier membranes: A clinical study with 40 partially edentulous patients. J. Oral Maxillofac. Surg. 1996, 54, 420–432. [Google Scholar] [CrossRef]
- Hjorting-Hansen, E. Bone grafting to the jaws with special reference to reconstructive preprosthetic surgery. A historical review. Mund Kiefer Gesichtschir. 2002, 6, 6–14. [Google Scholar] [CrossRef] [PubMed]
- Clavero, J.; Lundgren, S. Ramus or chin grafts for maxillary sinus inlay and local onlay augmentation: Comparison of donor site morbidity and complications. Clin. Implant Dent. Relat. Res. 2003, 5, 154–160. [Google Scholar] [CrossRef] [PubMed]
- Cricchio, G.; Lundgren, S. Donor site morbidity in two different approaches to anterior iliac crest bone harvesting. Clin. Implant Dent. Relat. Res. 2003, 5, 161–169. [Google Scholar] [CrossRef] [PubMed]
- Nkenke, E.; Neukam, F.W. Autogenous bone harvesting and grafting in advanced jaw resorption: Morbidity, resorption and implant survival. Eur. J. Oral Implantol. 2014, 7, 203–217. [Google Scholar]
- Bucholz, R.W. Nonallograft osteoconductive bone graft substitutes. Clin. Orthop. Relat. Res. 2002, 395, 44–52. [Google Scholar] [CrossRef]
- LeGeros, R.Z. Properties of osteoconductive biomaterials: Calcium phosphates. Clin. Orthop. Relat. Res. 2002, 395, 81–98. [Google Scholar] [CrossRef]
- Ogose, A.; Kondo, N.; Umezu, H.; Hotta, T.; Kawashima, H.; Tokunaga, K.; Ito, T.; Kudo, N.; Hoshino, M.; Gu, W.; et al. Histological assessment in grafts of highly purified beta-tricalcium phosphate (OSferion) in human bones. Biomaterials 2006, 27, 1542–1549. [Google Scholar] [CrossRef] [PubMed]
- Lichte, P.; Pape, H.C.; Pufe, T.; Kobbe, P.; Fischer, H. Scaffolds for bone healing: Concepts, materials and evidence. Injury 2011, 42, 569–573. [Google Scholar] [CrossRef] [PubMed]
- Minami, M.; Takechi, M.; Ohta, K.; Ohta, A.; Ninomiya, Y.; Takamoto, M.; Fukui, A.; Tada, M.; Kamata, N. Bone formation and osseointegration with titanium implant using granular- and block-type porous hydroxyapatite ceramics (IP-CHA). Dent. Mater. J. 2013, 32, 753–760. [Google Scholar] [CrossRef] [PubMed]
- Zijderveld, S.A.; Zerbo, I.R.; van den Bergh, J.P.; Schulten, E.A.; ten Bruggenkate, C.M. Maxillary sinus floor augmentation using a beta-tricalcium phosphate (Cerasorb) alone compared to autogenous bone grafts. Int. J. Oral Maxillofac. Implants 2005, 20, 432–440. [Google Scholar] [PubMed]
- Guarnieri, R.; Belleggia, F.; Ippoliti, S.; DeVilliers, P.; Stefanelli, L.V.; Di Carlo, S.; Pompa, G. Clinical radiographic, and histologic evaluation of maxillary sinus lift procedure using a highly purified xenogenic graft (Laddec®). J. Oral Maxillofac. Res. 2016, 7, e3. [Google Scholar] [CrossRef] [PubMed]
- Antunes, A.A.; Oliveira Neto, P.; de Santis, E.; Caneva, M.; Botticelli, D.; Salata, L.A. Comparisons between bio-oss((r)) and straumann((r)) bone ceramic in immediate and staged implant placement in dogs mandible bone defects. Clin. Oral Implants Res. 2013, 24, 135–142. [Google Scholar] [CrossRef] [PubMed]
- Merten, H.A.; Wiltfang, J.; Grohmann, U.; Hoenig, J.F. Intraindividual comparative animal study of alpha- and beta-tricalcium phosphate degradation in conjunction with simultaneous insertion of dental implants. J. Craniofac. Surg. 2001, 12, 59–68. [Google Scholar] [CrossRef] [PubMed]
- Schwarz, F.; Mihatovic, I.; Golubovic, V.; Hegewald, A.; Becker, J. Influence of two barrier membranes on staged guided bone regeneration and osseointegration of titanium implants in dogs: Part 1. Augmentation using bone graft substitutes and autogenous bone. Clin. Oral Implants Res. 2012, 23, 83–89. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Ryu, M.Y.; Baek, H.R.; Lee, H.K.; Seo, J.H.; Lee, K.M.; Lee, A.Y.; Zheng, G.B.; Chang, B.S.; Lee, C.K. The effects of recombinant human bone morphogenetic protein-2-loaded tricalcium phosphate microsphere-hydrogel composite on the osseointegration of dental implants in minipigs. Artif. Organs 2014, 38, 149–158. [Google Scholar] [CrossRef] [PubMed]
- Zou, D.; Guo, L.; Lu, J.; Zhang, X.; Wei, J.; Liu, C.; Zhang, Z.; Jiang, X. Engineering of bone using porous calcium phosphate cement and bone marrow stromal cells for maxillary sinus augmentation with simultaneous implant placement in goats. Tissue Eng. Part A 2012, 18, 1464–1478. [Google Scholar] [CrossRef] [PubMed]
- Aludden, H.C.; Mordenfeld, A.; Hallman, M.; Dahlin, C.; Jensen, T. Lateral ridge augmentation with bio-oss alone or bio-oss mixed with particulate autogenous bone graft: A systematic review. Int. J. Oral Maxillofac. Surg. 2017, 46, 1030–1038. [Google Scholar] [CrossRef] [PubMed]
- Brown, W.S.J.; Lehr, J.; Frazier, A. Crystallographic and chemical relations between octacalcium phosphate and hydroxyapatite. Nature 1962, 196, 1050–1055. [Google Scholar] [CrossRef]
- Tohda, H.; Yamada, M.; Yamaguchi, Y.; Yanagisawa, T. High-resolution electron microscopical observations of initial enamel crystals. J. Electron. Microsc. 1997, 46, 97–101. [Google Scholar] [CrossRef]
- Bodier-Houlle, P.; Steuer, P.; Voegel, J.C.; Cuisinier, F.J. First experimental evidence for human dentine crystal formation involving conversion of octacalcium phosphate to hydroxyapatite. Acta Crystallogr. D Biol. Crystallogr. 1998, 54, 1377–1381. [Google Scholar] [CrossRef] [PubMed]
- Crane, N.J.; Popescu, V.; Morris, M.D.; Steenhuis, P.; Ignelzi, M.A., Jr. Raman spectroscopic evidence for octacalcium phosphate and other transient mineral species deposited during intramembranous mineralization. Bone 2006, 39, 434–442. [Google Scholar] [CrossRef] [PubMed]
- Anada, T.; Kumagai, T.; Honda, Y.; Masuda, T.; Kamijo, R.; Kamakura, S.; Yoshihara, N.; Kuriyagawa, T.; Shimauchi, H.; Suzuki, O. Dose-dependent osteogenic effect of octacalcium phosphate on mouse bone marrow stromal cells. Tissue Eng. Part A 2008, 14, 965–978. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, O.; Kamakura, S.; Katagiri, T.; Nakamura, M.; Zhao, B.; Honda, Y.; Kamijo, R. Bone formation enhanced by implanted octacalcium phosphate involving conversion into ca-deficient hydroxyapatite. Biomaterials 2006, 27, 2671–2681. [Google Scholar] [CrossRef] [PubMed]
- Kawai, T.; Anada, T.; Honda, Y.; Kamakura, S.; Matsui, A.; Matsui, K.; Echigo, S.; Suzuki, O. Analysis of the osteoblastic cell differentiation by synthetic octacalcium phosphate (ocp) compared with commercially available beta-tcp ceramic. Jpn. J. Oral Maxillofac. Surg. 2010, 56, 2–8. [Google Scholar] [CrossRef]
- Suzuki, O.; Nakamura, M.; Miyasaka, Y.; Kagayama, M.; Sakurai, M. Bone formation on synthetic precursors of hydroxyapatite. Tohoku J. Exp. Med. 1991, 164, 37–50. [Google Scholar] [CrossRef] [PubMed]
- Kamakura, S.; Sasano, Y.; Shimizu, T.; Hatori, K.; Suzuki, O.; Kagayama, M.; Motegi, K. Implanted octacalcium phosphate is more resorbable than beta-tricalcium phosphate and hydroxyapatite. J. Biomed. Mater. Res. 2002, 59, 29–34. [Google Scholar] [CrossRef] [PubMed]
- Kamakura, S.; Sasaki, K.; Honda, Y.; Anada, T.; Suzuki, O. Octacalcium phosphate combined with collagen orthotopically enhances bone regeneration. J. Biomed. Mater. Res. B Appl. Biomater. 2006, 79, 210–217. [Google Scholar] [CrossRef] [PubMed]
- Iibuchi, S.; Matsui, K.; Kawai, T.; Sasaki, K.; Suzuki, O.; Kamakura, S.; Echigo, S. Octacalcium phosphate (OCP) collagen composites enhance bone healing in a dog tooth extraction socket model. Int. J. Oral Maxillofac. Surg. 2010, 39, 161–168. [Google Scholar] [CrossRef] [PubMed]
- Kawai, T.; Matsui, K.; Iibuchi, S.; Anada, T.; Honda, Y.; Sasaki, K.; Kamakura, S.; Suzuki, O.; Echigo, S. Reconstruction of critical-sized bone defect in dog skull by octacalcium phosphate combined with collagen. Clin. Implant Dent. Relat. Res. 2011, 13, 112–123. [Google Scholar] [CrossRef] [PubMed]
- Matsui, K.; Matsui, A.; Handa, T.; Kawai, T.; Suzuki, O.; Kamakura, S.; Echigo, S. Bone regeneration by octacalcium phosphate collagen composites in a dog alveolar cleft model. Int. J. Oral Maxillofac. Surg. 2010, 39, 1218–1225. [Google Scholar] [CrossRef] [PubMed]
- Miura, K.; Matsui, K.; Kawai, T.; Kato, Y.; Matsui, A.; Suzuki, O.; Kamakura, S.; Echigo, S. Octacalcium phosphate collagen composites with titanium mesh facilitate alveolar augmentation in canine mandibular bone defects. Int. J. Oral Maxillofac. Surg. 2012, 41, 1161–1169. [Google Scholar] [CrossRef] [PubMed]
- Tanuma, Y.; Matsui, K.; Kawai, T.; Matsui, A.; Suzuki, O.; Kamakura, S.; Echigo, S. Comparison of bone regeneration between octacalcium phosphate/collagen composite and beta-tricalcium phosphate in canine calvarial defect. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2013, 115, 9–17. [Google Scholar] [CrossRef] [PubMed]
- Kanda, N.; Matsui, K.; Kawai, T.; Edamatsu, H.; Tanuma, Y.; Suzuki, O.; Takahashi, T.; Kamakura, S. Implantation of octacalcium phosphate collagen composites (OCP/COL) after extraction of canine deciduous teeth achieved undisturbed permanent tooth eruption. Arch. Oral Biol. 2016, 72, 179–186. [Google Scholar] [CrossRef] [PubMed]
- Kawai, T.; Echigo, S.; Matsui, K.; Tanuma, Y.; Takahashi, T.; Suzuki, O.; Kamakura, S. First clinical application of octacalcium phosphate collagen composite in human bone defect. Tissue Eng. Part A 2014, 20, 1336–1341. [Google Scholar] [CrossRef] [PubMed]
- Kawai, T.; Suzuki, O.; Matsui, K.; Tanuma, Y.; Takahashi, T.; Kamakura, S. Octacalcium phosphate collagen composite facilitates bone regeneration of large mandibular bone defect in humans. J. Tissue Eng. Regen. Med. 2017, 11, 1641–1647. [Google Scholar] [CrossRef] [PubMed]
- KomLev, V.S.; Barinov, S.M.; Bozo, I.I.; Deev, R.V.; Eremin, I.I.; Fedotov, A.Y.; Gurin, A.N.; Khromova, N.V.; Kopnin, P.B.; Kuvshinova, E.A.; et al. Bioceramics composed of octacalcium phosphate demonstrate enhanced biological behavior. ACS Appl. Mater. Interfaces 2014, 6, 16610–16620. [Google Scholar] [CrossRef] [PubMed]
- Aerssens, J.; Boonen, S.; Lowet, G.; Dequeker, J. Interspecies differences in bone composition, density, and quality: Potential implications for in vivo bone research. Endocrinology 1998, 139, 663–670. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, O.; Nakamura, M.; Miyasaka, Y.; Kagayama, M.; Sakurai, M. Maclura pomifera agglutinin-binding glycoconjugates on converted apatite from synthetic octacalcium phosphate implanted into subperiosteal region of mouse calvaria. Bone Miner. 1993, 20, 151–166. [Google Scholar] [CrossRef]
- Fowler, B.O.; Moreno, E.C.; Brown, W.E. Infra-red spectra of hydroxyapatite, octacalcium phosphate and pyrolysed octacalcium phosphate. Arch. Oral Biol. 1966, 11, 477–492. [Google Scholar] [CrossRef]
- Nelson, D.G.; McLean, J.D. High-resolution electron microscopy of octacalcium phosphate and its hydrolysis products. Calcif. Tissue Int. 1984, 36, 219–232. [Google Scholar] [CrossRef] [PubMed]







© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kawai, T.; Matsui, K.; Ezoe, Y.; Kajii, F.; Suzuki, O.; Takahashi, T.; Kamakura, S. Efficacy of Octacalcium Phosphate Collagen Composite for Titanium Dental Implants in Dogs. Materials 2018, 11, 229. https://doi.org/10.3390/ma11020229
Kawai T, Matsui K, Ezoe Y, Kajii F, Suzuki O, Takahashi T, Kamakura S. Efficacy of Octacalcium Phosphate Collagen Composite for Titanium Dental Implants in Dogs. Materials. 2018; 11(2):229. https://doi.org/10.3390/ma11020229
Chicago/Turabian StyleKawai, Tadashi, Keiko Matsui, Yushi Ezoe, Fumihiko Kajii, Osamu Suzuki, Tetsu Takahashi, and Shinji Kamakura. 2018. "Efficacy of Octacalcium Phosphate Collagen Composite for Titanium Dental Implants in Dogs" Materials 11, no. 2: 229. https://doi.org/10.3390/ma11020229
APA StyleKawai, T., Matsui, K., Ezoe, Y., Kajii, F., Suzuki, O., Takahashi, T., & Kamakura, S. (2018). Efficacy of Octacalcium Phosphate Collagen Composite for Titanium Dental Implants in Dogs. Materials, 11(2), 229. https://doi.org/10.3390/ma11020229