The Mechanism of Onychomadesis (Nail Shedding) and Beau’s Lines Following Hand-Foot-Mouth Disease

 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Clinical Sample Preparation
2.2. Viral Culture and Virus DNA Detection in Clinical Samples
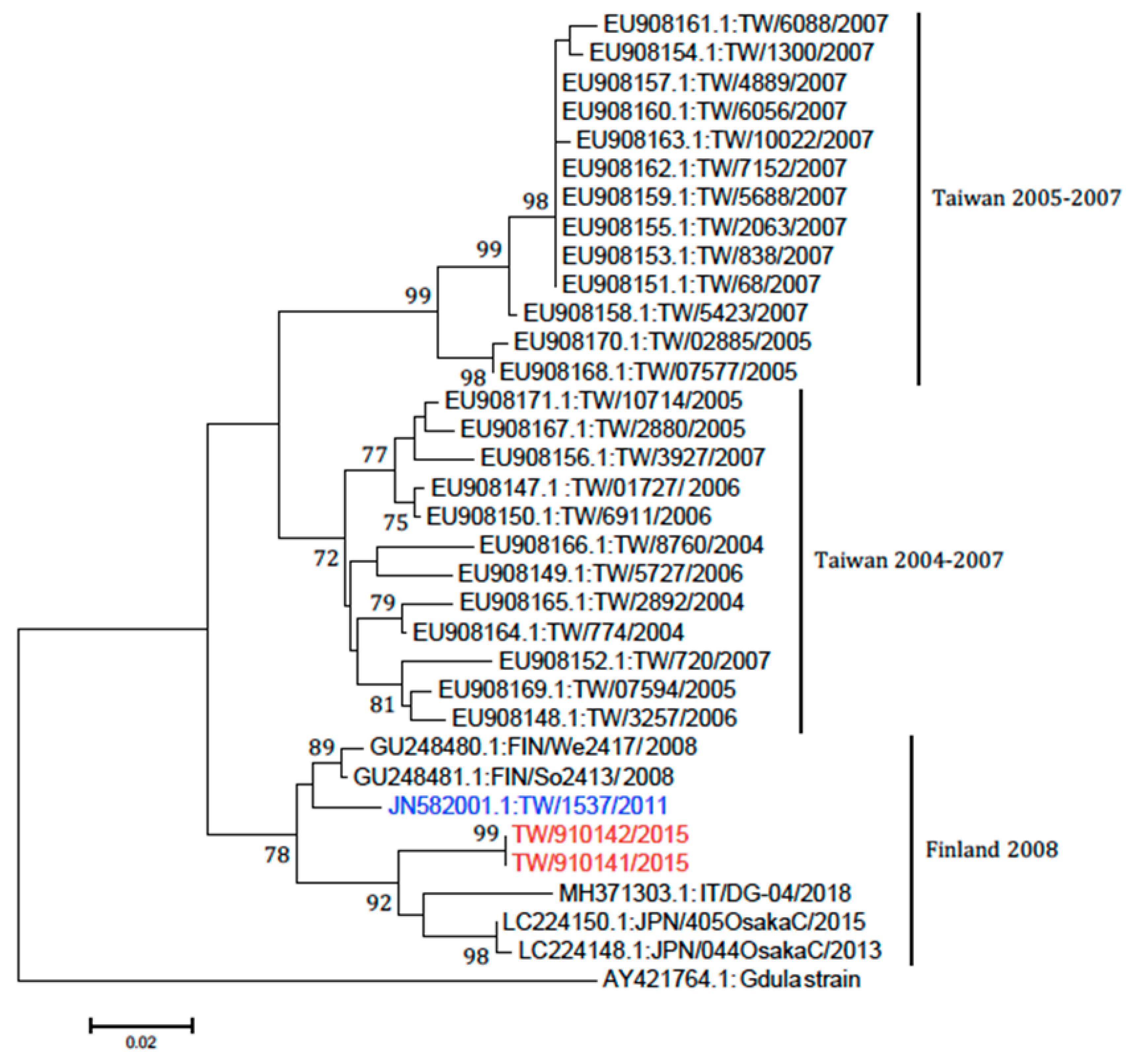
2.3. Phylogenetic Analysis
3. Result
4. Discussion
Supplementary Materials
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Clementz, G.C.; Mancini, A.J. Nail matrix arrest following hand-foot-mouth disease: A report of five children. Pediatr. Dermatol. 2000, 17, 7–11. [Google Scholar] [CrossRef] [PubMed]
- Bernier, V.; Labrèze, C.; Bury, F.; Taïeb, A. Nail matrix arrest in the course of hand, foot and mouth disease. Eur. J. Pediatr. 2001, 160, 649–651. [Google Scholar] [CrossRef] [PubMed]
- Chiu, H.H.; Wu, C.S.; Lan, C.E. Onychomadesis: A Late Complication of Hand, Foot, and Mouth Disease. J. Emerg. Med. 2017, 52, 243–245. [Google Scholar] [CrossRef] [PubMed]
- Hardin, J.; Haber, R.M. Onychomadesis: Literature review. Br. J. Dermatol. 2015, 172, 592–596. [Google Scholar] [CrossRef] [PubMed]
- Tamura, K.; Stecher, G.; Peterson, D.; Filipski, A.; Kumar, S. MEGA6: Molecular Evolutionary Genetics Analysis version 6.0. Mol. Biol. Evol. 2013, 30, 2725–2729. [Google Scholar] [CrossRef] [PubMed]
- Bonzel, L.; Tenenbaum, T.; Schroten, H.; Schildgen, O.; Schweitzer-Krantz, S.; Adams, O. Frequent detection of viral coinfection in children hospitalized with acute respiratory tract infection using a real-time polymerase chain reaction. Pediatr. Infect. Dis. J. 2008, 27, 589–594. [Google Scholar] [CrossRef] [PubMed]
- Oberste, M.S.; Maher, K.; Flemister, M.R.; Marchetti, G.; Kilpatrick, D.R.; Pallansch, M.A. Comparison of Classic and Molecular Approaches for the Identification of Untypeable Enteroviruses. J. Clin. Microbiol. 2000, 38, 1170–1174. [Google Scholar] [PubMed]
- Chung, W.H.; Shih, S.R.; Chang, C.F.; Lin, T.Y.; Huang, Y.C.; Chang, S.C.; Liu, M.T.; Ko, Y.S.; Deng, M.C.; Liau, Y.L.; et al. Clinicopathologic analysis of coxsackievirus a6 new variant induced widespread mucocutaneousbullous reactions mimicking severe cutaneous adverse reactions. J. Infect. Dis. 2013, 208, 1968–1978. [Google Scholar] [CrossRef] [PubMed]
- Chiu, H.H.; Lan, C.C.; Wu, C.S.; Kuo, K.C.; Chen, G.S.; Wei, K.C. Onychomadesis following hand-foot-and-mouth disease. Cutis 2016, 97, E20–E21. [Google Scholar] [PubMed]
- Shikuma, E.; Endo, Y.; Fujisawa, A.; Tanioka, M.; Miyachi, Y. Onychomadesis developed only on the nails having cutaneous lesions of severe hand–foot–mouth disease. Case Rep. Dermatol. Med. 2011, 2011, 324193. [Google Scholar] [CrossRef] [PubMed]
- Osterback, R.; Vuorinen, T.; Linna, M.; Susi, P.; Hyypiä, T.; Waris, M. Coxsackievirus A6 and hand, foot, and mouth disease, Finland. Emerg. Infect. Dis. 2009, 15, 1485–1488. [Google Scholar] [CrossRef] [PubMed]
- Wei, S.H.; Huang, Y.P.; Liu, M.C.; Tsou, T.P.; Lin, H.C.; Lin, T.L.; Tsai, C.Y.; Chao, Y.N.; Chang, L.Y.; Hsu, C.M. An outbreak of coxsackievirus A6 hand, foot, and mouth disease associated with onychomadesis in Taiwan, 2010. BMC Infect. Dis. 2011, 11, 346. [Google Scholar] [CrossRef] [PubMed]
- Kimmis, B.D.; Downing, C.; Tyring, S. Hand-foot-and-mouth disease caused by coxsackievirus A6 on the rise. Cutis 2018, 102, 353–356. [Google Scholar] [PubMed]
- Horsten, H.H.; Kemp, M.; Fischer, T.K.; Lindahl, K.H.; Bygum, A. Atypical Hand, Foot, and Mouth Disease Caused by Coxsackievirus A6 in Denmark: A Diagnostic Mimicker. Acta Derm. Venereol. 2018, 98, 350–354. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Case No. | Age/Sex | Interval after HFMD (days) | Nail Samples for PCR and Sequencing for HEV | Nail Samples for Virus Culture | Throat Swab for PCR and Sequencing for HEV | Throat Swab Sampling Date after HFMD Onset | Nail Samples for Transmission Electron Microscope |
|---|---|---|---|---|---|---|---|
| 1 | 3/F | 30 | (−) | ND | ND | ND | ND |
| 2 | 3/M | 50 | CVA6 | ND | ND | ND | ND |
| 3 | 4/M | 30 | (−) | ND | ND | ND | ND |
| 4 | 5/F | 30 | (−) | ND | ND | ND | ND |
| 5 | 15/M | 50 | (−) | ND | ND | ND | ND |
| 6 | 45/M | 60 | (−) | ND | ND | ND | ND |
| 7 | 30/F | 96 | (−) | ND | ND | ND | ND |
| 8 | 69/F | 60 | (−) | ND | ND | ND | ND |
| 9 | 1/F | 62 | CVA6 | (−) | CVA6 | 2nd day | ND |
| 10 | 31/M | 69 | CVA6 | (−) | CVA6 | 2nd day | viral particles (+) |
| 11 | 60/F | 50 | Echovirus | ND | Echovirus | 5th day | ND |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chiu, H.-H.; Liu, M.-T.; Chung, W.-H.; Ko, Y.-S.; Lu, C.-F.; Lan, C.-C.E.; Lu, C.-W.; Wei, K.-C. The Mechanism of Onychomadesis (Nail Shedding) and Beau’s Lines Following Hand-Foot-Mouth Disease. Viruses 2019, 11, 522. https://doi.org/10.3390/v11060522
Chiu H-H, Liu M-T, Chung W-H, Ko Y-S, Lu C-F, Lan C-CE, Lu C-W, Wei K-C. The Mechanism of Onychomadesis (Nail Shedding) and Beau’s Lines Following Hand-Foot-Mouth Disease. Viruses. 2019; 11(6):522. https://doi.org/10.3390/v11060522
Chicago/Turabian StyleChiu, Hsiu-Hui, Ming-Tsan Liu, Wen-Hung Chung, Yu-Shien Ko, Chin-Fang Lu, Cheng-Che E. Lan, Chun-Wei Lu, and Kai-Che Wei. 2019. "The Mechanism of Onychomadesis (Nail Shedding) and Beau’s Lines Following Hand-Foot-Mouth Disease" Viruses 11, no. 6: 522. https://doi.org/10.3390/v11060522
APA StyleChiu, H. -H., Liu, M. -T., Chung, W. -H., Ko, Y. -S., Lu, C. -F., Lan, C. -C. E., Lu, C. -W., & Wei, K. -C. (2019). The Mechanism of Onychomadesis (Nail Shedding) and Beau’s Lines Following Hand-Foot-Mouth Disease. Viruses, 11(6), 522. https://doi.org/10.3390/v11060522