Examining the Association of Socioeconomic Position with Microcephaly and Delayed Childhood Neurodevelopment among Children with Prenatal Zika Virus Exposure

 ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
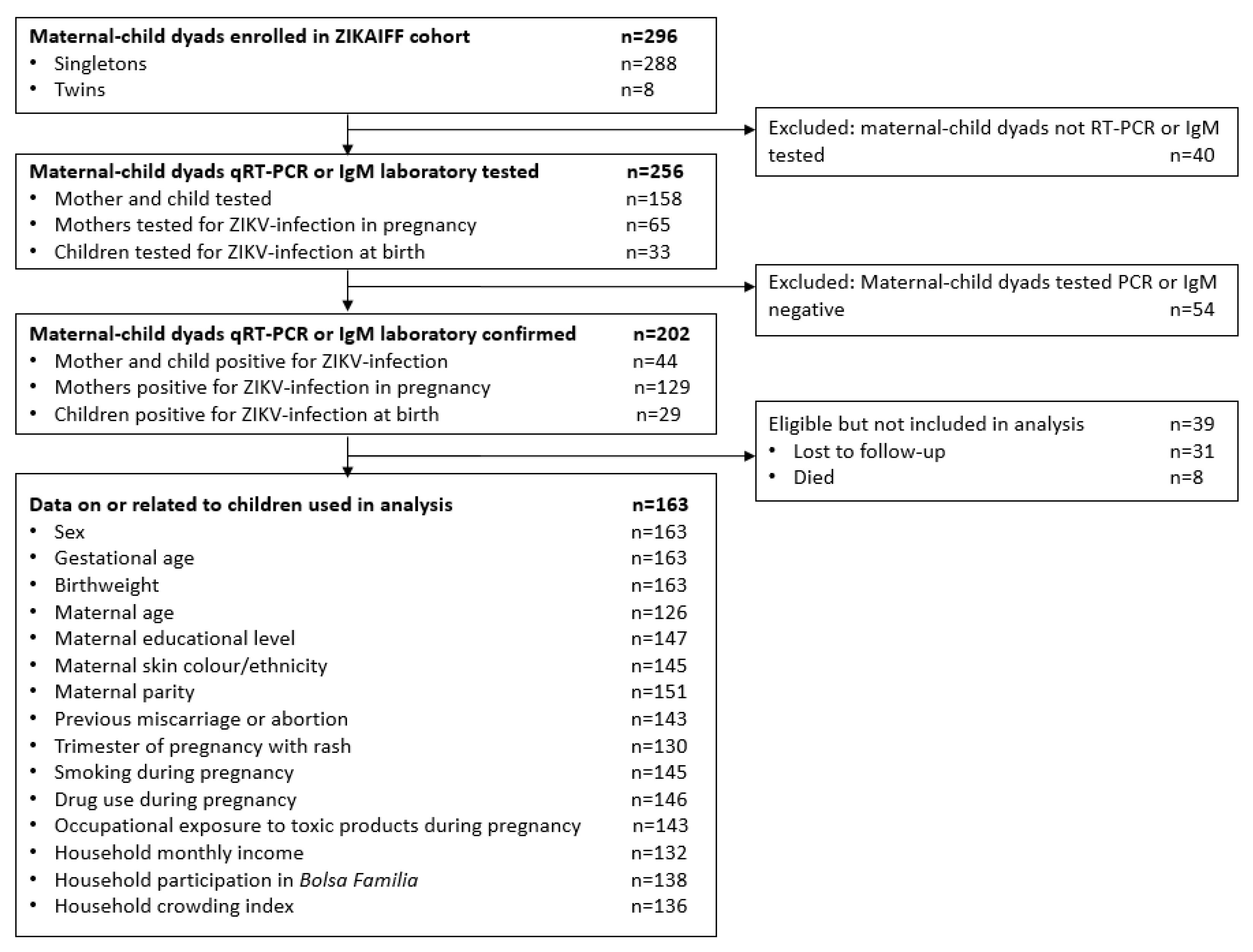
2.1. Study Population
2.2. Exposures
2.3. Outcomes
2.3.1. Infant Clinical Assessments
2.3.2. Neurological Evaluations
2.4. Additional Covariates
2.5. Data Cleaning and Missing Values
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Category | Total, No. | % Non-Missing Data | Cases with Complete Data No. (%) n = 83 | Cases with Missing Data No. (%) | p Value |
|---|---|---|---|---|---|---|
| Characteristics of children | ||||||
| Child sex | Female | 163 | 100% | 41 | 43 | 0.578 |
| Male | 42 | 37 | ||||
| Characteristics of mothers | ||||||
| Maternal educational level | Primary school, including partial | 147 | 90% | 16 | 6 | 0.119 |
| Secondary school, including partial | 38 | 39 | ||||
| Higher education, including partial | 29 | 10 | ||||
| Maternal race/ethnicity | White Brazilian and East Asian Brazilian | 145 | 89% | 34 | 22 | 0.645 |
| Mixed-race Afro-Brazilian | 35 | 31 | ||||
| Black Afro-Brazilian | 14 | 9 | ||||
| Maternal parity | ≤1 | 151 | 93% | 41 | 40 | 0.291 |
| 2 | 32 | 18 | ||||
| 3+ | 10 | 10 | ||||
| Previous miscarriage or abortion | No | 143 | 88% | 69 | 48 | 0.632 |
| Yes | 14 | 12 | ||||
| Trimester of pregnancy with rash | First | 130 | 80% | 39 | 17 | 0.443 |
| Second | 30 | 19 | ||||
| Third | 14 | 11 | ||||
| Did the mother smoke during pregnancy | No | 145 | 89% | 79 | 60 | 0.634 |
| Yes | 4 | 2 | ||||
| Did the mother use drugs during pregnancy | No | 146 | 90% | 80 | 58 | 0.256 |
| Yes | 3 | 5 | ||||
| Occupational exposure to toxic products during pregnancy | No | 143 | 88% | 65 | 46 | 0.816 |
| Yes | 18 | 14 | ||||
| Characteristics of household | ||||||
| Household monthly income (relative to minimum wage of BRL998) | Class A: >20× minimum wage | 132 | 81% | 38 | 29 | 0.684 |
| Class B: 10–20× minimum wage | 5 | 2 | ||||
| Class C: 4–10× minimum wage | 12 | 6 | ||||
| Class D: 2–4× minimum wage | 26 | 12 | ||||
| Class E: <2× minimum wage | 38 | 29 | ||||
| Household participation in Bolsa Família (government cash transfer scheme) | No | 138 | 85% | 67 | 61 | 0.513 |
| Yes | 16 | 11 | ||||
| Household crowding index (individuals in the house / rooms in the house) | <0.5 | 136 | 83% | 23 | 15 | 0.584 |
| 0.5–0.75 | 25 | 21 | ||||
| 0.75–1.0 | 23 | 10 | ||||
| 1.0+ | 12 | 7 | ||||
Appendix B
| Variable | Category | Adjusted Odds Ratio (95% CI) | p Value * |
|---|---|---|---|
| Maternal educational level a n = 240 | Primary school, including partial | 1 | <0.001 |
| Secondary school, including partial | 0.71 (0.33, 1.54) | ||
| Higher education, including partial | 0.22 (0.09, 0.55) | ||
| Maternal race/ethnicity b n = 212 | White Brazilians and East Asian Brazilians | 1 | 0.526 |
| Mixed-race Afro-Brazilians | 0.83 (0.34, 1.99) | ||
| Black Afro-Brazilians | 0.67 (0.34, 1.35) | ||
| Household monthly income (relative to minimum wage) c n = 204 | Classes A, B, C and D: >2× min wage | 1 | 0.004 |
| Class E: <2× min wage | 2.71 (1.36, 5.43) | ||
| Household participation in Bolsa Família (government cash transfer) scheme d n = 224 | No | 1 | 0.371 |
| Yes | 1.35 (0.70, 2.62) | ||
| Household crowding index (individuals in the house/rooms in the house) e n = 207 | Linear trend across four household crowding index groups (<0.5, 0.5–0.75, 0.75–1.0, 1.0+) | 1.48 (1.06, 2.09) | 0.021 |
Appendix C
| Variable | Category | No. (Col %) of Children Taking Bayley-III Tests | Unadjusted Estimated Difference in Language Scores (95% CI) | p Value */** | Unadjusted Estimated Difference in Motor Scores (95% CI) | p Value */** | Unadjusted Estimated Difference in Cognitive Scores (95% CI) | p Value */** |
|---|---|---|---|---|---|---|---|---|
| Characteristics of children | ||||||||
| Sex | Female | 57 (50.9%) | (Reference) | 0.429 | (Reference) | 0.937 | (Reference) | 0.752 |
| Male | 55 (49.1%) | −1.97 (−6.90, 2.96) | −0.19 (−4.84, 4.47) | 0.81 (−4.28, 5.90) | ||||
| Characteristics of mother | ||||||||
| Educational level | Primary school, including partial | 9 (8.0) | (Reference) | 0.459 | (Reference) | 0.94 | (Reference) | 0.139 |
| Secondary school, including partial | 50 (44.6%) | 2.34 (−7.00, 11.69) | −0.87 (−9.84, 8.10) | −3.63 (−12.92, 5.65) | ||||
| Higher education, including partial | 41 (36.6%) | 5.03 (−4.47, 14.53) | 0.01 (−9.11, 9.13) | 1.79 (−7.65, 11.23) | ||||
| Missing | 12 (10.7%) | |||||||
| Race/ethnicity | White Brazilians and East Asian Brazilians | 41 (36.6%) | (Reference) | 0.55 | (Reference) | 0.369 | (Reference) | 0.947 |
| Mixed-race Afro-Brazilians | 47 (42.0%) | −2.78 (−8.32, 2.77) | 3.67 (−1.62, 8.96) | 0.74 (−4.90, 6.38) | ||||
| Black Afro-Brazilians | 10 (8.9%) | −3.51 (−12.67, 5.64) | 3.42 (−5.31, 12.15) | 1.29 (−8.−1, 10.60) | ||||
| Missing | 14 (12.5%) | |||||||
| Parity | ≤1 | 57 (50.9%) | (Reference) | 0.211 | (Reference) | 0.007 | (Reference) | 0.566 |
| 2 | 34 (30.4%) | 0.66 (−4.97, 6.30) | −7.32 (−12.49, −2.16) | 0.93 (−4.92, 6.77) | ||||
| 3+ | 13 (11.6%) | 7.10 (−0.89, 15.10) | 3.04 (−4.28, 10.37) | 4.47 (−3.82, 12.76) | ||||
| Missing | 8 (7.1%) | |||||||
| Previous miscarriage or abortion | No | 80 (71.4%) | (Reference) | 0.62 | (Reference) | 0.552 | [Reference) | 0.932 |
| Yes | 16 (14.3%) | 1.76 (−5.27, 8.79) | −2.04 (−8.81, 4.74) | −0.31 (−7.56, 6.93) | ||||
| Missing | 16 (14.3%) | |||||||
| Trimester of pregnancy with rash | First | 25 (22.3%) | (Reference) | 0.138 | (Reference) | 0.037 | (Reference) | 0.523 |
| Second | 46 (41.1%) | −0.30 (−6.81, 6.21) | −6.25 (−12.26, −0.23) | −0.39 (−6.94, 6.16) | ||||
| Third | 23 (20.5%) | −6.56 (−14.13, 1.01) | −8.72 (−15.71, −1.73) | −3.87 (−11.48, 3.75) | ||||
| Missing | 18 (16.1%) | |||||||
| Smoke during pregnancy | No | 96 (85.0%) | (Reference) | 1 | (Reference) | −0.409 | (Reference) | 0.944 |
| Yes | 3 (2.7%) | 0.00 (−15.21, 15.22) | −5.63 (−19.12, 7.86) | −0.54 (−15.87, 14.79) | ||||
| Missing | 14 (12.4%) | |||||||
| Drug use during pregnancy | No | 95 (84.8%) | (Reference) | 0.121 | (Reference) | 0.797 | (Reference) | 0.818 |
| Yes | 3 (2.7%) | −9.30 (−21.09, 2.49) | 1.47 (−9.86, 12.81) | −1.39 (−13.38, 10.60) | ||||
| Missing | 14 (12.5%) | |||||||
| Occupational exposure to toxic products during pregnancy | No | 74 (66.1%) | (Reference) | 0.735 | (Reference) | 0.404 | (Reference) | 0.611 |
| Yes | 22 (19.6%) | 1.09 (−5.26, 7.44) | 2.54 (−3.49, 8.57) | 1.65 (−4.78, 8.09) | ||||
| Missing | 16 (14.3%) | |||||||
| Characteristics of household | ||||||||
| Monthly income (relative to minimum wage) | Classes A, B, C and D: > 2× min wage | 56 (50.0%) | (Reference) | 0.169 | (Reference) | 0.895 | (Reference) | 0.460 |
| Class E: < 2× Min wage | 35 (31.3%) | −4.03 (−9.79, 1.74) | −0.36 (−5.84, 5.12) | −2.16 (−7.95, 3.63) | ||||
| Missing | 21 (18.8%) | |||||||
| Participation in Bolsa Família | No | 78 (69.6%) | (Reference) | 0.078 | (Reference) | 0.039 | (Reference) | 0.019 |
| Yes | 13 (11.6%) | −7.05 (−14.92, 0.81) | −7.79 (−15.20, −0.39) | −9.42 (−17.23, −1.61) | ||||
| Missing | 21 (18.8%) | |||||||
| Household crowding index | <0.5 | 31 (27.7%) | (Reference) | 0.76 | (Reference) | 0.212 | (Reference) | 0.280 |
| 0.5–0.75 | 33 (29.5%) | −0.74 (−7.33, 5.85) | 5.17 (−0.99, 11.34) | 5.97 (−0.66, 12.59) | ||||
| 0.75–1.0 | 20 (17.9%) | −0.34 (−7.90, 7.22) | 0.94 (−6.13, 8.00) | 3.72 (−3.88, 11.31) | ||||
| 1.0+ | 8 (7.1%) | −5.57 (−16.02, 4.89) | 7.89 (−1.88, 17.65) | 7.22 (−3.29, 17.72) | ||||
| Missing | 20 (17.8%) | |||||||
References
- Platt, D.J.; Smith, A.M.; Arora, N.; Diamond, M.S.; Coyne, C.B.; Miner, J.J. Zika virus-related neurotropic flaviviruses infect human placental explants and cause fetal demise in mice. Sci. Transl. Med. 2018, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grant-Klein, R.J.; Baldwin, C.D.; Turell, M.J.; Rossi, C.A.; Li, F.; Lovari, R.; Crowder, C.D.; Matthews, H.E.; Rounds, M.A.; Eshoo, M.W.; et al. Rapid identification of vector-borne flaviviruses by mass spectrometry. Mol. Cell. Probes 2010, 24, 219–228. [Google Scholar] [CrossRef] [PubMed]
- Ritchie, S. Dengue Vector Bionomics: Why is Aedes aegypti such a good vector. In Dengue and Dengue Hemorrhagic Fever; CABI: Oxford, UK, 2014. [Google Scholar]
- Soares, F.; Abranches, A.D.; Villela, L.; Lara, S.; Araújo, D.; Nehab, S.; Silva, L.; Amaral, Y.; Junior, S.C.G.; Pone, S.; et al. Zika virus infection in pregnancy and infant growth, body composition in the first three months of life: A cohort study. Sci. Rep. 2019, 9, 19198. [Google Scholar] [CrossRef] [PubMed]
- Souza, W.V.; Albuquerque, M.; Vazquez, E.; Bezerra, L.C.A.; Mendes, A.; Lyra, T.M.; Araujo, T.V.B.; Oliveira, A.L.S.; Braga, M.C.; Ximenes, R.A.A.; et al. Microcephaly epidemic related to the Zika virus and living conditions in Recife, Northeast Brazil. BMC Public Health 2018, 18, 130. [Google Scholar] [CrossRef]
- Netto, E.M.; Moreira-Soto, A.; Pedroso, C.; Höser, C.; Funk, S.; Kucharski, A.J.; Rockstroh, A.; Kümmerer, B.M.; Sampaio, G.S.; Luz, E.; et al. High Zika Virus Seroprevalence in Salvador, Northeastern Brazil Limits the Potential for Further Outbreaks. mBio 2017, 8, e01390-17. [Google Scholar] [CrossRef] [Green Version]
- Goldfeld, S.; O’Connor, M.; Cloney, D.; Gray, S.; Redmond, G.; Badland, H.; Williams, K.; Mensah, F.; Woolfenden, S.; Kvalsvig, A.; et al. Understanding child disadvantage from a social determinants perspective. J. Epidemiol. Community Health 2018, 72, 223. [Google Scholar] [CrossRef] [Green Version]
- Alderman, H.; Behrman, J.R.; Glewwe, P.; Fernald, L.; Walker, S. Evidence of Impact of Interventions on Growth and Development during Early and Middle Childhood. In Child and Adolescent Health and Development; Bundy, D.A.P., Silva, N., Horton, S., Jamison, D.T., Patton, G.C., Eds.; The International Bank for Reconstruction and Development/The World Bank: Washington, DC, USA, 2017; pp. 79–98. [Google Scholar]
- Brasil, P.; Pereira, J.P.; Moreira, M.E.; Ribeiro Nogueira, R.M.; Damasceno, L.; Wakimoto, M.; Rabello, R.S.; Valderramos, S.G.; Halai, U.-A.; Salles, T.S.; et al. Zika Virus Infection in Pregnant Women in Rio de Janeiro. N. Engl. J. Med. 2016, 375, 2321–2334. [Google Scholar] [CrossRef]
- Corman, V.M.; Rasche, A.; Baronti, C.; Aldabbagh, S.; Cadar, D.; Reusken, C.B.; Pas, S.D.; Goorhuis, A.; Schinkel, J.; Molenkamp, R.; et al. Assay optimization for molecular detection of Zika virus. Bull. World Health Organ. 2016, 94, 880–892. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Zika MAC-ELISA: Intructions for Use. Available online: https://www.cdc.gov/zika/pdfs/zika-mac-elisa-instructions-for-use.pdf (accessed on 7 April 2020).
- The Global Health Network (TGHN). INTERGROWTH-21st Global Perinatal Package: The International Fetal and Newborn Growth Consortium for the 21st Century. Available online: https://intergrowth21.tghn.org/ (accessed on 7 April 2020).
- Alves, L.V.; Paredes, C.E.; Silva, G.C.; Mello, J.G.; Alves, J.G. Neurodevelopment of 24 children born in Brazil with congenital Zika syndrome in 2015: A case series study. BMJ Open 2018, 8, e021304. [Google Scholar] [CrossRef] [Green Version]
- Silva, P.F.S.; Eickmann, S.H.; Ximenes, R.A.d.A.; Montarroyos, U.R.; Lima, M.d.C.; Martelli, C.T.; Araújo, T.V.B.d.; Brickley, E.; Rodrigues, L.C.; Gonçalves, F.C.L.P.; et al. Pediatric neurodevelopment by prenatal Zika virus exposure: A cross-sectional study of the Microcephaly Epidemic Research Group Cohort. BMC Pediatr. 2020, 20, 472. [Google Scholar]
- Madaschi, V.; Mecca, T.P.; Macedo, E.C.; Paula, C.S. Bayley-III Scales of Infant and Toddler Development: Transcultural Adaptation and Psychometric Properties. Paidéia 2016, 26, 189–197. [Google Scholar] [CrossRef] [Green Version]
- Bayley, N. Bayley Scales of Infant and Toddler Development: Administration Manual, 3rd ed.; Psychorp: San Antonio, TX, USA, 2005. [Google Scholar]
- Victora, C.G.; Huttly, S.R.; Fuchs, S.C.; Olinto, M.T. The role of conceptual frameworks in epidemiological analysis: A hierarchical approach. Int. J. Epidemiol. 1997, 26, 224–227. [Google Scholar] [CrossRef] [Green Version]
- Brazil, F.G.O. Bolsa Família Program: A Decade of Social Inclusion in Brazil. Executive Summary; Institute for Applied Economic Research: Brasília, Brazil, 2014. [Google Scholar]
- Ross, E.J.; Graham, D.L.; Money, K.M.; Stanwood, G.D. Developmental Consequences of Fetal Exposure to Drugs: What We Know and What We Still Must Learn. Neuropsychopharmacology 2015, 40, 61–87. [Google Scholar] [CrossRef]
- Campos, M.C.; Dombrowski, J.G.; Phelan, J.; Marinho, C.R.F.; Hibberd, M.; Clark, T.G.; Campino, S. Zika might not be acting alone: Using an ecological study approach to investigate potential co-acting risk factors for an unusual pattern of microcephaly in Brazil. PLoS ONE 2018, 13, e0201452. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marmot, M. Closing the health gap. Scand. J. Public Health 2017, 45, 723–731. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuh, D.; Ben-Shlomo, Y.; Lynch, J.; Hallqvist, J.; Power, C. Life course epidemiology. J. Epidemiol. Community Health 2003, 57, 778. [Google Scholar] [CrossRef] [PubMed]
- Lynch, J.; Smith, G.D. A life course approach to chronic disease epidemiology. Annu. Rev. Public Health 2005, 26, 1–35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Skull, S.A.; Walker, A.C.; Ruben, A.R. Malnutrition and microcephaly in Australian Aboriginal children. Med J. Aust. 1997, 166, 412–414. [Google Scholar] [CrossRef] [PubMed]
- Lindsay, S.W.; Wilson, A.; Golding, N.; Scott, T.W.; Takken, W. Improving the built environment in urban areas to control Aedes aegypti-borne diseases. Bull. World Health Organ. 2017, 95, 607–608. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Galobardes, B.; Shaw, M.; Lawlor, D.A.; Lynch, J.W.; Davey Smith, G. Indicators of socioeconomic position (part 1). J. Epidemiol. Community Health 2006, 60, 7–12. [Google Scholar] [CrossRef] [Green Version]
- Krauss, M.J.; Morrissey, A.E.; Winn, H.N.; Amon, E.; Leet, T.L. Microcephaly: An epidemiologic analysis. Am. J. Obstet. Gynecol. 2003, 188, 1484–1490. [Google Scholar] [CrossRef] [PubMed]
- Silva, A.A.; Barbieri, M.A.; Alves, M.T.; Carvalho, C.A.; Batista, R.F.; Ribeiro, M.R.; Lamy-Filho, F.; Lamy, Z.C.; Cardoso, V.C.; Cavalli, R.C.; et al. Prevalence and Risk Factors for Microcephaly at Birth in Brazil in 2010. Pediatrics 2018, 141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krieger, N. Discrimination and health inequities. Int. J. Health Serv. Plan. Adm. Eval. 2014, 44, 643–710. [Google Scholar] [CrossRef] [PubMed]
- Carless, W. A Brazilian Student Mapped out Rio’s Racial Segregation. What He Found Was Startling. Available online: https://www.pri.org/stories/2015-11-02/brazilian-student-mapped-out-rios-racial-segregation-what-he-found-was-startling (accessed on 7 April 2020).
- Acevedo-Garcia, D.; Lochner, K.A.; Osypuk, T.L.; Subramanian, S.V. Future directions in residential segregation and health research: A multilevel approach. Am. J. Public Health 2003, 93, 215–221. [Google Scholar] [CrossRef] [PubMed]
- Carabali, M.; Austin, N.; King, N.B.; Kaufman, J.S. The Zika epidemic and abortion in Latin America: A scoping review. Glob Health Res Policy 2018, 3, 15. [Google Scholar] [CrossRef]
- Pescarini, J.M.; Williamson, E.; Nery, J.S.; Ramond, A.; Ichihara, M.Y.; Fiaccone, R.L.; Penna, M.L.F.; Smeeth, L.; Rodrigues, L.C.; Penna, G.O.; et al. Effect of a conditional cash transfer programme on leprosy treatment adherence and cure in patients from the nationwide 100 Million Brazilian Cohort: A quasi-experimental study. Lancet Infect. Dis. 2020, 20, 618–627. [Google Scholar] [CrossRef] [Green Version]
- Pescarini, J.M.; Williamson, E.; Ichihara, M.Y.; Fiaccone, R.L.; Forastiere, L.; Ramond, A.; Nery, J.S.; Penna, M.L.F.; Strina, A.; Reis, S.; et al. Conditional Cash Transfer Program and Leprosy Incidence: Analysis of 12.9 Million Families From the 100 Million Brazilian Cohort. Am. J. Epidemiol. 2020. [Google Scholar] [CrossRef]
- Jaitman, L. Urban infrastructure in Latin America and the Caribbean: Public policy priorities. Lat. Am. Econ. Rev. 2015, 24, 13. [Google Scholar] [CrossRef] [Green Version]
- Massuda, A.; Hone, T.; Leles, F.A.G.; de Castro, M.C.; Atun, R. The Brazilian health system at crossroads: Progress, crisis and resilience. BMJ Glob. Health 2018, 3, e000829. [Google Scholar] [CrossRef] [Green Version]
- Musoke, D.; Boynton, P.; Butler, C.; Musoke, M.B. Health seeking behaviour and challenges in utilising health facilities in Wakiso district, Uganda. Afr. Health Sci. 2014, 14, 1046–1055. [Google Scholar] [CrossRef] [Green Version]
- Nielsen-Saines, K.; Brasil, P.; Kerin, T.; Vasconcelos, Z.; Gabaglia, C.R.; Damasceno, L.; Pone, M.; Abreu de Carvalho, L.M.; Pone, S.M.; Zin, A.A.; et al. Delayed childhood neurodevelopment and neurosensory alterations in the second year of life in a prospective cohort of ZIKV-exposed children. Nat. Med. 2019, 25, 1213–1217. [Google Scholar] [CrossRef] [PubMed]
- Ximenes, R.A.d.A.; Miranda-Filho, D.d.B.; Brickley, E.B.; Montarroyos, U.R.; Martelli, C.M.T.; Araújo, T.V.B.d.; Rodrigues, L.C.; de Albuquerque, M.d.F.P.M.; de Souza, W.V.; Castanha, P.M.d.S.; et al. Zika virus infection in pregnancy: Establishing a case definition for clinical research on pregnant women with rash in an active transmission setting. PLoS Negl. Trop. Dis. 2019, 13, e0007763. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ziraba, A. How Outbreaks Like Ebola Extract Huge Social and Economic Costs. Available online: https://reliefweb.int/report/world/how-outbreaks-ebola-extract-huge-social-and-economic-costs (accessed on 7 April 2020).
- Koh, H.K.; Oppenheimer, S.C.; Massin-Short, S.B.; Emmons, K.M.; Geller, A.C.; Viswanath, K. Translating research evidence into practice to reduce health disparities: A social determinants approach. Am. J. Public Health 2010, 100 (Suppl. 1), S72–S80. [Google Scholar] [CrossRef] [PubMed]




| Variable | Category | Total, No. | No. (col%)/ Median (IQR) |
|---|---|---|---|
| Characteristics of children | |||
| Sex | Female | 163 | 84 (51.5%) |
| Male | 79 (48.5%) | ||
| Gestational age (weeks) | 163 | 38 (38–40) | |
| Birthweight (g) | 163 | 3060 (2675–3420) | |
| Age at last Bayley-III test (months) | 112 | 19.6 (12.8–36.0) | |
| Characteristics of mothers | |||
| Age at enrolment (years) | Median (IQR) | 126 | 30.8 (23.6–34.7) |
| Educational level | Primary school, including partial | 147 | 22 (15.0%) |
| Secondary school, including partial | 77 (52.4%) | ||
| Higher education, including partial | 48 (32.7%) | ||
| Race/ethnicity | White Brazilians | 145 | 53 (36.6%) |
| Mixed-race Afro-Brazilians | 66 (45.5%) | ||
| Black Afro-Brazilians | 23 (15.9%) | ||
| East Asian Brazilians | 3 (2.1%) | ||
| Parity | ≤1 | 151 | 81 (53.6%) |
| 2 | 50 (33.1%) | ||
| 3+ | 20 (13.3%) | ||
| Previous miscarriage or abortion | No | 143 | 117 (81.8%) |
| Yes | 26 (19.2%) | ||
| Trimester of pregnancy with rash | First | 130 | 56 (43.1%) |
| Second | 49 (37.7%) | ||
| Third | 25 (19.2%) | ||
| Smoking during pregnancy | No | 145 | 139 (95.9%) |
| Yes | 6 (4.1%) | ||
| Drug use during pregnancy | No | 146 | 138 (94.5%) |
| Yes | 8 (5.5%) | ||
| Occupational exposure to toxic products during pregnancy | No | 143 | 111 (77.6%) |
| Yes | 32 (22.4%) | ||
| Characteristics of household | |||
| Monthly income (relative to 2019 minimum wage of BRL 998) | Class A: >20× minimum wage | 132 | 2 (1.5%) |
| Class B: 10–20× minimum wage | 7 (5.3%) | ||
| Class C: 4–10× minimum wage | 18 (13.6%) | ||
| Class D: 2–4× minimum wage | 38 (28.8%) | ||
| Class E: <2× minimum wage | 67 (50.8%) | ||
| Participation in Bolsa Família | No | 138 | 111 (80.4%) |
| Yes | 27 (19.6%) | ||
| Household crowding index | <0.50 | 136 | 38 (27.9%) |
| 0.50–0.75 | 46 (33.8%) | ||
| 0.75–1.00 | 33 (24.3%) | ||
| 1.00+ | 19 (14.0%) | ||
| Variable | Category | Number of Children Exposed to ZIKV In Utero | No. (Row %) of Exposed Children with Microcephaly | Crude Odds Ratio (95% CI) | p Value */** |
|---|---|---|---|---|---|
| Characteristics of children | |||||
| Sex | Female | 84 | 27 (32.1%) | 1 | 0.808 |
| Male | 79 | 24 (30.4%) | 0.92 (0.47, 1.79) | ||
| Characteristics of mothers | |||||
| Educational level | Primary school, including partial | 22 | 13 (59.1%) | 1 | <0.001 |
| Secondary school, including partial | 77 | 27 (35.1%) | 0.37 (0.14, 0.99) | ||
| Higher education, including partial | 48 | 7 (14.6%) | 0.12 (0.04, 0.38) | ||
| Missing | 16 | 4 (25.0%) | |||
| Race/ethnicity | White Brazilian and East Asian Brazilian | 56 | 15 (26.8%) | 1 | 0.038 |
| Mixed-race Afro-Brazilian | 66 | 19 (28.8%) | 1.10 (0.50, 2.45) | ||
| Black Afro-Brazilian | 23 | 13 (56.5%) | 3.55 (1.29, 9.80) | ||
| Missing | 18 | 4 (22.2%) | |||
| Parity | ≤1 | 81 | 24 (29.6%) | 1 | 0.887 |
| 2 | 50 | 16 (32.0%) | 1.12 (0.52, 2.39) | ||
| 3+ | 20 | 7 (35.0%) | 1.28 (0.45, 3.60) | ||
| Missing | 12 | 4 (33.3%) | |||
| Previous miscarriage or abortion | No | 117 | 37 (31.6%) | 1 | 0.506 |
| Yes | 26 | 10 (38.5%) | 1.35 (0.56, 3.26) | ||
| Trimester of pregnancy with rash | First | 56 | 31 (55.4%) | 1 | <0.001 |
| Second | 49 | 3 (6.1%) | 0.05 (0.01, 0.19) | ||
| Third | 25 | 2 (8.0%) | 0.07 (0.02, 0.33) | ||
| Missing | 33 | 15 (45.5%) | |||
| Smoking during pregnancy | No | 139 | 44 (31.7%) | 1 | 0.363 |
| Yes | 6 | 3 (50.0%) | 2.16 (0.42, 11.13) | ||
| Missing | 18 | 4 (22.2%) | |||
| Drug use during pregnancy | No | 138 | 44 (31.9%) | 1 | 0.744 |
| Yes | 8 | 3 (37.5%) | 1.28 (0.29, 5.61) | ||
| Missing | 17 | 4 (23.5%) | |||
| Occupational exposure to toxic products during pregnancy | No | 111 | 37 (33.3%) | 1 | 0.824 |
| Yes | 32 | 10 (31.3%) | 0.90 (0.39, 2.12) | ||
| Missing | 20 | 4 (20.0%) | |||
| Characteristics of household | |||||
| Income per month (relative to minimum wage) | Classes A, B, C and D: >2× min wage | 65 | 9 (13.8%) | 1 | <0.001 |
| Class E: <2× min wage | 67 | 32 (47.8%) | 5.69 (2.43, 13.33) | ||
| Missing | 31 | 10 (32.3%) | |||
| Participation in Bolsa Família | No | 111 | 33 (29.7%) | 1 | 0.033 |
| Yes | 27 | 14 (51.9%) | 2.55 (1.08, 6.00) | ||
| Missing | 25 | 4 (16.0%) | |||
| Household crowding index | <0.5 | 38 | 7 (18.4%) | 1 | 0.081 |
| 0.5–0.75 | 46 | 13 (28.3%) | 1.74 (0.62, 4.94) | ||
| 0.75–1.0 | 33 | 13 (39.4%) | 2.88 (0.98, 8.45) | ||
| 1.0+ | 19 | 11 (57.9%) | 6.09 (1.79, 20.74) | ||
| Missing | 27 | 7 (25.9%) | |||
| Variable | Category | Adjusted Odds Ratio (95% CI) | p Value * |
|---|---|---|---|
| Maternal educational level a n = 147 | Primary school, including partial | 1 | <0.001 |
| Secondary school, including partial | 0.33 (0.11, 0.98) | ||
| Higher education, including partial | 0.10 (0.03, 0.36) | ||
| Maternal race/ethnicity b n = 129 | White Brazilian and East Asian Brazilian | 1 | 0.439 |
| Mixed-race Afro-Brazilian | 0.89 (0.35, 2.27) | ||
| Black Afro-Brazilian | 1.79 (0.55, 5.86) | ||
| Household monthly income c n = 122 | Classes A, B, C and D: > 2× min wage | 1 | 0.006 |
| Class E: <2× min wage | 3.85 (1.43, 10.37) | ||
| Household participation in Bolsa Família d n = 135 | No Yes | 1 1.74 (0.69, 4.37) | 0.239 |
| Household crowding index e n = 129 | Household crowding index groups (<0.5, 0.5–0.75, 0.75–1.0, 1.0+) | 1.83 (1.16, 2.91) | 0.008 |
| Composite Language | Composite Motor | Composite Cognitive | |||||
|---|---|---|---|---|---|---|---|
| Variables | Categories | Adjusted Estimated Difference in Composite Scores (95% CI) | p Value * | Adjusted Estimated Difference in Composite Scores (95% CI) | p Value * | Adjusted Estimated Difference in Composite Scores (95% CI) | p Value * |
| Maternal educational level a n = 83 | Primary school, including partial | (Reference) | 0.821 | (Reference) | 0.975 | (Reference) | 0.200 |
| Secondary school, including partial | 3.31(−7.96, 14.57) | −0.21 (−10.69, 10.26) | −4.19 (−15.09, 6.71) | ||||
| Higher education, including partial | 3.00 (−8.61, 14.57) | 0.51 (−10.27, 11.29) | 1.80 (−9.41, 13.01) | ||||
| Maternal race/ethnicity b n = 76 | White Brazilians and East Asian Brazilians | (Reference) | 0.945 | (Reference) | 0.253 | (Reference) | 0.262 |
| Mixed-race Afro-Brazilians | 0.88 (−6.29, 8.05) | 2.86 (−3.97, 9.69) | 4.56 (−2.33, 11.46) | ||||
| Black Afro-Brazilians | 1.53 (−10.67, 13.73) | 8.51 (−3.11, 20.13) | 6.38 (−5.35, 18.11) | ||||
| Household monthly income c n = 78 | Classes A, B, C and D: >2× min wage | (Reference) | 0.411 | (Reference) | 0.594 | (Reference) | 0.905 |
| Class E: <2× min wage | 2.77 (−4.58, 10.13) | 1.72 (−5.35, 8.80) | 0.41 (−7.12, 7.95) | ||||
| Household participation in Bolsa Família d n = 80 | No Yes | (Reference) −10.78 (−19.87, −1.69) | 0.011 | (Reference) −10.45 (−19.22, −1.69) | 0.011 | (Reference) −17.20 (−26.13, −8.28) | <0.001 |
| Household crowding index e n = 76 | Linear trend across four household crowding index groups (<0.5, 0.5–0.75, 0.75–1.0, 1.0+) | −1.45 (−5.11, 2.20) | 0.380 | 1.44 (−2.05, 4.92) | 0.363 | 2.79 (−0.72, 6.30) | 0.082 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Power, G.M.; Francis, S.C.; Sanchez Clemente, N.; Vasconcelos, Z.; Brasil, P.; Nielsen-Saines, K.; Brickley, E.B.; Moreira, M.E. Examining the Association of Socioeconomic Position with Microcephaly and Delayed Childhood Neurodevelopment among Children with Prenatal Zika Virus Exposure. Viruses 2020, 12, 1342. https://doi.org/10.3390/v12111342
Power GM, Francis SC, Sanchez Clemente N, Vasconcelos Z, Brasil P, Nielsen-Saines K, Brickley EB, Moreira ME. Examining the Association of Socioeconomic Position with Microcephaly and Delayed Childhood Neurodevelopment among Children with Prenatal Zika Virus Exposure. Viruses. 2020; 12(11):1342. https://doi.org/10.3390/v12111342
Chicago/Turabian StylePower, Grace M., Suzanna C. Francis, Nuria Sanchez Clemente, Zilton Vasconcelos, Patricia Brasil, Karin Nielsen-Saines, Elizabeth B. Brickley, and Maria E. Moreira. 2020. "Examining the Association of Socioeconomic Position with Microcephaly and Delayed Childhood Neurodevelopment among Children with Prenatal Zika Virus Exposure" Viruses 12, no. 11: 1342. https://doi.org/10.3390/v12111342
APA StylePower, G. M., Francis, S. C., Sanchez Clemente, N., Vasconcelos, Z., Brasil, P., Nielsen-Saines, K., Brickley, E. B., & Moreira, M. E. (2020). Examining the Association of Socioeconomic Position with Microcephaly and Delayed Childhood Neurodevelopment among Children with Prenatal Zika Virus Exposure. Viruses, 12(11), 1342. https://doi.org/10.3390/v12111342