
Characteristics of Particles and Debris Released after Implantoplasty: A Comparative Study



 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
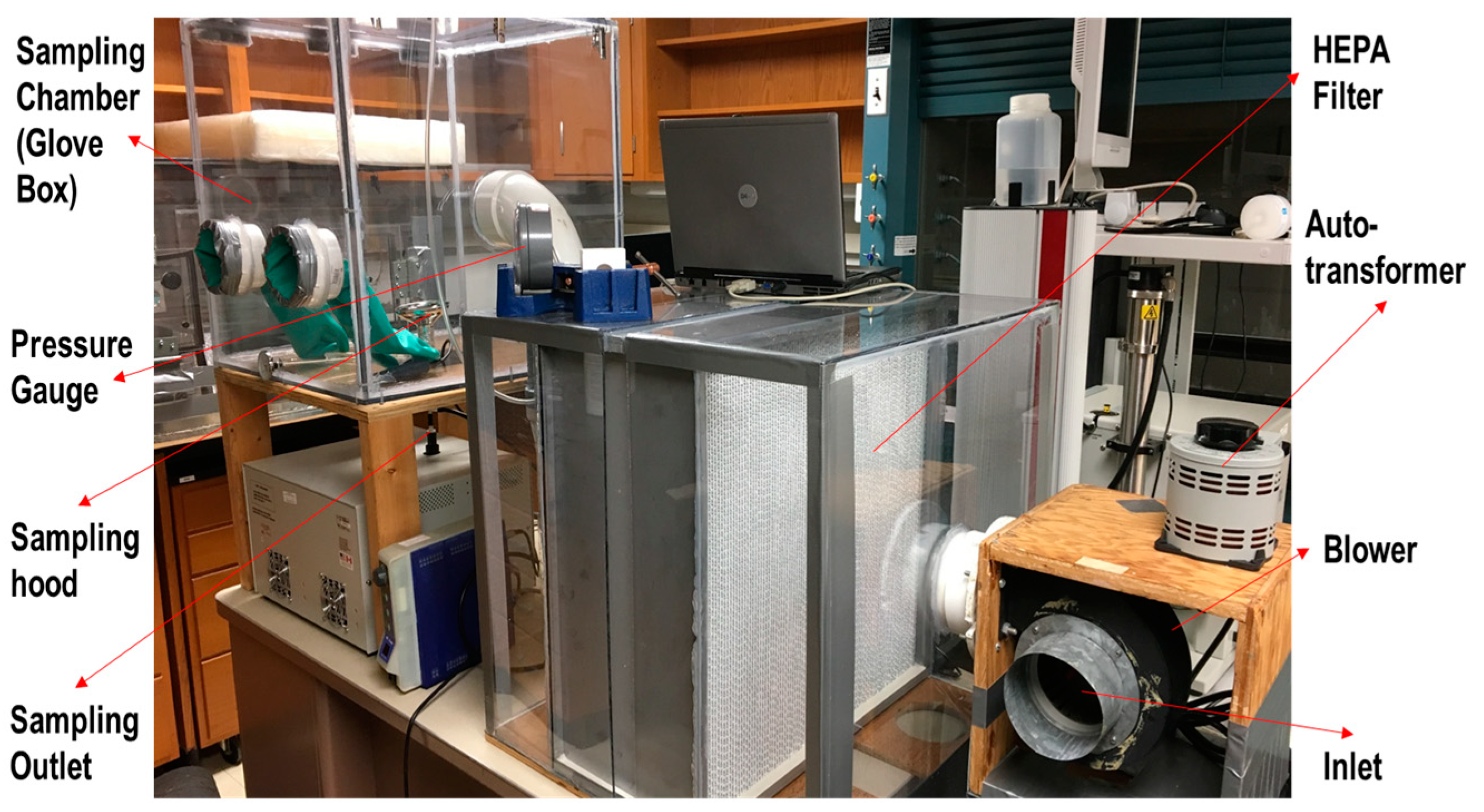
2.1. Experimental System
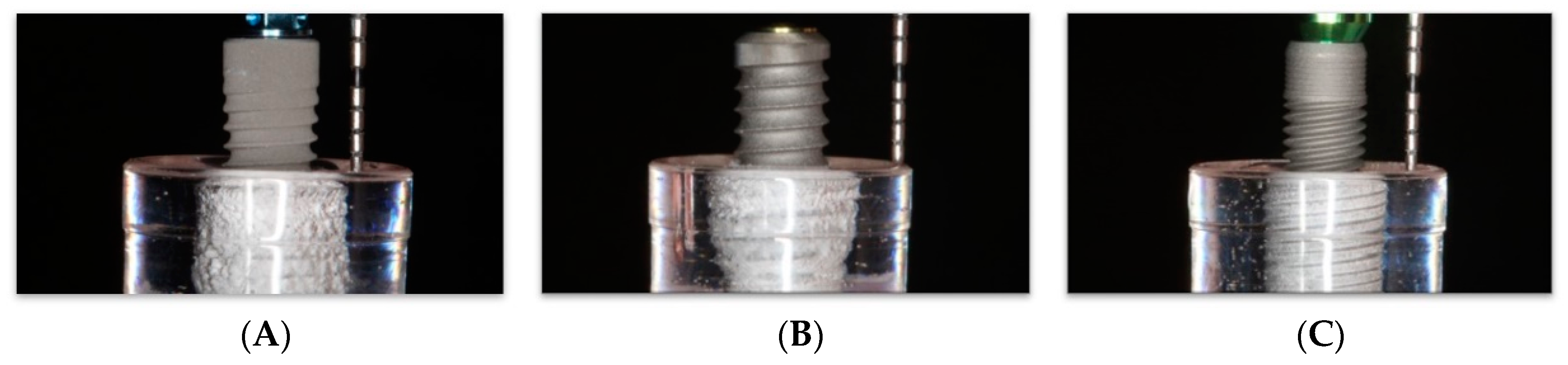
2.2. Implants
- Group A (Straumann® BLT, RC, SLA; 4.1 Ø mm, length 16 mm; Institut Straumann AG, Basel, Switzerland);
- Group B (BioHorizons® Tapered Plus; 4.6 mm × 15 mm; BioHorizons Plus, Birmingham, AL, USA).
- Group C (Zimmer® Tapered Screw-Vent MTX; 4.1 mm × 16 mm; Zimmer Dental Inc., Carlsbad, CA, USA).
2.3. Intra-Operator Calibration
2.4. Implantoplasty Procedures
2.5. Particle Collection and Analysis
2.6. Mechanical Properties
2.7. Statistical Analysis
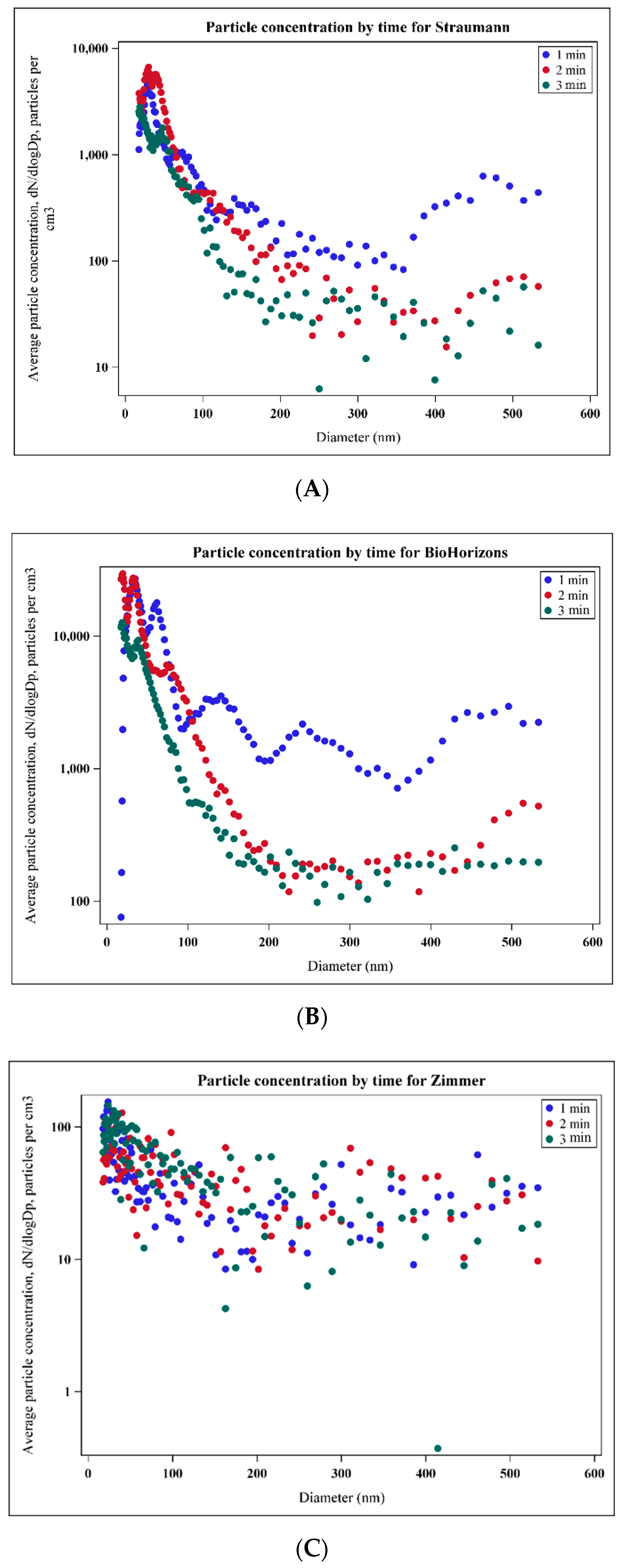
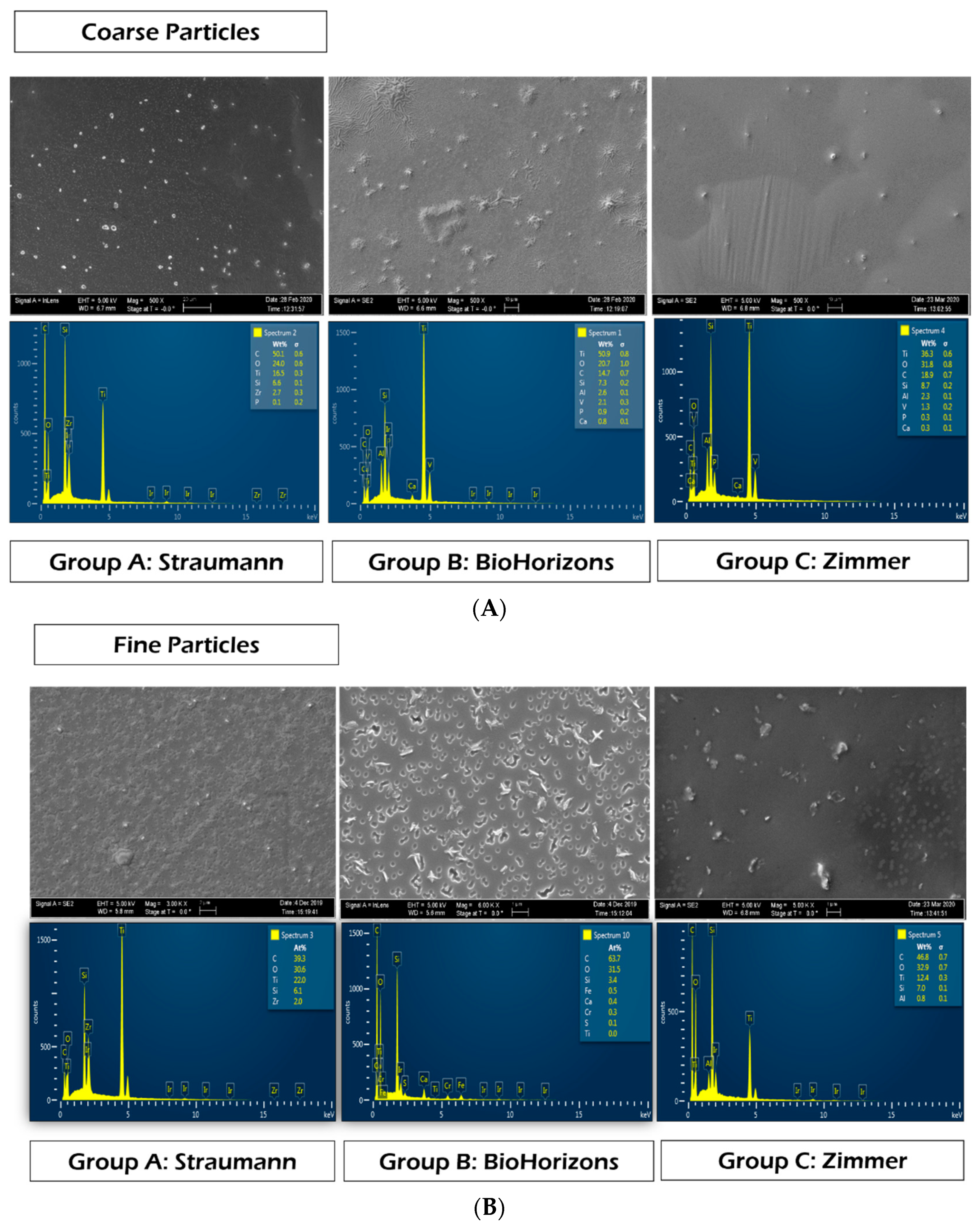
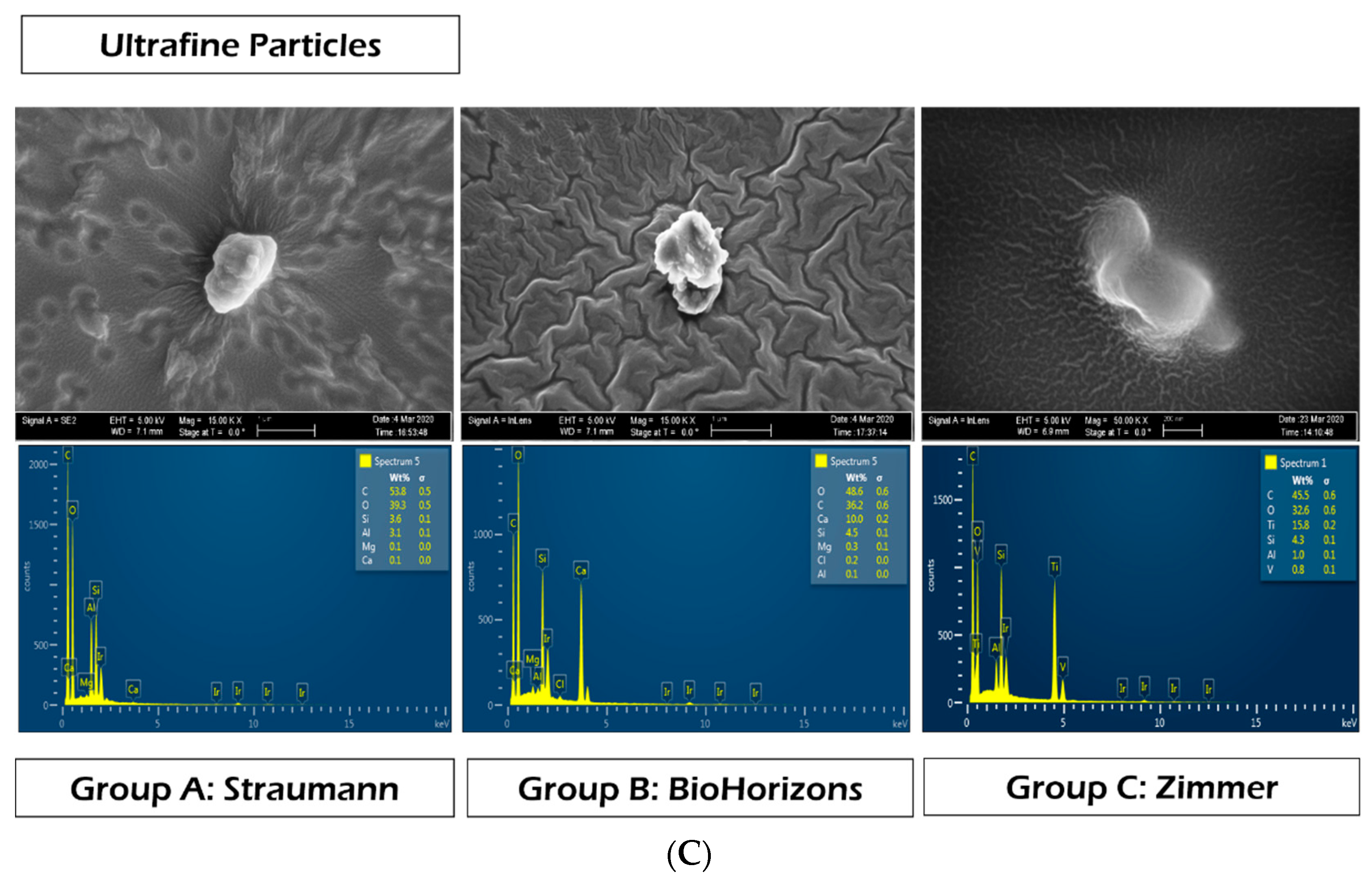
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Liu, X.; Chen, S.; Tsoi, J.K.H.; Matinlinna, J.P. Binary titanium alloys as dental implant materials-a review. Regen. Biomater. 2017, 4, 315–323. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leonhardt, A.; Bergström, C.; Lekholm, U. Microbiologic diagnostics at titanium implants. Clin. Implant. Dent. Relat. Res. 2003, 5, 226–232. [Google Scholar] [CrossRef]
- Lalor, P.A.; Revell, P.A.; Gray, A.B.; Wright, S.; Railton, G.T.; Freeman, M.A. Sensitivity to titanium. A cause of implant failure? J. Bone Jt. Surg. Br. 1991, 73, 25–28. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, J.J.; Skipor, A.K.; Patterson, L.M.; Hallab, N.J.; Paprosky, W.G.; Black, J.; Galante, J.O. Metal release in patients who have had a primary total hip arthroplasty. A prospective, controlled, longitudinal study. J. Bone Jt. Surg. Am. 1998, 80, 1447–1458. [Google Scholar] [CrossRef]
- Woodman, J.L.; Jacobs, J.J.; Galante, J.O.; Urban, R.M. Metal ion release from titanium-based prosthetic segmental replacements of long bones in baboons: A long-term study. J. Orthop. Res. Off. Publ. Orthop. Res. Soc. 1984, 1, 421–430. [Google Scholar] [CrossRef]
- Franchi, M.; Bacchelli, B.; Martini, D.; de Pasquale, V.; Orsini, E.; Ottani, V.; Fini, M.; Giavaresi, G.; Giardino, R.; Ruggeri, A. Early detachment of titanium particles from various different surfaces of endosseous dental implants. Biomaterials 2004, 25, 2239–2246. [Google Scholar] [CrossRef] [PubMed]
- Schliephake, H.; Reiss, G.; Urban, R.; Neukam, F.W.; Guckel, S. Metal release from titanium fixtures during placement in the mandible: An experimental study. Int. J. Oral Maxillofac. Implant. 1993, 8, 502–511. [Google Scholar]
- Senna, P.; Antoninha Del Bel Cury, A.; Kates, S.; Meirelles, L. Surface Damage on Dental Implants with Release of Loose Particles after Insertion into Bone. Clin. Implant. Dent. Relat. Res. 2015, 17, 681–692. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berglundh, T.; Armitage, G.; Araujo, M.G.; Avila-Ortiz, G.; Blanco, J.; Camargo, P.M.; Chen, S.; Cochran, D.; Derks, J.; Figuero, E.; et al. Peri-implant diseases and conditions: Consensus report of workgroup 4 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Periodontol. 2018, 89 (Suppl. S1), S313–S318. [Google Scholar] [CrossRef]
- Derks, J.; Håkansson, J.; Wennström, J.L.; Tomasi, C.; Larsson, M.; Berglundh, T. Effectiveness of implant therapy analyzed in a Swedish population: Early and late implant loss. J. Dent. Res. 2015, 94 (Suppl. S3), 44S–51S. [Google Scholar] [CrossRef] [Green Version]
- Monje, A.; Galindo-Moreno, P.; Tözüm, T.F.; Suárez-López del Amo, F.; Wang, H.-L. Into the Paradigm of Local Factors as Contributors for Peri-implant Disease: Short Communication. Int. J. Oral Maxillofac. Implants. 2016, 31, 288–292. [Google Scholar] [CrossRef]
- Wilson, T.G., Jr.; Valderrama, P.; Burbano, M.; Blansett, J.; Levine, R.; Kessler, H.; Rodrigues, D.C. Foreign Bodies Associated With Peri-Implantitis Human Biopsies. J. Periodontol. 2015, 86, 9–15. [Google Scholar] [CrossRef]
- Safioti, L.M.; Kotsakis, G.A.; Pozhitkov, A.E.; Chung, W.O.; Daubert, D.M. Increased Levels of Dissolved Titanium Are Associated With Peri-Implantitis—A Cross-Sectional Study. J. Periodontol. 2017, 88, 436–442. [Google Scholar] [CrossRef]
- Flatebø, R.S.; Johannessen, A.C.; Grønningsæter, A.G.; Bøe, O.E.; Gjerdet, N.R.; Grung, B.; Leknes, K.N. Host Response to Titanium Dental Implant Placement Evaluated in a Human Oral Model. J. Periodontol. 2006, 77, 1201–1210. [Google Scholar] [CrossRef]
- Ingham, E.; Fisher, J. The role of macrophages in osteolysis of total joint replacement. Biomaterials 2005, 26, 1271–1286. [Google Scholar] [CrossRef] [PubMed]
- del Amo, F.S.; Rudek, I.; Wagner, V.P.; Martins, M.D.; O’Valle, F.; Galindo-Moreno, P.; Giannobile, W.V.; Wang, H.; Castilho, R.M. Titanium Activates the DNA Damage Response Pathway in Oral Epithelial Cells: A Pilot Study. Int. J. Oral Maxillofac. Implant. 2017, 32, 1413–1420. [Google Scholar] [CrossRef] [Green Version]
- Fretwurst, T.; Buzanich, G.; Nahles, S.; Woelber, J.P.; Riesemeier, H.; Nelson, K. Metal elements in tissue with dental peri-implantitis: A pilot study. Clin. Oral Implant. Res. 2016, 27, 1178–1186. [Google Scholar] [CrossRef] [PubMed]
- Magone, K.; Luckenbill, D.; Goswami, T. Metal ions as inflammatory initiators of osteolysis. Arch. Orthop. Trauma Surg. 2015, 135, 683–695. [Google Scholar] [CrossRef] [PubMed]
- Shanbhag, A.S.; Jacobs, J.J.; Glant, T.T.; Gilbert, J.L.; Black, J.; Galante, J.O. Composition and morphology of wear debris in failed uncemented total hip replacement. J. Bone Jt. Surg. Br. 1994, 76, 60–67. [Google Scholar] [CrossRef]
- Archibeck, M.J.; Jacobs, J.J.; Roebuck, K.A.; Glant, T.T. The basic science of periprosthetic osteolysis. Instr. Course. Lect. 2001, 50, 185–195. [Google Scholar] [CrossRef]
- Olmedo, D.G.; Paparella, M.L.; Spielberg, M.; Brandizzi, D.; Guglielmotti, M.B.; Cabrini, R.L. Oral mucosa tissue response to titanium cover screws. J. Periodontol. 2012, 83, 973–980. [Google Scholar] [CrossRef]
- Purdue, P.E.; Koulouvaris, P.; Nestor, B.J.; Sculco, T.P. The central role of wear debris in periprosthetic osteolysis. HSS J. Hosp. Spec. Surg. 2006, 2, 102–113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wimhurst, J.A.; Brooks, R.A.; Rushton, N. Inflammatory responses of human primary macrophages to particulate bone cements in vitro. J. Bone Jt. Surg. Br. 2001, 83, 278–282. [Google Scholar] [CrossRef]
- Catelas, I.; Huk, O.L.; Petit, A.; Zukor, D.J.; Marchand, R.; Yahia, L. Flow cytometric analysis of macrophage response to ceramic and polyethylene particles: Effects of size, concentration, and composition. J. Biomed. Mater. Res. 1998, 41, 600–607. [Google Scholar] [CrossRef]
- Anitua, E.A. Enhancement of osseointegration by generating a dynamic implant surface. J. Oral Implantol. 2006, 32, 72–76. [Google Scholar] [CrossRef]
- De Maeztu, M.A.; Alava, J.I.; Gay-Escoda, C. Ion implantation: Surface treatment for improving the bone integration of titanium and Ti6Al4V dental implants. Clin. Oral Implant. Res. 2003, 14, 57–62. [Google Scholar] [CrossRef]
- Berglundh, T.; Gotfredsen, K.; Zitzmann, N.U.; Lang, N.P.; Lindhe, J. Spontaneous progression of ligature induced peri-implantitis at implants with different surface roughness: An experimental study in dogs. Clin. Oral Implant. Res. 2007, 18, 655–661. [Google Scholar] [CrossRef]
- Ramel, C.F.; Lüssi, A.; Özcan, M.; Jung, R.E.; Hämmerle, C.H.F.; Thoma, D.S. Surface roughness of dental implants and treatment time using six different implantoplasty procedures. Clin. Oral Implant. Res. 2016, 27, 776–781. [Google Scholar] [CrossRef] [PubMed]
- Ravidà, A.; Siqueira, R.; Saleh, I.; Saleh, M.H.A.; Giannobile, A.; Wang, H.L. Lack of Clinical Benefit of Implantoplasty to Improve Implant Survival Rate. J. Dent. Res. 2020, 99, 1348–1355. [Google Scholar] [CrossRef]
- Olmedo, D.G.; Nalli, G.; Verdú, S.; Paparella, M.L.; Cabrini, R.L. Exfoliative Cytology and Titanium Dental Implants: A Pilot Study. J. Periodontol. 2013, 84, 78–83. [Google Scholar] [CrossRef]
- Jayne, J.T.; Leard, D.C.; Zhang, X.; Davidovits, P.; Smith, K.A.; Kolb, C.E.; Worsnop, D.R. Development of an Aerosol Mass Spectrometer for Size and Composition Analysis of Submicron Particles. Aerosol. Sci. Technol. 2000, 33, 49–70. [Google Scholar] [CrossRef] [Green Version]
- Manero, J.M.; Gil, F.J.; Padrós, E.; Planell, J.A. Applications of Environmental Scanning Electron Microscopy (ESEM) in Biomaterials Field. Microsc. Res. Tech. 2003, 61, 469–480. [Google Scholar] [CrossRef]
- Gil, F.J.; Rodriguez, D.; Aparicio, C. Variation of roughness and adhesion strength of deposited apatite layers on titanium dental implants. Mater. Sci. Eng. C 2011, 31, 320–324. [Google Scholar] [CrossRef]
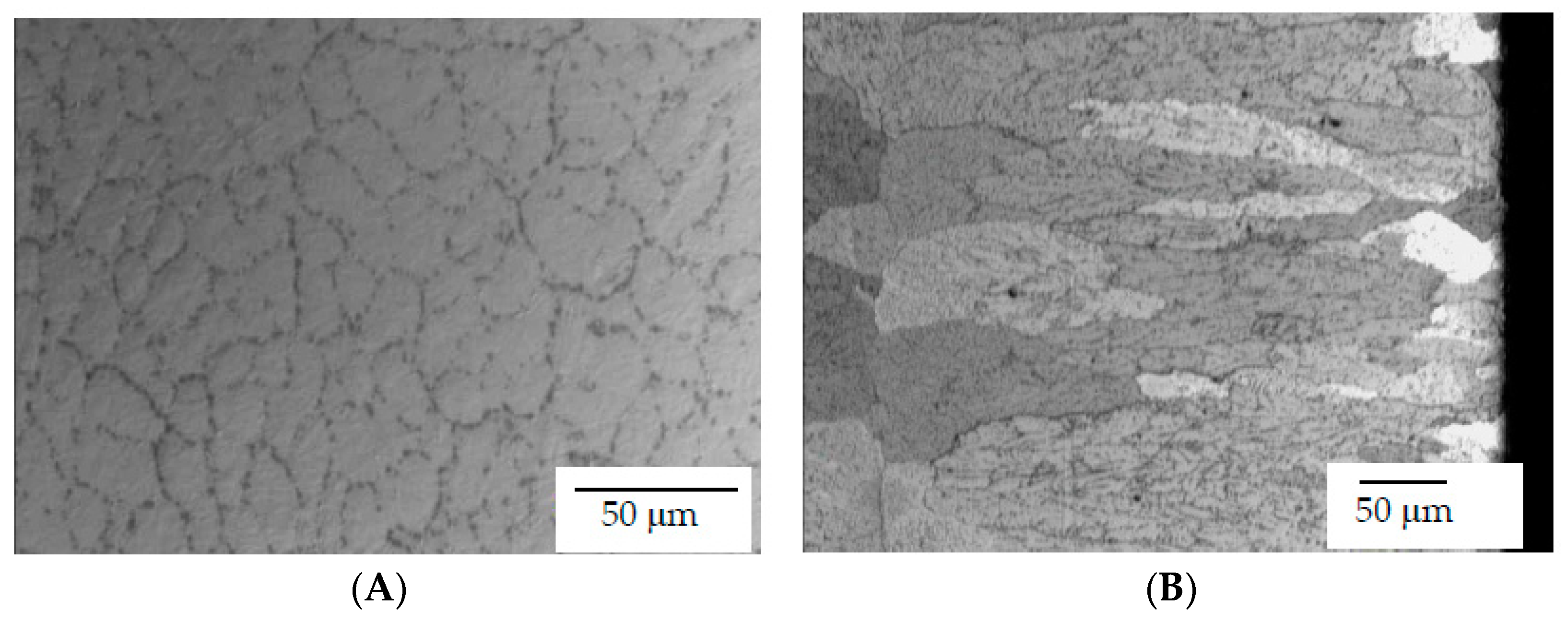
- Gil, F.J.; Rodríguez, D.; Planell, J.A. Grain growth kinetics of pure titanium. Scr. Met. Mater. 1995, 33, 1361–1366. [Google Scholar] [CrossRef]
- Gil, F.J.; Manero, J.M.; Ginebra, M.P.; Planell, J.A. The effect of cooling rate on the cyclic deformation of β-annealed Ti-6Al-4V. Mater. Sci. Eng. A 2003, 349, 150–155. [Google Scholar] [CrossRef]
- Gil, F.J.; Planell, J.A. Behaviour of normal grain growth kinetics in single phase titanium and titanium alloys. Mater. Sci. Eng. A 2000, 283, 17–24. [Google Scholar] [CrossRef]
- Ingram, J.H.; Stone, M.; Fisher, J.; Ingham, E. The influence of molecular weight, crosslinking and counterface roughness on TNF-alpha production by macrophages in response to ultra high molecular weight polyethylene particles. Biomaterials 2004, 25, 3511–3522. [Google Scholar] [CrossRef]
- Al-Saffar, N.; Khwaja, H.A.; Kadoya, Y.; Revell, P.A. Assessment of the Role of GM-CSF in the Cellular Transformation and the Development of Erosive Lesions around Orthopaedic Implants. Am. J. Clin. Pathol. 1996, 105, 628–639. [Google Scholar] [CrossRef] [Green Version]
- Sabokbar, A.; Rushton, N. Role of inflammatory mediators and adhesion molecules in the pathogenesis of aseptic loosening in total hip arthroplasties. J. Arthroplast. 1995, 10, 810–816. [Google Scholar] [CrossRef]
- Harrison, R.M.; Yin, J. Particulate matter in the atmosphere: Which particle properties are important for its effects on health? Sci. Total Environ. 2000, 249, 85–101. [Google Scholar] [CrossRef]
- Toledano-Serrabona, J.; Gil, F.J.; Camps-Font, O.; Valmaseda-Castellon, E.; Gay-Escoda, C.; Sánchez-Garcés, M.A. Physicochemical and Biological Characterization of Ti6Al4V particles obtained by Implantoplasty: An In vivo study. Materials 2021, 14, 6507. [Google Scholar] [CrossRef] [PubMed]
- Toledano-Serrabona, J.; Sánchez-Garcés, M.A.; Gay-Escoda, C.; Valmaseda-Castellon, E.; Camps-Font, O.; Verdeguer, P.; Molmeneu, M.; Gil, F.J. Mechanical properties and corrosión behavior of Ti6Al4V particles obtained by Implatoplasty. An in vivo study. Materials 2021, 14, 6519. [Google Scholar] [CrossRef] [PubMed]
- Gherlone, E.F.; Capparé, P.; Tecco, S.; Polizzi, E.; Pantaleo, G.; Gastaldi, G.; Grusovin, M.G. Implant Prosthetic Rehabilitation in Controlled HIV-Positive Patients: A Prospective Longitudinal Study with 1-Year Follow-Up. Clin. Implant. Dent. Relat. Res. 2016, 18, 725–734. [Google Scholar] [CrossRef] [PubMed]
- Rosso, M.; Blasi, G.; Gherlone, E.; Rosso, R. Effect of granulocyte-macrophage colony-stimulating factor on prevention of mucositis in head and neck cancer patients treated with chemo-radiotherapy. J. Chemother. 1997, 9, 382–385. [Google Scholar] [CrossRef] [PubMed]
- Ciancaglini, R.; Gherlone, E.F.; Redaelli, S.; Radaelli, G. The distribution of occlusal contacts in the intercuspal position and temporomandibular disorder. J. Oral Rehabil. 2002, 29, 1082–1090. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Manufacturer | Material | Current Generation | Technique | Chemical Treatment | Nanoscale |
|---|---|---|---|---|---|
| Straumann, Switzerland | Ti-15Zr | SLA | Blasting and acid-etched | N | N |
| Zimmer, Warsaw, IN, USA | Ti-6Al-4V | MTX | Blasting | N | N |
| BioHorizons, Birmingham, AL, USA | Ti-6Al-4V | Laser-Lok | Blasting | N | N |
| Comparisons | Pairwise Comparisons b | ||||
|---|---|---|---|---|---|
| Particle Size | p-Value a | Straumann vs. BioHorizons | Straumann vs. Zimmer | BioHorizons vs. Zimmer | |
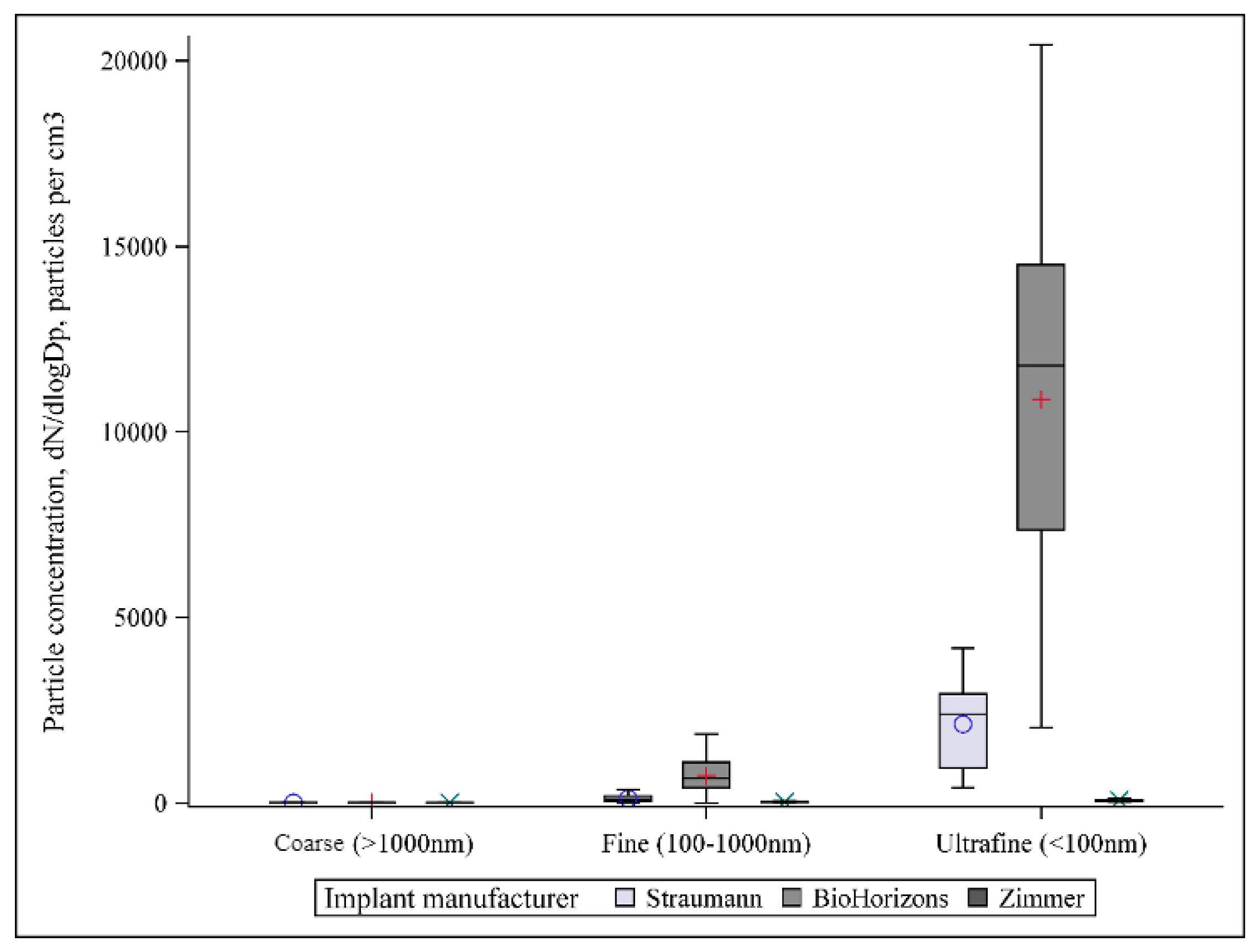
| Particle number size | Coarse (>1000 nm) | 0.7169 | <0.0001 | - | - |
| Fine (100–1000 nm) | <0.0001 | <0.0001 | <0.0001 | <0.0001 | |
| Ultrafine (<100 nm) | <0.0001 | <0.0001 | <0.0001 | <0.0001 | |
| Particle mass | Coarse (>1000 nm) | 0.0488 | <0.0001 | - | - |
| Fine (100–1000 nm) | <0.0001 | <0.0001 | <0.0001 | <0.0001 | |
| Ultrafine (<100 nm) | <0.0001 | <0.0001 | <0.0001 | <0.0001 | |
| Particle surface area | Coarse (>1000 nm) | 0.0009 | 0.0232 | 0.0050 | 0.0547 |
| Fine (100–1000 nm) | <0.0001 | <0.0001 | <0.0001 | <0.0001 | |
| Ultrafine (<100 nm) | <0.0001 | <0.0001 | <0.0001 | <0.0001 | |
| Implant System | Implant | Maximum Strength (MPa) | Yield Stress 0.2% (MPa) | Ductility (%) | Hardness (GPa) |
|---|---|---|---|---|---|
| Straumann | Ti15Zr | 897 (24) | 698 (20) | 22 (4) | 1.952 (137) |
| BioHorizons | Ti6Al4V * | 860 (37) | 657 (23) | 17 (4) | 1.118 (198) |
| Zimmer | Ti6Al4V | 1050 (35) | 740 (23) | 8 (2) | 1.451 (233) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, X.; Cai, C.; Gil, J.; Jantz, E.; Al Sakka, Y.; Padial-Molina, M.; Suárez-López del Amo, F. Characteristics of Particles and Debris Released after Implantoplasty: A Comparative Study. Materials 2022, 15, 602. https://doi.org/10.3390/ma15020602
Wu X, Cai C, Gil J, Jantz E, Al Sakka Y, Padial-Molina M, Suárez-López del Amo F. Characteristics of Particles and Debris Released after Implantoplasty: A Comparative Study. Materials. 2022; 15(2):602. https://doi.org/10.3390/ma15020602
Chicago/Turabian StyleWu, Xixi, Changjie Cai, Javier Gil, Elizabeth Jantz, Yacoub Al Sakka, Miguel Padial-Molina, and Fernando Suárez-López del Amo. 2022. "Characteristics of Particles and Debris Released after Implantoplasty: A Comparative Study" Materials 15, no. 2: 602. https://doi.org/10.3390/ma15020602
APA StyleWu, X., Cai, C., Gil, J., Jantz, E., Al Sakka, Y., Padial-Molina, M., & Suárez-López del Amo, F. (2022). Characteristics of Particles and Debris Released after Implantoplasty: A Comparative Study. Materials, 15(2), 602. https://doi.org/10.3390/ma15020602