Dental Glass Ionomer Cements as Permanent Filling Materials? – Properties, Limitations and Future Trends

Abstract
:1. Introduction
2. Historical Development
3. Cement Composition
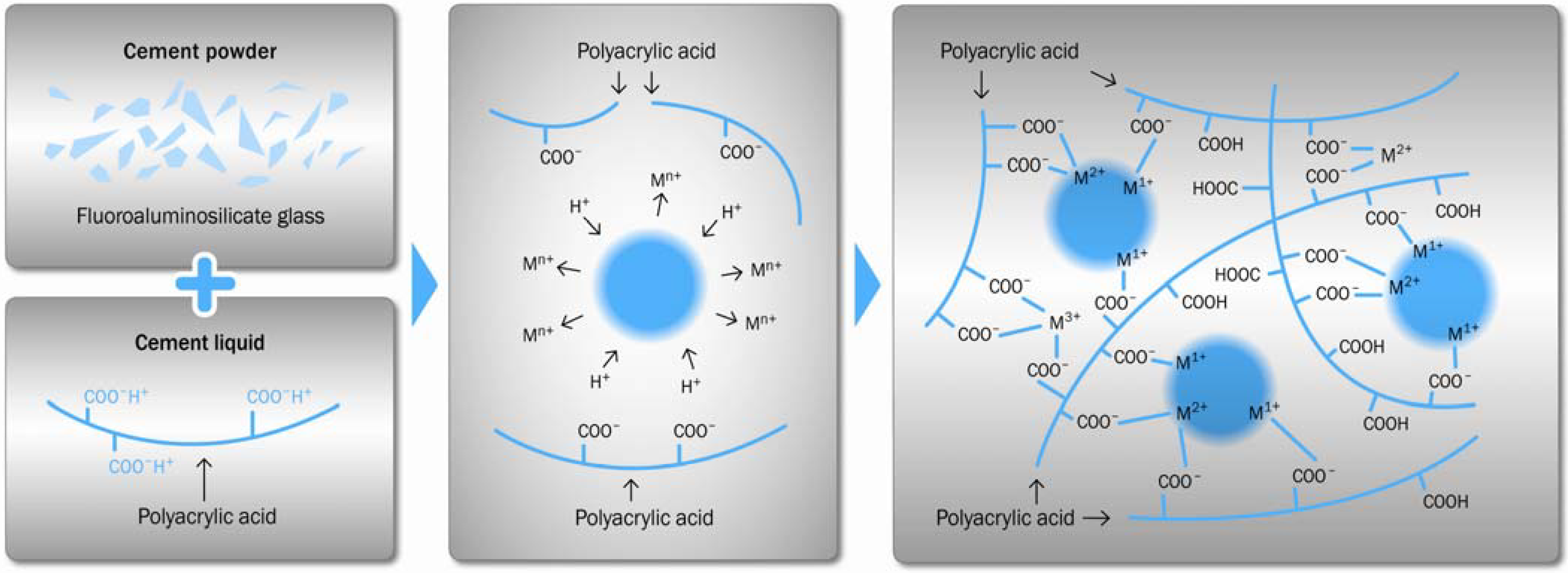
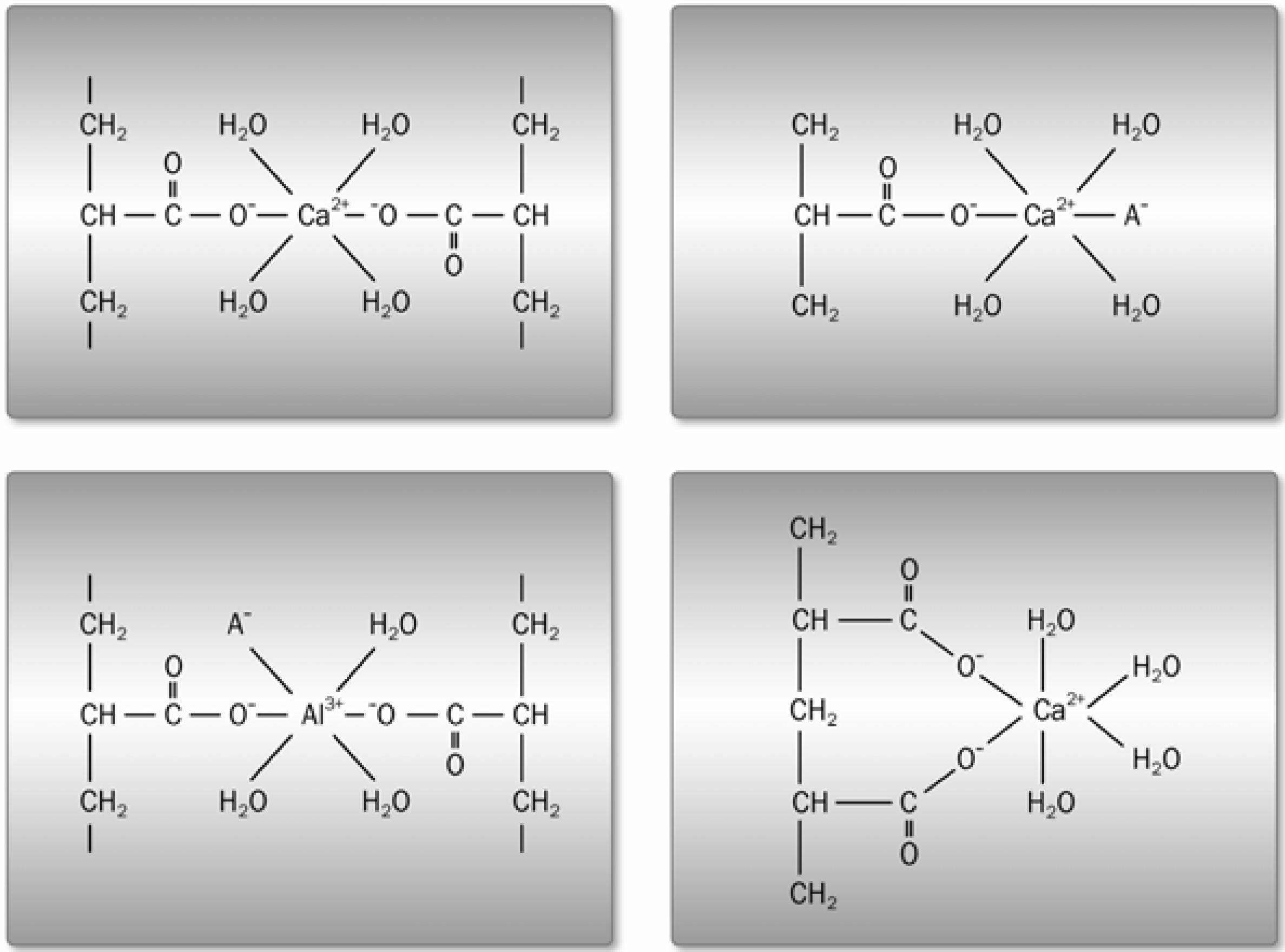
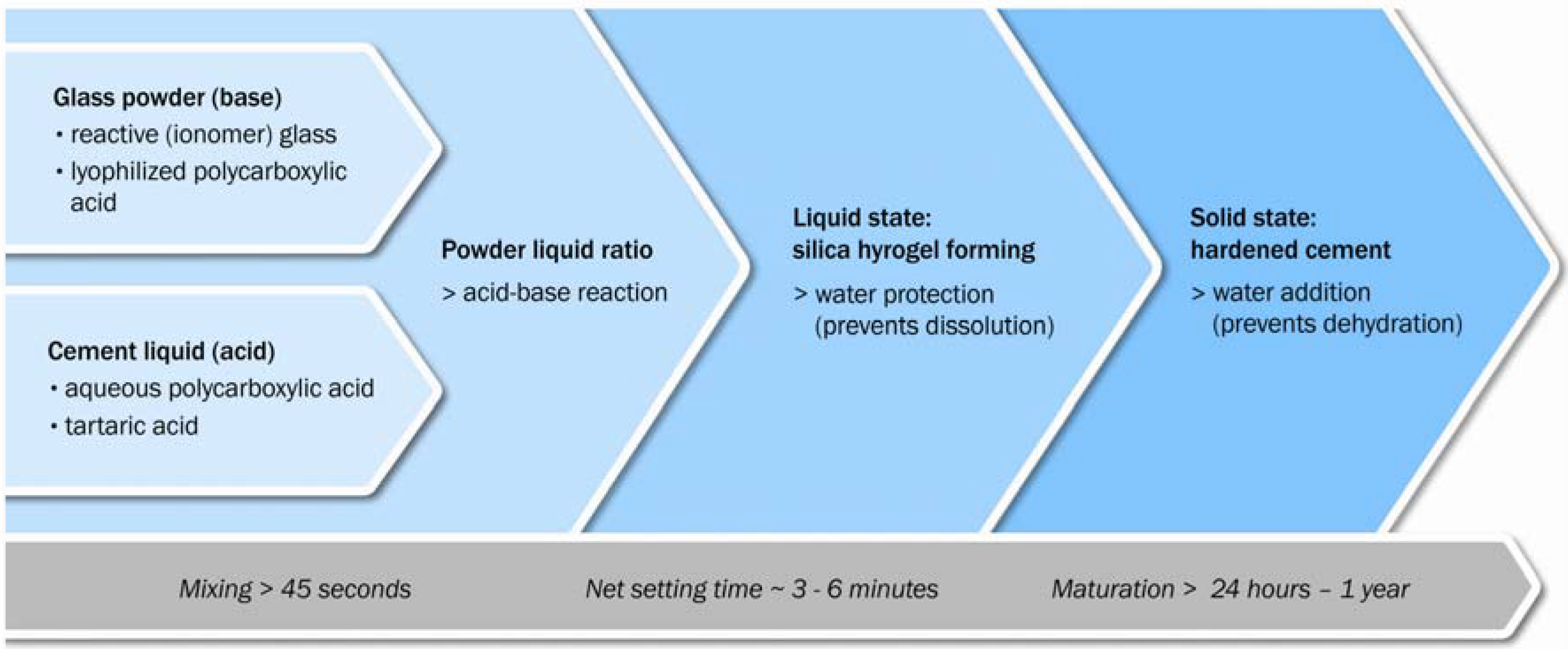
3.1. Acid-Base Reactions



3.2. Reactive (Ionomer) Glasses
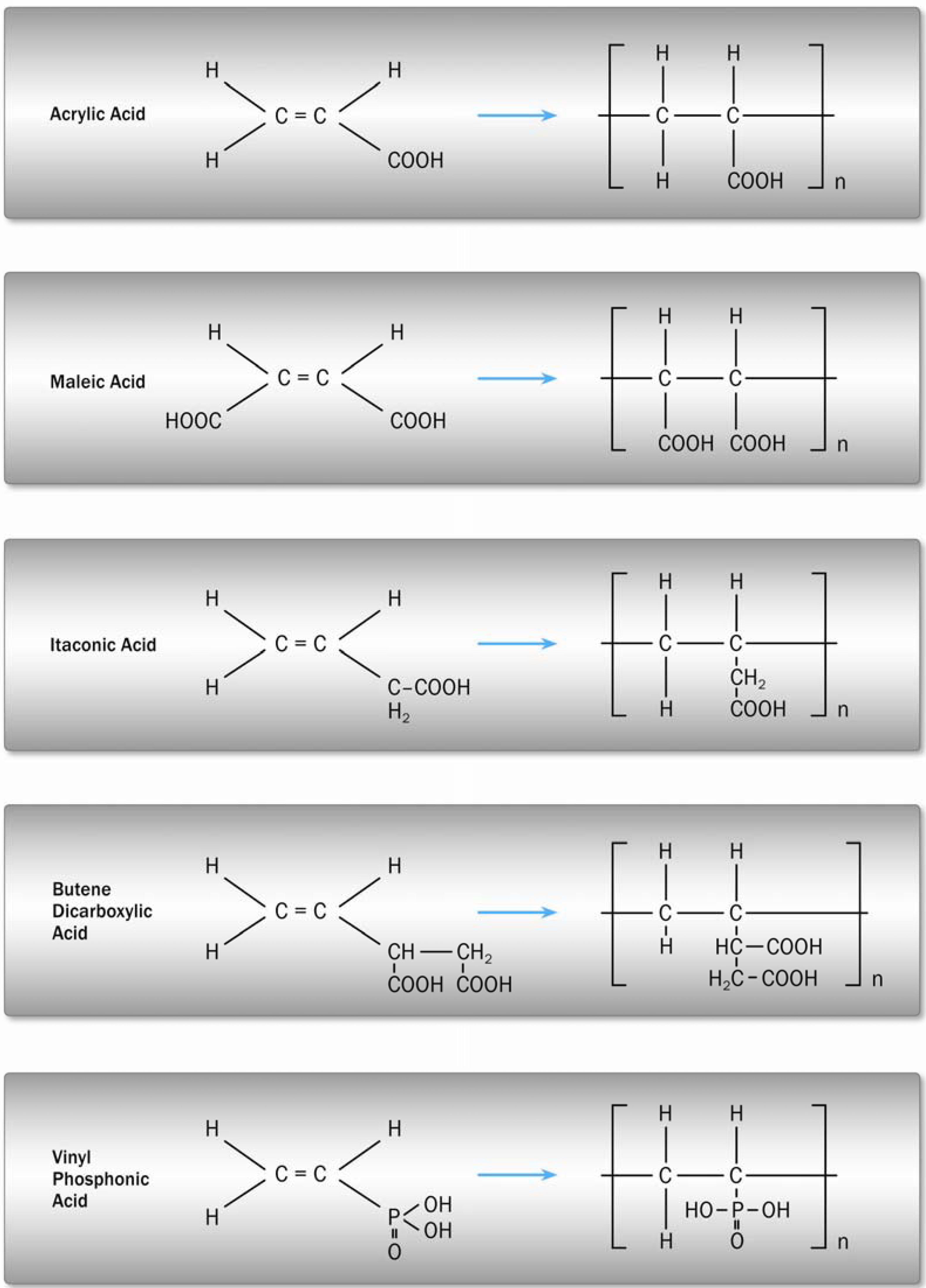
3.3. Polycarboxylic Acids

4. Material Properties
4.1. Linear-Elastic Mechanical Properties

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | FS [MPa] | CS [MPa] | Material | Test conditions |
|---|---|---|---|---|
| Bapna et al. 2002 [50] | 30.8/23.0 47.1/21.4 | - | Fuji II | 3-PB, as, 24 h/9 m |
| Dowling et al. 2009 [51] | - | 126/129 | Ketac Fil Plus | Capmix, ws, 24 h/Rotomix |
| Fleming et al. 2003 [52] | - | 87.9/67.9 | Fuji IX GP | Capsules, ws, 24 h/handmix |
| Iazzetti. et al. 2001 [53] | 22.6/15.4 | - | Fuji IX | 3-PB, ws, 24 h/7 d |
| Irie et al. 2008 [54] | 1.8/29.2 | - | Fuji IX GP | 3-PB, ws, immediate/24 h |
| Lohbauer et al. 2003 [41] | 19.7/33.0/35.2/36.7 | - | Ketac Molar | 4-PB, ws, 24 h/8 d/30 d/90 d |
| Lucksanasombool et al. 2002 [49] | 29.2 | 211 | Fuji IX | 3-PB, ws. 1 h |
| Moshaverinia et al. 2008 [55] | 14.8 | 161.0 | Fuji II | BB, ws, 24 h |
| Peez et al. 2006 [56] | 51 | 244 | Ketac Molar | 3-PB, ws, 24 h |
| Prosser et al. 1986 [44] | 16.4–33.0 | - | Experimental | p/l ratio, ws, 24 h |
| Xie et al. 2000 [11] | 22.6 | 251 | Ketac Fil | 3-PB, ws, 7 d |
4.2. Wear and Fatigue
4.3. Thermal Compatibility
| Material | CTE [ppm] |
|---|---|
| GIC | 10.2–11.4 |
| Resin composite | 14–50 |
| Amalgam | 22.1–28.0 |
| Porcelain | 12.0 |
| Human enamel | 11.4 |
| Human dentin | 8.3 |
4.4. Adhesion to Tooth Structure
4.5. Anticariogenic Properties
4.6. Clinical Performance
5. Reinforcing Concepts
5.1. Porosity Reduction

5.2. Second Phase Particle Reinforcement
5.3. Resin Modification
5.4. Resin Coating

6. Outlook
References
- Friberg, L.T.; Schrauzer, G.N. Status Quo and Perspectives of Amalgam and Other Dental Materials; Thieme: Stuttgart, Germany, 1995. [Google Scholar]
- Roulet, J.F. Benefits and disadvantages of tooth-coloured alternatives to amalgam. J. Dent. 1997, 25, 459–473. [Google Scholar] [CrossRef] [PubMed]
- Hickel, R.; Dasch, W.; Janda, R.; Tyas, M.; Anusavice, K. New direct restorative materials. Int. Dent. J. 1998, 48, 3–16. [Google Scholar] [CrossRef] [PubMed]
- Krämer, N.; Lohbauer, U.; Frankenberger, R. Adhesive luting of indirect restorations. Am. J. Dent. 2000, 13, 60–67. [Google Scholar]
- Manhart, J.; Kunzelmann, K.H.; Chen, H.Y.; Hickel, R. Mechanical properties of new composite restorative materials. J. Biomed. Mater. Res. 2000, 53, 353–361. [Google Scholar] [CrossRef] [PubMed]
- Van Meerbeek, B.; De Munck, J.; Yoshida, Y.; Inoue, S.; Vargas, M.; Vijay, P.; Van Landuyt, K.; Lambrechts, P.; Vanherle, G. Buonocore memorial lecture. Adhesion to enamel and dentin: current status and future challenges. Oper. Dent. 2003, 28, 215–235. [Google Scholar]
- Saito, S.; Tosaki, S.; Hirota, K. Advances in Glass Ionomer Cements; Davidson, C.L., Mjör, I.A., Eds.; Quintessence Publishing Co: Berlin, Germany, 1999; pp. 15–50. [Google Scholar]
- Nicholson, J.W. Chemistry of glass-ionomer cements: A review. Biomaterials 1998, 19, 485–494. [Google Scholar] [CrossRef] [PubMed]
- Anusavice, K. Challenges to the development of esthetic alternatives to dental amalgam in an dental research center. Trans. Acad. Dent. Mater. 1996, 9, 25–50. [Google Scholar]
- Yip, H.K.; Tay, F.R.; Ngo, H.; Smales, R.J.; Pashley, D.H. Bonding of contemporary glass ionomer cements to dentin. Dent. Mater. 2001, 17, 456–470. [Google Scholar] [CrossRef] [PubMed]
- Xie, D.; Brantley, W.A.; Culbertson, B.M.; Wang, G. Mechanical properties and microstructures of glass-ionomer cements. Dent. Mater. 2000, 16, 129–138. [Google Scholar] [CrossRef] [PubMed]
- Pelka, M.; Ebert, J.; Schneider, H.; Krämer, N.; Petschelt, A. Comparison of two- and three-body wear of glass-ionomers and composites. Eur. J. Oral. Sci. 1996, 104, 132–137. [Google Scholar] [CrossRef] [PubMed]
- Hickel, R.; Manhart, J.; Garcia-Godoy, F. Clinical results and new developments of direct posterior restorations. Am. J. Dent. 2000, 13, 41–54. [Google Scholar]
- Wilson, A.D.; McLean, J.W. Glass-Ionomer Cement; Quintessence Publishing Co: Berlin, Germany, 1988. [Google Scholar]
- Kobayashi, M.; Kon, M.; Miyai, K.; Asaoka, K. Strengthening of glass-ionomer cement by compounding short fibres with CaO-P2O5-SiO2-Al2O3 glass. Biomaterials 2000, 21, 2051–2058. [Google Scholar] [CrossRef] [PubMed]
- Lohbauer, U.; Walker, J.; Nikolaenko, S.; Werner, J.; Clare, A.; Petschelt, A.; Greil, P. Reactive fiber reinorced glass ionomer cements. Biomaterials 2003, 24, 2901–2907. [Google Scholar] [CrossRef] [PubMed]
- Smith, D. Development of glass ionomer cement systems. In Glass Ionomers: The Next Generation. 2nd International Symposium on Glass Ionomers, Philadelphia, PA, USA, June, 1994; Hunt, P.R., Ed.; International Symposia in Dentistry: Philadelphia, PA, USA, 1994. [Google Scholar]
- Craig, R.G. Restorative Dental Materials, 11th ed.; Mosby: London, UK, 2002. [Google Scholar]
- Wilson, A.D. Alumino-silicate polyacrylic acid and related cements. Br. Polym. J. 1974, 6, 165–179. [Google Scholar] [CrossRef]
- Wilson, A.D.; Kent, B.E.; Clinton, D.; Miller, R.P. The formation and microstructure of dental silicate cements. J. Mater. Sci. 1972, 7, 220–238. [Google Scholar] [CrossRef]
- Nicholson, J.W.; Brookman, P.J.; Lacy, O.M.; Wilson, A.D. Fourier transform infrared spectroscopic study of the role of tartaric acid in glass-ionomer dental cements. J. Dent. Res. 1988, 67, 1451–1454. [Google Scholar] [CrossRef] [PubMed]
- Barry, T.I.; Clinton, D.J.; Wilson, A.D. The structure of a glass-ionomer cement and its relationship to the setting process. J. Dent. Res. 1979, 58, 1072–1079. [Google Scholar] [CrossRef] [PubMed]
- Hückel, W. Structural Chemistry of Inorganic Compounds; Elsevier: Amsterdam, The Netherlands, 1950; Volume 1. [Google Scholar]
- Wasson, E.A.; Nicholson, J.W. New aspects of the setting of glass-ionomer cements. J. Dent. Res. 1993, 72, 481–483. [Google Scholar] [CrossRef] [PubMed]
- Nicholson, J.W.; Wilson, A.D. The effect of storage in aqueous solutions on glass-ionomer and zinc polycarboxylate dental cements. J. Mater. Sci.: Mater. Med. 2000, 11, 357–360. [Google Scholar]
- Crisp, S.; Lewis, B.G.; Wilson, A.D. Characterization of glass-ionomer cements: 5. The effect of tartaric acid concentration in the liquid component. J. Dent. 1979, 7, 304–312. [Google Scholar] [CrossRef] [PubMed]
- Wasson, E.A.; Nicholson, J.W. Studies on the setting chemistry of glass-ionomer cements. Clin. Mater. 1991, 7, 289–293. [Google Scholar] [CrossRef]
- Hench, L.L. Bioceramics: From concept to clinic. J. Am. Ceram. Soc. 1991, 47, 1487–1510. [Google Scholar] [CrossRef]
- Kent, B.E.; Lewis, B.G.; Wilson, A.D. Glass ionomer cement formulations: The preparation of novel fluoroalumosilicate glasses high in fluorine. J. Dent. Res. 1979, 58, 1607–1619. [Google Scholar] [CrossRef] [PubMed]
- Griffin, S.; Hill, R.G. Influence of glass composition on the properties of glass polyalkenoate cements. Part I: Influence of aluminum to silicon ratio. Biomaterials 1999, 20, 1579–1586. [Google Scholar] [CrossRef] [PubMed]
- Yoldas, B.E. The nature of the coexistence of four- and six-coordinated AL3+ in glass. Phys. Chem. Glass. 1971, 12, 28–32. [Google Scholar]
- Vogel, W. Glaschemie; Springer: Berlin, Germany, 1992. [Google Scholar]
- DeBarra, E.; Hill, R.G. Influence of glass composition on the properties of glass polyalkenoate cements. Part IIII: influence of fluorite content. Biomaterials 2000, 21, 563–569. [Google Scholar] [CrossRef] [PubMed]
- Griffin, S.; Hill, R.G. Influence of glass composition on the properties of glass polyalkenoate cements. Part II: Influence of fluorine content. Biomaterials 2000, 21, 693–698. [Google Scholar] [CrossRef] [PubMed]
- Wilson, A.D.; Crisp, S.; Prosser, H.J.; Lewis, B.G.; Merson, S.A. Aluminosilicate glasses for polyelectrolyte cements. Ind. Eng. Chem. Prod. Res. Dev. 1980, 19, 263–270. [Google Scholar] [CrossRef]
- Wood, D.; Hill, R. Structure-property relationship in ionomer glasses. Clin. Mater. 1991, 7, 301–312. [Google Scholar] [CrossRef]
- Billington, R.W.; Towler, M.; Hadley, P.; Pearson, G.J. Effects on glass ionomer of NaF addition. J. Dent. Res. 1998, 77, 1226. [Google Scholar]
- DeBarra, E.; Hill, R.G. Influence of alkali metal ions on the fracture properties of glass polyalkenoate (ionomer) cements. Biomaterials 1998, 19, 495–502. [Google Scholar] [CrossRef] [PubMed]
- Griffin, S.; Hill, R. Influence of poly(acrylic acid) molar mass on the fracture properties of glass polyalkenoate cement. J. Mater. Sci. 1998, 33, 5383–5396. [Google Scholar] [CrossRef]
- Cattani-Lorente, M.A.; Godin, C.; Meyer, J.M. Mechanical behavior of glass ionomer cements affected by long-term storage in water. Dent. Mater. 1994, 10, 37–44. [Google Scholar] [CrossRef] [PubMed]
- Lohbauer, U.; Frankenberger, R.; Krämer, N.; Petschelt, A. Time-dependent strength and fatigue resistance of dental direct restorative materials. J. Mater. Sci.: Mater. Med. 2003, 14, 1047–1053. [Google Scholar] [CrossRef]
- Hill, R.G. The fracture properties of glass polyalkenoate cements as a function of cement age. J. Mater. Sci. 1993, 28, 3851–3858. [Google Scholar] [CrossRef]
- Naasan, M.A.; Watson, T.F. Concentional glass ionomers as posterior restorations: A status report for the American Journal of Dentistry. Am. J. Dent. 1998, 11, 36–45. [Google Scholar] [PubMed]
- Prosser, H.J.; Powis, D.R.; Wilson, A.D. Glass-ionomer cements of improved flexural strength. J. Dent. Res. 1986, 65, 146–148. [Google Scholar] [CrossRef]
- Nicholson, J.W.; Amiri, M.A. The interaction of dental cements with aqueous solutions of varying pH. J. Mater. Sci.: Mater. Med. 1998, 9, 549–554. [Google Scholar] [CrossRef]
- Small, I.C.B.; Watson, T.F.; Chadwick, A.V.; Sidhu, S.K. Water sorption in resin-modified glass-ionomer cements: An in vitro comparison with other materials. Biomaterials 1998, 19, 545–550. [Google Scholar] [CrossRef] [PubMed]
- Soltesz, U.; Leupolz, M. Dimensionsverhalten von Glasionomerzementen in trockner und feuchter Umgebung. Dtsch. Zahnärztl. Z. 1993, 48, 431–435. [Google Scholar]
- Hill, R.G.; Wilson, A.D.; Warrens, C.P. The influence of poly (acrylic acid) molecular weight on the fracture toughness of glass-ionomer cements. J. Mater. Sci. 1989, 24, 363–371. [Google Scholar] [CrossRef]
- Lucksanasombool, P.; Higgs, W.A.J.; Higgs, R.J.E.D.; Swain, M.V. Time dependence of the mechanical properties of GICs in simulated physiological conditions. J. Mater. Sci.: Mater. Med. 2002, 13, 745–750. [Google Scholar] [CrossRef]
- Bapna, M.S.; Gadia, C.M.; Drummond, J.L. Effects of aging and cyclic loading on the mechanical properties of glass ionomer cements. Eur. J. Oral. Sci. 2002, 110, 330–334. [Google Scholar] [CrossRef] [PubMed]
- Dowling, A.H.; Fleming, G.J.P. Are encapsulated anterior glass-ionomer restoratives better than their hand-mixed equivalents? J. Dent. 2009, 37, 133–140. [Google Scholar] [CrossRef] [PubMed]
- Fleming, G.J.; Zala, D.M. An assessment of encapsulated versus hand-mixed glass ionomer restoratives. Oper. Dent. 2003, 28, 168–177. [Google Scholar] [PubMed]
- Iazzetti, G.; Burgess, J.O.; Gardiner, D. Selected mechanical properties of fluoride-releasing restorative materials. Oper. Dent. 2001, 26, 21–26. [Google Scholar] [PubMed]
- Irie, M.; Maruo, Y.; Nishigawa, G.; Suzuki, K.; Watts, D.C. Class I gap-formation in highly-viscous glass-ionomer restorations: Delayed vs. immediate polishing. Oper. Dent. 2008, 33, 196–202. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moshaverinia, A.; Ansari, S.; Movasaghi, Z.; Billington, R.W.; Darr, J.A.; Rehman, I.U. Modification of conventional glass-ionomer cements with N-vinylpyrrolidone containing polyacids, nano-hydroxy and fluoroapatite to improve mechanical properties. Dent. Mater. 2008, 24, 1381–1390. [Google Scholar] [CrossRef] [PubMed]
- Peez, R.; Frank, S. The physical-mechanical performance of the new KetacTM Molar Easymix compared to commercially available glass ionomer restoratives. J. Dent. 2006, 34, 582–587. [Google Scholar] [CrossRef] [PubMed]
- Braem, M.; Lambrechts, P.; Vanherle, G. Clinical relevance of laboratory fatigue studies. J. Dent. 1994, 22, 97–102. [Google Scholar] [CrossRef] [PubMed]
- Mioche, L.; Hiiemae, K.M.; Palmer, J.B. A posterior-anterior videofluorographic study of the intra-oral management of food in man. Arch. Oral. Biol. 2002, 47, 267–280. [Google Scholar] [CrossRef] [PubMed]
- Kunzelmann, K.H. Glass-ionomer cements, cemet cements, hybrid-glass-ionomers and compomers—laboratory trials—wear resistance. Trans. Acad. Dent. Mater. 1996, 9, 89–104. [Google Scholar]
- Davidson, C.L.; deGee, A.J. Verschleissverhalten dentaler composite-materialien. grundlage der tribologie und in-vitro-testung von composites und glas-ionomer-zementen. Phillip J. 1996, 13, 171–177. [Google Scholar]
- Soltesz, U.; Benkeser, G. Fatigue Behavior of Filling Materials; Oral Implantology and Biomaterials: Amsterdam, The Netherlands, 1989; pp. 281–286. [Google Scholar]
- Lohbauer, U.; Petschelt, A.; Greil, P. Lifetime prediction of CAD/CAM dental ceramics. J. Biomed. Mater. Res. 2002, 63, 780–785. [Google Scholar] [CrossRef] [PubMed]
- Esser, M.; Tinschert, J.; Marx, R. Material characteristics of the hard tissues of bovine versus human teeth. Dtsch. Zahnärztl. Z 1998, 53, 713–717. [Google Scholar]
- Wilson, A.D.; Prosser, H.J.; Powis, D.M. Mechanism of adhesion of polyelectrolyte cements to hydroxyapatite. J. Dent. Res. 1983, 62, 590–592. [Google Scholar] [CrossRef] [PubMed]
- Erickson, R.; Glasspoole, E.A. Bonding to Tooth Structure: A Comparison of glass ionomer cements and composite resin systems. In Glass Ionomers: The Next Generation. 2nd International Symposium on Glass Ionomers; Philadelphia, PA, USA, June, 1994; Hunt, P.R., Ed.; International Symposia in Dentistry: Philadelphia, PA, USA, 1994. [Google Scholar]
- Akinmade, A.O.; Nicholson, J.W. Glass-ionomer cements as adhesives. Part I: Fundamental aspects and their clinical relevance. J. Mater. Sci.: Mater. Med. 1993, 4, 95–101. [Google Scholar] [CrossRef]
- Powis, D.R.; Folleras, T.; Merson, S.A.; Wilson, A.D. Improved adhesion of a glass-ionomer cement to dentin and enamel. J. Dent. Res. 1982, 61, 1416–1422. [Google Scholar] [CrossRef] [PubMed]
- Mak, Y.F.; Lai, S.C.N.; Cheung, G.S.P.; Chan, A.W.K.; Tay, F.R.; Pashley, D.H. Micro-tensile bond testing to dentin and an indirect resin composite. Dent. Mater. 2002, 18, 609–621. [Google Scholar] [CrossRef] [PubMed]
- Wiegand, A.; Buchalla, W.; Attin, T. Review on fluoride-releasing restorative materials--fluoride release and uptake characteristics, antibacterial activity and influence on caries formation. Dent. Mater. 2007, 23, 343–362. [Google Scholar] [CrossRef] [PubMed]
- Forsten, L. Fluoride release and uptake by glass-ionomers and related materials and its clinical effect. Biomaterials 1998, 19, 503–508. [Google Scholar] [CrossRef] [PubMed]
- Momoi, Y.; McCabe, J.F. Fluoride release from light-activated glass ionomer restorative materials. Dent. Mater. 1993, 9, 151–154. [Google Scholar] [CrossRef] [PubMed]
- Köhler, B.; Rasmusson, C.G.; Ödman, P. A five-year clinical evaluation of class II composite resin restorations. J. Dent. 2000, 28, 111–116. [Google Scholar] [CrossRef] [PubMed]
- Frankenberger, R.; Garcia-Godoy, F.; Lohbauer, U.; Petschelt, A.; Krämer, N. Evaluation of resin composite materials. Part I: In vitro investigations. Am. J. Dent. 2005, 18, 23–27. [Google Scholar] [PubMed]
- Burke, F.J.T.; Wilson, N.H.F.; Cheung, S.W.; Mjör, I.A. Influence of patient factors on age of restorations at failure and reasons for their placement and replacement. J. Dent. 2001, 29, 317–324. [Google Scholar] [CrossRef] [PubMed]
- Klinge, S.; Kunstmann, K.; Frankenberger, R.; Krämer, N. Clinical behavior of viscous glass-ionomer cement in classes I and II cavities. J. Dent. Res. 1999, 78, 2285. [Google Scholar]
- Guggenberger, R.; May, R.; Stefan, K.P. New trends in glass-ionomer chemistry. Biomaterials 1998, 19, 479–483. [Google Scholar] [CrossRef] [PubMed]
- Jorgensen, K.D.; Iwaku, M.; Wakumoto, S. Vacuum-mixing of silicate cement. Acta Odontol. Scand. 1969, 27, 453–465. [Google Scholar] [CrossRef]
- Jones, C.S.; Pearson, G.J.; Billington, R.W. Effects of viscosity in capsulated glass-ionomer cements. J. Dent. Res. 1997, 76, 432. [Google Scholar]
- Nomoto, R.; Komoriyama, M.; McCabe, J.F.; Hirano, S. Effect of mixing method on the porosity of encapsulated glass ionomer cement. Dent. Mater. 2004, 20, 972–978. [Google Scholar] [CrossRef] [PubMed]
- Ngo, H.; Peters, M.C.; Mount, G.J. Porosity reduction as a way to increase shearing strength of capsulated glass-ionomer cements. Trans. Acad. Dent. Mater. 1996, 9, 258. [Google Scholar]
- Lohbauer, U.; Pelka, M.; Frankenberger, R.; Krämer, N. Influence of mixing procedures on wear resistance of glass ionomer cements. J. Dent. Res. 1999, 78, 988. [Google Scholar]
- Kerby, R.E.; Bleiholder, R.F. Physical properties of stainless steel and silver reinforced glass-ionomer cements. J. Dent. Res. 1991, 70, 1358–1361. [Google Scholar] [CrossRef] [PubMed]
- Kilpatrick, N.M.; Murray, J.J.; McCabe, J.F. The use of a reinforced glass-ionomer cement for the restoration of primary molars: A clinical trial. Br. Dent. J. 1995, 179, 175–179. [Google Scholar] [CrossRef] [PubMed]
- Sarkar, N.K. Metal-matrix interface in reinforced glass-ionomers. Dent. Mater. 1999, 15, 421–425. [Google Scholar] [CrossRef] [PubMed]
- Williams, J.A.; Billington, R.W.; Pearson, G. Silver and fluoride release from metal-reinforced glass-ionomer filling materials. J. Oral. Rehabil. 1997, 24, 369–375. [Google Scholar] [CrossRef] [PubMed]
- Kawano, F.; Kon, M.; Kobayashi, M.; Miyai, K. Reinforcement effect of short glass fibers with CaO-P2O5-SiO2-Al2O3 glass on strength of glass-ionomer cement. J. Dent. 2001, 29, 377–380. [Google Scholar] [CrossRef] [PubMed]
- Xu, H.H.K.; Eichmiller, F.C.; Barndt, P.R. Effects of fiber length and volume fraction on the reinforcement of calcium phosphate cement. J. Mater. Sci.: Mater. Med. 2001, 12, 57–65. [Google Scholar] [CrossRef]
- Lohbauer, U.; Frankenberger, R.; Clare, A.; Petschelt, A.; Greil, P. Toughening of glass ionomer cements by reactive glass fibers. Biomaterials 2004, 25, 5217–5225. [Google Scholar] [CrossRef] [PubMed]
- Yap, A.U.; Pek, Y.S.; Kumar, R.A.; Cheang, P.; Khor, K.A. Experimental studies on a new bioactive material: HAIonomer cements. Biomaterials 2002, 23, 955–962. [Google Scholar] [CrossRef] [PubMed]
- Gu, Y.W.; Yap, A.U.; Cheang, P.; Khor, K.A. Effects of incorporation of HA/ZrO(2) into glass ionomer cement (GIC). Biomaterials 2005, 26, 713–720. [Google Scholar] [CrossRef] [PubMed]
- McLean, J.W.; Nicholson, J.W.; Wilson, A.D. Proposed nomenclature for glass-ionomer dental cements and related materials. Quintessence Int. 1994, 25, 587–589. [Google Scholar] [PubMed]
- Mount, G.J. Buonocore Memorial Lecture. Glass-ionomer cements: Past, present and future. Oper. Dent. 1994, 19, 82–90. [Google Scholar] [PubMed]
- Mitra, S.B. Adhesion to dentin and physical properties of a light-cured glass-ionomer liner/base. J. Dent. Res. 1991, 70, 72–74. [Google Scholar] [CrossRef] [PubMed]
- Uno, S.; Finger, W.J.; Fritz, U. Long-term mechanical characteristics of resin modified glass ionomer restorative materials. Dent. Mater. 1996, 12, 64–69. [Google Scholar] [CrossRef] [PubMed]
- Sidhu, S.K.; Sherriff, M.; Watson, T.F. The effects of maturity and dehydration shrinkage on resin-modified glass ionomer restorations. J. Dent. Res. 1997, 76, 1495–1501. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, A.P.; Serra, M.C.; Paulillo, L.A.; Rodrigues Junior, A.L. Effectiveness of surface protection for resin-modified glass ionomer materials. Quintessence Int. 1999, 30, 427–431. [Google Scholar] [PubMed]
- Miyazaki, M.; Moore, B.K.; Onose, H. Effect of surface coatings on flexural properties of glass ionomers. Eur. J. Oral. Sci. 1996, 104, 600–604. [Google Scholar] [CrossRef] [PubMed]
- Kunzelmann, K.H. Glass-ionomer Cements, Cemet Cements, Hybrid-Glass-ionomers and compomers-laboratory trials wear resistance. Trans. Acad. Dent. Mater. 1996, 9, 89–104. [Google Scholar]
- Al-Naimi, O.T.; Itota, T.; Hobson, R.S.; McCabe, J.F. Fluoride release for restorative materials and its effect on biofilm formation in natural saliva. J. Mater. Sci.: Mater. Med. 2008, 19, 1243–1248. [Google Scholar] [CrossRef]
- Sidhu, S.K. Clinical evaluations of resin-modified glass-ionomer restorations. Dent. Mater. 2010, 26, 7–12. [Google Scholar] [CrossRef] [PubMed]
- Gemalmaz, D.; Yoruc, B.; Ozcan, M.; Alkumru, H.N. Effect of early water contact on solubility of glass ionomer luting cements. J. Prosthet. Dent. 1998, 80, 474–478. [Google Scholar] [CrossRef] [PubMed]
- Earl, M.S.; Hume, W.R.; Mount, G.J. Effect of varnishes and other surface treatments on water movement across the glass-ionomer cement surface. Aust. Dent. J. 1985, 30, 298–301. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues; Garcia, R.C.; De Goes, M.F.; Del Bel Cury, A.A. Influence of protecting agents on the solubility of glass ionomers. Am. J. Dent. 1995, 8, 294–296. [Google Scholar] [PubMed]
- Hotta, M.; Hirukawa, H.; Yamamoto, K. Effect of coating materials on restorative glass-ionomer cement surface. Oper. Dent. 1992, 17, 57–61. [Google Scholar] [PubMed]
- Using glass ionomers. Council on dental materials, instruments, and equipment. J. Am. Dent. Assoc. 1990, 121, 181–188. [Google Scholar]
- Tanaka, K.; Kato, K.; Noguchi, T.; Nakaseko, H.; Akahane, S. Change in translucency of posterior restorative glass-ionomer cements. J. Dent. Res. 2007, 86, 2025. [Google Scholar]
- Williams, J.A.; Billington, R.W.; Pearson, G.J. Effect of moisture protective coatings on the strength of a modern metal-reinforced glass–ionomer cement. J. Oral. Rehabil. 1998, 25, 535–540. [Google Scholar] [CrossRef] [PubMed]
- Kato, K.; Yarimizu, H.; Nakaseko, H.; Sakuma, T. Influence of coating material on conventional glass-ionomer cement. J. Dent. Res. 2008, 87, 487. [Google Scholar]
© 2010 by the authors; licensee Molecular Diversity Preservation International, Basel, Switzerland. This article is an open-access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Lohbauer, U. Dental Glass Ionomer Cements as Permanent Filling Materials? – Properties, Limitations and Future Trends. Materials 2010, 3, 76-96. https://doi.org/10.3390/ma3010076
Lohbauer U. Dental Glass Ionomer Cements as Permanent Filling Materials? – Properties, Limitations and Future Trends. Materials. 2010; 3(1):76-96. https://doi.org/10.3390/ma3010076
Chicago/Turabian StyleLohbauer, Ulrich. 2010. "Dental Glass Ionomer Cements as Permanent Filling Materials? – Properties, Limitations and Future Trends" Materials 3, no. 1: 76-96. https://doi.org/10.3390/ma3010076
APA StyleLohbauer, U. (2010). Dental Glass Ionomer Cements as Permanent Filling Materials? – Properties, Limitations and Future Trends. Materials, 3(1), 76-96. https://doi.org/10.3390/ma3010076