Prevention and Killing Efficacy of Carbapenem Resistant Enterobacteriaceae (CRE) and Vancomycin Resistant Enterococci (VRE) Biofilms by Antibiotic-Loaded Calcium Sulfate Beads

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Strains and Culture Conditions
2.2. Determination of Minimum Inhibitory Concentration (MIC) of Antibiotics Against CRE and VRE
2.3. Preparation of Antibiotic-Loaded Calcium Sulfate Beads (ALCSB)
2.4. Modified Kirby–Bauer Assay for Assessing the Repeat Zone of Inhibition (ZOI)
2.5. ALCSBs for Preventing Biofilm Formation
2.6. ALCSBs Killing Efficacy of Preformed Biofilms
2.7. Statistics
3. Results
3.1. Modified Kirby–Bauer Assay for Assessing the Repeat Zone of Inhibition (ZOI)
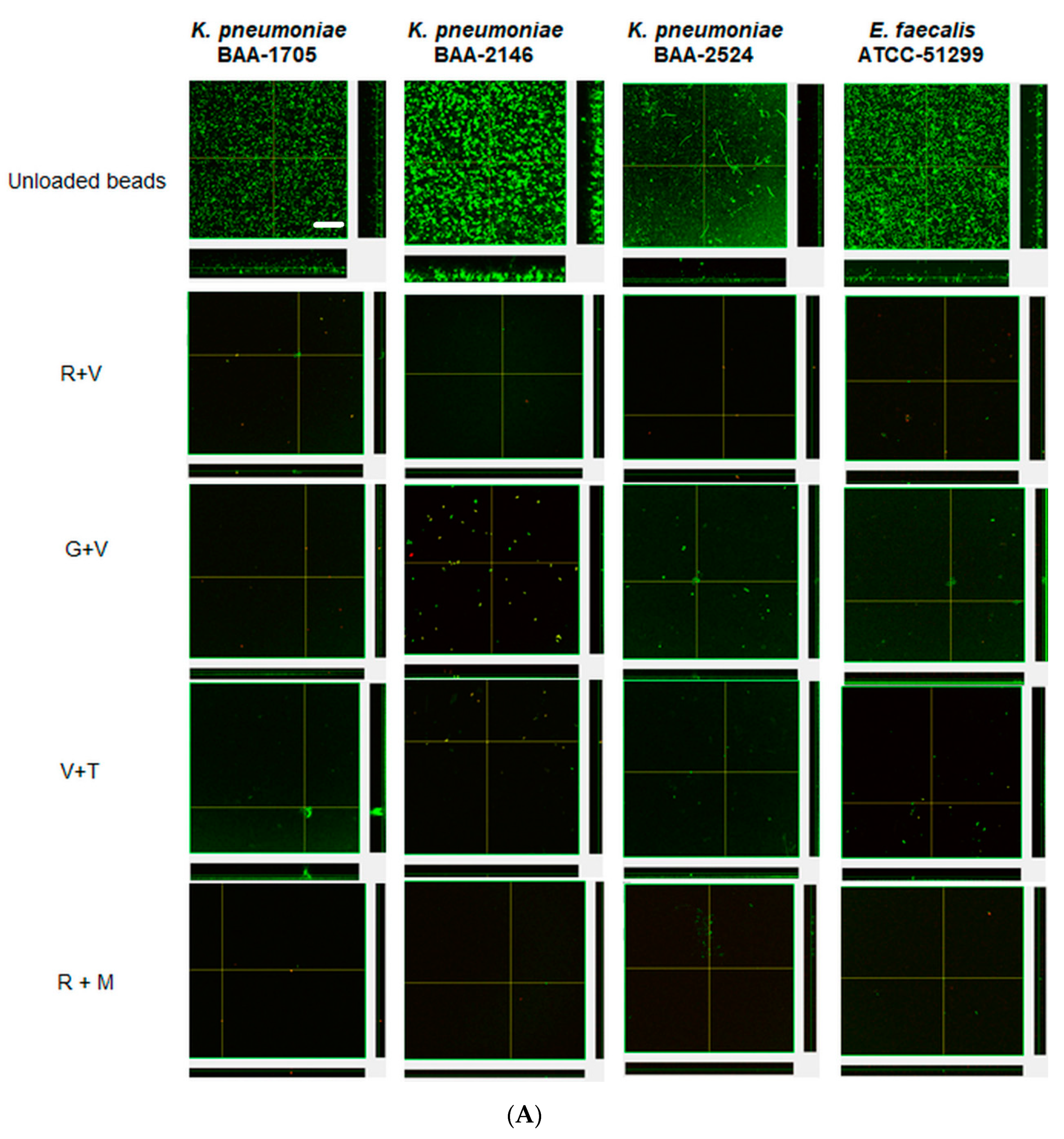
3.2. ALCSBs for Preventing Biofilm Formation
3.3. ALCSBs Killing Efficacy of Preformed Biofilms
4. Discussion
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Gutiérrez-Gutiérrez, B.; Sojo-Dorado, J.; Bravo-Ferrer, J.; Cuperus, N.; De Kraker, M.; Kostyanev, T.; Raka, L.; Daikos, G.; Feifel, J.; Folgori, L. EUropean prospective cohort study on Enterobacteriaceae showing REsistance to CArbapenems (EURECA): A protocol of a European multicentre observational study. BMJ Open 2017, 7, e015365. [Google Scholar] [CrossRef] [Green Version]
- Magill, S.S.; Edwards, J.R.; Bamberg, W.; Beldavs, Z.G.; Dumyati, G.; Kainer, M.A.; Lynfield, R.; Maloney, M.; McAllister-Hollod, L.; Nadle, J. Multistate point-prevalence survey of health care—Associated infections. N. Engl. J. Med. 2014, 370, 1198–1208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arias, C.A.; Murray, B.E. Emergence and management of drug-resistant enterococcal infections. Expert Rev. Anti-Infect. Ther. 2008, 6, 637–655. [Google Scholar] [CrossRef] [PubMed]
- Gupta, N.; Limbago, B.M.; Patel, J.B.; Kallen, A.J. Carbapenem-resistant Enterobacteriaceae: Epidemiology and prevention. Clin. Infect. Dis. 2011, 53, 60–67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Safdar, N.; Maki, D.G. The commonality of risk factors for nosocomial colonization and infection with antimicrobial-resistant Staphylococcus aureus, enterococcus, gram-negative bacilli, Clostridium difficile, and Candida. Ann. Intern. Med. 2002, 136, 834–844. [Google Scholar] [CrossRef] [PubMed]
- Aggarwal, V.K.; Rasouli, M.R.; Parvizi, J. Periprosthetic joint infection: Current concept. Indian J. Orthop. 2013, 47, 10. [Google Scholar]
- Tande, A.J.; Patel, R. Prosthetic joint infection. Clin. Microbiol. Rev. 2014, 27, 302–345. [Google Scholar] [CrossRef] [Green Version]
- Tzeng, A.; Tzeng, T.H.; Vasdev, S.; Korth, K.; Healey, T.; Parvizi, J.; Saleh, K.J. Treating periprosthetic joint infections as biofilms: Key diagnosis and management strategies. Diagn. Microbiol. Infect. Dis. 2015, 81, 192–200. [Google Scholar] [CrossRef]
- Kheir, M.M.; Tan, T.L.; Higuera, C.; George, J.; Della Valle, C.J.; Shen, M.; Parvizi, J. Periprosthetic joint infections caused by enterococci have poor outcomes. J. Arthroplast. 2017, 32, 933–947. [Google Scholar] [CrossRef] [PubMed]
- De Sanctis, J.; Teixeira, L.; Van Duin, D.; Odio, C.; Hall, G.; Tomford, J.W.; Perez, F.; Rudin, S.D.; Bonomo, R.A.; Barsoum, W.K. Complex prosthetic joint infections due to carbapenemase-producing Klebsiella pneumoniae: A unique challenge in the era of untreatable infections. Int. J. Infect. Dis. 2014, 25, 73–78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Howlin, R.; Brayford, M.; Webb, J.; Cooper, J.; Aiken, S.; Stoodley, P. Antibiotic-loaded synthetic calcium sulfate beads for prevention of bacterial colonization and biofilm formation in periprosthetic infections. Antimicrob. Agents Chemother. 2015, 59, 111–120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Costerton, J.W. Biofilm theory can guide the treatment of device-related orthopaedic infections. Clin. Orthop. Relat. Res.® 2005, 437, 7–11. [Google Scholar] [CrossRef] [PubMed]
- Gristina, A.G.; Costerton, J. Bacterial adherence to biomaterials and tissue. The significance of its role in clinical sepsis. JBJS 1985, 67, 264–273. [Google Scholar] [CrossRef]
- Jämsen, E.; Huhtala, H.; Puolakka, T.; Moilanen, T. Risk factors for infection after knee arthroplasty: A register-based analysis of 43,149 cases. JBJS 2009, 91, 38–47. [Google Scholar] [CrossRef] [PubMed]
- Parvizi, J.; Saleh, K.J.; Ragland, P.S.; Pour, A.E.; Mont, M.A. Efficacy of antibiotic-impregnated cement in total hip replacement. Acta Orthop. 2008, 79, 335–341. [Google Scholar] [CrossRef]
- McPherson, E.; Dipane, M.; Sherif, S. Dissolvable antibiotic beads in treatment of periprosthetic joint infection and revision arthroplasty-the use of synthetic pure calcium sulfate (Stimulan®) impregnated with vancomycin & tobramycin. Reconstr. Rev. 2013, 3. [Google Scholar] [CrossRef] [Green Version]
- Lum, Z.C.; Pereira, G.C. Local bio-absorbable antibiotic delivery in calcium sulfate beads in hip and knee arthroplasty. J. Orthop. 2018, 15, 676–678. [Google Scholar] [CrossRef]
- Mandell, J.B.; Orr, S.; Koch, J.; Nourie, B.; Ma, D.; Bonar, D.D.; Shah, N.; Urish, K.L. Large variations in clinical antibiotic activity against Staphylococcus aureus biofilms of periprosthetic joint infection isolates. J. Orthop. Res.® 2019, 37, 1604–1609. [Google Scholar] [CrossRef]
- Laycock, P.A.; Cooper, J.J.; Howlin, R.P.; Delury, C.; Aiken, S.; Stoodley, P. In vitro efficacy of antibiotics released from calcium sulfate bone void filler beads. Materials 2018, 11, 2265. [Google Scholar] [CrossRef] [Green Version]
- Dusane, D.H.; Brooks, J.R.; Sindeldecker, D.; Peters, C.W.; Li, A.; Farrar, N.R.; Diamond, S.M.; Knecht, C.S.; Plaut, R.D.; Delury, C. Complete Killing of Agar Lawn Biofilms by Systematic Spacing of Antibiotic-Loaded Calcium Sulfate Beads. Materials 2019, 12, 4052. [Google Scholar] [CrossRef] [Green Version]
- Jiranek, W.A.; Hanssen, A.D.; Greenwald, A.S. Antibiotic-loaded bone cement for infection prophylaxis in total joint replacement. J. Bone Jt. Surg. 2006, 88, 2487–2500. [Google Scholar] [CrossRef] [PubMed]
- Kenna, D.M.; Irojah, B.B.; Mudge, K.; Eveler, K. Absorbable Antibiotic Beads Prophylaxis in Immediate Breast Reconstruction. Plast. Reconstr. Surg. 2018, 141, 486e–492e. [Google Scholar] [CrossRef] [PubMed]
- Trujillo, J.M.; Logue, M.E.; Kunkel, R.; Demas, C.P. Off-label Usage of Absorbable Beads Containing Antibiotics for Prevention of Surgical Site Infections. Wounds 2017, 29, E84–E87. [Google Scholar] [CrossRef] [PubMed]
- Kallala, R.; Harris, W.E.; Ibrahim, M.; Dipane, M.; McPherson, E. Use of Stimulan absorbable calcium sulphate beads in revision lower limb arthroplasty: Safety profile and complication rates. Bone Jt. Res. 2018, 7, 570–579. [Google Scholar] [CrossRef] [PubMed]
- Maale, G.E.; Eager, J.J.; Mohammadi, D.K.; Calderon, F.A. Elution Profiles of Synthetic CaSO. Eur. J. Drug Metab. Pharmacokinet. 2020, 1–9. [Google Scholar] [CrossRef]
- Geladari, A.; Simitsopoulou, M.; Antachopoulos, C.; Roilides, E. Dose-Dependent Synergistic Interactions of Colistin with Rifampin, Meropenem, and Tigecycline against Carbapenem-Resistant Klebsiella pneumoniae Biofilms. Antimicrob. Agents Chemother. 2019, 63. [Google Scholar] [CrossRef] [Green Version]
- Houlihan, H.H.; Mercier, R.C.; Rybak, M.J. Pharmacodynamics of vancomycin alone and in combination with gentamicin at various dosing intervals against methicillin-resistant Staphylococcus aureus-infected fibrin-platelet clots in an in vitro infection model. Antimicrob. Agents Chemother. 1997, 41, 2497–2501. [Google Scholar] [CrossRef] [Green Version]
- Douthit, C.; Gudenkauf, B.; Hamood, A.; Mudaliar, N.; Caroom, C.; Jenkins, M. Effects of powdered rifampin and vancomycin solutions on biofilm production of staphylococcus aureus on orthopedic implants. J. Clin. Orthop. Trauma 2020, 11, S113–S117. [Google Scholar] [CrossRef]
- Pavoni, G.L.; Giannella, M.; Falcone, M.; Scorzolini, L.; Liberatore, M.; Carlesimo, B.; Serra, P.; Venditti, M. Conservative medical therapy of prosthetic joint infections: Retrospective analysis of an 8-year experience. Clin. Microbiol. Infect. 2004, 10, 831–837. [Google Scholar] [CrossRef] [Green Version]
- Kresken, M.; Körber-Irrgang, B. Performance of the Etest for susceptibility testing of Enterobacterales (Enterobacteriaceae) and Pseudomonas aeruginosa towards ceftazidime-avibactam. J. Clin. Microbiol. 2018, 56, e00528-18. [Google Scholar] [CrossRef] [Green Version]
- Kahlmeter, G.; Brown, D. Chapter 9. Laboratory control of antimicrobial therapy. In Antibiotic and Chemotherapy: Anti-infective Agents and Their Use in Therapy, 8th eds.; Finch, R.G., Greenwood, D., Norrby, S.R., Whitley, R.J., Eds.; Churchill Livingstone: London, UK, 2003; pp. 115–122. [Google Scholar]
- Li, J.; Liu, F.; Wang, Q.; Ge, P.; Woo, P.C.; Yan, J.; Zhao, Y.; Gao, G.F.; Liu, C.H.; Liu, C. Genomic and transcriptomic analysis of NDM-1 Klebsiella pneumoniae in spaceflight reveal mechanisms underlying environmental adaptability. Sci. Rep. 2014, 4, 6216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Warn, P.; Thommes, P.; Vaddi, S.; Corbett, D.; Coles, D.; Vaccaro, L.; Lister, T.; Parr Jr, T. In Vivo Efficacy of Combinations of Novel Antimicrobial Peptide Spr741 and Rifampicin in Short-Duration Murine Thigh Infection Models of Gram-Negative Bacterial Infection. Poster Monday-561. In Proceedings of the ASM Microbe 2016—American Society for Microbiology Conference, Boston, CA, USA, 16–20 June 2016. [Google Scholar]
- Chen, X.; Liu, Y.; Wang, C.; Hu, X.; Wu, Y.; Zhang, Y.; Bian, C.; You, X.; Hu, L. Synthesis and in vitro activity of asymmetric indole-based bisamidine compounds against Gram-positive and Gram-negative pathogens. Bioorg. Med. Chem. Lett. 2020, 30, 126887. [Google Scholar] [CrossRef]
- Munson, E.; Huband, M.D.; Castanheira, M.; Fedler, K.A.; Flamm, R.K. Determination of MIC and disk diffusion quality control guidelines for meropenem–vaborbactam, a novel carbapenem/boronic acid β-lactamase inhibitor combination. Diagn. Microbiol. Infect. Dis. 2018, 90, 324–328. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chaudhary, M.; Payasi, A. Antimicrobial susceptibility patterns and molecular characterization of Klebsiella pneumoniae clinical isolates from north Indian patients. Int. J. Med. Med. Sci. 2013, 46, 1218–1224. [Google Scholar]
- Ng, S.M.S.; Sioson, J.S.P.; Yap, J.M.; Ng, F.M.; Ching, H.S.V.; Teo, J.W.P.; Jureen, R.; Hill, J.; Chia, C.S.B. Repurposing Zidovudine in combination with Tigecycline for treating carbapenem-resistant Enterobacteriaceae infections. Eur. J. Clin. Microbiol. Infect. Dis. 2018, 37, 141–148. [Google Scholar] [CrossRef] [PubMed]
- Yoneda, A.; Thänert, R.; Burnham, C.-A.D.; Dantas, G. In vitro activity of meropenem/piperacillin/tazobactam triple combination therapy against clinical isolates of Staphylococcus aureus, Staphylococcus epidermidis, Staphylococcus pseudintermedius and vancomycin-resistant Enterococcus spp. Int. J. Antimicrob. Agents 2020, 55, 105864. [Google Scholar] [CrossRef]
- Naghili, H.; Tajik, H.; Mardani, K.; Rouhani, S.M.R.; Ehsani, A.; Zare, P. Validation of drop plate technique for bacterial enumeration by parametric and nonparametric tests. Vet Res Forum. 2013, 4, 179–183. [Google Scholar]
- Ben-David, A.; Davidson, C.E. Estimation method for serial dilution experiments. J. Microbiol. Methods 2014, 107, 214–221. [Google Scholar] [CrossRef] [Green Version]
- Desai, H.; Wong, R.; Pasha, A.K. A novel way of treating multidrug-resistant enterococci. N. Am. J. Med. Sci. 2016, 8, 229. [Google Scholar] [CrossRef] [Green Version]
- Tseng, S.-W.; Chi, C.-Y.; Chou, C.-H.; Wang, Y.-J.; Liao, C.-H.; Ho, C.-M.; Lin, P.-C.; Ho, M.-W.; Wang, J.-H. Eight years experience in treatment of prosthetic joint infections at a teaching hospital in Central Taiwan. J. Microbiol. Immunol. Infect. 2012, 45, 363–369. [Google Scholar] [CrossRef] [Green Version]
- Martinez-Pastor, J.; Vilchez, F.; Pitart, C.; Sierra, J.; Soriano, A. Antibiotic resistance in orthopaedic surgery: Acute knee prosthetic joint infections due to extended-spectrum beta-lactamase (ESBL)-producing Enterobacteriaceae. Eur. J. Clin. Microbiol. Infect. Dis. 2010, 29, 1039–1041. [Google Scholar] [CrossRef]
- Cooper, J.J.; Florance, H.; McKinnon, J.L.; Laycock, P.A.; Aiken, S.S. Elution profiles of tobramycin and vancomycin from high-purity calcium sulphate beads incubated in a range of simulated body fluids. J. Biomater. Appl. 2016, 31, 357–365. [Google Scholar] [CrossRef] [PubMed]
- Aiken, S.S.; Cooper, J.J.; Florance, H.; Robinson, M.T.; Michell, S. Local release of antibiotics for surgical site infection management using high-purity calcium sulfate: An in vitro elution study. Surg. Infect. 2015, 16, 54–61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kanellakopoulou, K.; Panagopoulos, P.; Giannitsioti, E.; Tsaganos, T.; Carrer, D.P.; Efstathopoulos, N.; Giamarellos-Bourboulis, E.J. In vitro elution of daptomycin by a synthetic crystallic semihydrate form of calcium sulfate, stimulan. Antimicrob. Agents Chemother. 2009, 53, 3106–3107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Panagopoulos, P.; Tsaganos, T.; Plachouras, D.; Carrer, D.P.; Papadopoulos, A.; Giamarellou, H.; Kanellakopoulou, K. In vitro elution of moxifloxacin and fusidic acid by a synthetic crystallic semihydrate form of calcium sulphate (StimulanTM). Int. J. Antimicrob. Agents 2008, 32, 485–487. [Google Scholar] [CrossRef] [PubMed]
- McConoughey, S.J.; Howlin, R.; Granger, J.F.; Manring, M.M.; Calhoun, J.H.; Shirtliff, M.; Kathju, S.; Stoodley, P. Biofilms in periprosthetic orthopedic infections. Future Microbiol. 2014, 9, 987–1007. [Google Scholar] [CrossRef] [Green Version]
- Zimmerli, W.; Sendi, P. Role of rifampin against staphylococcal biofilm infections in vitro, in animal models, and in orthopedic-device-related infections. Antimicrob. Agents Chemother. 2019, 63, e01746-18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tyers, M.; Wright, G.D. Drug combinations: A strategy to extend the life of antibiotics in the 21st century. Nat. Rev. Microbiol. 2019, 17, 141–155. [Google Scholar] [CrossRef]
- Karam, G.; Chastre, J.; Wilcox, M.H.; Vincent, J.-L. Antibiotic strategies in the era of multidrug resistance. Crit. Care 2016, 20, 136. [Google Scholar] [CrossRef] [Green Version]
- Zavascki, A.P.; Bulitta, J.B.; Landersdorfer, C.B. Combination therapy for carbapenem-resistant Gram-negative bacteria. Expert Rev. Anti-Infect. Ther. 2013, 11, 1333–1353. [Google Scholar] [CrossRef]
- Thieme, L.; Hartung, A.; Tramm, K.; Klinger-Strobel, M.; Jandt, K.D.; Makarewicz, O.; Pletz, M.W. MBEC Versus MBIC: The Lack of Differentiation between Biofilm Reducing and Inhibitory Effects as a Current Problem in Biofilm Methodology. Biol. Proced. Online 2019, 21, 18. [Google Scholar] [CrossRef]
- Castaneda, P.; McLaren, A.; Tavaziva, G.; Overstreet, D. Biofilm antimicrobial susceptibility increases with antimicrobial exposure time. Clin. Orthop. Relat. Res.® 2016, 474, 1659–1664. [Google Scholar] [CrossRef]
- Nicolau, D.P. Optimizing outcomes with antimicrobial therapy through pharmacodynamic profiling. J. Infect. Chemother. 2003, 9, 292–296. [Google Scholar] [CrossRef] [PubMed]
- Scott, D.M.; Rotschafer, J.C.; Behrens, F. Use of vancomycin and tobramycin polymethylmethacrylate impregnated beads in the management of chronic osteomyelitis. Drug Intell. Clin. Pharm. 1988, 22, 480–483. [Google Scholar] [CrossRef] [PubMed]
- Henry, S.L.; Galloway, K.P. Local antibacterial therapy for the management of orthopaedic infections. Clin. Pharmacokinet. 1995, 29, 36–45. [Google Scholar] [CrossRef] [PubMed]
- Bistolfi, A.; Massazza, G.; Verné, E.; Massè, A.; Deledda, D.; Ferraris, S.; Miola, M.; Galetto, F.; Crova, M. Antibiotic-loaded cement in orthopedic surgery: A review. ISRN Orthop. 2011, 2011. [Google Scholar] [CrossRef]
- Van de Belt, H.; Neut, D.; Schenk, W.; Van Horn, J.R.; Van de Mei, H.C.; Busscher, H.J. Infection of orthopedic implants and the use of antibiotic-loaded bone cements: A review. Acta Orthop. Scand. 2001, 72, 557–571. [Google Scholar] [CrossRef]
- Gogia, J.S.; Meehan, J.P.; Di Cesare, P.E.; Jamali, A.A. Local antibiotic therapy in osteomyelitis. Semin. Plast. Surg. 2009, 23, 100–107. [Google Scholar] [CrossRef] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Antibiotics MIC (µg/mL) | Strains | |||
|---|---|---|---|---|
| KP-1705 | KP-2146 | KP-2524 | EF-51299 | |
| Gentamicin (G) | 64 | >16 [32] | 16 | R |
| Rifampicin (R) | 64 | 16 [33] | 64 | 16 |
| Tobramycin (T) | 512 | >16 [32] | 16 | R |
| Vancomycin (V) | r | >128 [34] | R | 128 |
| Meropenem (M) | 8–64 [35] | 16 [36] | 43.75 [37] | 8 [38] |
| Antibiotics | Unloaded (U) | R + V | G + V | V + T | R + M |
|---|---|---|---|---|---|
| Rifampicin (R) | 0 | 600 mg/10cc (25 mg/mL) | 0 | 0 | 600 mg/10 cc (25 mg/mL) |
| Vancomycin (V) | 0 | 1000 mg/10cc (41.6 mg/mL) | 500 mg/10 cc (20.8 mg/mL) | 1000 mg/10 cc (41.6 mg/mL) | 0 |
| Gentamicin (G) | 0 | 0 | 240 mg/10 cc (10 mg/mL) | 0 | 0 |
| Meropenem (M) | 0 | 0 | 0 | 0 | 500 mg/10 cc (20.8 mg/mL) |
| Tobramycin (T) | 0 | 0 | 0 | 240 mg/10 cc (10 mg/mL) | 0 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stoodley, P.; Brooks, J.; Peters, C.W.; Jiang, N.; Delury, C.P.; Laycock, P.A.; Aiken, S.S.; Dusane, D.H. Prevention and Killing Efficacy of Carbapenem Resistant Enterobacteriaceae (CRE) and Vancomycin Resistant Enterococci (VRE) Biofilms by Antibiotic-Loaded Calcium Sulfate Beads. Materials 2020, 13, 3258. https://doi.org/10.3390/ma13153258
Stoodley P, Brooks J, Peters CW, Jiang N, Delury CP, Laycock PA, Aiken SS, Dusane DH. Prevention and Killing Efficacy of Carbapenem Resistant Enterobacteriaceae (CRE) and Vancomycin Resistant Enterococci (VRE) Biofilms by Antibiotic-Loaded Calcium Sulfate Beads. Materials. 2020; 13(15):3258. https://doi.org/10.3390/ma13153258
Chicago/Turabian StyleStoodley, Paul, Jacob Brooks, Casey W. Peters, Nan Jiang, Craig P. Delury, Phillip A. Laycock, Sean S. Aiken, and Devendra H. Dusane. 2020. "Prevention and Killing Efficacy of Carbapenem Resistant Enterobacteriaceae (CRE) and Vancomycin Resistant Enterococci (VRE) Biofilms by Antibiotic-Loaded Calcium Sulfate Beads" Materials 13, no. 15: 3258. https://doi.org/10.3390/ma13153258
APA StyleStoodley, P., Brooks, J., Peters, C. W., Jiang, N., Delury, C. P., Laycock, P. A., Aiken, S. S., & Dusane, D. H. (2020). Prevention and Killing Efficacy of Carbapenem Resistant Enterobacteriaceae (CRE) and Vancomycin Resistant Enterococci (VRE) Biofilms by Antibiotic-Loaded Calcium Sulfate Beads. Materials, 13(15), 3258. https://doi.org/10.3390/ma13153258