
Curing Cats with Feline Infectious Peritonitis with an Oral Multi-Component Drug Containing GS-441524

 , , ,
, , ,  , , , , , , , , ,
, , , , , , , , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Compound
2.2. In Vitro Efficacy of the Multi-Component Drug
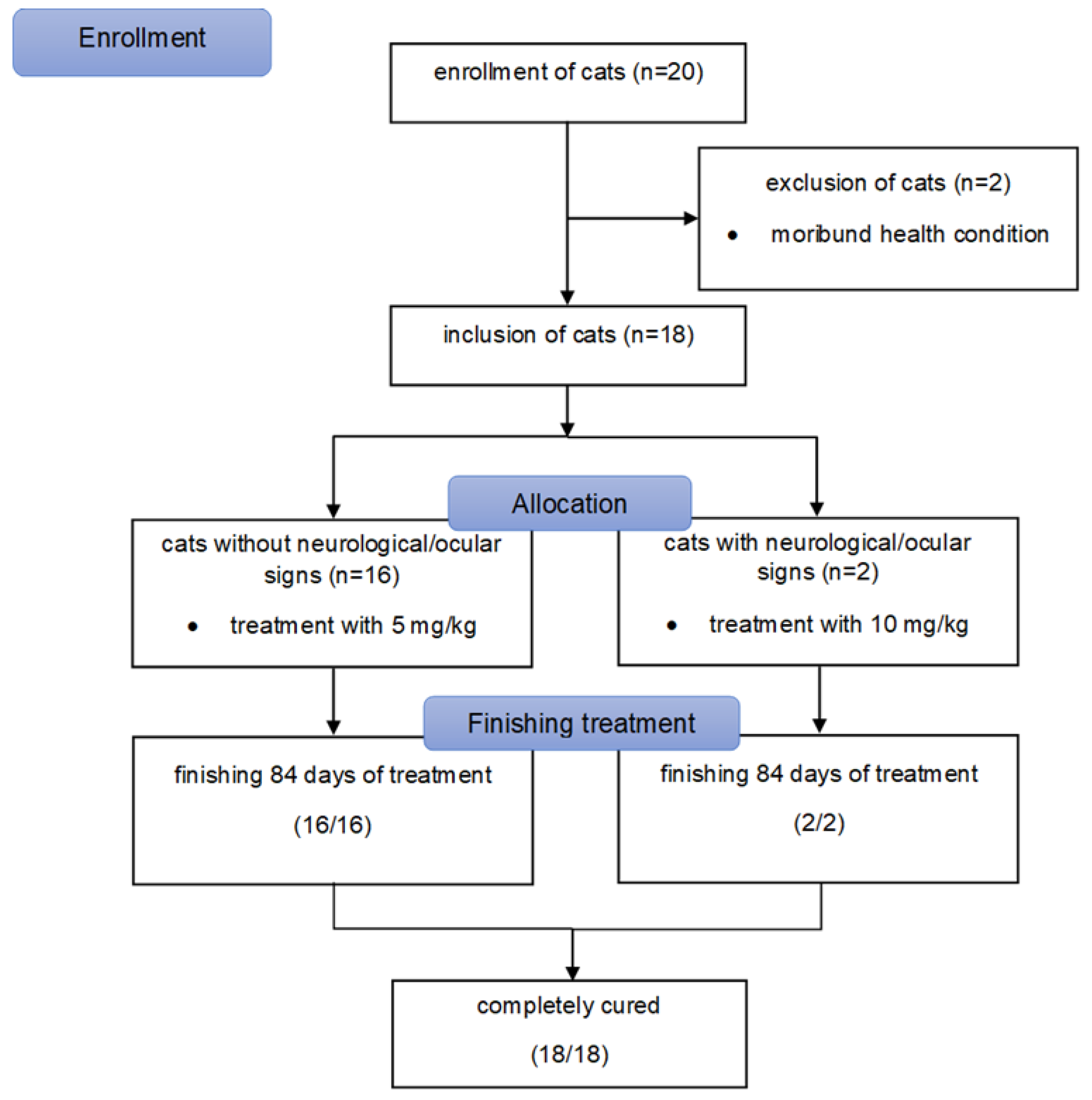
2.3. Patients of the Prospective In Vivo Study
2.4. In Vivo Study Design
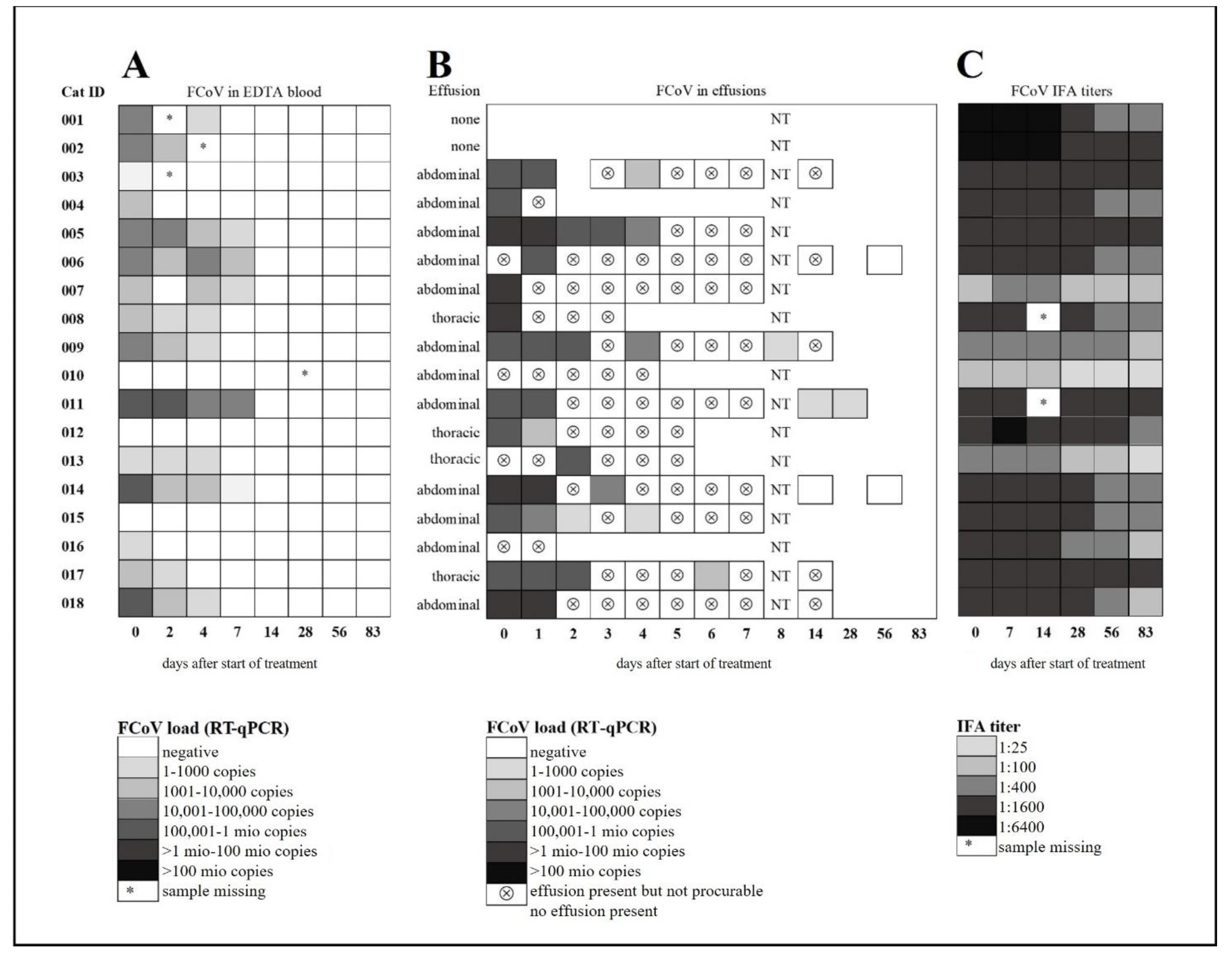
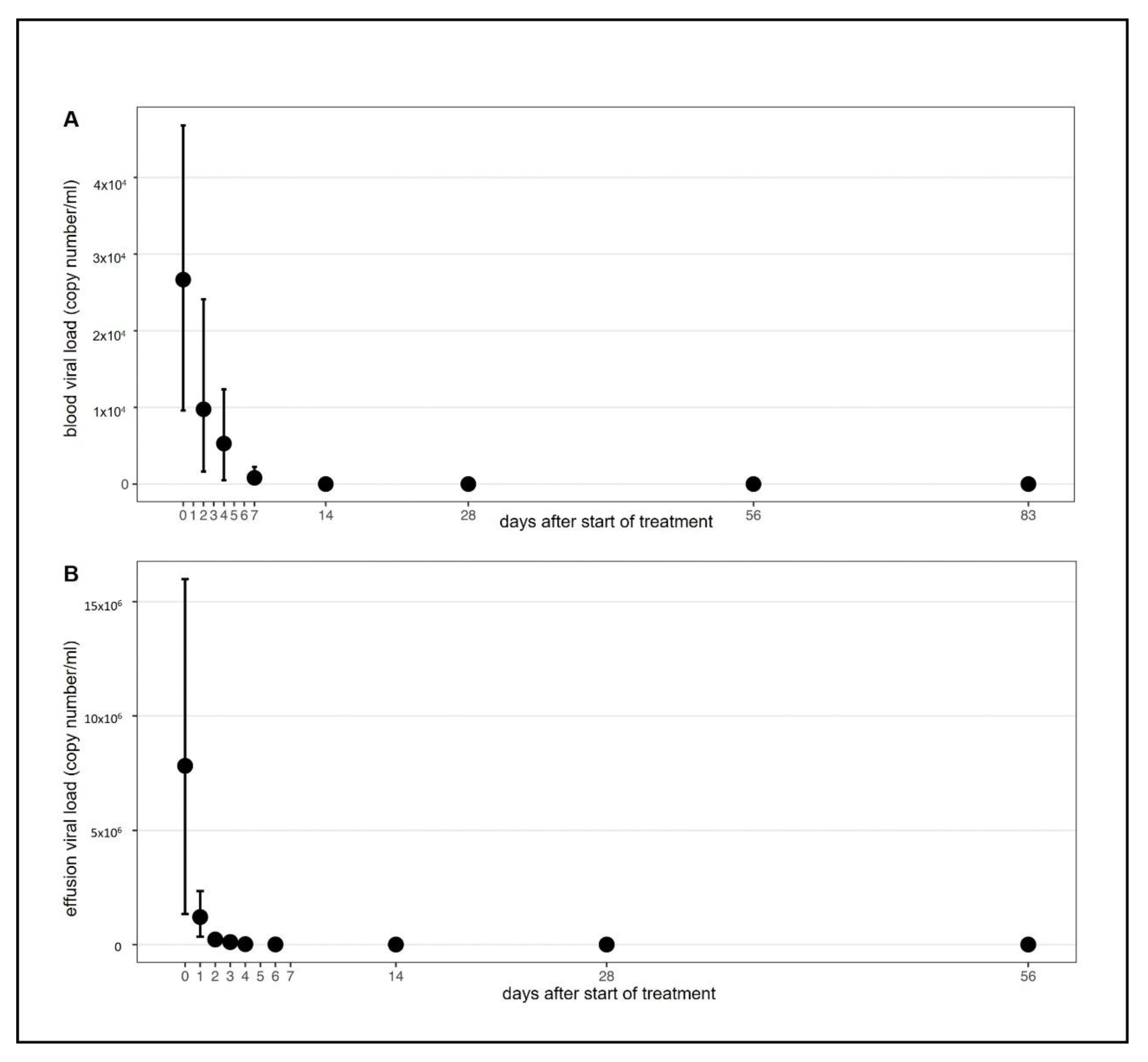
2.5. FCoV Viral Load in Blood and Effusion
2.6. Anti-FCoV Antibodies
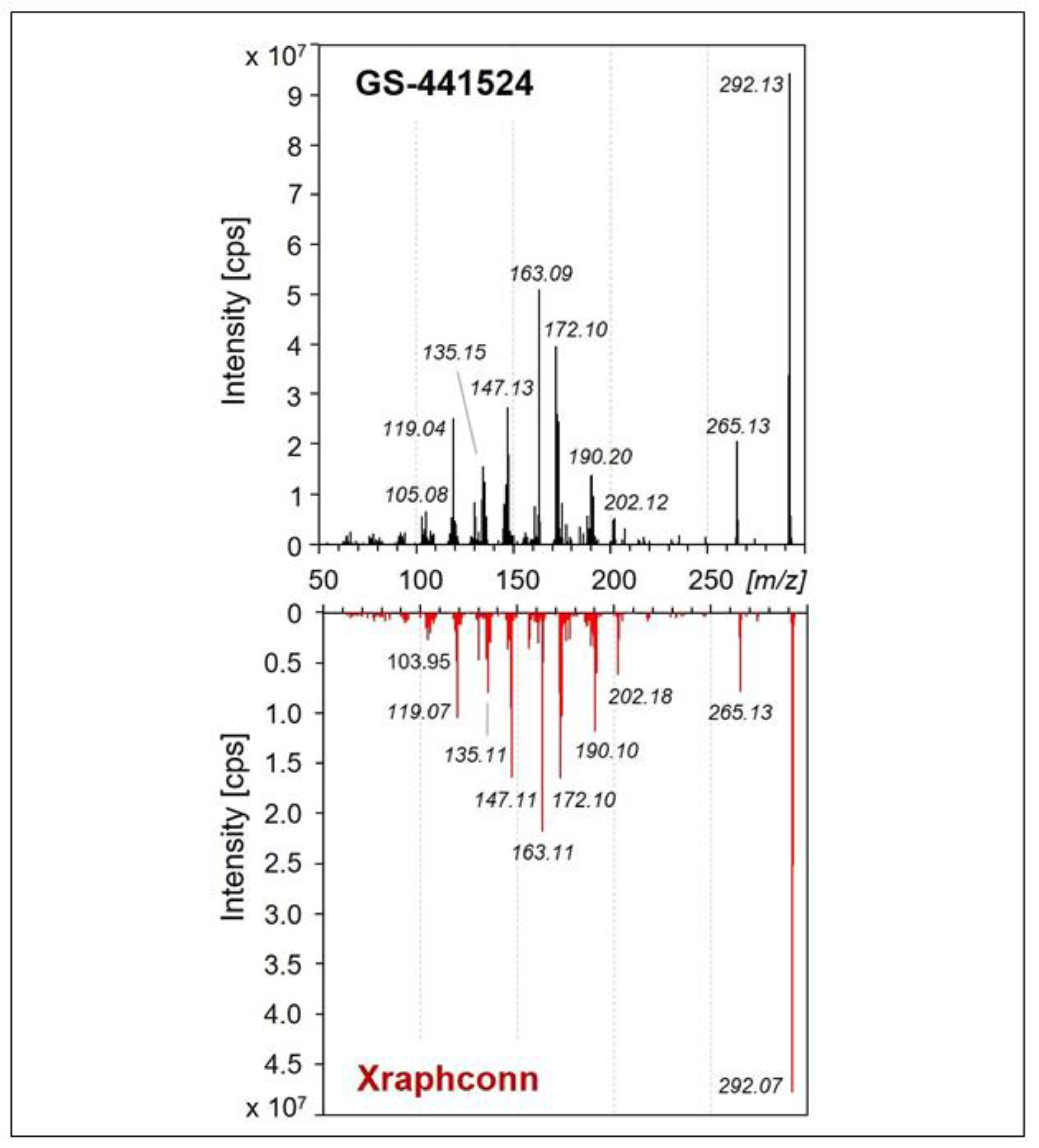
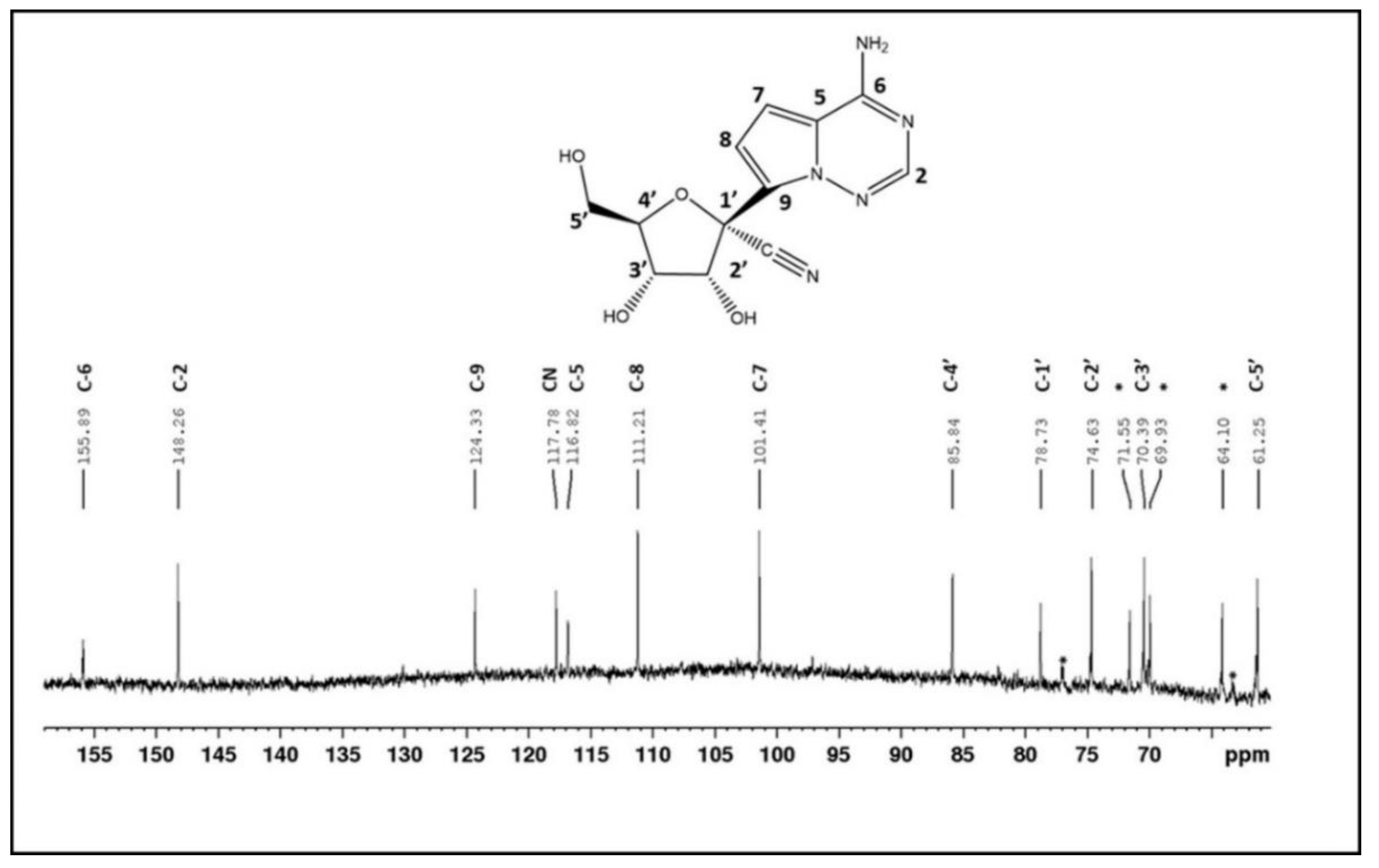
2.7. Characterization of the Active Ingredient in the Multi-Component Drug
2.8. Data Analysis
3. Results
3.1. Efficacy of the Multi-Component Drug In Vitro
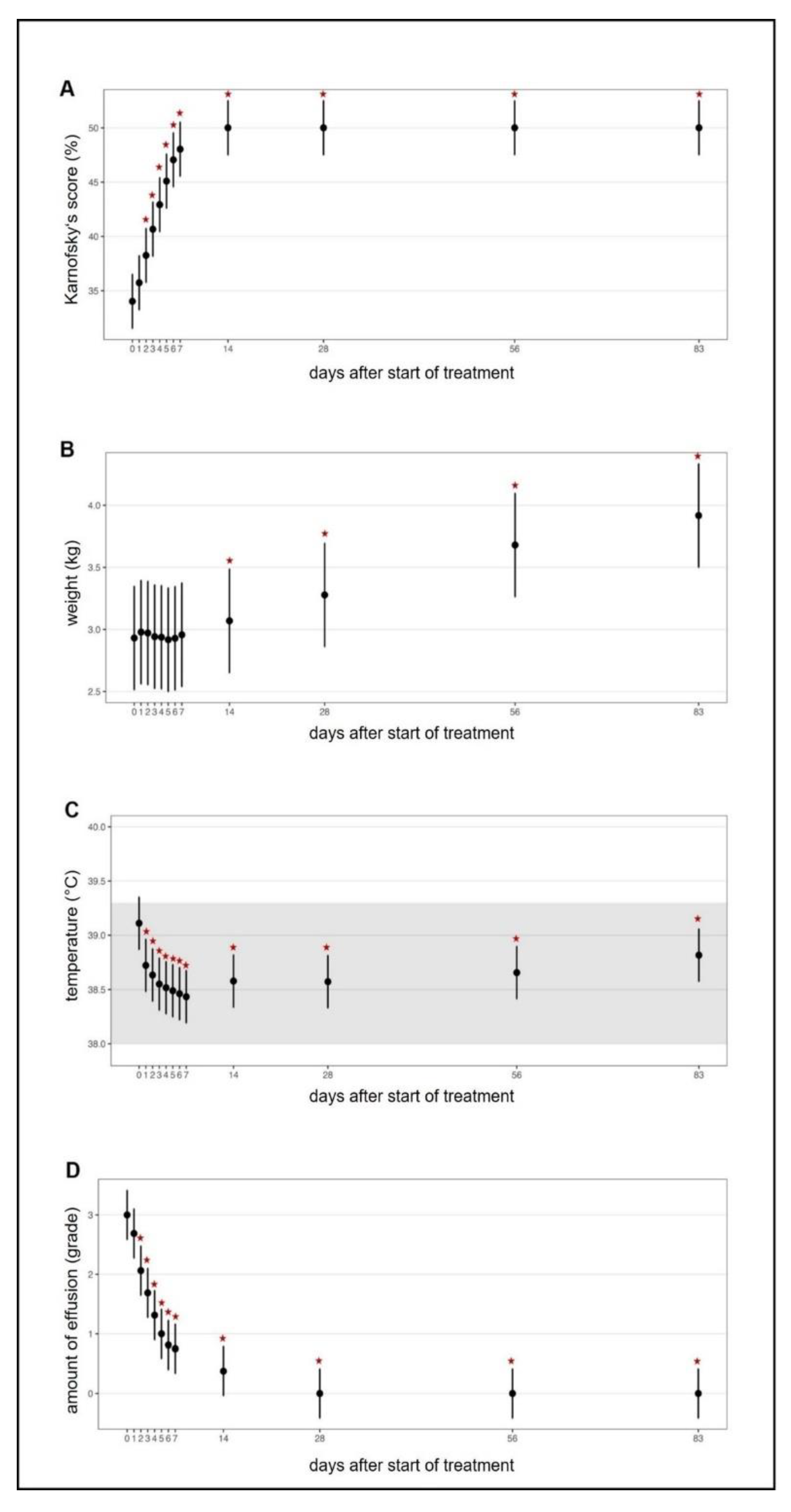
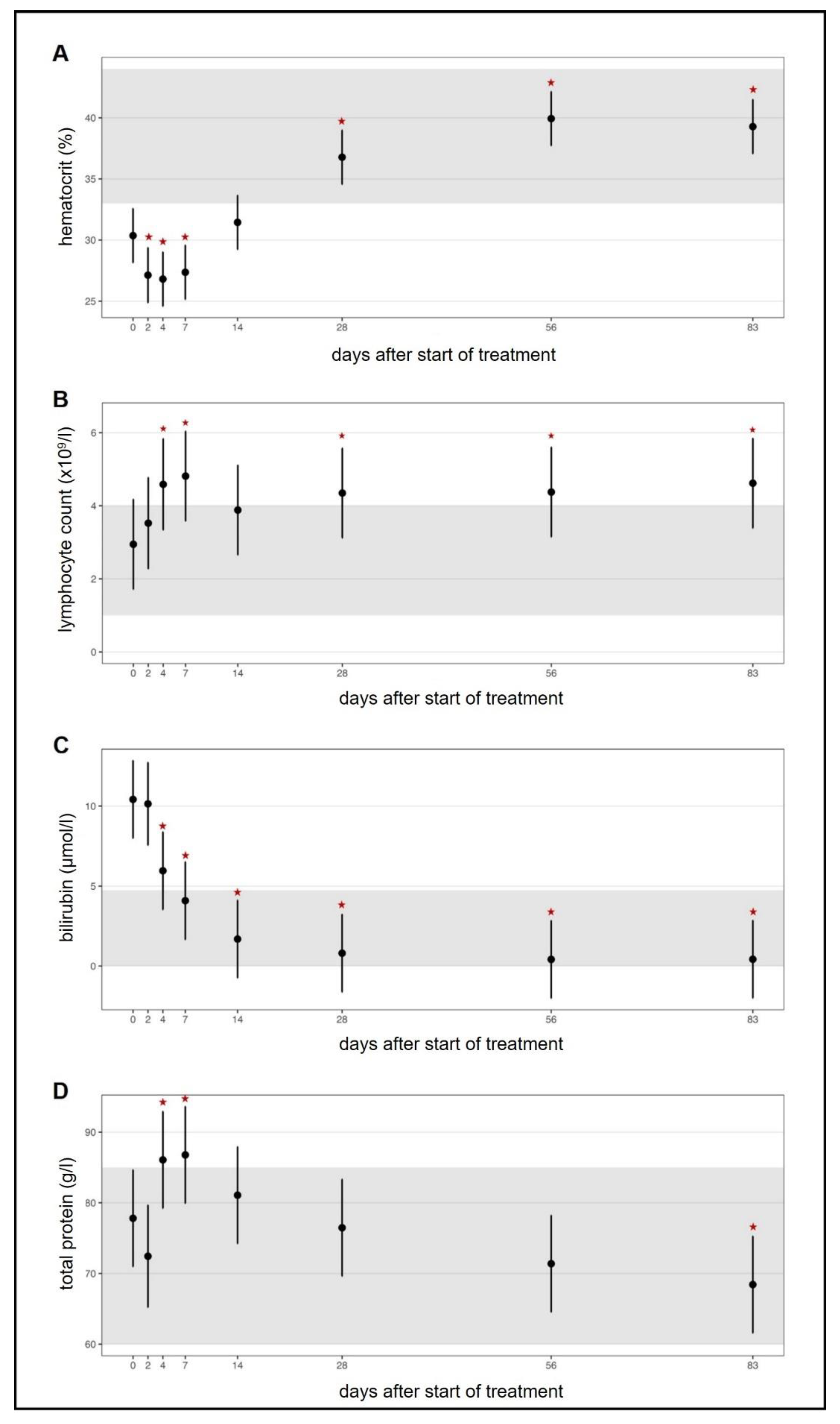
3.2. Efficacy of the Multi-Component Drug in Cats With FIP
3.3. Adverse Effects of the Multi-Comoonent Drug in Cats
3.4. Characterization of the Main Active Ingredient in the Multi-Component Drug
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lai, M.M.; Cavanagh, D. The Molecular Biology of Coronaviruses. Adv. Virus Res. 1997, 48, 1–100. [Google Scholar] [CrossRef]
- Woo, P.C.Y.; Lau, S.K.P.; Huang, Y.; Yuen, K.-Y. Coronavirus Diversity, Phylogeny and Interspecies Jumping. Exp. Biol. Med. 2009, 234, 1117–1127. [Google Scholar] [CrossRef]
- Woo, P.C.; Lau, S.K.; Lam, C.S.; Lau, C.C.; Tsang, A.K.; Lau, J.H.; Bai, R.; Teng, J.L.; Tsang, C.C.; Wang, M.; et al. Discovery of seven novel mammalian and avian coronaviruses in the genus deltacoronavirus supports bat coronaviruses as the gene source of alphacoronavirus and betacoronavirus and avian coronaviruses as the gene source of gammacoronavirus and deltacoronavirus. J. Virol. 2012, 86, 3995–4008. [Google Scholar] [PubMed]
- Amirian, E.S.; Levy, J.K. Current knowledge about the antivirals remdesivir (GS-5734) and GS-441524 as therapeutic options for coronaviruses. One Health 2020, 9, 100128. [Google Scholar] [CrossRef]
- Riphagen, S.; Gomez, X.; Gonzalez-Martinez, C.; Wilkinson, N.; Theocharis, P. Hyperinflammatory shock in children during COVID-19 pandemic. Lancet 2020, 395, 1607–1608. [Google Scholar] [CrossRef]
- Alberer, M.; von Both, U. Cats and kids: How a feline disease may help us unravel COVID-19 associated paediatric hyperin-flammatory syndrome. Infection 2021, 49, 191–193. [Google Scholar] [CrossRef] [PubMed]
- Lawrensia, S.; Henrina, J.; Wijaya, E.; Suciadi, L.P.; Saboe, A.; Cool, C.J. Pediatric Inflammatory Multisystem Syndrome temporally associated with SARS-CoV-2: A new challenge amid the pandemic. SN Compr. Clin. Med. 2020, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Korath, A.D.J.; Janda, J.; Untersmayr, E.; Sokolowska, M.; Feleszko, W.; Agache, I.; Seida, A.A.; Hartmann, K.; Jensen-Jarolim, E.; Pali-Schöll, I. One Health: EAACI Position Paper on coronaviruses at the human-animal interface, with a specific focus on comparative and zoonotic aspects of SARS-Cov-2. Allergy 2021. [Google Scholar] [CrossRef]
- Ritz, S.; Egberink, H.; Hartmann, K. Effect of feline interferon-omega on the survival time and quality of life of cats with feline infectious peritonitis. J. Vet. Intern. Med. 2007, 21, 1193–1197. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, N.C.; Allen, C.E.; Lyons, L. Pathogenesis of feline enteric coronavirus infection. J. Feline Med. Surg. 2008, 10, 529–541. [Google Scholar] [CrossRef] [PubMed]
- Poland, A.M.; Vennema, H.; E Foley, J.; Pedersen, N.C. Two related strains of feline infectious peritonitis virus isolated from immunocompromised cats infected with a feline enteric coronavirus. J. Clin. Microbiol. 1996, 34, 3180–3184. [Google Scholar] [CrossRef] [PubMed]
- Vennema, H.; Poland, A.; Foley, J.; Pedersen, N.C. Feline infectious peritonitis viruses arise by mutation from endemic feline enteric coronaviruses. Virology 1998, 243, 150–157. [Google Scholar] [CrossRef] [PubMed]
- Addie, D.D.; Jarrett, O. A study of naturally occurring feline coronavirus infections in kittens. Vet. Rec. 1992, 130, 133–137. [Google Scholar] [CrossRef]
- Pedersen, N.C.; Liu, H.; Dodd, K.A.; Pesavento, P.A. Significance of Coronavirus Mutants in Feces and Diseased Tissues of Cats Suffering from Feline Infectious Peritonitis. Viruses 2009, 1, 166–184. [Google Scholar] [CrossRef] [PubMed]
- Chang, H.W.; Egberink, H.F.; Halpin, R.; Spiro, D.J.; Rottier, P.J. Spike protein fusion peptide and feline coronavirus virulence. Emerg. Infect. Dis. 2012, 18, 1089–1095. [Google Scholar] [CrossRef]
- Pedersen, N.C.; Liu, H.; Scarlett, J.; Leutenegger, C.M.; Golovko, L.; Kennedy, H.; Kamal, F.M. Feline infectious peritonitis: Role of the feline coronavirus 3c gene in intestinal tropism and pathogenicity based upon isolates from resident and adopted shelter cats. Virus Res. 2012, 165, 17–28. [Google Scholar] [CrossRef] [PubMed]
- Barker, E.; Tasker, S.; Gruffydd-Jones, T.; Tuplin, C.; Burton, K.; Porter, E.; Day, M.; Harley, R.; Fews, D.; Helps, C.; et al. Phylogenetic Analysis of Feline Coronavirus Strains in an Epizootic Outbreak of Feline Infectious Peritonitis. J. Vet. Intern. Med. 2013, 27, 445–450. [Google Scholar] [CrossRef]
- Licitra, B.N.; Millet, J.K.; Regan, A.D.; Hamilton, B.S.; Rinaldi, V.D.; Duhamel, G.E.; Whittaker, G.R. Mutation in spike protein cleavage site and pathogenesis of feline coronavirus. Emerg. Infect. Dis. 2013, 19, 1066–1073. [Google Scholar] [CrossRef]
- Rottier, P.J.; Nakamura, K.; Schellen, P.; Volders, H.; Haijema, B.J. Acquisition of macrophage tropism during the pathogene-sis of feline infectious peritonitis is determined by mutations in the feline coronavirus spike protein. J. Virol. 2005, 79, 14122–14130. [Google Scholar] [CrossRef]
- Fischer, Y.; Ritz, S.; Weber, K.; Sauter-Louis, C.; Hartmann, K. Randomized, placebo controlled study of the effect of propen-tofylline on survival time and quality of life of cats with feline infectious peritonitis. J. Vet. Intern. Med. 2011, 25, 1270–1276. [Google Scholar] [CrossRef]
- Weiss, R.C.; Cox, N.R.; Martinez, M.L. Evaluation of free or liposome-encapsulated ribavirin for antiviral therapy of experi-mentally induced feline infectious peritonitis. Res. Vet. Sci. 1993, 55, 162–172. [Google Scholar] [CrossRef]
- Weiss, R.C.; Cox, N.R.; Boudreaux, M.K. Toxicologic effects of ribavirin in cats. J. Vet. Pharmacol. Ther. 1993, 16, 301–316. [Google Scholar] [CrossRef] [PubMed]
- Weiss, R.C.; Oostrom-Ram, T. Inhibitory effects of ribavirin alone or combined with human alpha interferon on feline infec-tious peritonitis virus replication in vitro. Vet. Microbiol. 1989, 20, 255–265. [Google Scholar] [CrossRef]
- Dickinson, P.J.; Bannasch, M.; Thomasy, S.M.; Murthy, V.D.; Vernau, K.M.; Liepnieks, M.; Montgomery, E.; Knickelbein, K.E.; Murphy, B.; Pedersen, N.C. Antiviral treatment using the adenosine nucleoside analogue GS-441524 in cats with clinically diagnosed neurological feline infectious peritonitis. J. Vet. Intern. Med. 2020, 34, 1587–1593. [Google Scholar] [CrossRef]
- Pedersen, N.C.; Perron, M.; Bannasch, M.; Montgomery, E.; Murakami, E.; Liepnieks, M.; Liu, H. Efficacy and safety of the nucleoside analog GS-441524 for treatment of cats with naturally occurring feline infectious peritonitis. J. Feline Med. Surg. 2019, 21, 271–281. [Google Scholar] [CrossRef]
- Addie, D.; Covell-Ritchie, J.; Jarrett, O.; Fosbery, M. Rapid Resolution of Non-Effusive Feline Infectious Peritonitis Uveitis with an Oral Adenosine Nucleoside Analogue and Feline Interferon Omega. Viruses 2020, 12, 1216. [Google Scholar] [CrossRef]
- Pedersen, N.C.; Kim, Y.; Liu, H.; Kankanamalage, A.C.G.; Eckstrand, C.; Groutas, W.C.; Bannasch, M.; Meadows, J.M.; Chang, K.-O. Efficacy of a 3C-like protease inhibitor in treating various forms of acquired feline infectious peritonitis. J. Feline Med. Surg. 2018, 20, 378–392. [Google Scholar] [CrossRef] [PubMed]
- Murphy, B.; Perron, M.; Murakami, E.; Bauer, K.; Park, Y.; Eckstrand, C.; Liepnieks, M.; Pedersen, N. The nucleoside analog GS-441524 strongly inhibits feline infectious peritonitis (FIP) virus in tissue culture and experimental cat infection studies. Vet. Microbiol. 2018, 219, 226–233. [Google Scholar] [CrossRef] [PubMed]
- Agostini, M.L.; Andres, E.L.; Sims, A.C.; Graham, R.L.; Sheahan, T.P.; Lu, X.; Smith, E.C.; Case, J.B.; Feng, J.Y.; Jordan, R.; et al. Coronavirus Susceptibility to the Antiviral Remdesivir (GS-5734) is Mediated by the Viral Polymerase and the Proofreading Exoribonuclease. mBio 2018, 9, e00221-18. [Google Scholar] [CrossRef]
- Jorgensen, S.C.J.; Kebriaei, R.; Dresser, L.D. Remdesivir: Review of Pharmacology, Pre-clinical data, and emerging clinical experience for COVID-19. Pharmacotherapy 2020, 40, 659–671. [Google Scholar] [CrossRef] [PubMed]
- Huang, T.; Sun, L.; Kang, D.; Poongavanam, V.; Liu, X.; Zhan, P.; Menéndez-Arias, L. Search, Identification, and Design of Effective Antiviral Drugs Against Pandemic Human Coronaviruses. Single Mol. Single Cell Seq. 2021, 1322, 219–260. [Google Scholar] [CrossRef]
- Kim-Hellmuth, S.; Hermann, M.; Eilenberger, J.; Ley-Zaporozhan, J.; Fischer, M.; Hauck, F.; Klein, C.; Haas, N.; Kappler, M.; Huebner, J.; et al. SARS-CoV-2 triggering severe acute respiratory distress syndrome and secondary hemophagocytic lymphohistiocytosis in a 3-year-old child with Down Syndrome. J. Pediatric. Infect. Dis. Soc. 2021, 10, 543–546. [Google Scholar] [CrossRef]
- Hartmann, K.; Day, M.J.; Thiry, E.; Lloret, A.; Frymus, T.; Addie, D.; Boucraut-Baralon, C.; Egberink, H.; Gruffydd-Jones, T.; Horzinek, M.C.; et al. Feline injection-site sarcoma: ABCD guidelines on prevention and management. J. Feline Med. Surg. 2015, 17, 606–613. [Google Scholar] [CrossRef]
- Jones, S.; Novicoff, W.; Nadeau, J.; Evans, S. Unlicensed GS-441524-like antiviral therapy can be effective for at home treatment of feline infectious peritonitis. Animals 2021, 11, 2257. [Google Scholar] [CrossRef] [PubMed]
- Yin, Y.; Li, T.; Wang, C.; Liu, X.; Ouyang, H.; Ji, W.; Liu, J.; Liao, X.; Li, J.; Hu, C. A retrospective study of clinical and laboratory features and treatment on cats highly suspected of feline infectious peritonitis in Wuhan, China. Sci. Rep. 2021, 11, 5208. [Google Scholar] [CrossRef] [PubMed]
- Felten, S.; Hartmann, K. Diagnosis of Feline Infectious Peritonitis: A Review of the Current Literature. Viruses 2019, 11, 1068. [Google Scholar] [CrossRef] [PubMed]
- European Advisory Board on Cat Diseases (ABCD). FIP Diagnosis Tool. August 2021. Available online: http://www.abcdcatsvets.org/wp-content/uploads/2021/09/FIP_diagnosis_tool.pdf (accessed on 21 October 2021).
- European Advisory Board on Cat Disease (ABCD). Feline Infectious Peritonitis. March 2021. Available online: http://www.abcdcatsvets.org/feline-infectious-peritonitis/http://www.abcdcatsvets.org/feline-infectious-peritonitis/ (accessed on 14 September 2021).
- Dülsner, A.; Hack, R.; Krüger, C.; Pils, M.; Scherer, K.; Schmelting, B.; Schmidt, M.; Weinert, H.; Jordan, T. Fachinformation aus dem Ausschuss für Tier-Schutzbeauftragte und dem Arbeitskreis 4 in der TVT.; Empfehlung zur Blutentnahme bei Versuchstieren, Insbesondere Kleinen Versuchstieren. 2017. Available online: http://www.gv-solas.de/fileadmin/user_upload/pdf_publikation/Tierschutzbeauftragte/tie_blutentnahme17 (accessed on 14 September 2021).
- Hartmann, K.; Kuffer, M. Karnofsky’s score modified for cats. Eur. J. Med. Res. 1998, 3, 95–98. [Google Scholar]
- Taffin, E.R.L.; Paepe, D.; Campos, M.; Duchateau, L.; Goris, N.; De Roover, K.; Daminet, S. Evaluation of a modified Karnofsky score to assess physical and psychological wellbeing of cats in a hospital setting. J. Feline Med. Surg. 2016, 18, 913–920. [Google Scholar] [CrossRef]
- Gut, M.; Leutenegger, C.M.; Huder, J.B.; Pedersen, N.C.; Lutz, H. One-tube fluorogenic reverse transcription-polymerase chain reaction for the quantitation of feline coronaviruses. J. Virol. Methods 1999, 77, 37–46. [Google Scholar] [CrossRef]
- Lutz, H.; Hauser, B.; Horzinek, M. On the serological diagnosis of feline infectious peritonitis. Prakt Tierarzt 1984, 65, 406–408. [Google Scholar]
- Osterhaus, A.D.; Horzinek, M.C.; Reynolds, D.J. Seroepidemiology of feline infectious peritonitis virus infections using trans-missible gastroenteritis virus as antigen. Zent. Vet. B 1977, 24, 835–841. [Google Scholar] [CrossRef] [PubMed]
- Brunner, C.; Kanellos, T.; Meli, M.L.; Sutton, D.J.; Gisler, R.; Gomes-Keller, M.A.; Hofmann-Lehmann, R.; Lutz, H. Antibody induction after combined application of an adjuvanted recombinant FeLV vaccine and a multivalent modified live virus vac-cine with a chlamydial component. Vaccine 2006, 24, 1838–1846. [Google Scholar] [CrossRef]
- Felten, S.; Klein-Richers, U.; Hofmann-Lehmann, R.; Bergmann, M.; Unterer, S.; Leutenegger, C.M.; Hartmann, K. Correlation of feline coronavirus shedding in feces with coronavirus antibody titer. Pathogens 2020, 9, 598. [Google Scholar] [CrossRef] [PubMed]
- International Renal Interest Society IRIS. IRIS Grading of AKI. 2016. Available online: http://www.iris-kidney.com/guidelines/grading (accessed on 14 September 2021).
- Davis, A.L.; Laue, E.D.; Keeler, J.; Moskau, D.; Lohman, J. Absorption-mode two-dimensional NMR spectra recorded using pulsed field gradients. J. Magn. Reson. (1969) 1991, 94, 637–644. [Google Scholar] [CrossRef]
- Griesinger, C.; Otting, G.; Wuethrich, K.; Ernst, R.R. Clean TOCSY for proton spin system identification in macromolecules. J. Am. Chem. Soc. 1988, 110, 7870–7872. [Google Scholar] [CrossRef]
- Ruiz-Cabello, J.; Vuister, G.W.; Moonen, C.T.; Van Gelderen, P.; Cohen, J.S.; Van Zijl, P.C. Gradient-enhanced heteronuclear correlation spectroscopy: Theory and experimental aspects. J. Magn. Reson. 2011, 213, 446–466. [Google Scholar] [CrossRef]
- Warren, T.K.; Jordan, R.; Lo, M.K.; Ray, A.S.; Mackman, R.L.; Soloveva, V.; Siegel, D.; Perron, M.; Bannister, R.; Hui, H.C.; et al. Therapeutic efficacy of the small molecule GS-5734 against Ebola virus in rhesus monkeys. Nature 2016, 531, 381–385. [Google Scholar] [CrossRef]
- Hartmann, K.; Binder, C.; Hirschberger, J.; Cole, D.; Reinacher, M.; Schroo, S.; Frost, J.; Egberink, H.; Lutz, H.; Hermanns, W. Comparison of different tests to diagnose feline infectious peritonitis. J. Vet. Intern. Med. 2003, 17, 781–790. [Google Scholar] [CrossRef] [PubMed]
- Riemer, F.; Kuehner, K.A.; Ritz, S.; Sauter-Louis, C.; Hartmann, K. Clinical and laboratory features of cats with feline infectious peritonitis—A retrospective study of 231 confirmed cases (2000–2010). J. Feline Med. Surg. 2016, 18, 348–356. [Google Scholar] [CrossRef]
- Tecles, F.; Caldín, M.; Tvarijonaviciute, A.; Escribano, D.; Martinez-Subiela, S.; Cerón, J. Serum biomarkers of oxidative stress in cats with feline infectious peritonitis. Res. Vet. Sci. 2015, 100, 12–17. [Google Scholar] [CrossRef] [PubMed]
- Hazuchova, K.; Held, S.; Neiger, R. Usefulness of acute phase proteins in differentiating between feline infectious peritonitis and other diseases in cats with body cavity effusions. J. Feline Med. Surg. 2016, 19, 809–816. [Google Scholar] [CrossRef]
- Giordano, A.; Spagnolo, V.; Colombo, A.; Paltrinieri, S. Changes in some acute phase protein and immunoglobulin concen-trations in cats affected by feline infectious peritonitis or exposed to feline coronavirus infection. Vet. J. 2004, 167, 38–44. [Google Scholar] [CrossRef]
- Sasaki, K.; Ma, Z.; Khatlani, T.S.; Okuda, M.; Inokuma, H.; Onishi, T. Evaluation of feline serum amyloid A (SAA) as an in-flammatory marker. J. Vet. Med. Sci. 2003, 65, 545–548. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, N.C.; Eckstrand, C.; Liu, H.; Leutenegger, C.; Murphy, B. Levels of feline infectious peritonitis virus in blood, effusions, and various tissues and the role of lymphopenia in disease outcome following experimental infection. Vet. Microbiol. 2015, 175, 157–166. [Google Scholar] [CrossRef] [PubMed]
- Doenges, S.J.; Weber, K.; Dorsch, R.; Fux, R.; Hartmann, K. Comparison of real-time reverse transcriptase polymerase chain reaction of peripheral blood mononuclear cells, serum and cell-free body cavity effusion for the diagnosis of feline infectious peritonitis. J. Feline Med. Surg. 2016, 19, 344–350. [Google Scholar] [CrossRef] [PubMed]
- Felten, S.; Leutenegger, C.M.; Balzer, H.-J.; Pantchev, N.; Matiasek, K.; Wess, G.; Egberink, H.; Hartmann, K. Sensitivity and specificity of a real-time reverse transcriptase polymerase chain reaction detecting feline coronavirus mutations in effusion and serum/plasma of cats to diagnose feline infectious peritonitis. BMC Vet. Res. 2017, 13, 1–11. [Google Scholar] [CrossRef]
- Felten, S.; Weider, K.; Doenges, S.; Gruendl, S.; Matiasek, K.; Hermanns, W.; Mueller, E.; Matiasek, L.; Fischer, A.; Weber, K.; et al. Detection of feline coronavirus spike gene mutations as a tool to diagnose feline infectious peritonitis. J. Feline Med. Surg. 2017, 19, 321–335. [Google Scholar] [CrossRef] [PubMed]
- Tappuni, A.R. Immune reconstitution inflammatory syndrome. Adv. Dent. Res. 2011, 23, 90–96. [Google Scholar] [CrossRef]
- Paltrinieri, S.; Ponti, W.; Comazzi, S.; Giordano, A.; Poli, G. Shifts in circulating lymphocyte subsets in cats with feline infec-tious peritonitis (FIP): Pathogenic role and diagnostic relevance. Vet. Immunol. Immunopathol. 2003, 96, 141–148. [Google Scholar] [CrossRef]
- Dean, G.A.; Olivry, T.; Stanton, C.; Pedersen, N.C. In vivo cytokine response to experimental feline infectious peritonitis virus infection. Vet. Microbiol. 2003, 97, 1–12. [Google Scholar] [CrossRef]
- Haagmans, B.L.; Egberink, H.; Horzinek, M.C. Apoptosis and T-cell depletion during feline infectious peritonitis. J. Virol. 1996, 70, 8977–8983. [Google Scholar] [CrossRef] [PubMed]
- Kipar, A.; Kohler, K.; Leukert, W.; Reinacher, M. A comparison of lymphatic tissues from cats with spontaneous feline infec-tious peritonitis (FIP), cats with FIP virus infection but no FIP, and cats with no infection. J. Comp. Pathol. 2001, 125, 182–191. [Google Scholar] [CrossRef]
- Takano, T.; Hohdatsu, T.; Hashida, Y.; Kaneko, Y.; Tanabe, M.; Koyama, H. A “possible” involvement of TNF-alpha in apoptosis induction in peripheral blood lymphocytes of cats with feline infectious peritonitis. Vet. Microbiol. 2007, 119, 121–131. [Google Scholar] [CrossRef] [PubMed]
- Takano, T.; Hohdatsu, T.; Toda, A.; Tanabe, M.; Koyama, H. TNF-alpha, produced by feline infectious peritonitis virus (FIPV)-infected macrophages, upregulates expression of type II FIPV receptor feline aminopeptidase N in feline macrophages. Virology 2007, 364, 64–72. [Google Scholar] [CrossRef] [PubMed]
- Kipar, A.; Bellmann, S.; Gunn-Moore, D.; Leukert, W.; Köhler, K.; Menger, S.; Reinacher, M.; Gunn-Moore, D. Histopathological alterations of lymphatic tissues in cats without feline infectious peritonitis after long-term exposure to FIP virus. Vet. Microbiol. 1999, 69, 131–137. [Google Scholar] [CrossRef]
- Kipar, A.; Meli, M.L.; Failing, K.; Euler, T.; Gomes-Keller, M.A.; Schwartz, D.; Lutz, H.; Reinacher, M. Natural feline corona-virus infection: Differences in cytokine patterns in association with the outcome of infection. Vet. Immunol. Immunopathol. 2006, 112, 141–155. [Google Scholar] [CrossRef]
- Mateos González, M.; Sierra Gonzalo, E.; Casado Lopez, I.; Arnalich Fernández, F.; Beato Pérez, J.L.; Monge Monge, D.; Vargas Núñez, J.A.; García Fenoll, R.; Suárez Fernández, C.; Freire Castro, S.J.; et al. The prognostic value of eosinophil recovery in COVID-19: A multicentre, retrospective cohort study on patients hospitalised in Spanish hospitals. J. Clin. Med. 2021, 10, 305. [Google Scholar] [CrossRef]
- Kroegel, C.; Schreiber, J. Der eosinophile Granulozyt—Vom Ursprung bis zur therapeutischen Zielzelle. Der Pneumol. 2018, 15, 297–298. [Google Scholar] [CrossRef]
- Fraissé, M.; Logre, E.; Mentec, H.; Cally, R.; Plantefève, G.; Contou, D. Eosinophilia in critically ill COVID-19 patients: A French monocenter retrospective study. Crit Care 2020, 24, 635. [Google Scholar] [CrossRef]
- Reinhart, W.H.; Sung, L.P.; Chien, S. Quantitative relationship between Heinz body formation and red blood cell deformabil-ity. Blood 1986, 68, 1376–1383. [Google Scholar] [CrossRef]
- Baetge, C.L.; Smith, L.C.; Azevedo, C.P. Clinical Heinz Body Anemia in a Cat after Repeat Propofol Administration Case Report. Front. Vet. Sci. 2020, 7, 591556. [Google Scholar] [CrossRef] [PubMed]
- Webb, C.B.; Twedt, D.C.; Fettman, M.J.; Mason, G. S-adenosylmethionine (SAMe) in a feline acetaminophen model of oxida-tive injury. J. Feline Med. Surg. 2003, 5, 69–75. [Google Scholar] [CrossRef]
- Christopher, M.M.; White, J.G.; Eaton, J.W. Erythrocyte Pathology and Mechanisms of Heinz Body-mediated Hemolysis in Cats. Vet. Pathol. 1990, 27, 299–310. [Google Scholar] [CrossRef]
- Addie, D.D.; Curran, S.; Bellini, F.; Crowe, B.; Sheehan, E.; Ukrainchuk, L.; Decaro, N. Oral Mutian®X stopped faecal feline coronavirus shedding by naturally infected cats. Res. Vet. Sci. 2020, 130, 222–229. [Google Scholar] [CrossRef] [PubMed]
- Yan, V.C.; Muller, F.L. Advantages of the Parent Nucleoside GS-441524 over Remdesivir for Covid-19 Treatment. ACS Med. Chem. Lett. 2020, 11, 1361–1366. [Google Scholar] [CrossRef]
- Xie, J.; Wang, Z. Can remdesivir and its parent nucleoside GS-441524 be potential oral drugs? An in vitro and in vivo DMPK assessment. Acta Pharm. Sin. B 2021, 11, 1607–1616. [Google Scholar] [CrossRef]
- Yan, V.C.; Pham, C.D.; Yan, M.J.; Yan, A.J.; Khadka, S.; Arthur, K.; Ackroyd, J.J.; Georgiou, D.K.; Roon, L.E.; Bushman, L.R.; et al. Pharmacokinetics of Orally Administered GS-441524 in Dogs. [Preprint]. 2021 bioRxiv (posted 31 May 2021). Available online: https://www.biorxiv.org/content/10.1101/2021.02.04.429674v3 (accessed on 14 September 2021).
- Whittaker, E.; Bamford, A.; Kenny, J.; Kaforou, M.; Jones, C.E.; Shah, P.; Ramnarayan, P.; Fraisse, A.; Miller, O.; Davies, P.; et al. Clinical characteristics of 58 children with a Pediatric Inflammatory Multisystem Syndrome temporally associated with SARS-CoV-2. JAMA 2020, 324, 259–269. [Google Scholar] [CrossRef]
- Levin, M. Childhood Multisystem Inflammatory Syndrome—A New Challenge in the Pandemic. N. Engl. J. Med. 2020, 383, 393–395. [Google Scholar] [CrossRef]
- Alberer, M.; Hartmann, K.; Matiasek, K.; Hofmann-Lehmann, R.; Felten, S.; Meli, M.; von Both, U. Treating persisting intestinal SARS-CoV-2 Infection to Prevent MIS-C—A Role for GS-441524? J. Clin. Investig. 2021. Available online: https://www.jci.org/eletters/view/149633#sec1 (accessed on 14 September 2021).










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cat | Age (Months) | Sex | Breed | Additional Cats in the Household (Number) | Diagnosis of FIP 1 | FIP-Associated Cardinal Signs | Dosage (mg/kg q24h) | Adverse Effects and Duration (on Days of Treatment) | Other Unrelated Diseases before Treatment | Other Unrelated Diseases Developing during Treatment | Additional Symptomatic Therapy |
|---|---|---|---|---|---|---|---|---|---|---|---|
| cat 1 | 6.0 | male neutered | ESH | yes (1) | immunohisto-chemistry (eye) | ocular signs | 10 mg/kg | lymphocytosis (2–end2) | fluid therapy 3, metamizole 4 | ||
| cat 2 | 6.3 | male intact | ESH | yes (1) | immunohisto-chemistry (eye) | neurologic signs, ocular signs | 10 mg/kg | lymphocytosis (0–end) | surgical wound infection after eye enucleation | fluid therapy, antibiotics 5, buprenorphine 6 | |
| cat 3 | 9.8 | male neutered | ESH | yes (1) | RT-PCR detecting S gene mutations (effusion) | abdominal effusion | 5 mg/kg | increased liver enzyme activity (4–14) | renal mineraliza-tion | fluid therapy, antibiotics, maropitant 7, mirtazapine 8 | |
| cat 4 | 7.2 | male intact | ESH | yes (1) | RT-PCR detecting S gene mutations (effusion) | abdominal effusion | 5 mg/kg | lymphocytosis (2–end), eosinophilia (14–56) | fluid therapy, metamizole-sodium, antibiotics, maropitant, mirtazapine | ||
| cat 5 | 6.4 | female intact | ESH | yes (1) | RT-PCR detecting S gene mutations (effusion) | abdominal effusion | 5 mg/kg | lymphocytosis (0–end), increased liver enzyme activity (4–83), eosinophilia (14–end) | fluid therapy, antibiotics | ||
| cat 6 | 10.7 | male neutered | ESH | yes (1) | RT-PCR detecting S gene mutations (effusion) | abdominal effusion | 5 mg/kg | lymphocytosis (83–end) | antibiotics, mirtazapine | ||
| cat 7 | 4.7 | male intact | Siamese | yes (1) | RT-PCR detecting S gene mutations (effusion) | abdominal effusion, thoracic effusion | 5 mg/kg | lymphocytosis (0–end), increased liver enzyme activity (4–83), eosinophilia (14–end) | chronic gingivo-stomatitis | fluid therapy, antibiotics, silymarin 9 | |
| cat 8 | 6.4 | male intact | Maine Coon | no | RT-PCR detecting S gene mutations (effusion) | thoracic effusion | 5 mg/kg | lymphocytosis (0–14), eosinophilia (14–83) | chronic gingivo- stomatitis | fluid therapy, antibiotics, oxygen cage 10 | |
| cat 9 | 8.9 | male neutered | ESH | yes (3) | RT-PCR detecting S gene mutations (effusion) | abdominal effusion | 5 mg/kg | lymphocytosis (28–end), increased liver enzyme activity (4–83), eosinophilia (28–end) | fluid therapy, antibiotics, mirtazapine, silymarin | ||
| cat 10 | 39.1 | female neutered | ESH | yes (3) | immunohisto-chemistry (lymph node) | abdominal effusion | 5 mg/kg | eosinophilia (0–end) | intestinal parasite infestation (Giardia spp., treated with fenbendazole) | ||
| cat 11 | 56.5 | female neutered | ESH | yes (3) | RT-PCR detecting S gene mutations (effusion) | abdominal effusion | 5 mg/kg | lymphocytosis (0–14), increased liver enzyme activity (4–97) | fluid therapy, antibiotics | ||
| cat 12 | 11.7 | male neutered | Birman | yes (1) | immunohisto-chemistry (lymphnode), RT-PCR detecting S gene mutations (effusion) | thoracic effusion | 5 mg/kg | lymphocytosis (2–end), increased liver enzyme activity (28–56), eosinophilia (28–83) | fluid therapy, antibiotics, buprenorphine | ||
| cat 13 | 28.8 | female intact | Maine Coon | yes (9) | RT-PCR detecting S gene mutations (effusion) | thoracic effusion | 5 mg/kg | eosinophilia (28–end) | rhinitis | fluid therapy, antibiotics | |
| cat 14 | 7.5 | male intact | ESH | yes (1) | RT-PCR detecting S gene mutations (effusion) | abdominal effusion | 5 mg/kg | intestinal parasite infestation (Giardia spp., treated with fenbendazole) | fluid therapy, antibiotics, maropitant, mirtazapine, buprenorphine, pregabalin 11 | ||
| cat 15 | 7.6 | male intact | Maine Coon | yes (1) | RT-PCR detecting S gene mutations (effusion) | abdominal effusion | 5 mg/kg | lymphocytosis (2–56), eosinophilia (2–28) | distorsion on right forelimb | fluid therapy, antibiotics, buprenorphine, meloxicam 12 | |
| cat 16 | 8.9 | female neutered | BSH | yes (1) | RT-PCR detecting S gene mutations (effusion) | abdominal effusion | 5 mg/kg | lymphocytosis (7–14), increased liver enzyme activity (2–14) | chronic gingivo-stomatitis | fluid therapy, mirtazapine | |
| cat 17 | 7.7 | male intact | Scottish Fold | yes (1) | RT-PCR detecting S gene mutations (effusion) | thoracic effusion | 5 mg/kg | lymphocytosis (2–end), eosinophilia (28–end) | otitis externa | pyothorax | fluid therapy, antibiotics |
| cat 18 | 7.6 | female intact | ESH | yes (2) | RT-PCR detecting S gene mutations (effusion) | abdominal effusion | 5 mg/kg | lymphocytosis (0–end), eosinophilia (2–end) | fluid therapy, antibiotics |
| Adverse Effect | Number of Cats | Grade | Median Day of First Appearance (Range) | Symptomatic Treatment | |
|---|---|---|---|---|---|
| Heinz body formation 1 | 1/18 | moderate | 83 | S-adenosyl-methionine | |
| 14/18 3 | 4/14 | mild | 4.5 (2–83) | no | |
| Lymphocytosis 2 | 6/14 | moderate | 1 (0–28) | no | |
| 4/14 | severe | 1 (0–2) | no | ||
| Eosinophilia 4 | 11/18 3 | 11/11 | mild | 14 (0–28) | no |
| increased liver enzyme activity 5 | 8/11 | mild | 28 (2–83) | no | |
| 11/18 | 1/11 | moderate | 4 | no | |
| 2/11 | severe | 4 | silymarin |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Krentz, D.; Zenger, K.; Alberer, M.; Felten, S.; Bergmann, M.; Dorsch, R.; Matiasek, K.; Kolberg, L.; Hofmann-Lehmann, R.; Meli, M.L.; et al. Curing Cats with Feline Infectious Peritonitis with an Oral Multi-Component Drug Containing GS-441524. Viruses 2021, 13, 2228. https://doi.org/10.3390/v13112228
Krentz D, Zenger K, Alberer M, Felten S, Bergmann M, Dorsch R, Matiasek K, Kolberg L, Hofmann-Lehmann R, Meli ML, et al. Curing Cats with Feline Infectious Peritonitis with an Oral Multi-Component Drug Containing GS-441524. Viruses. 2021; 13(11):2228. https://doi.org/10.3390/v13112228
Chicago/Turabian StyleKrentz, Daniela, Katharina Zenger, Martin Alberer, Sandra Felten, Michèle Bergmann, Roswitha Dorsch, Kaspar Matiasek, Laura Kolberg, Regina Hofmann-Lehmann, Marina L. Meli, and et al. 2021. "Curing Cats with Feline Infectious Peritonitis with an Oral Multi-Component Drug Containing GS-441524" Viruses 13, no. 11: 2228. https://doi.org/10.3390/v13112228
APA StyleKrentz, D., Zenger, K., Alberer, M., Felten, S., Bergmann, M., Dorsch, R., Matiasek, K., Kolberg, L., Hofmann-Lehmann, R., Meli, M. L., Spiri, A. M., Horak, J., Weber, S., Holicki, C. M., Groschup, M. H., Zablotski, Y., Lescrinier, E., Koletzko, B., von Both, U., & Hartmann, K. (2021). Curing Cats with Feline Infectious Peritonitis with an Oral Multi-Component Drug Containing GS-441524. Viruses, 13(11), 2228. https://doi.org/10.3390/v13112228