
Biomechanical Behavior Evaluation of Resin Cement with Different Elastic Modulus on Porcelain Laminate Veneer Restorations Using Micro-CT-Based Finite Element Analysis

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. 3D Solid Model Generation
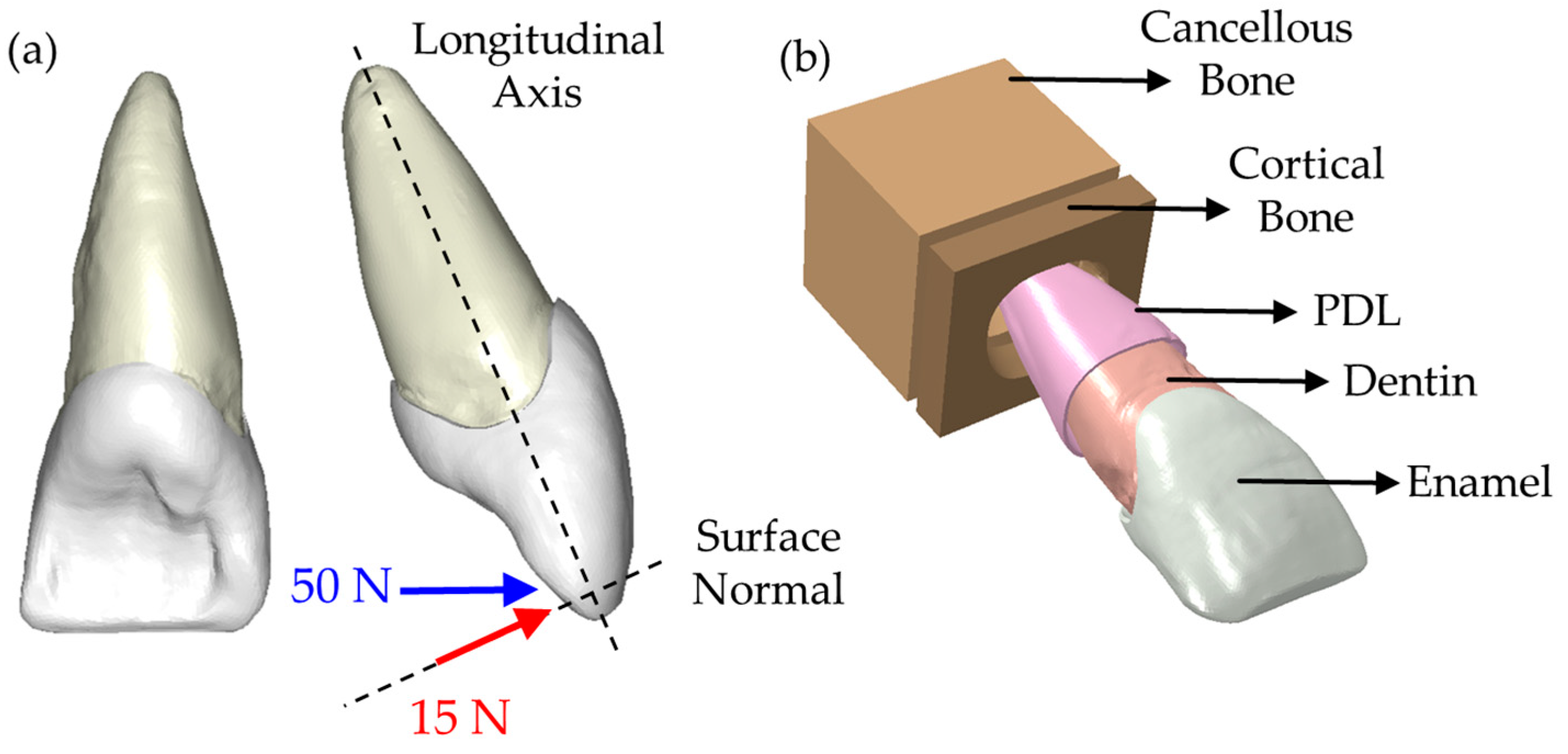
2.2. 3D FE Modeling
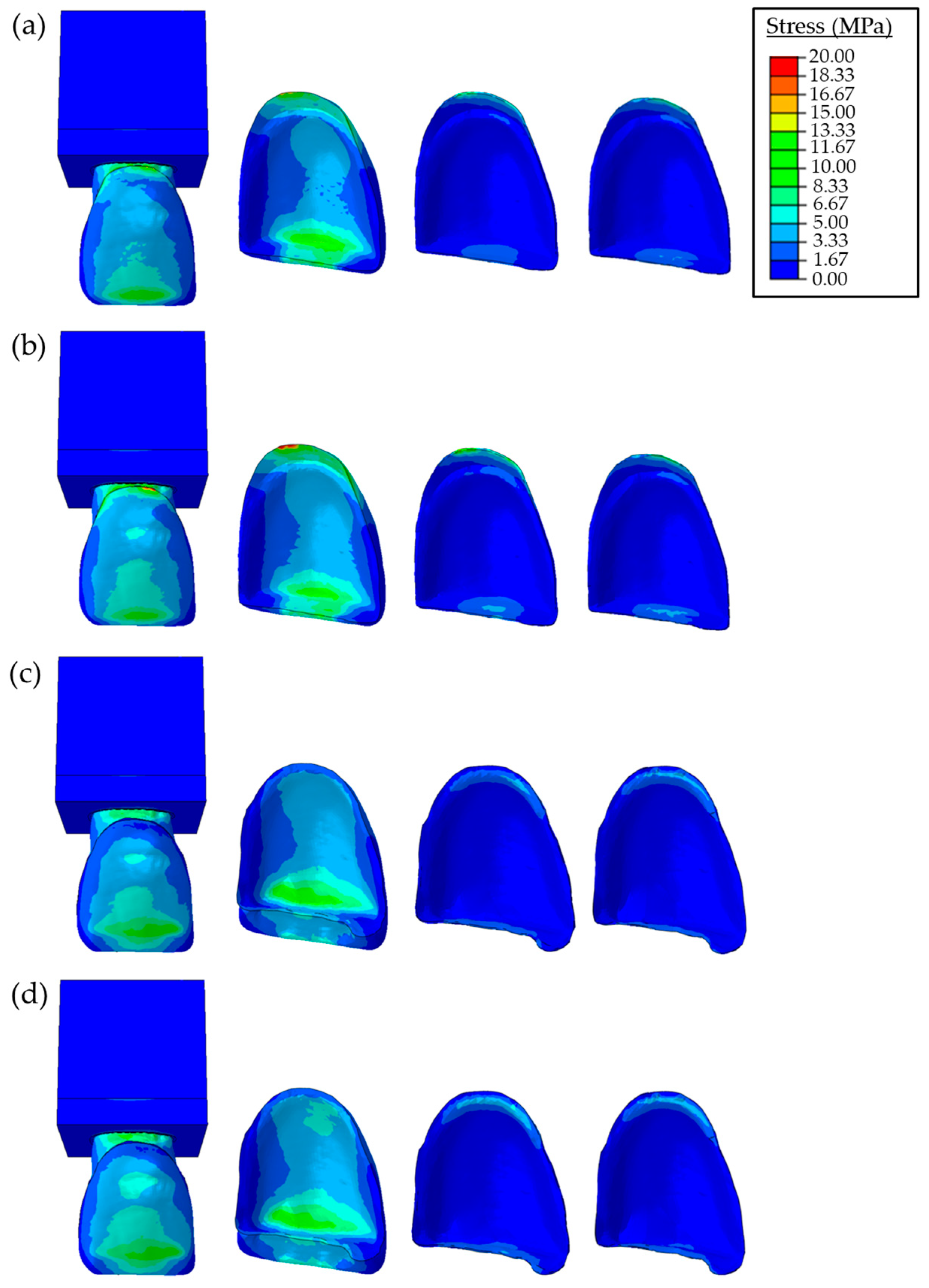
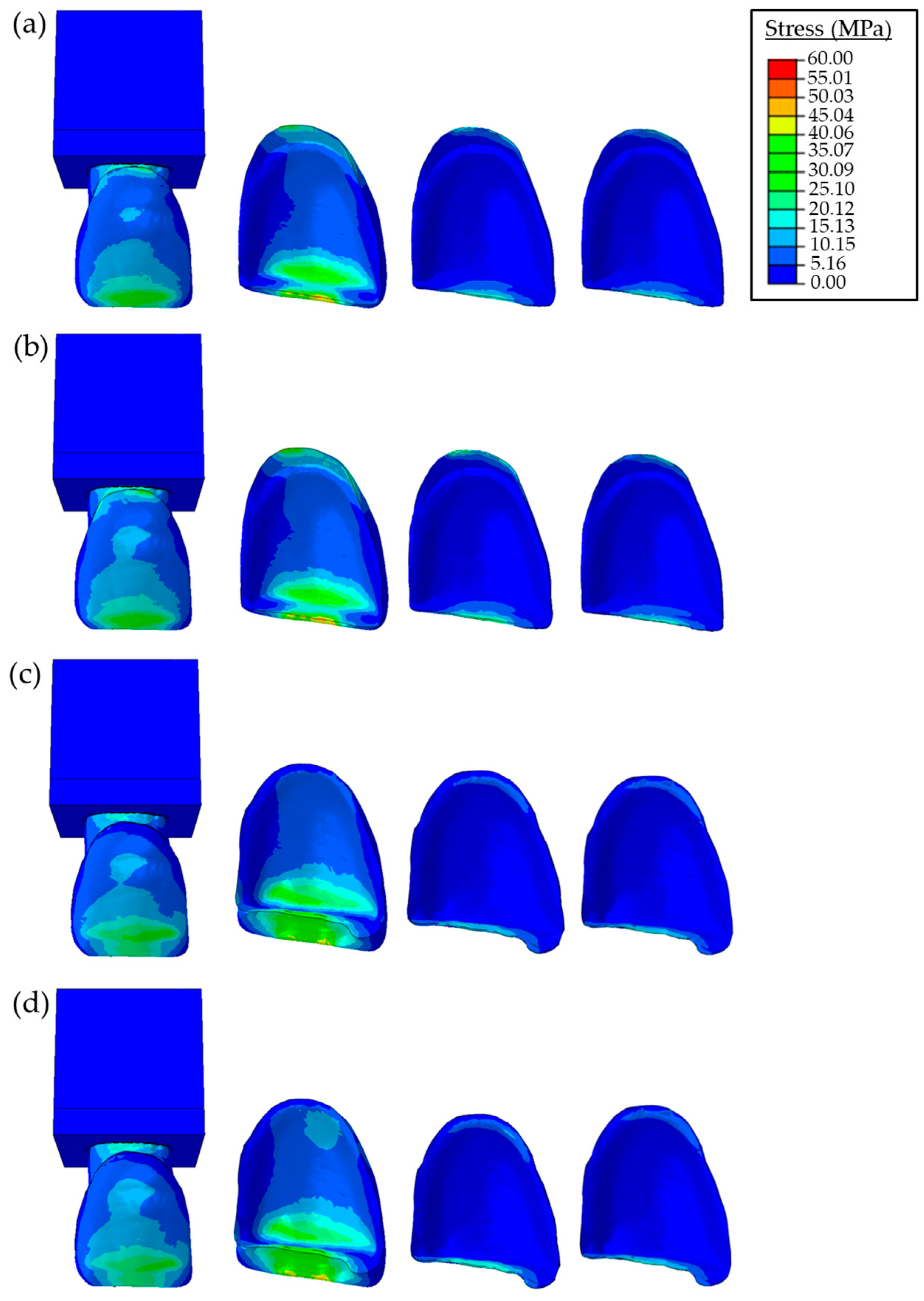
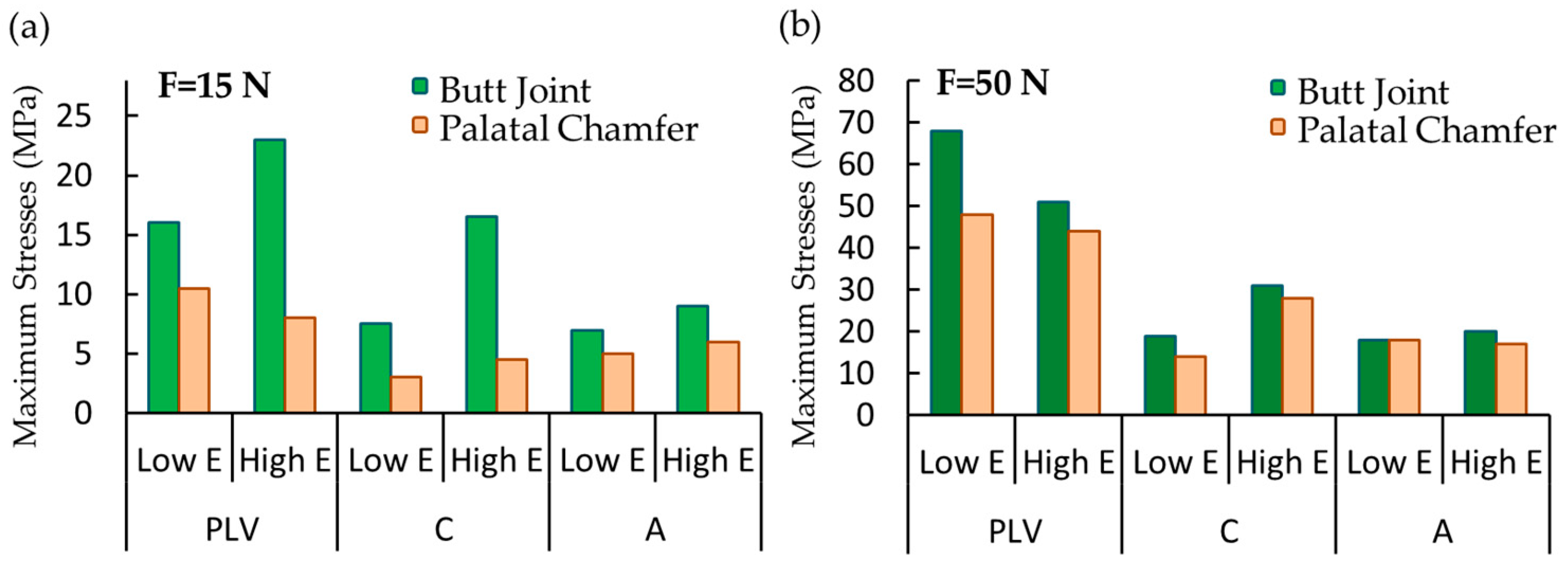
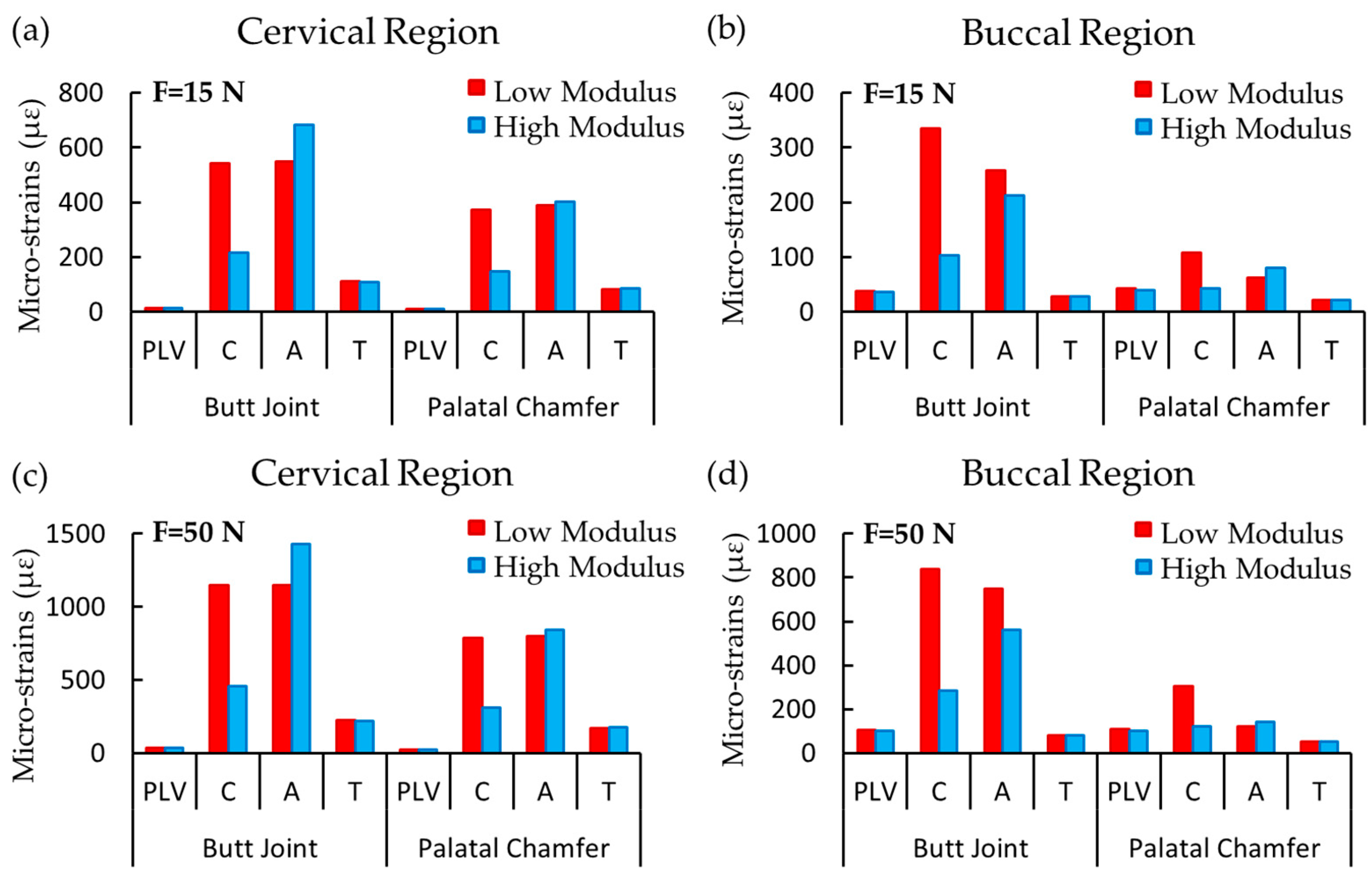
3. Results
4. Discussion
5. Conclusions
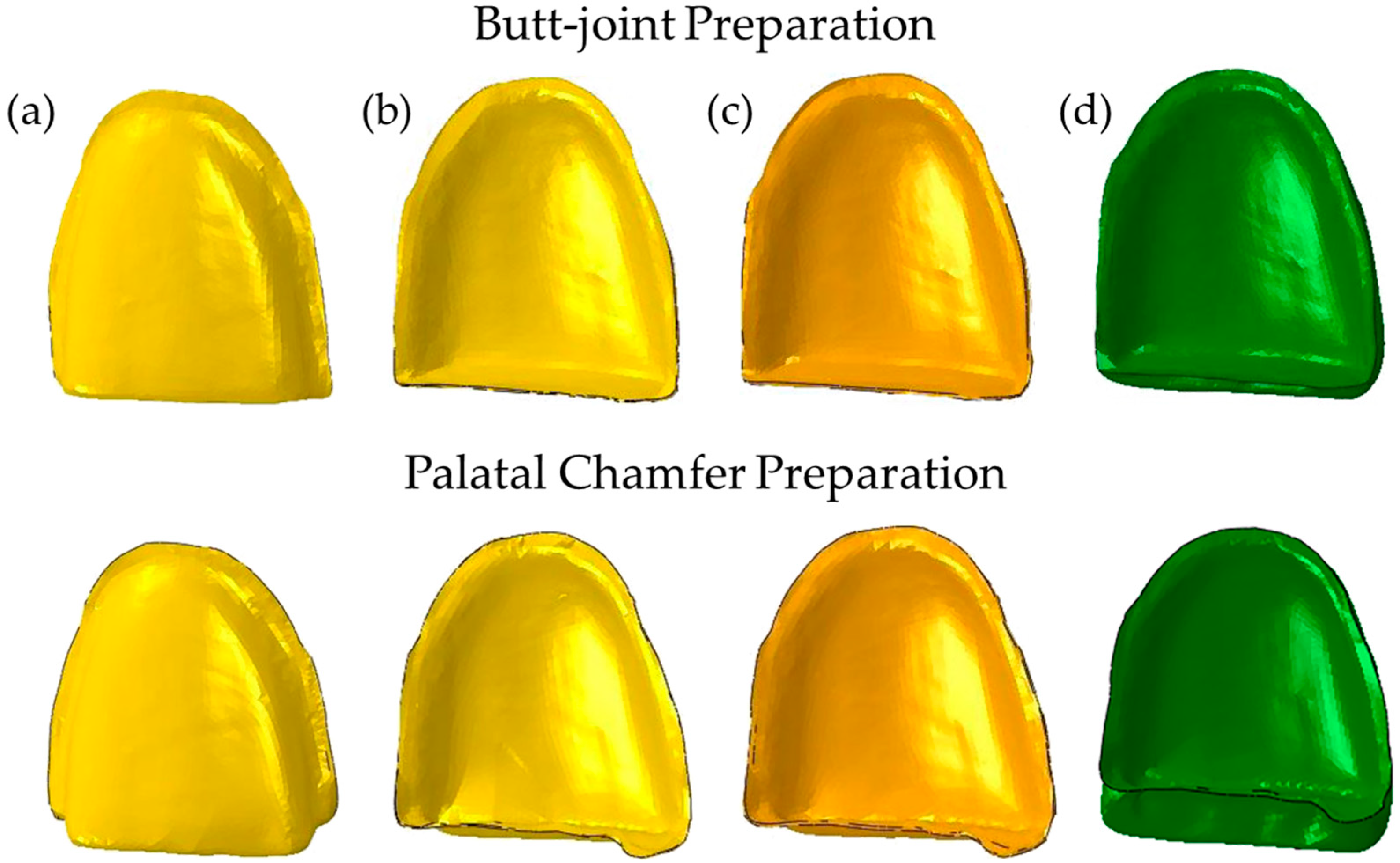
- PLV restorations with the palatal chamfer involving the incisal margin design results in biomechanical responses closer to that of a sound tooth compared to restorations using butt joints.
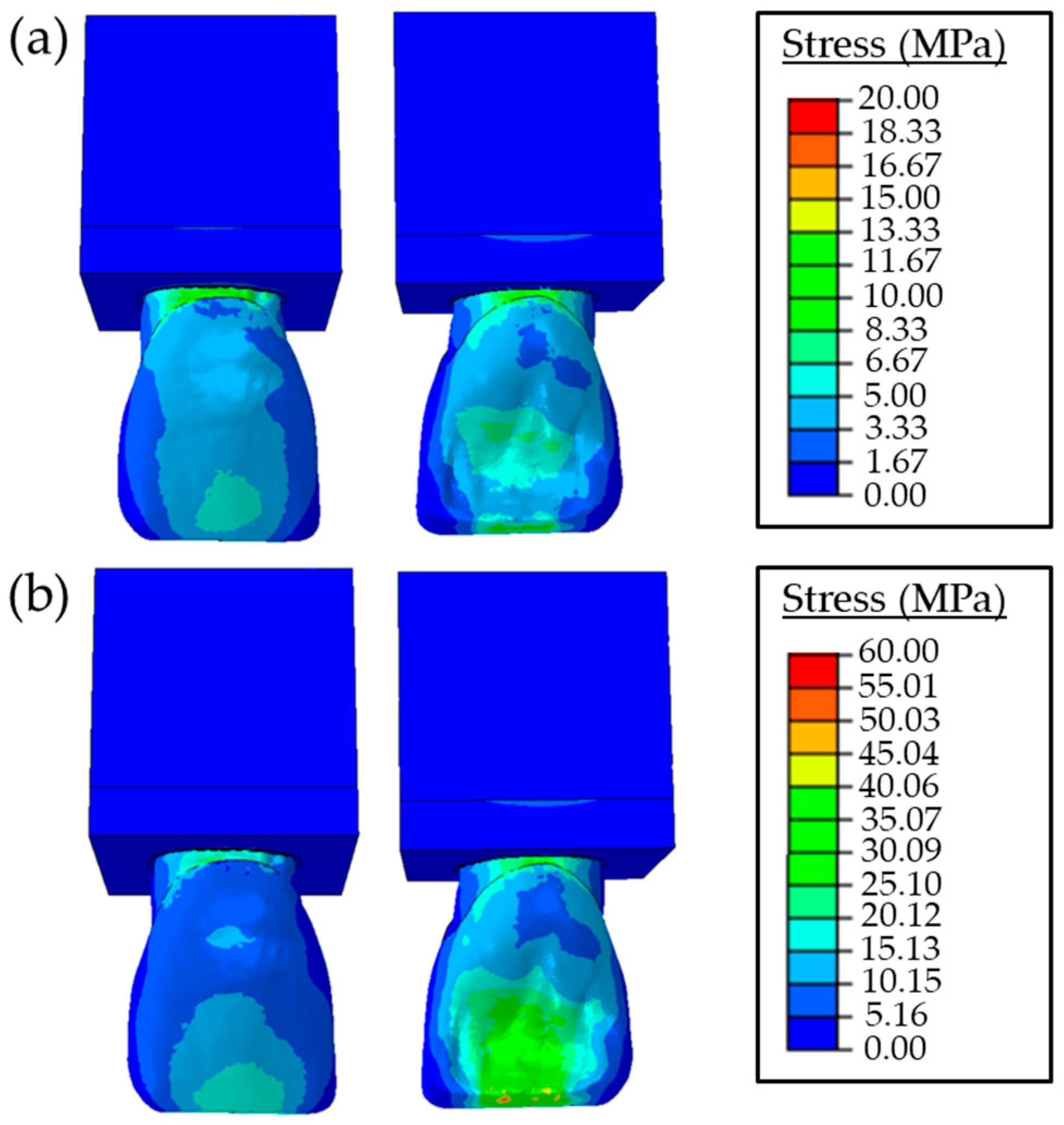
- Regardless of the magnitude and angle of the load and the elasticity modulus of the resin cement, the PLV restorations with butt joint preparation showed higher stress distributions compared to those with palatal chamfer preparation.
- An increase in the elasticity modulus of the resin cement induced slightly larger stresses on the adhesive layer, tooth tissues, and restorative materials.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Peumans, M.; Van Meerbeek, B.; Lambrechts, P.; Vanherle, G. Porcelain veneers: A review of the literature. J. Dent. 2000, 28, 163–177. [Google Scholar]
- Peumans, M.; De Munck, J.; Fieuws, S.; Lambrechts, P.; Vanherle, G.; Van Meerbeek, B. A Prospective Ten-year Clinical Trial of Porcelain Veneers. J. Adhes. Dent. 2004, 6, 65–76. [Google Scholar]
- Beier, U.S.; Kapferer, I.; Burtscher, D.; Dumfahrt, H. Clinical Performance of Porcelain Laminate Veneers for Up to 20 Years. Int. J. Prosthodont. 2012, 25, 79–86. [Google Scholar]
- Layton, D.M.; Walton, T.R. The Up to 21-Year Clinical Outcome and Survival of Feldspathic Porcelain Veneers: Accounting for Clustering. Int. J. Prosthodont. 2012, 25, 604–612. [Google Scholar] [PubMed]
- Zarone, F.; Sorrentino, R.; Apicella, D.; Valentino, B.; Ferrari, M.; Aversa, R.; Apicella, A. Evaluation of the biomechanical behavior of maxillary central incisors restored by means of endocrowns compared to a natural tooth: A 3D static linear finite elements analysis. Dent. Mater. 2006, 2, 1035–1044. [Google Scholar] [CrossRef] [PubMed]
- Shahrbaf, S.; Van Noort, R.; Mirzakouchaki, B.; Ghassemieh, E.; Martina, N. Fracture strength of machined ceramic crowns as a function of tooth preparation design and the elastic modulus of the cement. Dent. Mater. 2014, 30, 234–241. [Google Scholar] [CrossRef]
- Penteado, M.M.; Tribst, J.P.M.; Dal Piva, A.M.D.O.; Archangelo, K.C.; Bottino, M.A.; Borges, A.L.S. Influence of different restorative material and cement on the stress distribution of ceramic veneer in upper central incisor. Indian J. Dent. Res. 2020, 31, 236–240. [Google Scholar] [PubMed]
- Sokolowski, G.; Szczesio, A.; Bociong, K.; Kaluzinska, K.; Lapinska, B.; Sokolowski, J.; Domarecka, M.; Lukomska-Szymanska, M. Dental resin cements-The influence of water sorption on contraction stress changes and hydroscopic expansion. Materials 2018, 11, 973. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, H.; Lin, C.; Sun, M.; Chang, Y. Numerical investigation of macro- and micro-mechanics of a ceramic veneer bonded with various cement thicknesses using the typical and submodeling finite element approaches. J. Dent. 2009, 37, 141–148. [Google Scholar] [CrossRef] [PubMed]
- Addisson, O.; Marquis, P.; Fleming, G. Resin Elasticity and the Strengthening of All-ceramic Restorations. J. Dent. Res. 2007, 86, 519–523. [Google Scholar] [CrossRef] [Green Version]
- Tian, T.; Tsoi, J.K.H.; Matinlinna, J.P.; Burrow, M.F. Aspects of bonding between resin luting cements and glass ceramic materials. Dent. Mater. 2014, 30, e147–e162. [Google Scholar] [CrossRef] [PubMed]
- Spazzin, A.O.; Guarda, G.; Oliveira-Ogliari, A.; Correr-Sobrinho, F.L.L.; Moraes, R. Strengthening of Porcelain Provided by Resin Cements and Flowable Composites. Oper. Dent. 2016, 41, 179–188. [Google Scholar] [CrossRef] [Green Version]
- Spazzin, A.O.; Bacchi, A.; Alessandretti, R.; Santos, M.B.; Basso, G.R.; Griggs, J.; Moraes, R.R. Ceramic strengthening by tuning the elastic moduli of resin-based luting agents. Dent. Mater. 2017, 33, 358–366. [Google Scholar] [CrossRef]
- Barbon, F.J.; Moraes, R.R.; Isolan, C.P.; Spazzin, A.O.; Boscato, N. Influence of inorganic filler content of resin luting agents and use of adhesive on the performance of bonded ceramic. J. Prosthet. Dent. 2019, 122, 566.e1–566.e11. [Google Scholar]
- Magne, P.; Kwon, K.; Belser, U.C.; Hodges, J.S.; Douglas, W.H. Crack propensity of porcelain laminate veneers: A simulated operatory. J. Prosthet. Dent. 1999, 81, 327–334. [Google Scholar] [CrossRef] [PubMed]
- Ausiello, P.; Apicella, A.; Davidson, C.; Rengo, S. 3D-finite element analyses of cusp movements in a human upper premolar, restored with adhesive resin-based composites. J. Biomech. 2001, 34, 1269–1277. [Google Scholar] [CrossRef]
- Magne, P. Efficient 3D finite element analysis of dental restorative procedures using micro-CT data. Dent. Mater. 2007, 23, 539–548. [Google Scholar] [CrossRef]
- Kulczyk, T.; Rychlik, M.; Lorkiewicz-Muszyńska, D.; Abreu-Głowacka, M.; Czajka-Jakubowska, A.; Przystańska, A. Computed tomography versus optical scanning: A comparison of different methods of 3D data acquisition for tooth replication. BioMed Res. Int. 2019, 2019, 4985121. [Google Scholar] [CrossRef] [Green Version]
- Magne, P.; Tan, D.T. Incisor compliance following operative procedures: A rapid 3-D finite element analysis using micro-CT data. J. Adhes. Dent. 2008, 10, 49–56. [Google Scholar] [PubMed]
- Ausiello, P.; Franciosa, P.; Martorelli, M.; Watts, D.C. Mechanical behavior of post-restored upper canine teeth: A 3D FE analysis. Dent. Mater. 2011, 27, 1285–1294. [Google Scholar] [CrossRef] [PubMed]
- Rocha, E.P.; Anchieta, R.B.; Freitas-Junior, A.C.; de Almeida, E.O.; Cattaneo, P.M.; Ko, C.C. Mechanical behavior of ceramic veneer in zirconia-based restorations: A 3-dimensional finite element analysis using microcomputed tomography data. J. Prosthet. Dent. 2011, 105, 14–20. [Google Scholar] [CrossRef] [PubMed]
- Huang, X.Q.; Hong, N.R.; Zou, L.Y.; Wu, S.Y.; Li, Y. Estimation of stress distribution and risk of failure for maxillary premolar restored by occlusal veneer with different CAD/CAM materials and preparation designs. Clin. Oral Investig. 2020, 24, 3157–3167. [Google Scholar] [CrossRef] [PubMed]
- Celebi, A.T.; Icer, E.; Eren, M.M.; Baykasoglu, C.; Mugan, A.; Yildiz, E. Thermal-stress analysis of ceramic laminate veneer restorations with different incisal preparations using micro-computed tomography-based 3D finite element models. J. Mech. Behav. Biomed. Mater. 2017, 75, 302–313. [Google Scholar] [CrossRef] [PubMed]
- Asmussen, E.; Peutzfeldt, A.; Sahafi, A. Finite element analysis of stresses in endodontically treated, dowel-restored teeth. J. Prosthet. Dent. 2005, 94, 321–329. [Google Scholar] [CrossRef] [PubMed]
- Singh, V.; Misra, A.; Marangos, O.; Park, J.; Ye, Q.; Kieweg, S.L.; Spencer, P. Fatigue life prediction of dentin–adhesive interface using micromechanical stress analysis. Dent. Mater. 2011, 27, e187–e195. [Google Scholar] [CrossRef] [Green Version]
- De Andrade, G.S.; Pinto, A.B.A.; Tribst, J.P.M.; Chun, E.P.; Borges, A.L.S.; Saavedra, G.S.F.A. Does overlay preparation design affect polymerization shrinkage stress distribution? A 3D FEA study. Comput. Methods Biomech. Biomed. Eng. 2021, 24, 1026–1034. [Google Scholar] [CrossRef]
- Atsu, S.S.; Aka, P.S.; Kucukesmen, H.C.; Kilicarslan, M.A.; Atakan, C. Age-related changes in tooth enamel as measured by electron microscopy: Implications for porcelain laminate veneers. J. Prosthet. Dent. 2005, 94, 336–341. [Google Scholar] [CrossRef]
- Blunck, U.; Fischer, S.; Hajtó, J.; Frei, S.; Frankenberger, R. Ceramic laminate veneers: Effect of preparation design and ceramic thickness on fracture resistance and marginal quality in vitro. Clin. Oral Investig. 2020, 24, 2445–2754. [Google Scholar] [CrossRef]
- O’Mahony, A.M.; Williams, J.L.; Katz, J.O.; Spencer, P. Anisotropic elastic properties of cancellous bone from a human edentulous mandible. Clin. Oral Implants Res. 2000, 11, 415–421. [Google Scholar] [CrossRef]
- Sorrentino, R.; Apicella, D.; Riccio, C.; Gherlone, E.; Zarone, F.; Aversa, R.; Garcia-Godoy, F.; Ferrari, M.; Apicella, A. Nonlinear visco-elastic finite element analysis of different porcelain veneers configuration. J. Biomed. Mater. Res. Part B Appl. Biomater. 2009, 91, 727–736. [Google Scholar] [CrossRef]
- Aversa, R.; Apicella, D.; Perillo, L.; Sorrentino, R.; Zarone, F.; Ferrari, M.; Apicella, A. Non-linear elastic three-dimensional finite element analysis on the effect of endocrown material rigidity on alveolar bone remodeling process. Dent. Mater. 2009, 25, 678–690. [Google Scholar] [CrossRef]
- Spears, I.R.; Van Noort, R.; Crompton, R.H.; Cardew, G.E.; Howard, I.C. The effects of enamel anisotropy on the distribution of stress in a tooth. J. Dent. Res. 1993, 72, 1526–1531. [Google Scholar] [CrossRef] [PubMed]
- Su, M.Z.; Chang, H.H.; Chiang, Y.C.; Cheng, J.H.; Fuh, L.J.; Wang, C.Y.; Lin, C.P. Modeling viscoelastic behavior of periodontal ligament with nonlinear finite element analysis. J. Dent. Sci. 2013, 8, 121–128. [Google Scholar] [CrossRef] [Green Version]
- Arat Bilhan, S.; Baykasoglu, C.; Bilhan, H.; Kutay, O.; Mugan, A. Effect of attachment types and number of implants supporting mandibular overdentures on stress distribution: A computed tomography-based 3D finite element analysis. J. Biomech. 2015, 48, 130–137. [Google Scholar] [CrossRef] [PubMed]
- Daas, M.; Dubois, G.; Bonnet, A.S.; Lipinski, P.; Rignon-Bret, C. A complete finite element model of a mandibular implant-retained overdenture with two implants: Comparison between rigid and resilient attachment configurations. Med. Eng. Phys. 2008, 30, 218–225. [Google Scholar] [CrossRef]
- Geng, J.P.A.; Tan, K.B.C.; Liu, G.R. Application of finite element analysis in implant dentistry: A review of the literature. J. Prosthet. Dent. 2001, 85, 585–598. [Google Scholar] [CrossRef] [Green Version]
- Richmond, B.G.; Wright, B.W.; Grosse, I.; Dechow, P.C.; Ross, C.F.; Spencer, M.A.; Strait, D.S. Finite element analysis in functional morphology. Anat. Rec. Part A Discov. Mol. Cell. Evol. Biol. 2005, 283, 259–274. [Google Scholar] [CrossRef]
- Magne, P.; Douglas, W.H. Design optimization and evolution of bonded ceramics for the anterior dentition: A finite-element analysis. Quintessence Int. 1999, 30, 661–672. [Google Scholar]
- Li, Z.; Yang, Z.; Zuo, L.; Meng, Y. A three-dimensional finite element study on anterior laminate veneers with different incisal preparations. J. Prosthet. Dent. 2014, 112, 325–333. [Google Scholar] [CrossRef]
- Sorrentino, R.; Aversa, R.; Ferro, V.; Auriemma, T.; Zarone, F.; Ferrari, M.; Apicella, A. Three-dimensional finite element analysis of strain and stress distributions in endodontically treated maxillary central incisors restored with diferent post, core and crown materials. Dent. Mater. 2007, 23, 983–993. [Google Scholar] [CrossRef]
- Dawood, S.N.; Al-Zahawi, A.R.; Sabri, L.A. Mechanical and thermal stress behavior of a conservative proposed veneer preparation design for restoring misaligned anterior teeth: A 3D finite element analysis. Appl. Sci. 2020, 10, 5814. [Google Scholar] [CrossRef]
- Jankar, A.S.; Kale, Y.; Kangane, S.; Ambekar, A.; Sinha, M.; Chaware, S. Comparative evaluation of fracture resistance of Ceramic Veneer with three different incisal design preparations-An In-vitro Study. J. Int. Oral Health. 2014, 6, 48–54. [Google Scholar]
- Zhang, Y.; Sailer, I.; Lawn, B.R. Fatigue of dental ceramics. J. Dent. 2013, 41, 1135–1147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zarone, F.; Apicella, D.; Sorrentino, R.; Ferro, V.; Aversa, R.; Apicella, A. Influence of tooth preparation design on the stress distribution in maxillary central incisors restored by means of alumina porcelain veneers: A 3D-finite element analysis. Dent. Mater. 2005, 21, 1178–1188. [Google Scholar] [CrossRef] [PubMed]
- De Bragança, G.F.; Mazão, J.D.; Versluis, A.; Soares, C.J. Effect of luting materials, presence of tooth preparation, and functional loading on stress distribution on ceramic laminate veneers: A finite element analysis. J. Prosthet. Dent. 2021, 125, 778–787. [Google Scholar] [CrossRef]
- Castelnuovo, J.; Tjan, A.H.L.; Phillips, K.; Nicholls, J.I.; Kois, J.C. Fracture load and mode of failure of ceramic veneers with different preparations. J. Prosthet. Dent. 2000, 83, 171–180. [Google Scholar] [CrossRef] [PubMed]
- Öztürk, E.; Bolay, Ş.; Hickel, R.; Ilie, N. Influence of ceramic thickness and type on micromechanical properties of light-cured adhesive bonding agents. Acta Odontol. Scand. 2014, 72, 543–548. [Google Scholar] [CrossRef] [PubMed]
- Spazzin, A.O.; Galafassi, D.; De Meira-Junior, A.D.; Braz, R.; Garbin, C.A. Influence of post and resin cement on stress distribution of maxillary central incisors restored with direct resin composite. Oper. Dent. 2009, 34, 223–229. [Google Scholar] [CrossRef] [Green Version]
- Öztürk, E.; Bolay, Ş.; Hickel, R.; Ilie, N. Shear bond strength of porcelain laminate veneers to enamel, dentine and enamel–dentine complex bonded with different adhesive luting systems. J. Dent. 2013, 41, 97–105. [Google Scholar] [CrossRef]
- Magni, E.; Ferrari, M.; Hickel, R.; Ilie, N. Evaluation of the mechanical properties of dental adhesives and glass-ionomer cements. Clin. Oral Investig. 2010, 14, 79–87. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Structures and Materials | Elasticity Modulus (MPa) | Poisson’s Ratio |
|---|---|---|
| Enamel [5] | 84,100 | 0.33 |
| Dentin [5] | 18,600 | 0.32 |
| Periodontal ligament [24] | 68.9 | 0.45 |
| Spongious bone [24] | 1370 | 0.30 |
| Cortical bone [24] | 13,700 | 0.30 |
| Adhesive [25] | 5000 | 0.29 |
| Cement with low modulus Variolink Veneer, Ivoclar Vivadent AG, Schaan, Liechtenstein [*] | 4500 | 0.24 |
| Cement with high modulus Ena Cem HF, Micerium S.p.A., Avegno (GE), Italy [*] | 12,850 | 0.24 |
| Porcelain laminate veneer IPS e.max Press, Ivoclar Vivadent AG, Schaan, Liechtenstein [*] | 95,000 | 0.23 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mert Eren, M.; Celebi, A.T.; İçer, E.; Baykasoğlu, C.; Mugan, A.; Yücel, T.; Yıldız, E. Biomechanical Behavior Evaluation of Resin Cement with Different Elastic Modulus on Porcelain Laminate Veneer Restorations Using Micro-CT-Based Finite Element Analysis. Materials 2023, 16, 2378. https://doi.org/10.3390/ma16062378
Mert Eren M, Celebi AT, İçer E, Baykasoğlu C, Mugan A, Yücel T, Yıldız E. Biomechanical Behavior Evaluation of Resin Cement with Different Elastic Modulus on Porcelain Laminate Veneer Restorations Using Micro-CT-Based Finite Element Analysis. Materials. 2023; 16(6):2378. https://doi.org/10.3390/ma16062378
Chicago/Turabian StyleMert Eren, Meltem, Alper Tunga Celebi, Esra İçer, Cengiz Baykasoğlu, Ata Mugan, Taner Yücel, and Esra Yıldız. 2023. "Biomechanical Behavior Evaluation of Resin Cement with Different Elastic Modulus on Porcelain Laminate Veneer Restorations Using Micro-CT-Based Finite Element Analysis" Materials 16, no. 6: 2378. https://doi.org/10.3390/ma16062378
APA StyleMert Eren, M., Celebi, A. T., İçer, E., Baykasoğlu, C., Mugan, A., Yücel, T., & Yıldız, E. (2023). Biomechanical Behavior Evaluation of Resin Cement with Different Elastic Modulus on Porcelain Laminate Veneer Restorations Using Micro-CT-Based Finite Element Analysis. Materials, 16(6), 2378. https://doi.org/10.3390/ma16062378