
Pathological Characteristics of a Patient with Severe Fever with Thrombocytopenia Syndrome (SFTS) Infected with SFTS Virus through a Sick Cat’s Bite

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient
2.2. Cat
2.3. Measurement of SFTSV Genome Load with Real-Time RT-PCR in Blood
2.4. Antibody Detection with Indirect Immunofluorescence Assay
2.5. Measurement of SFTSV Genome Load with Real-Time RT-PCR in Tissues
2.6. Pathological and Immunohistochemical Analyses
2.7. Ethical Statement
3. Results
3.1. Patient Presentation
3.2. Cat Presentation
3.3. Dynamics of SFTSV Loads and Immunological Responses in Sera
3.4. Pathological Findings
3.4.1. Gross Pathology
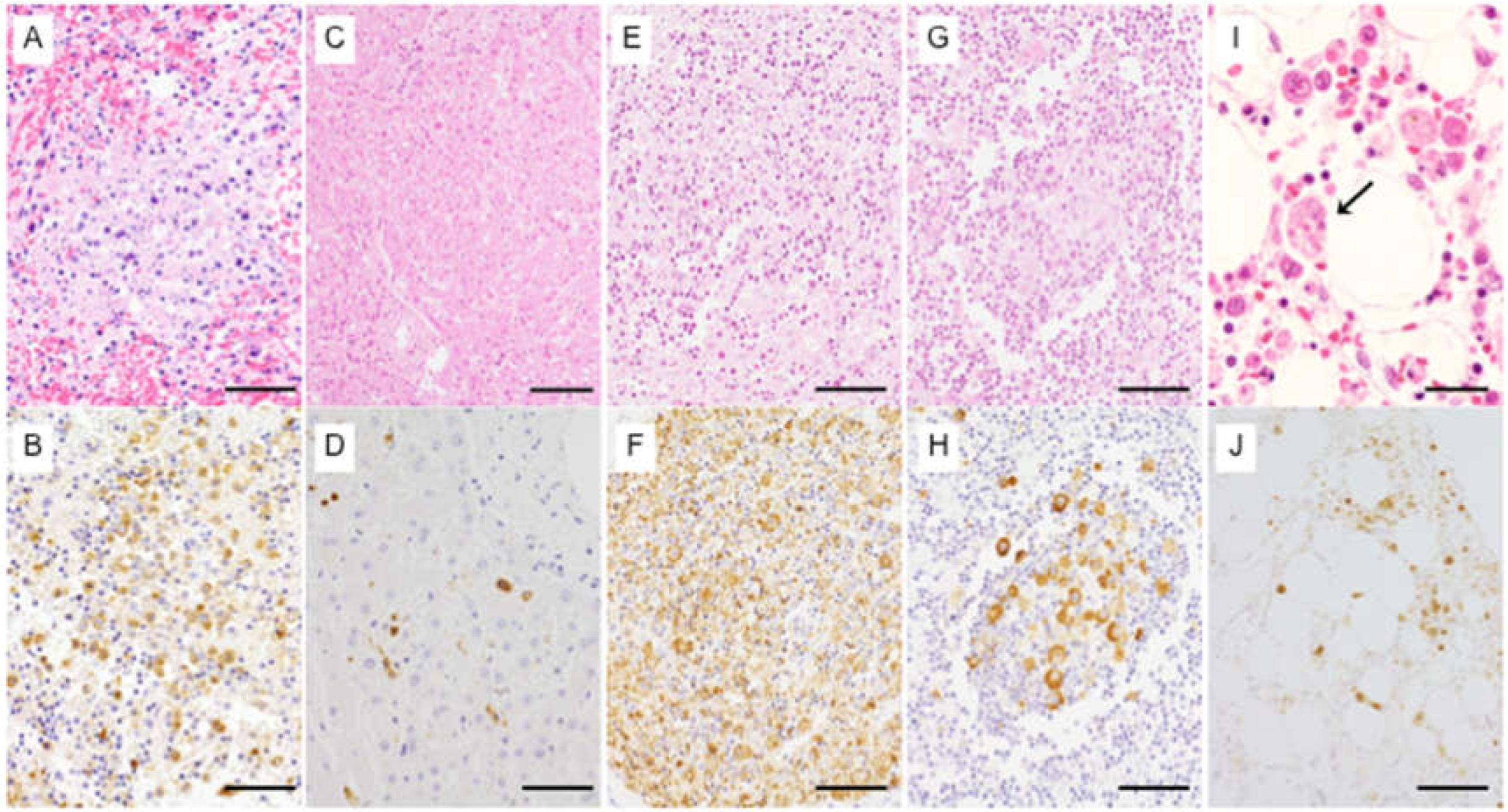
3.4.2. Histopathology and Immunohistochemistry
3.4.3. SFTSV-RNA Measurement in Organs
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Yu, X.J.; Liang, M.F.; Zhang, S.Y.; Liu, Y.; Li, J.D.; Sun, Y.L.; Zhang, L.; Zhang, Q.F.; Popov, V.L.; Li, C.; et al. Fever with thrombocytopenia associated with a novel bunyavirus in China. N. Engl. J. Med. 2011, 364, 1523–1532. [Google Scholar]
- Xu, B.; Liu, L.; Huang, X.; Ma, H.; Zhang, Y.; Du, Y.; Wang, P.; Tang, X.; Wang, H.; Kang, K.; et al. Metagenomic analysis of fever, thrombocytopenia and leukopenia syndrome (FTLS) in Henan Province, China: Discovery of a new bunyavirus. PLoS Pathog. 2011, 7, e1002369. [Google Scholar] [CrossRef]
- Takahashi, T.; Maeda, K.; Suzuki, T.; Ishido, A.; Shigeoka, T.; Tominaga, T.; Kamei, T.; Honda, M.; Ninomiya, D.; Sakai, T.; et al. The first identification and retrospective study of Severe Fever with Thrombocytopenia Syndrome in Japan. J. Infect. Dis. 2014, 209, 816–827. [Google Scholar]
- Kim, K.H.; Yi, J.; Kim, G.; Choi, S.J.; Jun, K.I.; Kim, N.H.; Choe, P.G.; Kim, N.J.; Lee, J.K.; Oh, M.D. Severe fever with thrombocytopenia syndrome, South Korea, 2012. Emerg. Infect. Dis. 2013, 19, 1892–1894. [Google Scholar] [CrossRef]
- Lin, T.L.; Ou, S.C.; Maeda, K.; Shimoda, H.; Chan, J.P.; Tu, W.C.; Hsu, W.L.; Chou, C.C. The first discovery of severe fever with thrombocytopenia syndrome virus in Taiwan. Emerg. Microbes Infect. 2020, 9, 148–151. [Google Scholar] [CrossRef]
- Tran, X.C.; Yun, Y.; Van An, L.; Kim, S.H.; Thao, N.T.P.; Man, P.K.C.; Yoo, J.R.; Heo, S.T.; Cho, N.H.; Lee, K.H. Endemic severe fever with thrombocytopenia syndrome, Vietnam. Emerg. Infect. Dis. 2019, 25, 1029–1031. [Google Scholar] [CrossRef]
- Saijo, M. Circulation of severe fever with thrombocytopenia syndrome virus (SFTSV) in nature: Transmission of SFTSV between mammals and ticks. In Severe Fever with Thrombocytopenia Syndrome; Saijo, M., Ed.; Springer: Singapore, 2019; pp. 151–172. [Google Scholar]
- Kobayashi, Y.; Kato, H.; Yamagishi, T.; Shimada, T.; Matsui, T.; Yoshikawa, T.; Kurosu, T.; Shimojima, M.; Morikawa, S.; Hasegawa, H.; et al. Severe fever with thrombocytopenia syndrome, Japan, 2013–2017. Emerg. Infect. Dis. 2020, 26, 692–699. [Google Scholar] [CrossRef] [Green Version]
- Kato, H.; Yamagishi, T.; Shimada, T.; Matsui, T.; Shimojima, M.; Saijo, M.; Oishi, K.; SFTS Epidemiological Research Group-Japan. Epidemiological and clinical features of severe fever with thrombocytopenia syndrome in Japan, 2013–2014. PLoS ONE 2016, 11, e0165207. [Google Scholar] [CrossRef]
- Matsuu, A.; Momoi, Y.; Nishiguchi, A.; Noguchi, K.; Yabuki, M.; Hamakubo, E.; Take, M.; Maeda, K. Natural severe fever with thrombocytopenia syndrome virus infection in domestic cats in Japan. Vet. Microbiol. 2019, 236, 108346. [Google Scholar]
- Matsuno, K.; Nonoue, N.; Noda, A.; Kasajima, N.; Noguchi, K.; Takano, A.; Shimoda, H.; Orba, Y.; Muramatsu, M.; Sakoda, Y.; et al. Fatal tickborne phlebovirus infection in captive cheetahs, Japan. Emerg. Infect. Dis. 2018, 24, 1726–1729. [Google Scholar] [CrossRef]
- Kida, K.; Matsuoka, Y.; Shimoda, T.; Matsuoka, H.; Yamada, H.; Saito, T.; Imataki, O.; Kadowaki, N.; Noguchi, K.; Maeda, K.; et al. A case of cat-to-human transmission of severe fever with thrombocytopenia syndrome virus. Jpn. J. Infect. Dis. 2019, 72, 356–358. [Google Scholar] [CrossRef] [Green Version]
- Yamanaka, A.; Kirino, Y.; Fujimoto, S.; Ueda, N.; Himeji, D.; Miura, M.; Sudaryatma, P.E.; Sato, Y.; Tanaka, H.; Mekata, H.; et al. Direct transmission of severe fever with thrombocytopenia syndrome virus from domestic cat to veterinary personnel. Emerg. Infect. Dis. 2020, 26, 2994–2998. [Google Scholar] [CrossRef]
- Hu, J.; Li, Z.; Cai, J.; Liu, D.; Zhang, X.; Jiang, R.; Guo, X.; Liu, D.; Zhang, Y.; Cui, L.; et al. A cluster of bunyavirus-associated severe fever with thrombocytopenia syndrome cases in a coastal plain area in China, 2015: Identification of a previously unidentified endemic region for severe fever with thrombocytopenia bunyavirus. Open Forum Infect. Dis. 2019, 6, ofz209. [Google Scholar] [CrossRef]
- Jung, I.Y.; Choi, W.; Kim, J.; Wang, E.; Park, S.W.; Lee, W.J.; Choi, J.Y.; Kim, H.Y.; Uh, Y.; Kim, Y.K. Nosocomial person-to-person transmission of severe fever with thrombocytopenia syndrome. Clin. Microbiol. Infect. 2019, 25, 633.e1–633.e4. [Google Scholar] [CrossRef]
- Jia, B.; Wu, W.; Huang, R.; Wang, G.; Song, P.; Li, Y.; Liu, Y.; Xiong, Y.; Yan, X.; Hao, Y.; et al. Characterization of clinical features and outcome for human-to-human transmitted severe fever with thrombocytopenia syndrome. Infect. Dis. 2018, 50, 601–608. [Google Scholar]
- Zhu, Y.; Wu, H.; Gao, J.; Zhou, X.; Zhu, R.; Zhang, C.; Bai, H.; Abdullah, A.S.; Pan, H. Two confirmed cases of severe fever with thrombocytopenia syndrome with pneumonia: Implication for a family cluster in East China. BMC Infect. Dis. 2017, 17, 537. [Google Scholar] [CrossRef] [Green Version]
- Tang, X.; Wu, W.; Wang, H.; Du, Y.; Liu, L.; Kang, K.; Huang, X.; Ma, H.; Mu, F.; Zhang, S.; et al. Human-to-human transmission of severe fever with thrombocytopenia syndrome bunyavirus through contact with infectious blood. J. Infect. Dis. 2013, 207, 736–739. [Google Scholar] [CrossRef] [Green Version]
- Chen, H.; Hu, K.; Zou, J.; Xiao, J. A cluster of cases of human-to-human transmission caused by severe fever with thrombocytopenia syndrome bunyavirus. Int. J. Infect. Dis. 2013, 17, e206–e208. [Google Scholar] [CrossRef] [Green Version]
- Yoshikawa, T.; Fukushi, S.; Tani, H.; Fukuma, A.; Taniguchi, S.; Toda, S.; Shimazu, Y.; Yano, K.; Morimitsu, T.; Ando, K.; et al. Sensitive and specific PCR systems for detection of both Chinese and Japanese severe fever with thrombocytopenia syndrome virus strains and prediction of patient survival based on viral load. J. Clin. Microbiol. 2014, 52, 3325–3333. [Google Scholar] [CrossRef] [Green Version]
- Fukuma, A.; Fukushi, S.; Yoshikawa, T.; Tani, H.; Taniguchi, S.; Kurosu, T.; Egawa, K.; Suda, Y.; Singh, H.; Nomachi, T.; et al. Severe fever with thrombocytopenia syndrome virus antigen detection using monoclonal antibodies to the nucleocapsid protein. PLoS Negl. Trop. Dis. 2016, 10, e0004595. [Google Scholar]
- Suzuki, T.; Sato, Y.; Sano, K.; Arashiro, T.; Katano, H.; Nakajima, N.; Shimojima, M.; Kataoka, M.; Takahashi, K.; Wada, Y.; et al. Severe fever with thrombocytopenia syndrome virus targets B cells in lethal human infections. J. Clin. Investig. 2020, 130, 799–812. [Google Scholar] [CrossRef]
- Saijo, M. Pathology of severe fever with thrombocytopenia syndrome. In Severe Fever with Thrombocytopenia Syndrome; Saijo, M., Ed.; Springer: Singapore, 2019; pp. 137–150. [Google Scholar]
- Hiraki, T.; Yoshimitsu, M.; Suzuki, T.; Goto, Y.; Higashi, M.; Yokoyama, S.; Tabuchi, T.; Futatsuki, T.; Nakamura, K.; Hasegawa, H.; et al. Two autopsy cases of severe fever with thrombocytopenia syndrome (SFTS) in Japan: A pathognomonic histological feature and unique complication of SFTS. Pathol. Int. 2014, 64, 569–575. [Google Scholar] [CrossRef]
- Kaneko, M.; Shikata, H.; Matsukage, S.; Maruta, M.; Shinomiya, H.; Suzuki, T.; Hasegawa, H.; Shimojima, M.; Saijo, M. A patient with severe fever with thrombocytopenia syndrome and hemophagocytic lymphohistiocytosis-associated involvement of the central nervous system. J. Infect. Chemother. 2018, 24, 292–297. [Google Scholar] [CrossRef]
- Nakano, A.; Ogawa, H.; Nakanishi, Y.; Fujita, H.; Mahara, F.; Shiogama, K.; Tsutsumi, Y.; Takeichi, T. Hemophagocytic lymphohistiocytosis in a fatal case of severe fever with thrombocytopenia syndrome. Intern. Med. 2017, 56, 1597–1602. [Google Scholar] [CrossRef] [Green Version]
- Uehara, N.; Yano, T.; Ishihara, A.; Saijou, M.; Suzuki, T. Fatal severe fever with thrombocytopenia syndrome: An autopsy case report. Intern. Med. 2016, 55, 831–838. [Google Scholar] [CrossRef] [Green Version]
- Park, E.S.; Shimojima, M.; Nagata, N.; Ami, Y.; Yoshikawa, T.; Iwata-Yoshikawa, N.; Fukushi, S.; Watanabe, S.; Kurosu, T.; Kataoka, M.; et al. Severe fever with thrombocytopenia syndrome phlebovirus causes lethal viral hemorrhagic fever in cats. Sci. Rep. 2019, 9, 11990. [Google Scholar]


{kind=link}
| Categories | Normal Range | Day 5 | Day 8 | Day 9 | Day 11 |
|---|---|---|---|---|---|
| Total blood cell counts | |||||
| WBC (×103 cells/µL) | 3.3–8.6 | 1.9 | 0.5 | 0.5 | 3.1 |
| Platelets (×103 cells/µL) | 158–348 | 133 | 67 | 52 | 49 |
| RBC (×106 cells/µL) | 3.86–4.92 | 4.50 | 4.67 | 4.61 | 5.14 |
| Serum chemistry | |||||
| TP (g/dL) | 6.6–8.1 | 6.8 | 6.1 | 5.4 | 5.7 |
| ALB (g/dL) | 4.1–5.1 | 4.1 | 3.5 | 3.1 | 2.9 |
| TB (mg/dL) | 0.40–1.50 | 0.64 | 0.71 | 0.58 | 1.85 |
| AST (U/L) | 13–30 | 23 | 494 | 1210 | 3784 |
| ALT (U/L) | 7–23 | 14 | 169 | 376 | 961 |
| LDH (U/L) | 124–222 | 187 | 940 | 1584 | 5021 |
| ALP (U/L) | 106–322 | 189 | 201 | 220 | 425 |
| γ-GTP (U/L) | 9–32 | 15 | 23 | 26 | 85 |
| BUN (mg/dL) | 8.0–20.0 | 14.3 | 17.6 | NT | 31.4 |
| CRE (mg/dL) | 0.46–0.79 | 0.57 | 0.58 | 0.52 | 0.90 |
| Na (mmol/L) | 138–145 | 133 | 134 | 133 | 130 |
| K (mmol/L) | 3.6–4.8 | 4.2 | 3.6 | 3.6 | 4.5 |
| Cl (mmol/L) | 101–108 | 96 | 93 | 96 | 94 |
| CRP (mg/dL)) | 0.00–0.14 | 0.04 | 0.03 | 0.06 | 0.04 |
| PT (second) | 10.5–15.5 | NT | 14.2 | 14.4 | 15.0 |
| APTT (second) | 30.0–40.0 | NT | 65.3 | 76.7 | 82.1 |
| Fibrinogen (mg/dL) | 150.0–450.0 | NT | 229.0 | NT | 203.0 |
| D-dimer (µg/mL) | 0.00–0.40 | NT | 11.51 | 12.88 | 9.07 |
| Categories | Normal Range | Values |
|---|---|---|
| Total blood cell counts | ||
| WBC (×103 cells/µL) | 2.07–17.02 | 0.87 |
| Platelet (×103 cells/µL) | 151–600 | 12 |
| RBC (×106 cells/µL) | 6.54–12.20 | 9.76 |
| Serum chemistry | ||
| TP (g/dL) | 5.2–8.2 | 7.7 |
| ALB (g/dL) | 2.2–3.9 | 2.6 |
| ALT (U/L) | 12–130 | 234 |
| ALP (U/L) | 14–192 | <10 |
| TB (mg/dL) | 0–0.9 | 5.3 |
| BUN (mg/dL) | 13–33 | 25 |
| CRE (mg/dL) | 0.6–1.6 | 1.1 |
| Na (mmol/L) | 150–165 | 149 |
| K (mmol/L) | 3.7–5.9 | 3.1 |
| Cl (mmol/L) | 115–156 | 110 |
| Urinalysis | ||
| Protein | Negative | ++ |
| Hematuria | Negative | +++ |
| Tissue Section | Measurement of SFTSV Genome with Quantitative Real-Time Reverse Transcription PCR Assay | IHC | ||
|---|---|---|---|---|
| SFTSV RNA (Copies/Reaction) | β-Actin (Copies/Reaction) | Copies/Cell * | (SFTSV-NP) | |
| Spleen | 4.73 × 104 | 7.96 × 103 | 8.91 × 103 | ++++ |
| Liver | 2.53 × 103 | 5.81 × 103 | 6.53 × 102 | ++ |
| Adrenal gland | 6.08 × 101 | 1.98 × 103 | 4.62 × 101 | ++ |
| Bone marrow | 1.23 × 100 | 4.36 × 101 | 4.24 × 101 | ++ |
| Left subclavian lymph node | 2.08 × 102 | 8.83 × 103 | 3.54 × 101 | ++ |
| Lung | 9.52 × 101 | 5.85 × 103 | 2.44 × 101 | + |
| Thyroid | 4.02 × 101 | 4.80 × 103 | 1.26 × 101 | + |
| Mesenteric lymph node | 3.88 × 101 | 4.99 × 103 | 1.17 × 101 | ++ |
| Kidney | 4.81 × 101 | 8.51 × 103 | 8.48 × 101 | + |
| Subcarinal lymph node | 1.90 × 101 | 6.19 × 103 | 4.61 × 101 | ++ |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tsuru, M.; Suzuki, T.; Murakami, T.; Matsui, K.; Maeda, Y.; Yoshikawa, T.; Kurosu, T.; Shimojima, M.; Shimada, T.; Hasegawa, H.; et al. Pathological Characteristics of a Patient with Severe Fever with Thrombocytopenia Syndrome (SFTS) Infected with SFTS Virus through a Sick Cat’s Bite. Viruses 2021, 13, 204. https://doi.org/10.3390/v13020204
Tsuru M, Suzuki T, Murakami T, Matsui K, Maeda Y, Yoshikawa T, Kurosu T, Shimojima M, Shimada T, Hasegawa H, et al. Pathological Characteristics of a Patient with Severe Fever with Thrombocytopenia Syndrome (SFTS) Infected with SFTS Virus through a Sick Cat’s Bite. Viruses. 2021; 13(2):204. https://doi.org/10.3390/v13020204
Chicago/Turabian StyleTsuru, Masatoshi, Tadaki Suzuki, Tomoyuki Murakami, Kumiko Matsui, Yuuji Maeda, Tomoki Yoshikawa, Takeshi Kurosu, Masayuki Shimojima, Tomome Shimada, Hideki Hasegawa, and et al. 2021. "Pathological Characteristics of a Patient with Severe Fever with Thrombocytopenia Syndrome (SFTS) Infected with SFTS Virus through a Sick Cat’s Bite" Viruses 13, no. 2: 204. https://doi.org/10.3390/v13020204
APA StyleTsuru, M., Suzuki, T., Murakami, T., Matsui, K., Maeda, Y., Yoshikawa, T., Kurosu, T., Shimojima, M., Shimada, T., Hasegawa, H., Maeda, K., Morikawa, S., & Saijo, M. (2021). Pathological Characteristics of a Patient with Severe Fever with Thrombocytopenia Syndrome (SFTS) Infected with SFTS Virus through a Sick Cat’s Bite. Viruses, 13(2), 204. https://doi.org/10.3390/v13020204