Enhancement of Gingival Tissue Adherence of Zirconia Implant Posts: In Vitro Study

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Zirconia Materials
2.2. Dynamic Mechanical Analysis
2.3. Experimental Data Processing
2.4. In Silico Modeling
2.5. Statistical Analysis
3. Results
3.1. Stiffness and Invariant Values Analysis
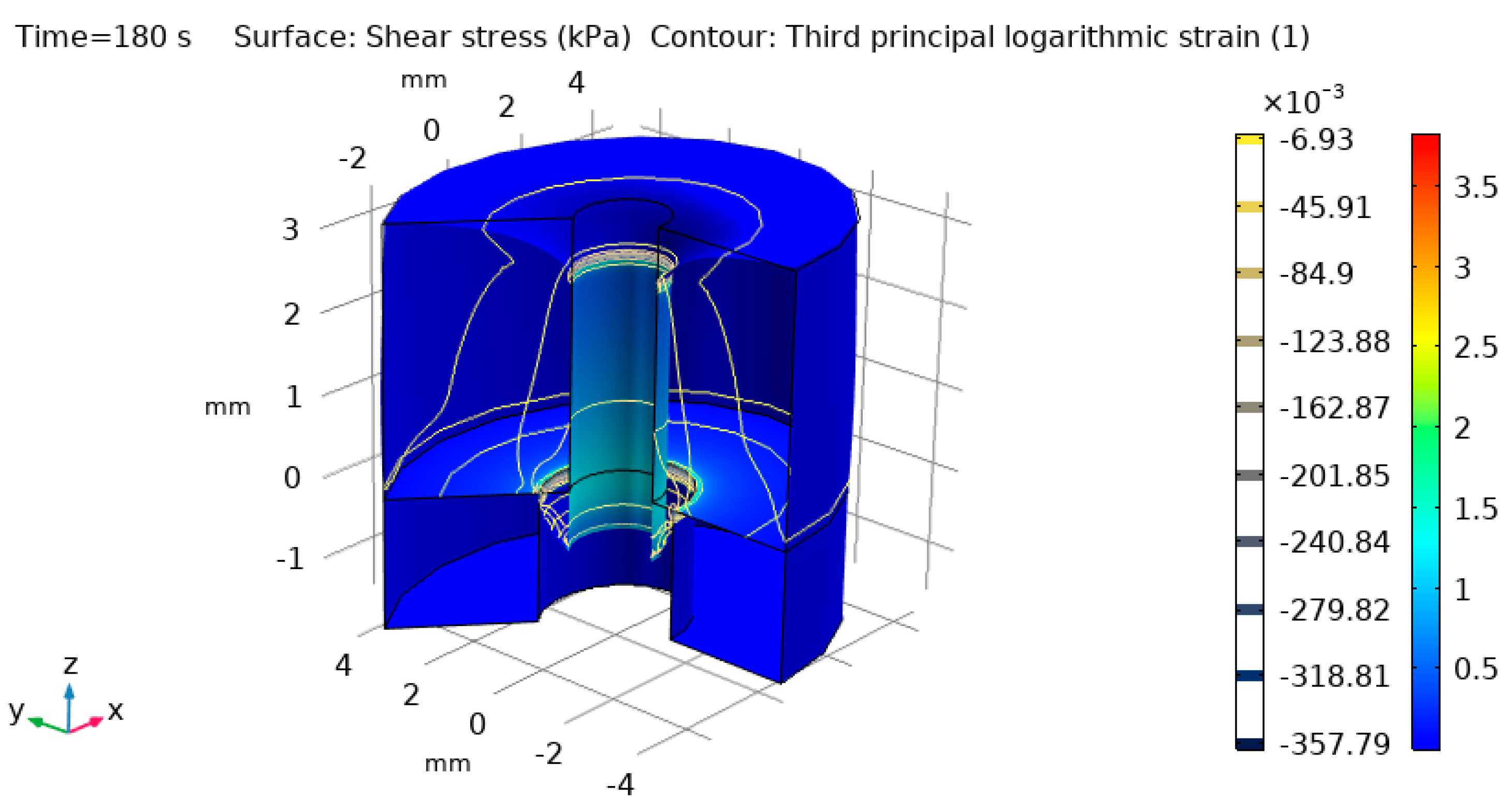
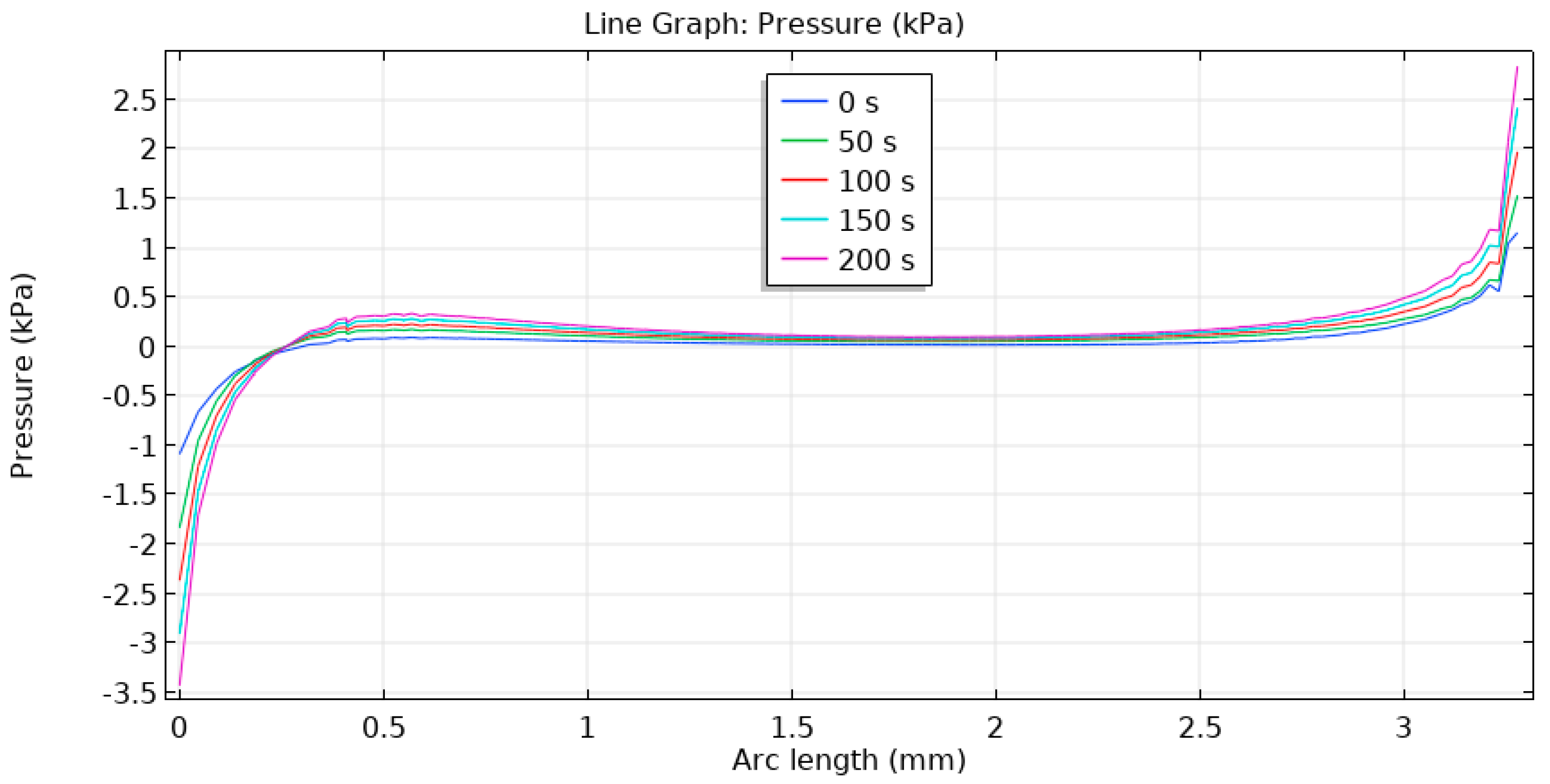
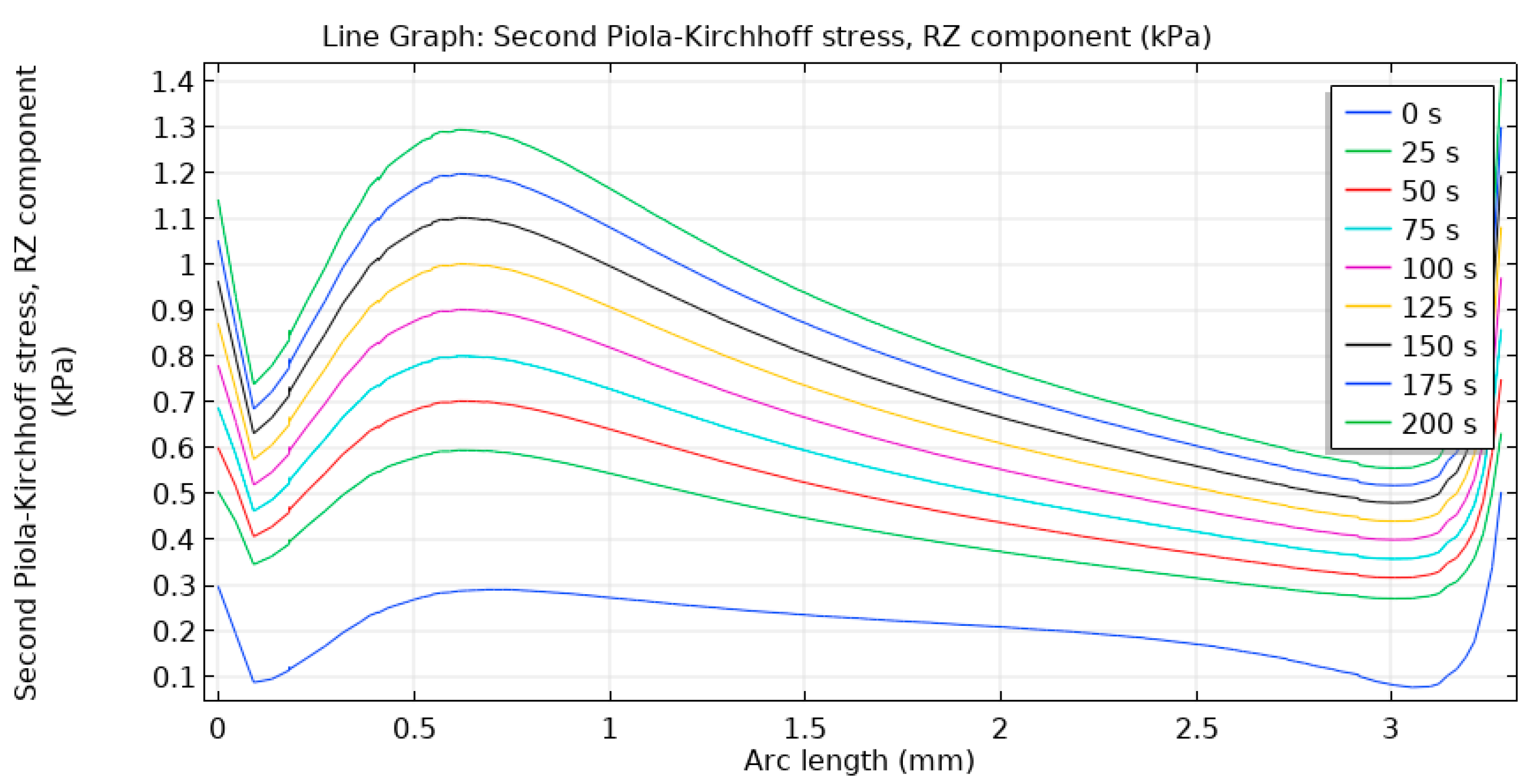
3.2. Computer in Silico Simulation
4. Discussion
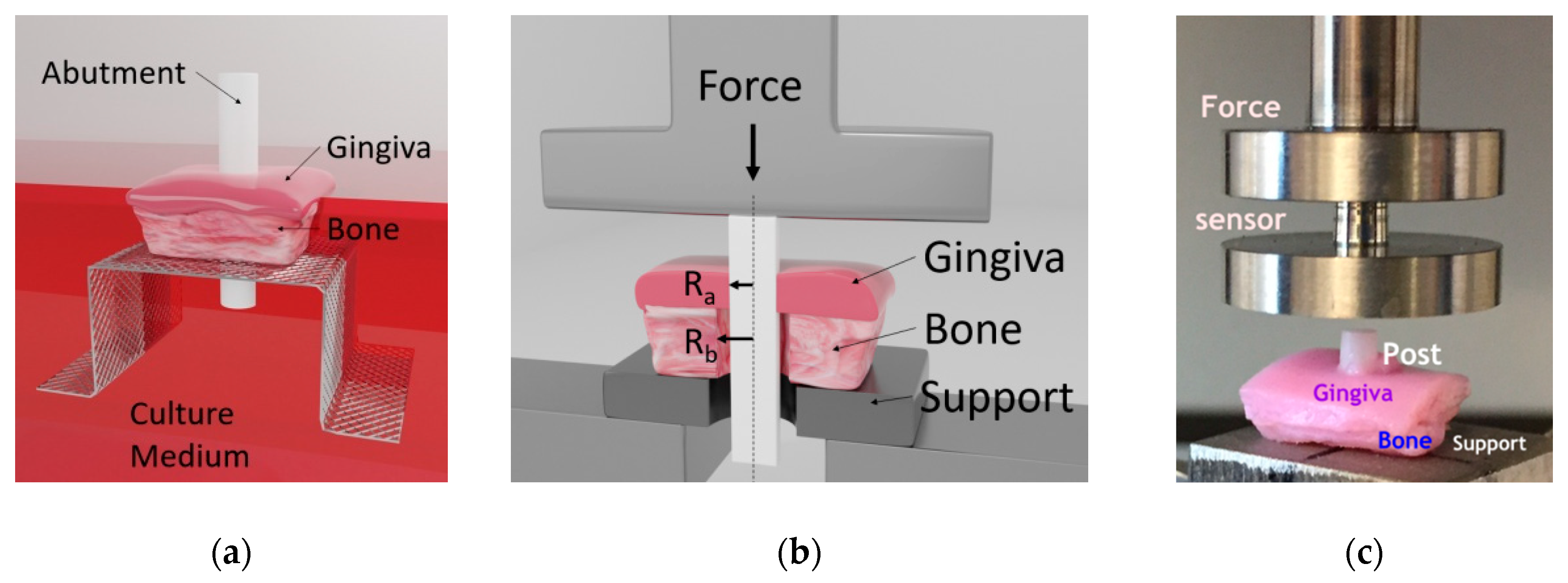
- For in vitro mechanical testing of posts (and likely also full-size abutments) adherence to the gingival tissue it is useful to simulate the “worst case” when the implant fails in osseointegration but when abutment can still prevent pathogens penetration due to its sufficient tissue–abutment interface quality. It is reasonable to assume the abutments (posts) would equally perform in the normal case too when the tissue dynamic displacement is less than 50 μm in amplitude at 1 Hz.
- The tests are needed to be properly planned and executed in the right way to make the design of dental biomaterials with an enhanced clinical value. This concerns samples preparation, test conditions and results analysis.
- For the first time, invariant values (viscostiffness and material memory values) have been extracted from experimental data for these zirconia posts without application or assumption of a material model (viscoelastic or others). These values comprise time-convoluted data and are better predictors for materials performance comparison than traditional stiffness (stress/strain ratios), as the latter depends on the way stresses and strains are defined.
- Invariant values can be used in computer in silico simulations using a simple linear elastic material approach but with the values of elastic properties substituted with these values instead of some constants. This can simplify calculations and extend them into more realistic clinical cases with 3D implant placement planning and outcome estimation.
- An example using in silico simulation has demonstrated that coated zirconia posts would cause low hydrostatic pressure to gingival tissue, which is important to support blood circulation and regeneration of the surrounding tissues. Analogous non-coated zirconia posts would have failed earlier in the same conditions (even if they would have the same or lower pressure values).
5. Conclusions
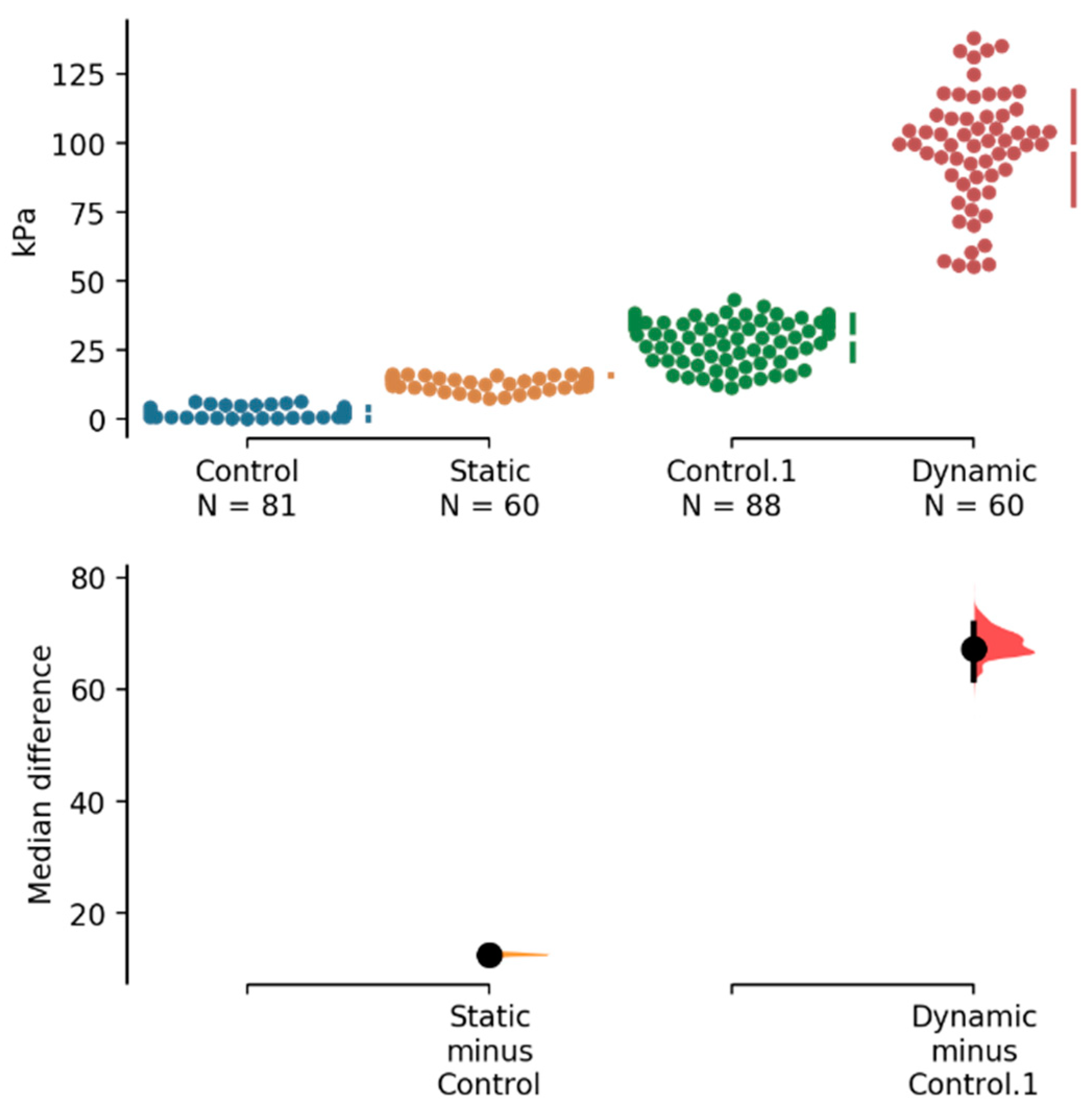
- ~2-fold improvement in static stiffness (stress/strain ratio),
- ~3-fold improvement in dynamic stiffness (dynamic stress/strain ratio),
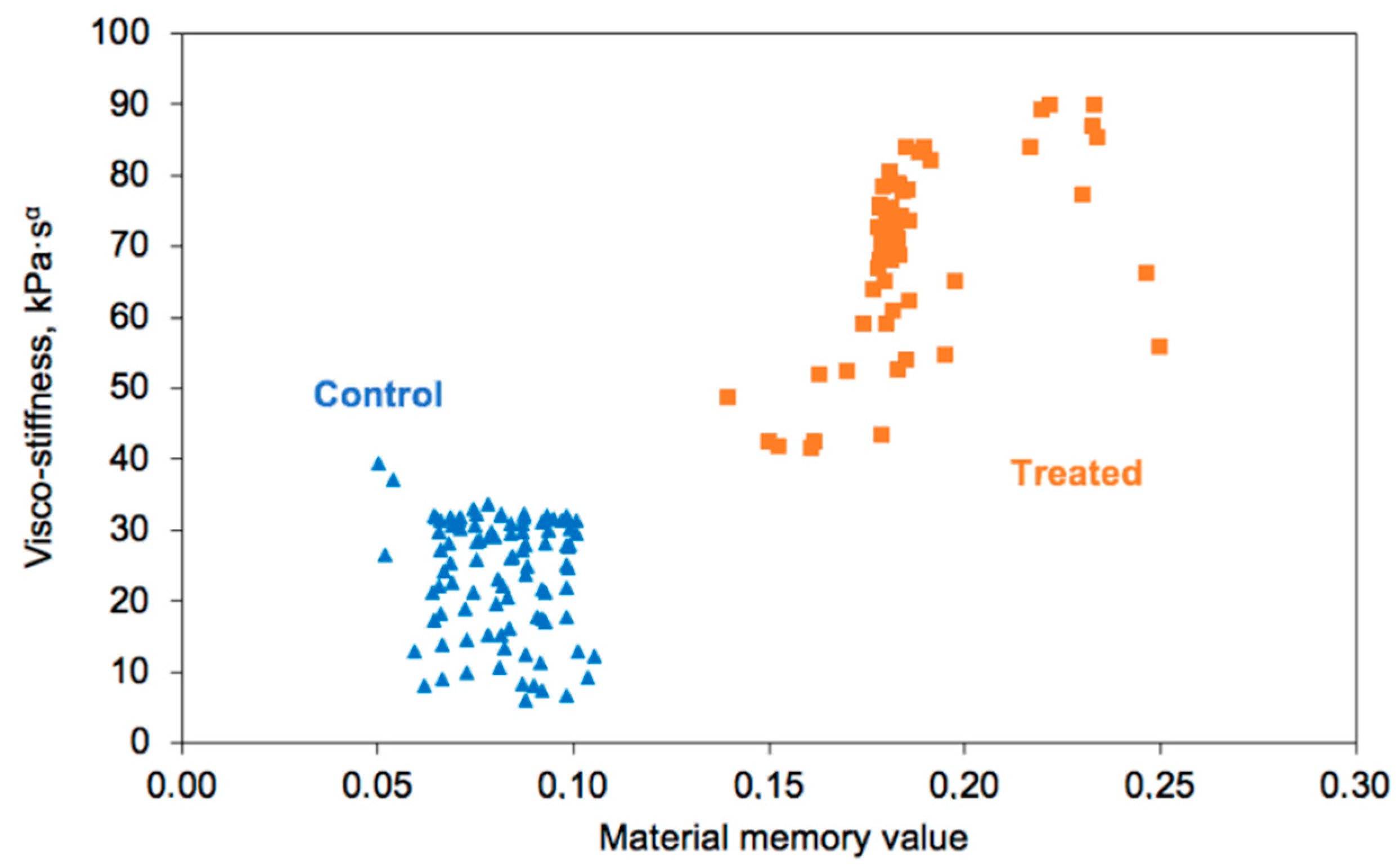
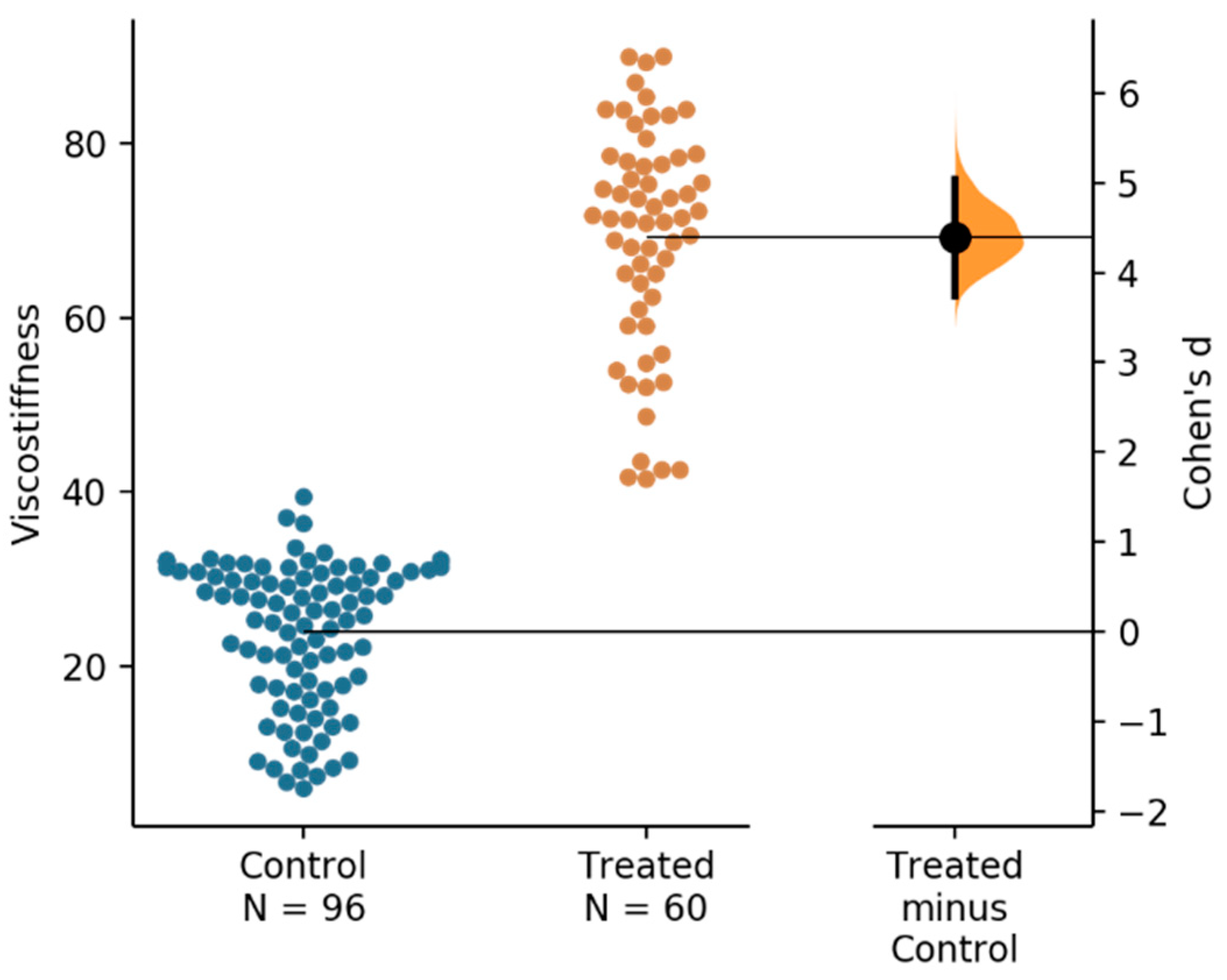
- ~2.5-fold increase in invariant viscostiffness and,
- ~3–4-fold increase in material memory value
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Malet, J.; Mora, F.; Bouchard, F. Implant Dentistry At-A-Glance; John Wiley & Sons: Oxford, UK, 2012; 144p. [Google Scholar]
- Chehroudi, B.; Brunette, D.M. Subcutaneous microfabricated surfaces inhibit epithelial recession and promote long-term survival of percutaneous implants. Biomaterials 2002, 23, 229–237. [Google Scholar] [CrossRef]
- Greenstein, G.; Cavallaro, J.; Romanos, G.; Tarnow, D. Clinical recommendations for avoiding and managing surgical complications associated with implant dentistry: A review. J. Periodontol. 2008, 79, 1317–1329. [Google Scholar] [CrossRef]
- Gehrke, S.A.; Shibli, J.A.; Aramburú, J.S., Jr.; de Val, J.E.M.S.; Girardo, J.L.C.; Dedavid, B.A. Effects of different torque levels on the implant-abutment interface in a conical internal connection. Braz. Oral Res. 2016, 30, e40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goktas, S.; Dmytryk, J.J.; McFetridge, P.S. Biomechanical behavior of oral soft tissues. J. Periodontol. 2011, 82, 1178–1186. [Google Scholar] [CrossRef] [PubMed]
- Davies, D.G.; Parsek, M.R.; Pearson, J.P.; Iglewski, B.H.; Costerton, J.W.; Greenberg, E.P. The involvement of cell-to-cell signals in the development of a bacterial biofilm. Science 1998, 280, 295–298. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wloka, M.; Rehage, H.; Flemming, H.C.; Wingender, J. Structure and rheological behaviour of the extracellular polymeric substance network of mucoid Pseudomonas aeruginosa biofilms. Biofilms 2005, 2, 275–283. [Google Scholar] [CrossRef]
- Haanaes, H.R. Implants and infections with special reference to oral bacteria. J. Clin. Periodontol. 1990, 17, 516–524. [Google Scholar] [CrossRef]
- Rimondini, L.; Gasik, M. Bacterial attachment and biofilm formation on biomaterials: The case of dental and orthopaedic implants. In Biomaterials and Immune Response: Complications, Mechanisms and Immunomodulation; Vrana, E.N., Ed.; CRC Press: Boca Raton, FL, USA, 2018; 249p. [Google Scholar]
- Canullo, L.; Dehner, J.F.; Penarrocha, D.; Checchi, V.; Mazzoni, A.; Breschi, L. Soft tissue response to titanium abutments with different surface treatment: Preliminary histologic report of a randomized controlled trial. BioMed Res. Intern. 2016, 2952530. [Google Scholar] [CrossRef]
- Pereira, J.; Tavares, F.P.; Lima, K.C.; Carreiro, A.F.P.; Henriques, B.; Silva, F.S.; Nascimento, R.M.; Lopez-Lopez, J.; Souza, J.C.M. Relation between dental implant joint surfaces and biofilm formation. Dentistry 2015, 5, 296. [Google Scholar] [CrossRef] [Green Version]
- Gasik, M.; Van Mellaert, L.; Pierron, D.; Braem, A.; Hofmans, D.; De Waelheyns, E.; Anné, J.; Harmand, M.F.; Vleugels, J. Reduction of biofilm infection risks and promotion of osteointegration for optimized surfaces of titanium implants. Adv. Healthc. Mater. 2012, 1, 117–127. [Google Scholar] [CrossRef]
- Shahramian, K.; Gasik, M.; Kangasniemi, I.; Walboomers, F.; Willberg, J.; Abdulmajeed, A.; Närhi, T. Zirconia implants with improved attachment to the gingival tissue. J. Periodontol. 2020, 91, 1213–1224. [Google Scholar] [CrossRef] [PubMed]
- Scarano, A.; Piattelli, M.; Caputi, S.; Favero, G.A.; Piattelli, A. Bacterial adhesion on commercially pure titanium and zirconium oxide disks: An in vivo human study. J. Periodontol. 2004, 75, 292–296. [Google Scholar] [CrossRef] [PubMed]
- Van Brakel, R.; Meijer, G.J.; Verhoeven, J.W.; Jansen, J.; De Putter, C.; Cune, M.S. Soft tissue response to zirconia and titanium implant abutments: An in vivo within-subject comparison. J. Clin. Periodontol. 2012, 39, 995–1001. [Google Scholar] [CrossRef] [PubMed]
- Andersson, B.; Glauser, R.; Maglione, M.; Taylor, Å. Ceramic implant abutments for short-span FPDs: A prospective 5-year multicenter study. Intern. J. Prosthod. 2003, 16, 640–646. [Google Scholar]
- Sivaraman, K.; Chopra, A.; Narayan, A.I.; Balakrishnan, D. Is zirconia a viable alternative to titanium for oral implant? A critical review. J. Prosthodont. Res. 2017, 62, 121–133. [Google Scholar] [CrossRef]
- Matinlinna, J.P. (Ed.) Handbook of Oral Biomaterials; Pan Stanford Publishing Pte. Ltd.: Singapore, 2014. [Google Scholar]
- Lyons, K.; Swain, M. Clinical trials in zirconia: A systematic review. J. Oral Rehabil. 2010, 37, 641–652. [Google Scholar]
- Rompen, E.; Domken, O.; Degidi, M.; Pontes, A.E.P.; Piattelli, A. The effect of material characteristics, of surface topography and of implant components and connections on soft tissue integration: A literature review. Clin. Oral Implants Res. 2006, 17 (Suppl. 2), 55–67. [Google Scholar] [CrossRef]
- Gasik, M.; Bilotsky, Y. In Vitro Method for Measurement and Model-Free Evaluation of Time-Invariant Biomaterials Functions. U.S. Patent 10379106B2, 13 August 2019. [Google Scholar]
- Natali, A.N.; Pavan, P.G.; Scarpa, C. Numerical analysis of tooth mobility: Formulation of a non-linear constitutive law for the periodontal ligament. Dent. Mater. 2004, 20, 623–629. [Google Scholar] [CrossRef]
- Gasik, M. Understanding biomaterial-tissue interface quality: Combined in vitro evaluation. Sci. Technol. Adv. Mater. 2017, 18, 550–562. [Google Scholar] [CrossRef] [Green Version]
- Maslov, V. The characteristics of pseudo-differential operators and difference schemes. Actes Congrès Intern. Math. 1970, 2, 755–769. [Google Scholar]
- Gasik, M. Biomechanical characterization of engineered tissues and implants for tissue/organ replacement applications. In Biomaterials for Organ and Tissue Regeneration; Vrana, N.E., Knopf-Marques, H., Barthes, J., Eds.; Woodhead Publishing: Cambridge, UK, 2020; pp. 599–627. [Google Scholar]
- Xiao, H. Invariant characteristic representations for classical and micropolar anisotropic elasticity tensors. J. Elast. 1995, 40, 239–265. [Google Scholar] [CrossRef]
- Bagley, R.L.; Torvik, P.J. A theoretical basis for the application of fractional calculus to viscoelasticity. J. Rheol. 1983, 27, 201–210. [Google Scholar] [CrossRef]
- Rodríguez, R.F.; Salinas-Rodríguez, E.; Fujioka, J. Fractional time fluctuations in viscoelasticity: A comparative study of correlations and elastic moduli. Entropy 2018, 20, 28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coussot, C.; Kalyanam, S.; Yapp, R.; Insana, M.F. Fractional derivative models for ultrasonic characterization of polymer and breast tissue viscoelasticity. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2009, 56, 715–726. [Google Scholar] [CrossRef] [Green Version]
- Sanctuary, C.S.; Wiskott, H.W.A.; Justiz, J.; Botsis, J.; Belser, U.C. In vitro time-dependent response of periodontal ligament to mechanical loading. J. Appl. Physiol. 2005, 99, 2369–2378. [Google Scholar] [CrossRef] [PubMed]
- Ho, J.; Tumkaya, T.; Aryal, S.; Choi, H.; Claridge-Chang, A. Moving beyond p-values: Everyday data analysis with estimation plots. Nat. Methods 2019, 1548–7105. [Google Scholar] [CrossRef]
- Knowlson, G.T.G.; Basset, H.F.M. The pressures exerted on the trachea by endotracheal inflatable cuffs. Br. J. Anesth. 1970, 42, 834–837. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stoodley, P.; Cargo, R.; Rupp, C.J.; Wilson, S.; Klapper, I. Biofilm material properties as related to shear-induced deformation and detachment phenomena. J. Ind. Microb. Biotechnol. 2002, 29, 361–367. [Google Scholar] [CrossRef]
- Bharate, V.; Kumar, Y.; Koli, D.; Pruthi, G.; Jain, V. Effect of different abutment materials (zirconia or titanium) on the crestal bone height in 1 year. J. Oral Biol. Craniofac. Res. 2019, 10, 372–374. [Google Scholar] [CrossRef]
- Kajiwara, N.; Masaki, C.; Mukaibo, T.; Kondo, Y.; Nakamoto, T.; Hosokawa, R. Soft tissue biological response to zirconia and metal implant abutments compared with natural tooth: Microcirculation monitoring as a novel bioindicator. Implant Dent. 2015, 24, 37–41. [Google Scholar] [CrossRef] [Green Version]
- Wong, J.W.; Gallant-Behm, C.; Wiebe, C.; Mak, K.; Hart, D.A.; Larjava, H.; Häkkinen, L. Wound healing in oral mucosa results in reduced scar formation as compared with skin: Evidence from the red duroc pig model and humans. Wound Repair Regener. 2009, 17, 717–729. [Google Scholar] [CrossRef] [PubMed]
- Han, J.; Zhao, J.; Shen, Z. Zirconia ceramics in metal-free implant dentistry. Adv. Appl. Ceram. 2017, 116, 138–150. [Google Scholar] [CrossRef] [Green Version]
- Denry, I.; Kelly, J.R. State of the art of zirconia for dental applications. Dent. Mater. 2008, 24, 299–307. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Static | Dynamic (1 Hz in This Work) |
|---|---|---|
| Shear stress | ||
| True strain | ||
| Engineering strain |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zühlke, A.; Gasik, M.; Shahramian, K.; Närhi, T.; Bilotsky, Y.; Kangasniemi, I. Enhancement of Gingival Tissue Adherence of Zirconia Implant Posts: In Vitro Study. Materials 2021, 14, 455. https://doi.org/10.3390/ma14020455
Zühlke A, Gasik M, Shahramian K, Närhi T, Bilotsky Y, Kangasniemi I. Enhancement of Gingival Tissue Adherence of Zirconia Implant Posts: In Vitro Study. Materials. 2021; 14(2):455. https://doi.org/10.3390/ma14020455
Chicago/Turabian StyleZühlke, Alexandra, Michael Gasik, Khalil Shahramian, Timo Närhi, Yevgen Bilotsky, and Ilkka Kangasniemi. 2021. "Enhancement of Gingival Tissue Adherence of Zirconia Implant Posts: In Vitro Study" Materials 14, no. 2: 455. https://doi.org/10.3390/ma14020455
APA StyleZühlke, A., Gasik, M., Shahramian, K., Närhi, T., Bilotsky, Y., & Kangasniemi, I. (2021). Enhancement of Gingival Tissue Adherence of Zirconia Implant Posts: In Vitro Study. Materials, 14(2), 455. https://doi.org/10.3390/ma14020455