Biomimetic Mineralizing Agents Recover the Micro Tensile Bond Strength of Demineralized Dentin

 ,
,  and
and 
Abstract
:1. Introduction
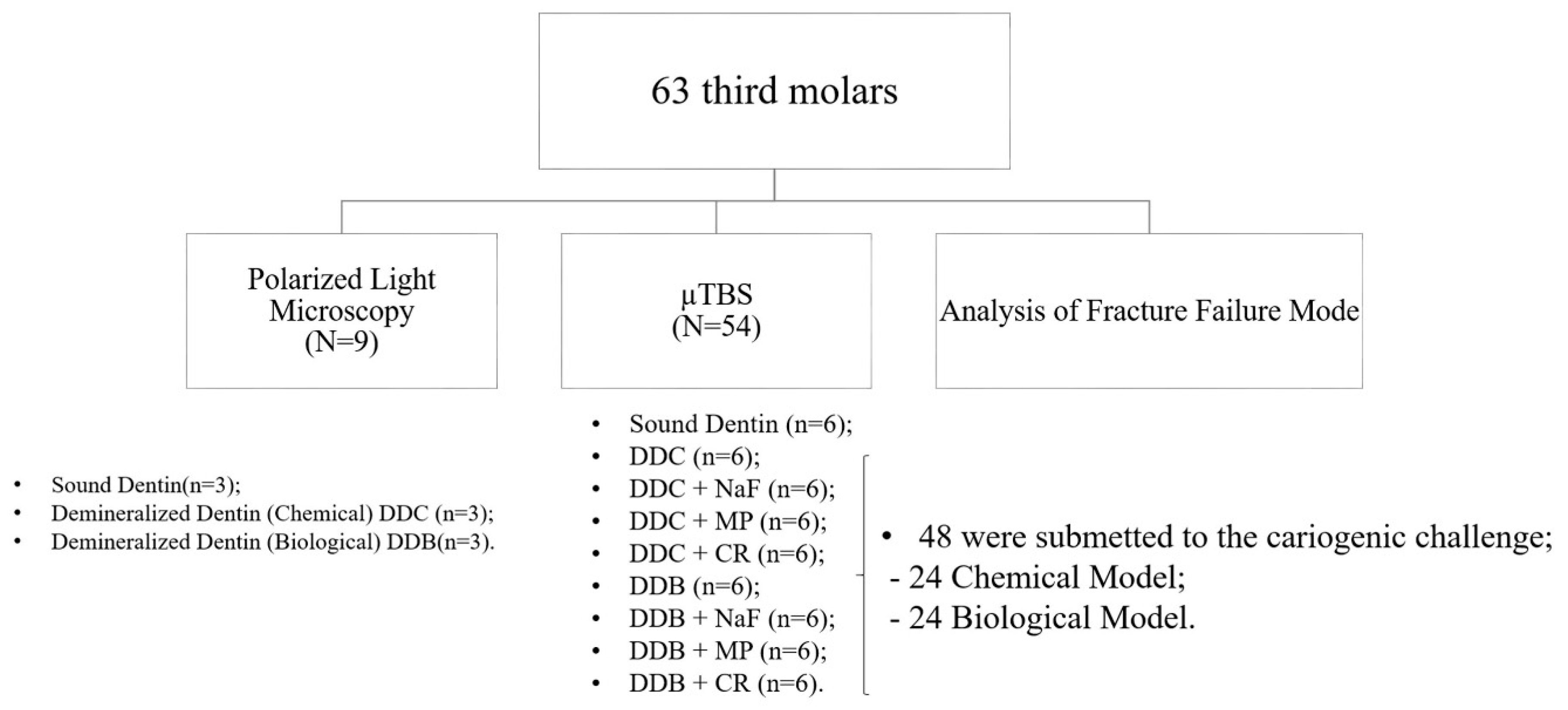
2. Materials and Methods
2.1. Artificial Dentin Caries-Like Lesions (DCLL) Production Protocols
2.1.1. Chemical Model
2.1.2. Biological Model
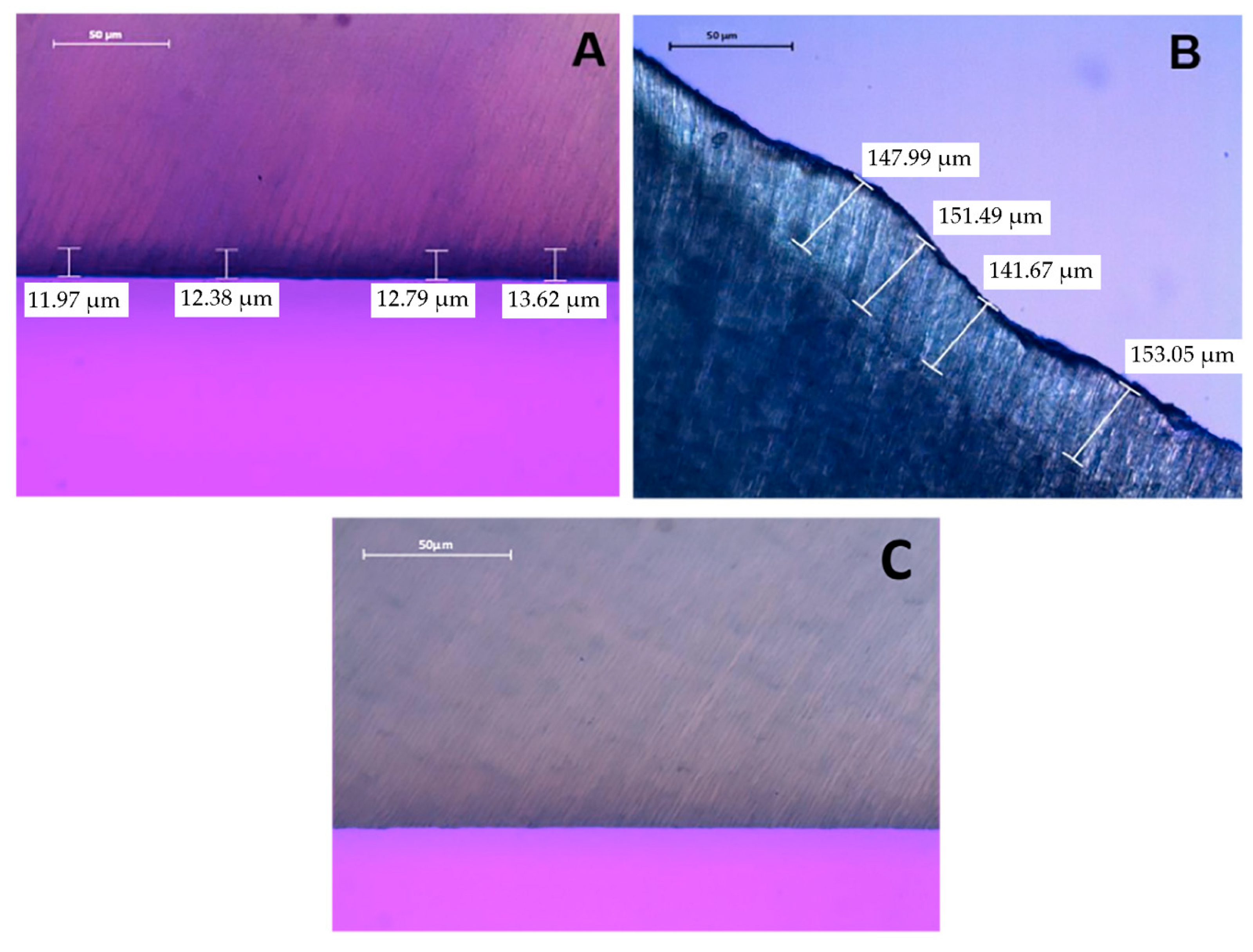
2.2. Polarized Light Microscopy (PLM)
2.3. Dentin Surface Treatment
2.4. Bonding Procedures
2.5. Microtensile Bond Strength Test (µTBS)
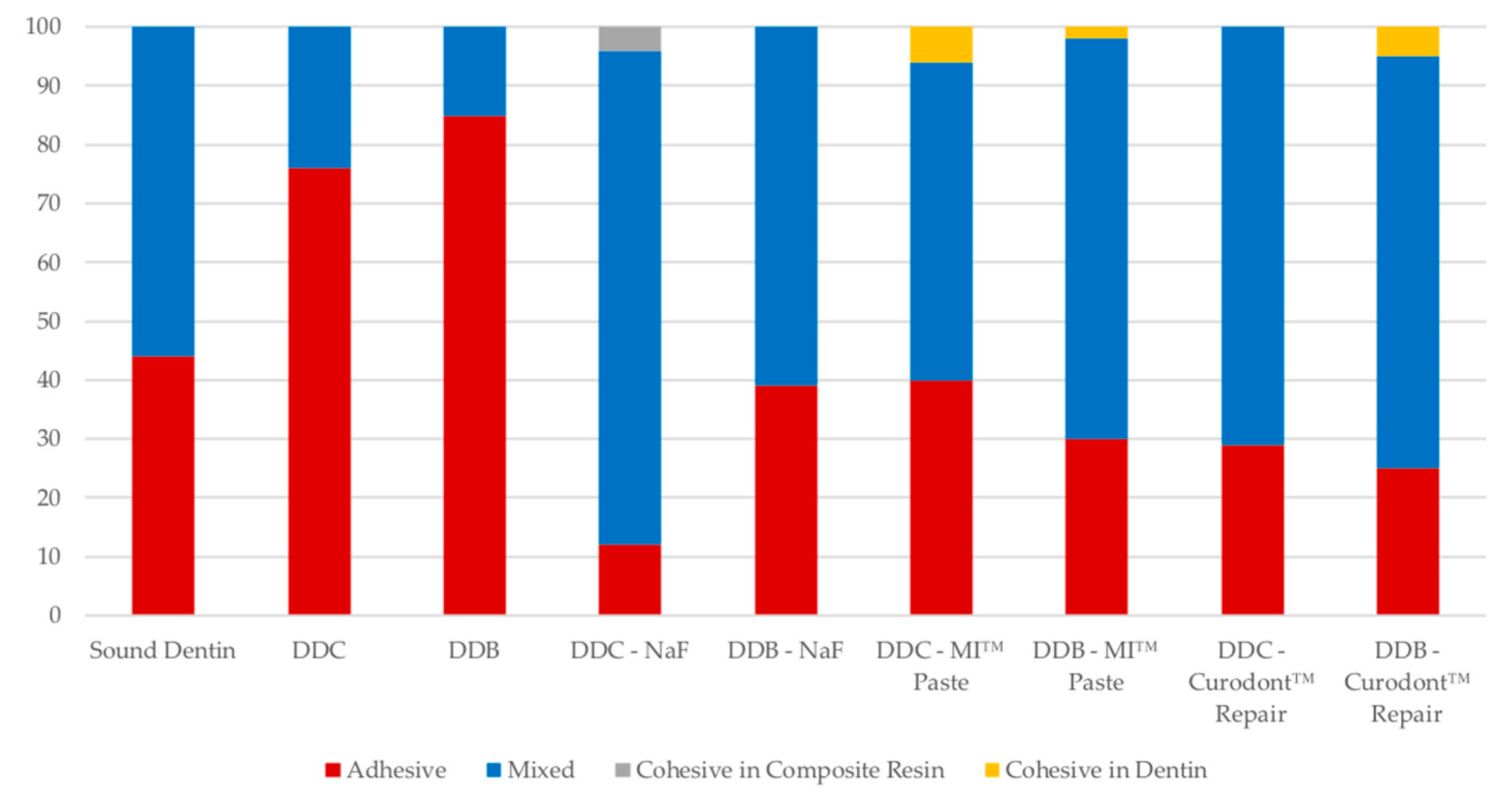
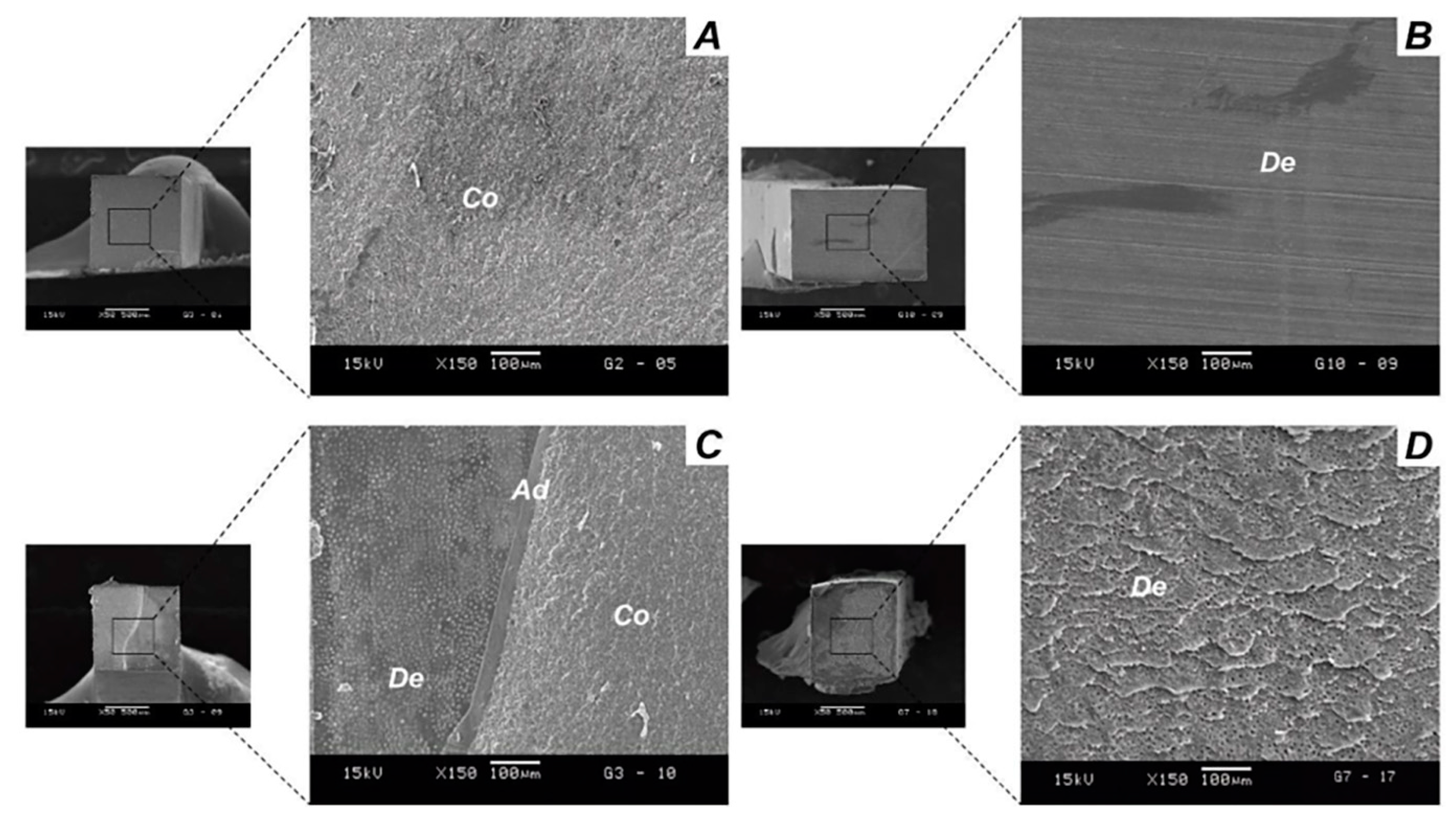
2.6. Analysis of Failure Mode
2.7. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Nakabayashi, N.; Kojima, K.; Masuhara, E. The promotion of adhesion by the infiltration of monomers into tooth substrates. J. Biomed. Mater. Res. 1982, 16, 265–273. [Google Scholar] [CrossRef] [PubMed]
- Van, M.B.; Perdigão, J.; Lambrechts, P.; Vanherle, G. The clinical performance of adhesives. J. Dent. 1998, 26, 1–20. [Google Scholar]
- Kassebaum, N.J.; Bernabé, E.; Dahiya, M.; Bhandari, B.; Murray, C.J.; Marcenes, W. Global burden of untreated caries: A systematic review and metaregression. J. Dent. Res. 2015, 94, 650–658. [Google Scholar] [CrossRef] [PubMed]
- Spencer, P.; Wang, Y. Adhesive phase separation at the dentin interface under wet bonding conditions. J. Biomed. Mater. Res. 2002, 62, 447–456. [Google Scholar] [CrossRef] [PubMed]
- de Carvalho, F.G.; de Fucio, S.B.; Sinhoreti, M.A.; Correr-Sobrinho, L.; Puppin-Rontani, R.M. Confocal laser scanning microscopic analysis of the depth of dentin caries-like lesions in primary and permanent teeth. Braz. Dent. J. 2008, 19, 139–144. [Google Scholar] [CrossRef] [PubMed]
- Perdigão, J.; Reis, A.; Loguercio, A.D. Dentin adhesion and MMPs: A comprehensive review. J. Esthet. Restor. Dent. 2013, 25, 219–241. [Google Scholar] [CrossRef] [PubMed]
- Tjäderhane, L. Dentin bonding: Can we make it last? Oper. Dent. 2015, 40, 4–18. [Google Scholar] [CrossRef] [PubMed]
- Nakajima, M.; Kunawarote, S.; Prasansuttiporn, T.; Tagami, J. Bonding to caries-affected dentin. Jpn. Dent. Sci. Rev. 2011, 47, 102–114. [Google Scholar] [CrossRef] [Green Version]
- Niu, L.N.; Zhang, W.; Pashley, D.H.; Breschi, L.; Mao, J.; Chen, J.H.; Tay, F.R. Biomimetic remineralization of dentin. Dent. Mater. 2014, 30, 77–96. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tay, F.R.; Pashley, D.H. Biomimetic remineralization of resin-bonded acid-etched dentin. J. Dent. Res. 2009, 88, 719–724. [Google Scholar] [CrossRef] [PubMed]
- Reynolds, E.C. Calcium phosphate-based remineralization systems: Scientific evidence? Aust. Dent. J. 2008, 53, 268–273. [Google Scholar] [CrossRef] [PubMed]
- Brackett, M.G.; Agee, K.A.; Brackett, W.W.; Key, W.O.; Sabatini, C.; Kato, M.T.; Buzalaf, M.A.; Tjäderhane, L.; Pashley, D.H. Effect of Sodium Fluoride on the endogenous MMP Activity of Dentin Matrices. J. Nat. Sci. 2015, 1, 1–11. [Google Scholar]
- Borges, B.C.; Souza-Junior, E.J.; da Costa Gde, F.; Pinheiro, I.V.; Sinhoreti, M.A.; Braz, R.; Montes, M.A. Effect of dentin pre-treatment with a casein phosphopeptide-amorphous calcium phosphate (CPP-ACP) paste on dentin bond strength in tridimensional cavities. Acta Odontol. Scand. 2013, 71, 271–277. [Google Scholar] [CrossRef] [PubMed]
- Shafiei, F.; Derafshi, R.; Memarpour, M. Bond strength of self-adhering materials: Effect of dentin-desensitizing treatment with a CPP-ACP paste. Int. J. Periodontics Restor. Dent. 2017, 37, 337–343. [Google Scholar] [CrossRef] [PubMed]
- Brunton, P.A.; Davies, R.P.; Burke, J.L.; Smith, A.; Aggeli, A.; Brookes, S.J.; Kirkham, J. Treatment of early caries lesions using biomimetic self-assembling peptides—A clinical safety trial. Br. Dent. J. 2013, 215, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Schlee, M.; Schad, T.; Koch, J.H.; Cattin, P.C.; Rathe, F. Clinical performance of self-assembling peptide P11-4 in the treatment of initial proximal carious lesions: A practice-based case series. J. Investig. Clin. Dent. 2018, 9, e12286. [Google Scholar] [CrossRef] [PubMed]
- Barbosa-Martins, L.F.; de Sousa, J.P.; de Castilho, A.R.F.; Puppin-Rontani, J.; Davies, R.P.W.; Puppin-Rontani, R.M. Enhancing bond strength on demineralized dentin by pre-treatment with selective remineralising agents. J. Mech. Behav. Biomed. Mater. 2018, 81, 214–221. [Google Scholar] [CrossRef] [PubMed]
- Erhardt, M.C.; Rodrigues, J.A.; Valentino, T.A.; Ritter, A.V.; Pimenta, L.A. In vitro μTBS of one-bottle adhesive systems: Sound versus artificially-created caries-affected dentin. J. Biomed. Mater. Res. B Appl. Biomater. 2008, 86, 181–187. [Google Scholar] [CrossRef] [PubMed]
- Marquezan, M.; Corrêa, F.N.; Sanabe, M.E.; Rodrigues Filho, L.E.; Hebling, J.; Guedes-Pinto, A.C.; Mendes, F.M. Artificial methods of dentine caries induction: A hardness and morphological comparative study. Arch. Oral Biol. 2009, 54, 1111–1117. [Google Scholar] [CrossRef] [PubMed]
- Zanchi, C.H.; Lund, R.G.; Perrone, L.R.; Ribeiro, G.A.; Del Pino, F.A.; Pinto, M.B.; Demarco, F.F. Microtensile bond strength of two-step etch-and-rinse adhesive systems on sound and artificial caries-affected dentin. Am. J. Dent. 2010, 23, 152–156. [Google Scholar] [PubMed]
- Sanabe, M.E.; de Souza Costa, C.A.; Hebling, J. Exposed collagen in aged resin–dentin bonds produced on sound and caries-affected dentin in the presence of chlorhexidine. J. Adhes. Dent. 2011, 13, 117–124. [Google Scholar] [PubMed]
- Joves, G.J.; Inoue, G.; Nakashima, S.; Sadr, A.; Nikaido, T.; Tagami, J. Mineral density, morphology and bond strength of natural versus artificial caries-affected dentin. Dent. Mater. J. 2013, 32, 138–143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pacheco, L.F.; Banzi, É.; Rodrigues, E.; Soares, L.E.; Pascon, F.M.; Correr-Sobrinho, L.; Puppin-Rontani, R.M. Molecular and structural evaluation of dentin caries-like lesions produced by different artificial models. Braz. Dent. J. 2013, 24, 610–618. [Google Scholar] [CrossRef] [PubMed]
- Zancopé, B.R.; Rodrigues, L.P.; Parisotto, T.M.; Steiner-Oliveira, C.; Rodrigues, L.K.A.; Nobre-dos-Santos, M. CO2 laser irradiation enhances CaF2 formation and inhibits lesion progression on demineralized dental enamel—In vitro study. Lasers Med. Sci. 2016, 31, 539–547. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, S.; Breschi, L.; Özcan, M.; Pfefferkorn, F.; Ferrari, M.; Van Meerbeek, B. Academy of Dental Materials guidance on in vitro testing of dental composite bonding effectiveness to dentin/enamel using micro-tensile bond strength (μTBS) approach. Dent. Mater. 2017, 33, 133–143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bacchi, A.; Abuna, G.; Babbar, A.; Sinhoreti, M.A.C.; Feitosa, V.P. Influence of 3-month simulated pulpal pressure on the microtensile bond strength of simplified resin luting systems. J. Adhes. Dent. 2015, 17, 265–271. [Google Scholar] [PubMed]
- Peixoto, A.C.; Bicalho, A.A.; Isolan, C.P.; Maske, T.T.; Moraes, R.R.; Cenci, M.S.; Soares, C.J.; Faria-e-Silva, A.L. Bonding of adhesive luting agents to caries-affected dentin induced by a microcosm biofilm model. Oper. Dent. 2015, 40, 102–111. [Google Scholar] [CrossRef] [PubMed]
- Qi, Y.P.; Li, N.; Niu, L.N.; Primus, C.M.; Ling, J.Q.; Pashley, D.H.; Tay, F.R. Remineralization of artificial dentinal caries lesions by biomimetically modified mineral trioxide aggregate. Acta Biomater. 2012, 8, 836–842. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robinson, C.; Brookes, S.J.; Kirkham, J.; Wood, S.R.; Shore, R.C. In vitro studies of the penetration of adhesive resins into artificial caries-like lesions. Caries Res. 2001, 35, 136–141. [Google Scholar] [CrossRef] [PubMed]
- Lenzi, T.L.; Calvo, A.F.; Tedesco, T.K.; Ricci, H.A.; Hebling, J.; Raggio, D.P. Effect of method of caries induction on aged resin–dentin bond of primary teeth. BMC Oral Health 2015, 15, 79. [Google Scholar] [CrossRef] [PubMed]
- Yoshiyama, M.; Doi, J.; Nishitani, Y.; Itota, T.; Tay, F.R.; Carvalho, R.M.; Pashley, D.H. Bonding ability of adhesive resins to caries-affected and caries-infected dentin. J. Appl. Oral Sci. 2004, 12, 171–176. [Google Scholar] [CrossRef] [PubMed]
- Doozandeh, M.; Firouzmandi, M.; Mirmohammadi, M. The simultaneous effect of extended etching time and casein phosphopeptide-amorphous calcium phosphate containing paste application on shear bond strength of etch-and-rinse adhesive to caries-affected dentin. J. Contemp. Dent. Pract. 2015, 16, 794–799. [Google Scholar] [CrossRef] [PubMed]
- Ceballos, L.; Camejo, D.G.; Victoria Fuentes, M.; Osorio, R.; Toledano, M.; Carvalho, R.M.; Pashley, D.H. Microtensile bond strength of total-etch and self-etching adhesives to caries-affected dentine. J. Dent. 2003, 31, 469–477. [Google Scholar] [CrossRef]
- Fusayama, T.; Kurosaki, N. Structure and removal of carious dentin. Int. Dent. J. 1972, 22, 401–411. [Google Scholar] [PubMed]
- Wang, S.; Huang, C.; Zheng, T.L.; Zhang, Z.X.; Wang, Y.N.; Cheng, X.R. Microtensile bond strength and morphological evaluations of total-etch and self-etch adhesives to caries-affected dentin. Zhonghua Kou Qiang Yi Xue Za Zhi 2006, 41, 323–326. [Google Scholar] [PubMed]
- Sano, H.; Yoshiyama, M.; Ebisu, S.; Burrow, M.F.; Takatsu, T.; Ciucchi, B.; Carvalho, R.; Pashley, D.H. Comparative SEM and TEM observations of nanoleakage within the hybrid layer. Oper. Dent. 1995, 20, 160–167. [Google Scholar] [PubMed]
- Stanislawczuk, R.; Pereira, F.; Muñoz, M.A.; Luque, I.; Farago, P.V.; Reis, A.; Loguercio, A.D. Effects of chlorhexidine-containing adhesives on the durability of resin–dentine interfaces. J. Dent. 2014, 42, 39–47. [Google Scholar] [CrossRef] [PubMed]
- Nassar, M.; Hiraishi, N.; Shimokawa, H.; Tamura, Y.; Otsuki, M.; Kasugai, S.; Ohya, K.; Tagami, J. The inhibition effect of non-protein thiols on dentinal matrix metalloproteinase activity and HEMA cytotoxicity. J. Dent. 2014, 42, 312–318. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Kim, Y.K.; Dai, L.; Li, N.; Khan, S.O.; Pashley, D.H.; Tay, F.R. Hierarchical and non-hierarchical mineralisation of collagen. Biomaterials 2011, 32, 1291–1300. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bahari, M.; Savadi Oskoee, S.; Kimyai, S.; Pouralibaba, F.; Farhadi, F.; Norouzi, M. Effect of casein phosphopeptide-amorphous calcium phosphate treatment on microtensile bond strength to carious affected dentin using two adhesive strategies. J. Dent. Res. Dent. Clin. Dent. Prospects 2014, 8, 141–147. [Google Scholar] [PubMed]
- Reynolds, E.C. Anticariogenic complexes of amorphous calcium phosphate stabilized by casein phosphopeptides: A review. Spec. Care Dent. 1998, 18, 8–16. [Google Scholar] [CrossRef]
- Cross, K.J.; Huq, N.L.; Reynolds, E.C. Casein phosphopeptides in oral health--chemistry and clinical applications. Curr. Pharm. Des. 2007, 13, 793–800. [Google Scholar] [CrossRef] [PubMed]
- Kumar, V.L.; Itthagarun, A.; King, N.M. The effect of casein phosphopeptide-amorphous calcium phosphate on remineralization of artificial caries-like lesions: An in vitro study. Aust. Dent. J. 2008, 53, 34–40. [Google Scholar] [CrossRef] [PubMed]
- Cao, Y.; Mei, M.L.; Xu, J.; Lo, E.C.; Li, Q.; Chu, C.H. Biomimetic mineralisation of phosphorylated dentine by CPP-ACP. J. Dent. 2013, 41, 818–825. [Google Scholar] [CrossRef] [PubMed]
- Rahiotis, C.; Vougiouklakis, G. Effect of a CPP-ACP agent on the demineralization and remineralization of dentine in vitro. J. Dent. 2007, 35, 695–698. [Google Scholar] [CrossRef] [PubMed]
- Sattabanasuk, V.; Burrow, M.F.; Shimada, Y.; Tagami, J. Resin bonding to dentine after casein phosphopeptide-amorphous calcium phosphate (CPP-ACP) treatments. J. Adhes. Sci. Technol. 2009, 23, 1149–1161. [Google Scholar] [CrossRef]
- Adebayo, O.A.; Burrow, M.F.; Tyas, M.J. Resin-dentine interfacial morphology following CPP-ACP treatment. J. Dent. 2010, 38, 96–105. [Google Scholar] [CrossRef] [PubMed]
- Rahiotis, C.; Vougiouklakis, G.; Eliades, G. Characterization of oral films formed in the presence of a CPP-ACP agent: An in situ study. J. Dent. 2008, 36, 272–280. [Google Scholar] [CrossRef] [PubMed]
- Jee, S.S.; Thula, T.T.; Gower, L.B. Development of bone-like composites via the polymer-induced liquid-precursor (PILP) process. Part 1: Influence of polymer molecular weight. Acta Biomater. 2010, 6, 3676–3686. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Gu, L.; Breschi, L.; Tjäderhane, L.; Choi, K.K.; Pashley, D.H.; Tay, F.R. Implication of ethanol wet-bonding in hybrid layer remineralization. J. Dent. Res. 2010, 89, 575–580. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.Y.; Zhang, L.; Chen, J.H. The role of dentinal matrix metalloproteinases in collagenous degeneration of tooth tissue. Zhonghua Kou Qiang Yi Xue Za Zhi 2011, 46, 379–381. [Google Scholar] [PubMed]
- Cao, Y.; Liu, W.; Ning, T.; Mei, M.L.; Li, Q.L.; Lo, E.C.; Chu, C.H. A novel oligopeptide simulating dentine matrix protein 1 for biomimetic mineralization of dentine. Clin. Oral. Investig. 2014, 18, 873–881. [Google Scholar] [CrossRef] [PubMed]
- Aggeli, A.; Bell, M.; Boden, N.; Carrick, L.M.; Strong, A.E. Self-assembling peptide polyelectrolyte beta-sheet complexes form nematic hydrogels. Angew. Chem. 2003, 42, 5761–5764. [Google Scholar] [CrossRef]
- Kirkham, J.; Firth, A.; Vernals, D.; Boden, N.; Robinson, C.; Shore, R.C.; Brookes, S.J.; Aggeli, A. Self-assembling peptide scaffolds promote enamel remineralization. J. Dent. Res. 2007, 86, 426–430. [Google Scholar] [CrossRef] [PubMed]
- ten Cate, J.M. Remineralization of caries lesions extending into dentin. J. Dent. Res. 2001, 80, 1407–1411. [Google Scholar] [CrossRef] [PubMed]
- Marshall, G.W., Jr.; Balooch, M.; Kinney, J.H.; Marshall, S.J. Atomic force microscopy of conditioning agents on dentin. J. Biomed. Mater. Res. 1995, 29, 1381–1387. [Google Scholar] [CrossRef] [PubMed]
- Kato, M.T.; Bolanho, A.; Zarella, B.L.; Salo, T.; Tjäderhane, L.; Buzalaf, M.A. Sodium fluoride inhibits MMP-2 and MMP-9. J. Dent. Res. 2014, 93, 74–77. [Google Scholar] [CrossRef] [PubMed]
- Altinci, P.; Mutluay, M.; Seseogullari-Dirihan, R.; Pashley, D.; Tjäderhane, L.; Tezvergil-Mutluay, A. NaF inhibits matrix-bound cathepsin-mediated dentin matrix degradation. Caries Res. 2016, 50, 124–132. [Google Scholar] [CrossRef] [PubMed]
- Arends, J.; Christoffersen, J. Nature and role of loosely bound fluoride in dental caries. J. Dent. Res. 1990, 69, 601–605. [Google Scholar] [CrossRef] [PubMed]
- Arends, J.; Christoffersen, J.; Ruben, J.; Jongebloed, W.L. Remineralization of bovine dentine in vitro. The influence of the F content in solution on mineral distribution. Caries Res. 1989, 23, 309–314. [Google Scholar] [CrossRef] [PubMed]
- Prabhakar, A.R.; Manojkumar, A.J.; Basappa, N. In vitro remineralization of enamel subsurface lesions and assessment of dentine tubule occlusion from NaF dentifrices with and without calcium. J. Indian Soc. Pedodontics Prev. Dent. 2013, 31, 29–35. [Google Scholar] [CrossRef] [PubMed]
- Comar, L.P.; Souza, B.M.; Gracindo, L.F.; Buzalaf, M.A.; Magalhães, A.C. Impact of experimental nano-HAP pastes on bovine enamel and dentin submitted to a pH cycling model. Braz. Dent. J. 2013, 24, 273–278. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Materials (Manufactures) | Main Components | Batch Number | Application Mode |
|---|---|---|---|
| 0.2% NaF Solution | 0.2 g of NaF in 100 mL deionized water | Made in the Lab * | 1. Apply 1.0 mL of 0.2% NaF solution |
| Ca2+ and PO43− Solution | Saturated solution of Ca2+ and PO43− (1.5 mmol/L calcium, 0.9 mmol/L phosphate, and 150 mmol/L KCl in 20 mmol/L cacodylic buffer, pH 7.0) [24]. | Made in the Lab | 1. Apply 0.1 mL of Ca2+ and PO43− solution |
| MI™ Paste—GC Internacional, Itabashi-ku, Tóquio, Japão | Glycerol, CPP-ACP, D-Sorbitol, Propylene glycol, Titanium dioxide and silicon | N2347319 | 1. Apply 0.1 mL of MI™ Paste |
| Curodont™ Repair—Credentis AG, Dorfstrasse, Windisch, Switzerland | P11-4 peptide—amino acid sequence—(Ace-Gln-Gln-Arg-Phe-Glu-Trp-Glu-Phe-Glu-Gln-Gln-NH2) | N342x | 1. Apply 50 µL of Curodont™ Repair for 5 min 2. Apply 0.1 mL of Ca2+ and PO43− solution |
| Scotchbond™ Universal Etchant—3M ESPE; St Paul, MN, USA | 32% phosphoric acid | N345 | 1. Apply etchant for 15 s 2. Rinse for 10 s |
| Adper Single Bond 2.0—3M ESPE; St Paul, MN, USA | HEMA, water, ethanol, Bis-GMA, dimethacrylates, amines, metacrylate functional copolymer of polyacrylic and polyitaconic acids, 10% by weight of 5 nanometer-diameter spherical sílica particles | N42912 | 3. Blot water excess 4. Apply 2 consecutive coats of adhesive for 15 s with gentle agitation 5. Gently air dry for 5 s 6. Light-cure for 10 s |
| Filtek™ Z350 XT—3M ESPE; St Paul, MN, USA | BIS-GMA, Bis-EMA, UDMA, TEG-DMA, camphorquinone, non-agglomerated silica nanoparticles | N98354 | 1. Incremental insertion 2 mm 2. Light-cure for 20 s |
| Experimental Groups | Artificial Caries Development Models | |
|---|---|---|
| Chemical Model | Biological Model | |
| Sound Dentin | 43.32 ± 4.35 | |
| Demineralized Dentin | 21.96 ± 5.92 Ca * | 22.89 ± 2.68 Da * |
| Demineralized Dentin + NaF | 33.43 ± 10.42 Ba * | 26.94 ± 6.70 Cb * |
| Demineralized Dentin + MI Paste™ (CPP-ACP) | 45.25 ± 8.83 Aa * | 47.95 ± 6.69 Aa * |
| Demineralized Dentin + Curodont™ Repair (P11-4) | 46.42 ± 12.03 Aa * | 42.07 ± 7.83 Bb |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barbosa-Martins, L.F.; Sousa, J.P.d.; Alves, L.A.; Davies, R.P.W.; Puppin-Rontanti, R.M. Biomimetic Mineralizing Agents Recover the Micro Tensile Bond Strength of Demineralized Dentin. Materials 2018, 11, 1733. https://doi.org/10.3390/ma11091733
Barbosa-Martins LF, Sousa JPd, Alves LA, Davies RPW, Puppin-Rontanti RM. Biomimetic Mineralizing Agents Recover the Micro Tensile Bond Strength of Demineralized Dentin. Materials. 2018; 11(9):1733. https://doi.org/10.3390/ma11091733
Chicago/Turabian StyleBarbosa-Martins, Luiz Filipe, Jossaria Pereira de Sousa, Lívia Araújo Alves, Robert Philip Wynn Davies, and Regina Maria Puppin-Rontanti. 2018. "Biomimetic Mineralizing Agents Recover the Micro Tensile Bond Strength of Demineralized Dentin" Materials 11, no. 9: 1733. https://doi.org/10.3390/ma11091733
APA StyleBarbosa-Martins, L. F., Sousa, J. P. d., Alves, L. A., Davies, R. P. W., & Puppin-Rontanti, R. M. (2018). Biomimetic Mineralizing Agents Recover the Micro Tensile Bond Strength of Demineralized Dentin. Materials, 11(9), 1733. https://doi.org/10.3390/ma11091733