
Forest Therapy for Women with Gynaecological Cancer—A Feasibility Study to Find New Alternatives in Cancer Rehabilitation




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
1.1. Rehabilitation in Gynaecological Cancer
1.2. The Use of Nature-Based Interventions, Forest Therapy and Forest Bathing
1.3. Forest Bathing in Cancer Rehabilitation
- Is a nature-based group intervention with forest bathing perceived as beneficial by the participants?
- Which aspects of the intervention are perceived as beneficial vs. non-beneficial?
- Which aspects of the forest site are perceived as beneficial vs. non-beneficial?
- Can forest bathing improve quality of life and mood, and reduce anxiety/depression and fatigue?
- What problems or complaints are positively affected by the intervention?
- What components of the forest bathing intervention contribute to the effect?
2. Materials and Methods
2.1. Participants and Recruitment
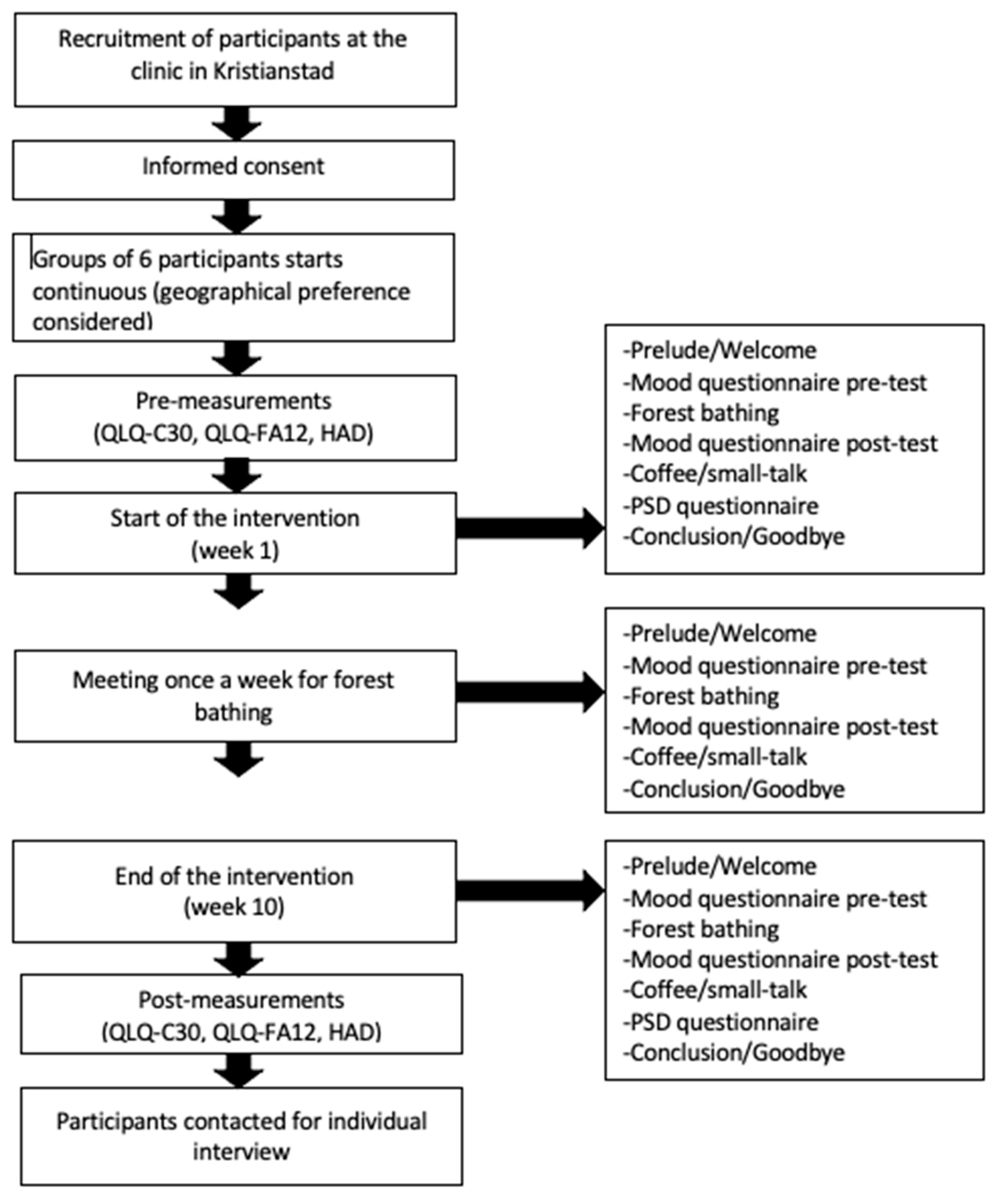
2.2. The Intervention
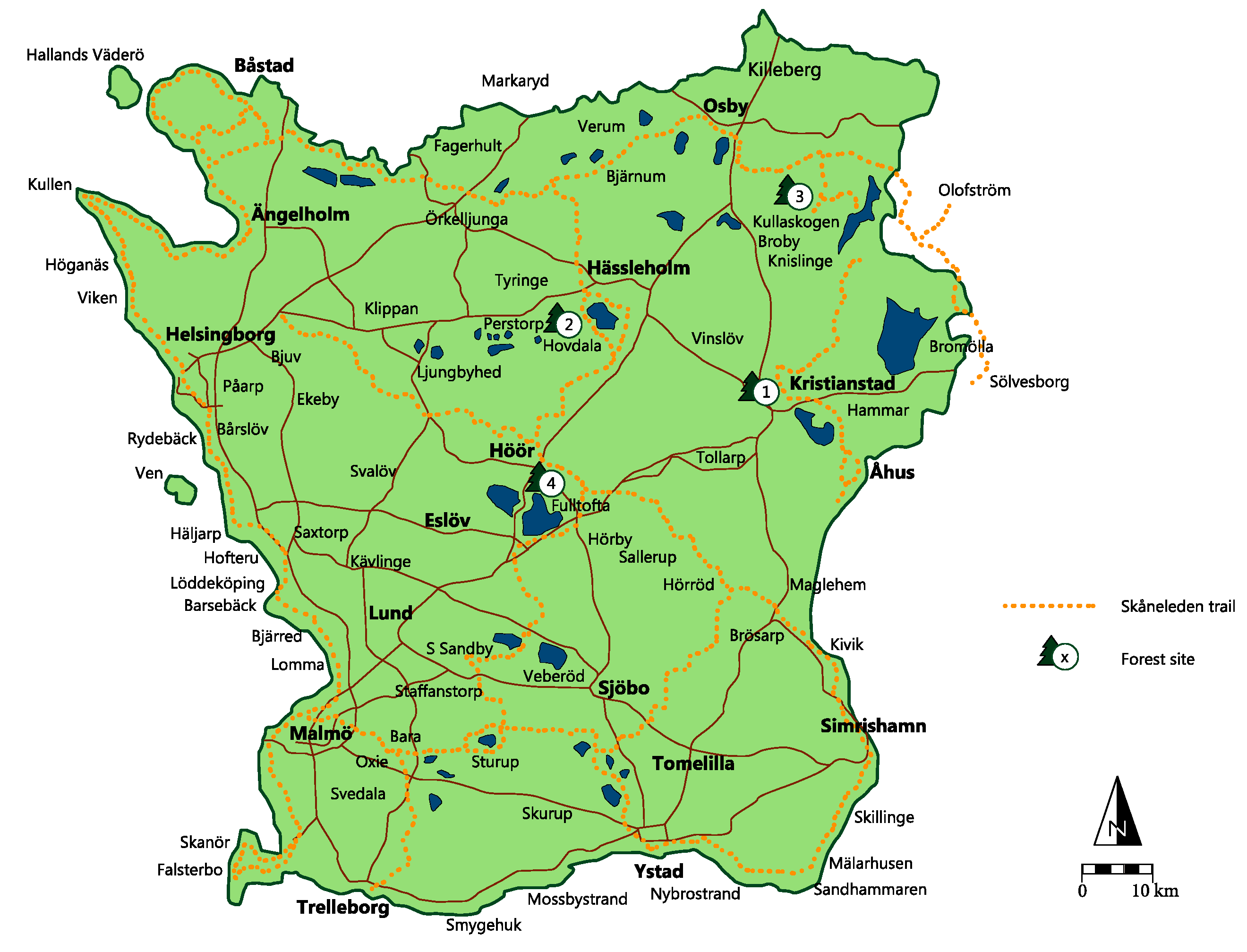
2.3. The Forest Sites/Venues
2.4. Outcome Measurements
2.5. Interviews
2.6. Perceived Sensory Dimensions (PSD)
2.7. Data Analysis
2.8. Ethical Considerations
3. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Armes, J.; Crowe, M.; Colbourne, L.; Morgan, H.; Murrells, T.; Oakley, C.; Palmer, N.; Ream, E.; Young, A.; Richardson, A. Patients’ Supportive Care Needs Beyond the End of Cancer Treatment: A Prospective, Longitudinal Survey. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2009, 27, 6172–6179. [Google Scholar] [CrossRef]
- Corner, J. Addressing the needs of cancer survivors: Issues and challenges. Expert Rev. Pharm. Outcomes Res. 2008, 8, 443–451. [Google Scholar] [CrossRef] [PubMed]
- Nationellt Vårdprogram Livmoderkroppscancer—RCC Kunskapsbanken. Available online: https://kunskapsbanken.cancercentrum.se/diagnoser/livmoderkroppscancer/vardprogram/ (accessed on 10 September 2022).
- Nationellt Vårdprogram Äggstockscancer, Epitelial—RCC Kunskapsbanken. Available online: https://kunskapsbanken.cancercentrum.se/diagnoser/aggstockscancer-epitelial/vardprogram/ (accessed on 10 September 2022).
- Beesley, V.L.; Price, M.A.; Webb, P.M.; O’Rourke, P.; Marquart, L.; Group AOCS; Australian Ovarian Cancer Study—Quality of Life Study Investigators; Phyllis N Butow. Changes in supportive care needs after first-line treatment for ovarian cancer: Identifying care priorities and risk factors for future unmet needs. Psycho Oncol. 2013, 22, 1565–1571. [Google Scholar] [CrossRef] [PubMed]
- Dobilas, A.; Moberg, L.; Borgfeldt, C. Areas to Improve Quality of Life after Ovarian Tumor Surgery and Adjuvant Treatment. Vivo 2021, 35, 2399–2408. [Google Scholar] [CrossRef] [PubMed]
- Stavraka, C.; Ford, A.; Ghaem-Maghami, S.; Crook, T.; Agarwal, R.; Gabra, H.; Blagden, S. A study of symptoms described by ovarian cancer survivors. Gynecol. Oncol. 2012, 125, 59–64. [Google Scholar] [CrossRef]
- Nord, C.; Mykletun, A.; Thorsen, L.; Bjoro, T.; Fåsso, S. Self-reported health and use of health care services in long-term cancer survivors. Int. J. Cancer 2005, 2, 307–316. [Google Scholar] [CrossRef]
- Regionala Cancercentrum i samverkan. Nationellt Vårdprogram Cancerrehabilitering. RCC. 2014. Available online: https://kunskapsbanken.cancercentrum.se/diagnoser/cancerrehabilitering/vardprogram/ (accessed on 10 September 2022).
- Gerber, L.H.; Hodsdon, B.; Comis, L.E.; Chan, L.; Gallin, J.I.; McGarvey, C.L., III. A Brief Historical Perspective of Cancer Rehabilitation and Contributions from the National Institutes of Health. PM&R 2017, 9, S297–S304. [Google Scholar] [CrossRef]
- Wigzell, O. Cancerrehabilitering. Förslag till utveckling. Socialstyrelsen 2022, 2022-5-7936. Available online: https://www.socialstyrelsen.se/globalassets/sharepoint-dokument/artikelkatalog/ovrigt/2022-5-7936.pdf (accessed on 10 September 2022).
- Digitala Lösningar Kan ge Fler Tillgång Till Cancerrehabilitering [Digital Solutions Can Provide More Access to Cancer Rehabilitation]. Available online: https://www.dagensmedicin.se/opinion/debatt/digitala-losningar-kan-ge-fler-tillgang-till-cancerrehabilitering/ (accessed on 4 February 2022).
- Harper, N.; Rose, K.; Segal, D. (Eds.) An introduction to nature for therapy. In Nature-Based Therapy. Practitioner´s Guide to Working Outdoors with Children, Youth and Families; New Society Publisher: Gabriola Island, BC, Canada, 2019; pp. 1–21. [Google Scholar]
- Corazon, S.S.; Stigsdotter, U.K.; Jensen, A.G.C.; Nilsson, K. Development of the nature-based therapy concept for patients with stress-related illness at the Danish healing forest garden Nacadia. J. Ther. Hortic. 2010, 20, 34–50. [Google Scholar] [CrossRef]
- Kristjánsdóttir, H.L.; Sigurðardóttir, S.; Pálsdóttir, A.M. The Restorative Potential of Icelandic Nature. Int. J. Environ. Res. Public Health 2020, 17, 9095. [Google Scholar] [CrossRef]
- Vujcic, M.; Tomicevic-Dubljevic, J.; Grbic, M.; Lecic-Tosevski, D.; Vukovic, O.; Toskovic, O. Nature based solution for improving mental health and well-being in urban areas. Environ. Res. 2017, 158, 385–392. [Google Scholar] [CrossRef]
- Christiana, R.W.; Besenyi, G.M.; Gustat, J.; Horton, T.H.; Schultz, C.L. A scoping review of the health benefits of nature-based physical activity. J. Healthy Eat. Act. Living 2021, 3, 127–160. [Google Scholar] [CrossRef]
- Shanahan, D.F.; Astell–Burt, T.; Barber, E.A.; Brymer, E.; Cox, D.T.C.; Dean, J.; Depledge, M.; Fuller, R.A.; Hartig, T.; Irvine, K.N.; et al. Nature—Based Interventions for Improving Health and Wellbeing: The Purpose, the People and the Outcomes. Sports 2019, 7, 141. [Google Scholar] [CrossRef] [PubMed]
- Ray, H.; Jakubec, S.L. Nature-based experiences and health of cancer survivors. Complement. Ther. Clin. Pract. 2014, 20, 188–192. [Google Scholar] [CrossRef] [PubMed]
- Ahmadi, F.; Ahmadi, N. Nature as the Most Important Coping Strategy among Cancer Patients: A Swedish Survey. J. Relig. Health 2015, 54, 1177–1190. [Google Scholar] [CrossRef]
- Heród, A.; Szewcyk-Taranek, B.; Pálsdóttir, A.M. Nature-Based Interventions in the Forest Environment: A Review. LTV-Fak. Faktabl. SLU Alnarp 2022, 7, 1–4. Available online: https://publications.slu.se/ (accessed on 4 February 2022).
- Lee, M.; Park, B. Effects of Forest Healing Program on Depression, Stress and Cortisol Changes of Cancer Patients. J. People Plants Environ. 2020, 23, 245–254. [Google Scholar] [CrossRef]
- Nakau, M.; Imanishi, J.; Imanishi, J.; Watanabe, S.; Imanishi, A.; Baba, T.; Hirai, K.; Ito, T.; Chiba, W.; Morimoto, Y. Spiritual Care of Cancer Patients by Integrated Medicine in Urban Green Space: A Pilot Study. Explore 2013, 9, 87–90. [Google Scholar] [CrossRef]
- Hansen, M.M.; Jones, R.; Tocchini, K. Shinrin-Yoku (Forest Bathing) and Nature Therapy: A State-of-the-Art Review. Int. J. Environ. Res. Public Health 2017, 14, 851. [Google Scholar] [CrossRef]
- Clarke, F.J.; Kotera, Y.; McEwan, K. A Qualitative Study Comparing Mindfulness and Shinrin-Yoku (Forest Bathing): Practitioners’ Perspectives. Sustainability 2021, 13, 6761. [Google Scholar] [CrossRef]
- Antonelli, M.; Donelli, D.; Carlone, L.; Maggini, V.; Firenzuoli, F.; Bedeschi, E. Effects of forest bathing [shinrin-yoku] on individual well-being: An umbrella review. Int. J. Environ. Health Res. 2022, 32, 1842–1867. [Google Scholar] [CrossRef]
- Muro, A.; Feliu-Soler, A.; Canals, J.; Parrado, E.; Sanz, A. Psychological benefits of Forest Bathing during the COVID-19 pandemic: A pilot study in a Mediterranean forest close to urban areas. J. For. Res. 2022, 27, 71–75. [Google Scholar] [CrossRef]
- Wen, Y.; Yan, Q.; Pan, Y.; Gu, X.; Liu, Y. Medical empirical research on forest bathing [Shinrin-yoku]: A systematic review. Environ. Health Prev. Med. 2019, 24, 70. [Google Scholar] [CrossRef]
- Li, Q.; Kobayashi, M.; Kumeda, S.; Ochiai, T.; Miura, T.; Kagawa, T.; Imai, M.; Wang, Z.; Otsuka, T.; Kawada, T. Effects of forest bathing on cardiovascular and metabolic parameters in middle-aged males. Evid. Based Complement. Altern. Med. 2016, 2016, 2587381. [Google Scholar] [CrossRef]
- Qing, L. Effects of forest environment (Shinrin-yoku/Forest bathing) on health promotion and disease prevention—The Establishment of ‘Forest Medicine’. Environ. Health Prev. Med. 2022, 27, 43. [Google Scholar] [CrossRef]
- Lee, K.H.; Son, Y.H.; Kim, S.; Lee, D.K. Healing experiences of middle-aged women through an urban forest therapy program. Urban For. Urban Green. 2019, 38, 383–391. [Google Scholar] [CrossRef]
- Sonntag-Öström, E.; Stenlund, T.; Nordin, M.; Lundell, Y.; Ahlgren, C.; Fjellman-Wiklund, A.; Järvholm, L.S.; Dolling, A. Nature’s effect on my mind”—Patients qualitative experiences of a forest-based rehabilitation programme. Urban For. Urban Green. 2015, 14, 607–614. [Google Scholar] [CrossRef]
- Li, K.; Morimotoi, K.; Nakadai, A.; Inagaki, H.; Katsumata, M.; Shimizu, T.; Hirata, Y.; Hirata, K.; Suzuki, H.; Miyazakf, Y.; et al. Forest bathing enhances human natural killer activity and expression of anti-cancer proteins. Int. J. Immunopathol. Pharmacol. 2007, 20, 3–8. [Google Scholar] [CrossRef] [PubMed]
- Høegmark, S.; Elmose Andersen, T.; Grahn, P.; Kaya Roessler, K. The Wildman Programme. A Nature-Based Rehabilitation Programme Enhancing Quality of Life for Men on Long-Term Sick Leave: Study Protocol for a Matched Controlled Study in Denmark. Int. J. Environ. Res. Public Health 2020, 1710, 3368. [Google Scholar] [CrossRef]
- Sonntag-Öström, E.; Nordin, M.; Dolling, A.; Lundell, Y.; Nilsson, L.; Slunga Järvholm, L. Can rehabilitation in boreal forest help recovery from exhaustion disorder?—The randomized clinical trial ForRest. Scand. J. For. Res. 2015, 30, 732–748. [Google Scholar] [CrossRef]
- Hillman, H.C.; Erickson, K.I.; Kramer, A.F. Be smart, exercise your heart: Exercise effects on your brain and cognition. Nat. Rev. Neurosci. 2008, 9, 58–65. [Google Scholar] [CrossRef] [PubMed]
- Dahlin, E.; Nyberg, L.; Backman, L.; Neely, A.S. Plasticity of executive functioning in young and older adults: Immediate training gains, transfer, and long-term maintenance. Psychol. Aging 2008, 23, 720–730. [Google Scholar] [CrossRef]
- Fayers, P.; Bottomley, A. Quality of life research within the EORTC—The EORTC QLQ-C30. Eur. J. Cancer 2002, 38, S125–S133. [Google Scholar] [CrossRef]
- Weis, J.; Tomaszewski, K.A.; Hammerlid, E.; Ignacio Arraras, J.; Conroy, T.; Lanceley, A.; Schmidt, H.; Wirtz, M.; Singer, S.; Pinto, M.; et al. International Psychometric Validation of an EORTC Quality of Life Module Measuring Cancer Related Fatigue (EORTC QLQ-FA12). JNCI J. Natl. Cancer Inst. 2017, 109. [Google Scholar] [CrossRef] [PubMed]
- Zigmond, A.S.; Snaith, R.P. The Hospital Anxiety and Depression Scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef]
- SBU—Statens Beredning för Medicinsk Utvärdering. Behandling av Depressionssjukdomar: En Systematisk Litteraturöversikt: Sammanfattning av SBU:s Rapport. [SBU—The State’s Preparation for Medical Evaluation. Treatment of Depressive Disorders: A Systematic Literature Review: Summary of SBU’s Report]; SBU—Statens Beredning för Medicinsk Utvärdering: Stockholm, Sweden, 2004; Available online: https://www.sbu.se/contentassets/00f42eab171e4ab699292a6bb6db920c/depression-vol-1.pdf (accessed on 10 September 2022).
- McNair, D.M.; Lorr, M.; Droppleman, L.F. Manual for the Profile of Mood States [POMS]; Educational and Industrial Testing Service: San Diego, CA, USA, 1971. [Google Scholar]
- Zuckerman, M. Development of a situation-specific trait-state test for the prediction and measurement of affective responses. J. Consul. Clin. Psychol. 1977, 45, 513–523. [Google Scholar] [CrossRef] [PubMed]
- Sonntag-Öström, E.; Nordin, M.; Slunga Järvholm, L.; Lundell, Y.; Brännström, R.; Dolling, A. Can the boreal forest be used for rehabilitation and recovery from stress-related exhaustion?—A pilot study. Scand. J. For. Res. 2011, 26, 245–256. [Google Scholar] [CrossRef]
- Pálsdóttir, A.M.; Stigsdotter, U.; Persson, D.; Thorpert, P.; Grahn, P. The qualities of natural environments that support the rehabilitation process of individuals with stress-related mental disorder in nature-based rehabilitation. Urban For. Urban Green. 2018, 29, 312–321. [Google Scholar] [CrossRef]
- Stoltz, J.; Grahn, P. Perceived sensory dimensions: An evidence-based approach to greenspace aesthetics. Urban For. Urban Green. 2021, 59, 126989. [Google Scholar] [CrossRef]
- Smith, J.A.; Flowers, P.; Larkin, M. Interpretative Phenomenological Analysis: Theory, Method and Research; SAGE Publications Ltd.: London, UK, 2009. [Google Scholar] [CrossRef]






Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Anundi, H.; Dolling, A.; Pálsdóttir, A.M. Forest Therapy for Women with Gynaecological Cancer—A Feasibility Study to Find New Alternatives in Cancer Rehabilitation. Forests 2023, 14, 333. https://doi.org/10.3390/f14020333
Anundi H, Dolling A, Pálsdóttir AM. Forest Therapy for Women with Gynaecological Cancer—A Feasibility Study to Find New Alternatives in Cancer Rehabilitation. Forests. 2023; 14(2):333. https://doi.org/10.3390/f14020333
Chicago/Turabian StyleAnundi, Hanna, Ann Dolling, and Anna María Pálsdóttir. 2023. "Forest Therapy for Women with Gynaecological Cancer—A Feasibility Study to Find New Alternatives in Cancer Rehabilitation" Forests 14, no. 2: 333. https://doi.org/10.3390/f14020333
APA StyleAnundi, H., Dolling, A., & Pálsdóttir, A. M. (2023). Forest Therapy for Women with Gynaecological Cancer—A Feasibility Study to Find New Alternatives in Cancer Rehabilitation. Forests, 14(2), 333. https://doi.org/10.3390/f14020333