
Recent Hydroxychloroquine Use Is Not Significantly Associated with Positive PCR Results for SARS-CoV-2: A Nationwide Observational Study in South Korea

 , , ,
, , ,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Database
2.2. Patient Consent Statement
2.3. Definitions
2.4. Statistical Analysis
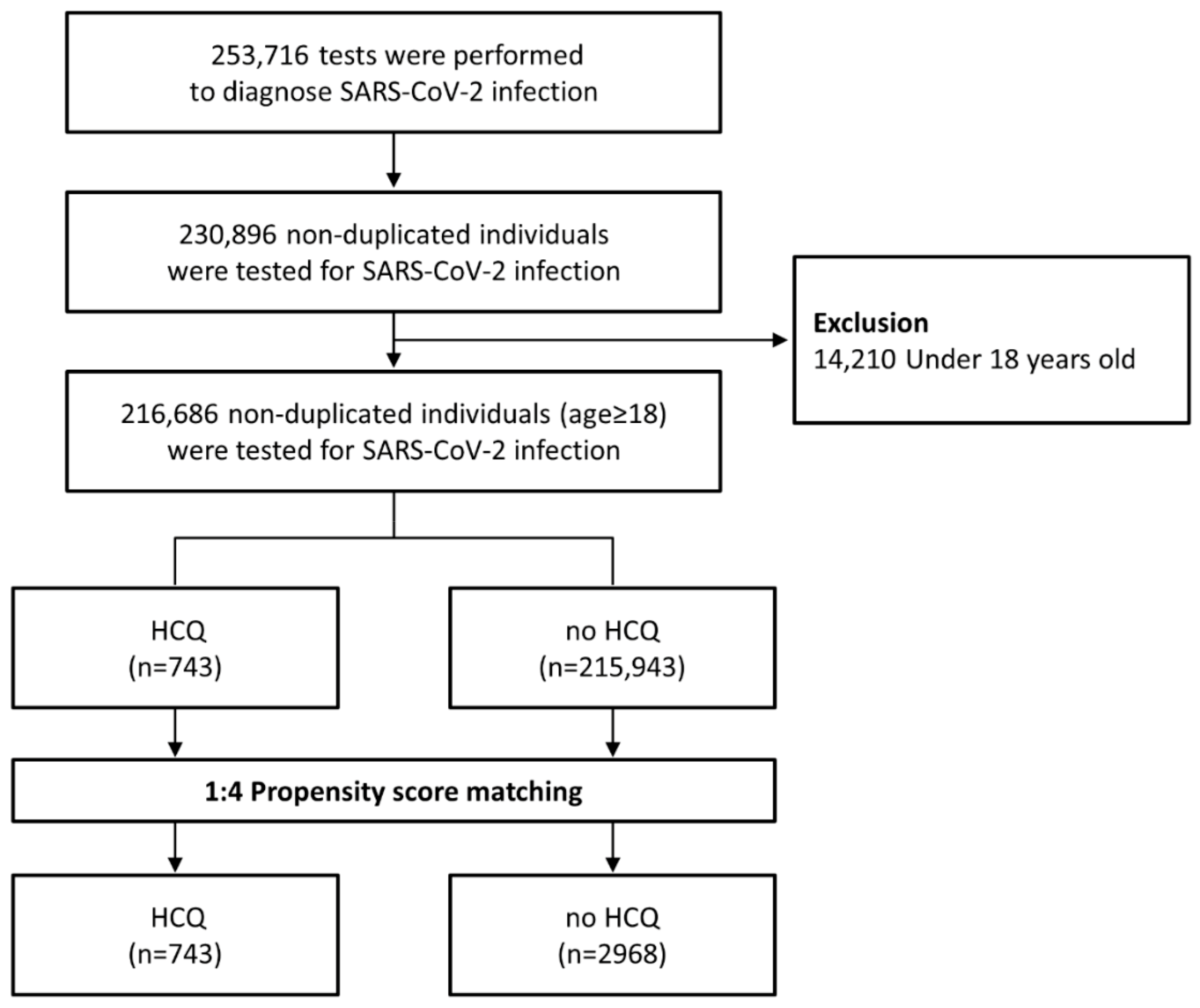
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Parks, J.M.; Smith, J.C. How to Discover Antiviral Drugs Quickly. N. Engl. J. Med. 2020, 382, 2261–2264. [Google Scholar] [CrossRef]
- Martinez, M.A. Compounds with Therapeutic Potential against Novel Respiratory 2019 Coronavirus. Antimicrob. Agents Chemother. 2020. [Google Scholar] [CrossRef] [Green Version]
- Kupferschmidt, K.; Cohen, J. Race to find COVID-19 treatments accelerates. Science 2020, 367, 1412–1413. [Google Scholar] [CrossRef] [Green Version]
- Lima, W.G.; Brito, J.C.M.; Overhage, J.; Nizer, W. The potential of drug repositioning as a short-term strategy for the control and treatment of COVID-19 (SARS-CoV-2): A systematic review. Arch. Virol. 2020, 165, 1729–1737. [Google Scholar] [CrossRef] [PubMed]
- Beigel, J.H.; Tomashek, K.M.; Dodd, L.E.; Mehta, A.K.; Zingman, B.S.; Kalil, A.C.; Hohmann, E.; Chu, H.Y.; Luetkemeyer, A.; Kline, S.; et al. Remdesivir for the Treatment of Covid-19—Preliminary Report. N. Engl. J. Med. 2020, 383, 1813–1826. [Google Scholar] [CrossRef] [PubMed]
- Hung, I.F.; Lung, K.C.; Tso, E.Y.; Liu, R.; Chung, T.W.; Chu, M.Y.; Ng, Y.-Y.; Lo, J.; Chan, J.; Tam, A.R.; et al. Triple combination of interferon beta-1b, lopinavir-ritonavir, and ribavirin in the treatment of patients admitted to hospital with COVID-19: An open-label, randomised, phase 2 trial. Lancet 2020, 395, 1695–1704. [Google Scholar] [CrossRef]
- Vincent, M.J.; Bergeron, E.; Benjannet, S.; Erickson, B.R.; Rollin, P.E.; Ksiazek, T.G.; Seidah, N.G.; Nichol, S.T. Chloroquine is a potent inhibitor of SARS coronavirus infection and spread. Virol. J. 2005, 2, 69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, M.; Cao, R.; Zhang, L.; Yang, X.; Liu, J.; Xu, M.; Shi, Z.; Hu, Z.; Zhong, W.; Xiao, G. Remdesivir and chloroquine effectively inhibit the recently emerged novel coronavirus (2019-nCoV) in vitro. Cell Res. 2020, 30, 269–271. [Google Scholar] [CrossRef]
- Yao, X.; Ye, F.; Zhang, M.; Cui, C.; Huang, B.; Niu, P.; Liu, X.; Zhao, L.; Dong, E.; Song, C.; et al. In Vitro Antiviral Activity and Projection of Optimized Dosing Design of Hydroxychloroquine for the Treatment of Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2). Clin. Infect. Dis. 2020, 71, 732–739. [Google Scholar] [CrossRef] [Green Version]
- Gao, J.; Tian, Z.; Yang, X. Breakthrough: Chloroquine phosphate has shown apparent efficacy in treatment of COVID-19 associated pneumonia in clinical studies. Biosci. Trend 2020, 14, 72–73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gautret, P.; Lagier, J.C.; Parola, P.; Hoang, V.T.; Meddeb, L.; Mailhe, M.; Doudier, B.; Courjon, J.; Giordanengo, V.; Vieira, V.E.; et al. Hydroxychloroquine and azithromycin as a treatment of COVID-19: Results of an open-label non-randomized clinical trial. Int. J. Antimicrob. Agents 2020, 56, 105949. [Google Scholar] [CrossRef]
- Mahévas, M.; Tran, V.T.; Roumier, M.; Chabrol, A.; Paule, R.; Guillaud, C.; Fois, E.; Lepeule, R.; Szwebel, T.-A.; Lescure, F.-X.; et al. Clinical efficacy of hydroxychloroquine in patients with covid-19 pneumonia who require oxygen: Observational comparative study using routine care data. BMJ 2020, 369, m1844. [Google Scholar]
- Tang, W.; Cao, Z.; Han, M.; Wang, Z.; Chen, J.; Sun, W.; Wu, Y.; Xiao, W.; Liu, S.; Chen, E.; et al. Hydroxychloroquine in patients with mainly mild to moderate coronavirus disease 2019: Open label, randomised controlled trial. BMJ 2020, 369, m1849. [Google Scholar] [CrossRef]
- Boulware, D.R.; Pullen, M.F.; Bangdiwala, A.S.; Pastick, K.A.; Lofgren, S.M.; Okafor, E.C.; Skipper, C.P.; Nascene, A.A.; Nicol, M.R.; Abassi, M.; et al. A Randomized Trial of Hydroxychloroquine as Postexposure Prophylaxis for Covid-19. N. Engl. J. Med. 2020, 383, 517–525. [Google Scholar] [CrossRef] [PubMed]
- Schrezenmeier, E.; Dörner, T. Mechanisms of action of hydroxychloroquine and chloroquine: Implications for rheumatology. Nat. Rev. Rheumatol. 2020, 16, 155–166. [Google Scholar] [CrossRef] [PubMed]
- Tan, K.R.; Magill, A.J.; Parise, M.E.; Arguin, P.M. Doxycycline for malaria chemoprophylaxis and treatment: Report from the CDC expert meeting on malaria chemoprophylaxis. Am. J. Trop. Med. Hyg. 2011, 84, 517–531. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Monti, S.; Balduzzi, S.; Delvino, P.; Bellis, E.; Quadrelli, V.S.; Montecucco, C. Clinical course of COVID-19 in a series of patients with chronic arthritis treated with immunosuppressive targeted therapies. Ann. Rheum. Dis. 2020, 79, 667–668. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lahouati, M.; Mériglier, E.; Martin, L.; Bouchet, S.; Desclaux, A.; Bonnet, F. COVID-19 infection also occurs in patients taking hydroxychloroquine. J. Antimicrob. Chemother. 2020, 75, 2014–2015. [Google Scholar] [CrossRef]
- Ahn, B.Y.; Kang, C.K.; Seo, J.D.; Choe, P.G.; Song, S.H.; Park, W.B.; Park, S.W.; Kim, N.J.; Oh, M.-D. A Case of Breakthrough COVID-19 during Hydroxychloroquine Maintenance. J. Korean Med. Sci. 2020, 35, e231. [Google Scholar] [CrossRef]
- Abella, B.S.; Jolkovsky, E.L.; Biney, B.T.; Uspal, J.E.; Hyman, M.C.; Frank, I.; Hensley, S.E.; Gill, S.; Vogl, D.T.; Maillard, I.; et al. Efficacy and Safety of Hydroxychloroquine vs Placebo for Pre-exposure SARS-CoV-2 Prophylaxis Among Health Care Workers: A Randomized Clinical Trial. JAMA Intern. Med. 2020. [Google Scholar] [CrossRef]
- Rajasingham, R.; Bangdiwala, A.S.; Nicol, M.R.; Skipper, C.P.; Pastick, K.A.; Axelrod, M.L.; Pullen, M.F.; Nascene, A.; Williams, D.; Engen, N.W.; et al. Hydroxychloroquine as pre-exposure prophylaxis for COVID-19 in healthcare workers: A randomized trial. Clin. Infect. Dis. 2020. [Google Scholar] [CrossRef] [PubMed]
- Mavrikakis, M.; Papazoglou, S.; Sfikakis, P.P.; Vaiopoulos, G.; Rougas, K. Retinal toxicity in long term hydroxychloroquine treatment. Ann. Rheum. Dis. 1996, 55, 187–189. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cipriani, A.; Zorzi, A.; Ceccato, D.; Capone, F.; Parolin, M.; Donato, F.; Fioretto, P.; Pesavento, R.; Previato, L.; Maffei, P.; et al. Arrhythmic profile and 24-hour QT interval variability in COVID-19 patients treated with hydroxychloroquine and azithromycin. Int. J. Cardiol. 2020, 316, 280–284. [Google Scholar] [CrossRef]
- Chorin, E.; Wadhwani, L.; Magnani, S.; Dai, M.; Shulman, E.; Nadeau-Routhier, C.; Knotts, R.; Bar-Cohen, R.; Kogan, E.; Barbhaiya, C.; et al. QT interval prolongation and torsade de pointes in patients with COVID-19 treated with hydroxychloroquine/azithromycin. Heart Rhythm 2020, 17, 1425–1433. [Google Scholar] [CrossRef]
- Mercuro, N.J.; Yen, C.F.; Shim, D.J.; Maher, T.R.; McCoy, C.M.; Zimetbaum, P.J.; Gold, H.S. Risk of QT interval prolongation associated with use of hydroxychloroquine with or without concomitant azithromycin among hospitalized patients testing positive for Coronavirus Disease 2019 (COVID-19). JAMA Cardiol. 2020, 5, 1036–1041. [Google Scholar] [CrossRef]
- Peck, K.R. Early diagnosis and rapid isolation: Response to COVID-19 outbreak in Korea. Clin. Microbiol. Infect. 2020, 26, 805–807. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| n (%) | |
|---|---|
| Patients Tested for SARS-CoV-2 | |
| Characteristics | (n = 216,686) |
| Age, mean (SD), y | 49.4 (19.9) |
| <50 | 115,759 (53.4) |
| ≥50 | 100,927 (46.6) |
| Sex | |
| Male | 102,754 (47.4) |
| Female | 113,932 (52.6) |
| Insurance type | |
| National health insurance | 204,421 (94.3) |
| Medicaid and veteran health care | 12,265 (5.7) |
| Region a | |
| Seoul metropolitan area | 108,570 (50.1) |
| Daegu–Gyeongbuk | 34,309 (15.8) |
| Other | 73,807 (34.1) |
| Underlying diseases | |
| Hypertension | 60,441 (27.9) |
| Dyslipidemia | 59,735 (27.6) |
| Chronic lung diseases | 49,203 (22.7) |
| Diabetes | 35,636 (16.4) |
| Solid tumor | 22,571 (10.4) |
| Ischemic heart disease | 15,290 (7.1) |
| Heart failure | 13,086 (6) |
| Chronic kidney disease | 9665 (4.5) |
| Liver cirrhosis | 3144 (1.5) |
| Depression | 2511 (1.2) |
| Inflammatory bowel disease | 685 (0.3) |
| Hematologic malignancy | 1552 (0.7) |
| Solid-organ transplantation | 1220 (0.6) |
| Rheumatic diseases | |
| Systemic lupus erythematosus | 465 (0.2) |
| Rheumatoid arthritis | 4152 (1.9) |
| Spondyloarthropathy | 526 (0.2) |
| Immunosuppressants use | |
| Biologics | 43 (0.02) |
| Corticosteroid | 8478 (3.9) |
| Other | 2656 (1.2) |
| Outcome | |
| Positive test result for SARS-CoV-2 | 5881 (2.7) |
| Mortality due to COVID-19 | 140/5881 (2.3) |
| Before Matching, n (%) | After 1:4 Matching, n (%) | |||||||
|---|---|---|---|---|---|---|---|---|
| Characteristics | HCQ Users (n = 743) | Nonusers (n = 215,943) | P | SDM | HCQ Users (n = 743) | Nonusers (n = 2968) | P | SDM |
| Age, mean (SD), y | 56.6 (17.1) | 49.4 (19.9) | <0.001 | 0.388 | 56.6 (17.1) | 57.3 (17.4) | 0.35 | −0.039 |
| <50 | 250 (33.6) | 115,509 (53.5) | <0.001 | −0.408 | 250 (33.6) | 970 (32.7) | 0.62 | 0.021 |
| ≥50 | 493 (66.4) | 100,434 (46.5) | 493 (66.4) | 1998 (67.3) | ||||
| Sex | ||||||||
| Male | 134 (18.0) | 102,620 (47.5) | <0.001 | −0.662 | 134 (18.0) | 536 (18.1) | >0.99 | −0.001 |
| Female | 609 (82.0) | 113,323 (52.5) | 609 (82.0) | 2432 (81.9) | ||||
| Insurance type | ||||||||
| National health insurance | 677 (91.1) | 203,744 (94.4) | <0.001 | −0.125 | 677 (91.1) | 2723 (91.7) | 0.58 | −0.022 |
| Medicaid and veteran healthcare | 66 (8.9) | 12,199 (5.6) | 66 (8.9) | 245 (8.3) | ||||
| Underlying diseases | ||||||||
| Hypertension | 340 (45.8) | 60,101 (27.8) | <0.001 | 0.378 | 340 (45.8) | 1312 (44.2) | 0.45 | 0.031 |
| Dyslipidemia | 410 (55.2) | 59,325 (27.5) | <0.001 | 0.586 | 410 (55.2) | 1709 (57.6) | 0.24 | −0.048 |
| Chronic lung diseases | 276 (37.1) | 48,927 (22.7) | <0.001 | 0.321 | 276 (37.1) | 1139 (38.4) | 0.54 | −0.025 |
| Diabetes | 165 (22.2) | 35,471 (16.4) | <0.001 | 0.147 | 165 (22.2) | 660 (22.2) | >0.99 | −0.001 |
| Solid tumor | 88 (11.8) | 22,483 (10.4) | 0.20 | 0.046 | 88 (11.8) | 382 (12.9) | 0.45 | −0.031 |
| Ischemic heart disease | 81 (10.9) | 15,209 (7) | <0.001 | 0.135 | 81 (10.9) | 295 (9.9) | 0.44 | 0.032 |
| Heart failure | 84 (11.3) | 13,002 (6) | <0.001 | 0.189 | 84 (11.3) | 292 (9.8) | 0.24 | 0.048 |
| Chronic kidney disease | 75 (10.1) | 9590 (4.4) | <0.001 | 0.219 | 75 (10.1) | 243 (8.2) | 0.10 | 0.066 |
| Liver cirrhosis | 19 (2.6) | 3125 (1.4) | 0.01 | 0.079 | 19 (2.6) | 50 (1.7) | 0.12 | 0.061 |
| Depression | 14 (1.9) | 2497 (1.2) | 0.06 | 0.06 | 14 (1.9) | 53 (1.8) | 0.86 | 0.007 |
| Inflammatory bowel disease | 2 (0.3) | 683 (0.3) | 0.82 | −0.009 | 2 (0.3) | 5 (0.2) | 0.57 | 0.022 |
| Hematologic malignancy | 11 (1.5) | 1541 (0.7) | 0.01 | 0.074 | 11 (1.5) | 41 (1.4) | 0.84 | 0.008 |
| Solid-organ transplantation | 7 (0.9) | 1213 (0.6) | 0.17 | 0.044 | 7 (0.9) | 17 (0.6) | 0.30 | 0.043 |
| Rheumatic diseases | ||||||||
| Systemic lupus erythematosus | 231 (31.1) | 234 (0.1) | <0.001 | 0.944 | 231 (31.1) | 12 (0.4) | <0.001 | 0.929 |
| Rheumatoid arthritis | 533 (71.7) | 3619 (1.7) | <0.001 | 2.116 | 533 (71.7) | 107 (3.6) | <0.001 | 1.977 |
| Spondyloarthropathy | 6 (0.8) | 520 (0.2) | 0.002 | 0.079 | 6 (0.8) | 10 (0.3) | 0.11 | 0.062 |
| Immunosuppressant use | ||||||||
| Biologics | 1 (0.1) | 42 (0) | 0.14 | 0.042 | 1 (0.1) | 0 (0) | 0.20 | 0.052 |
| Corticosteroid | 447 (60.2) | 8031 (3.7) | <0.001 | 1.521 | 447 (60.2) | 166 (5.6) | <0.001 | 1.427 |
| Other | 294 (39.6) | 2362 (1.1) | <0.001 | 1.088 | 294 (39.6) | 50 (1.7) | <0.001 | 1.060 |
| Outcome | ||||||||
| Positive test result for SARS-CoV-2 | 16 (2.2) | 5865 (2.7) | 0.35 | 16 (2.2) | 91 (3.1) | 0.18 | ||
| Mortality due to COVID-19 | 0/16 (0) | 140/5865 (2.4) | >0.99 | 0/16 (0) | 0/91 (0) | >0.99 | ||
| Odds Ratio | 95% CI | P | |
|---|---|---|---|
| Primary Analysis (HCQ ≥ 1 Month) | |||
| Unadjusted analysis | 0.79 | 0.48–1.30 | 0.35 |
| PS-matching cohort | |||
| unadjusted | 0.69 | 0.40–1.19 | 0.18 |
| Adjusted for region a | 0.80 | 0.43–1.52 | 0.50 |
| Adjusted for immunosuppressant use b | 0.69 | 0.34–1.38 | 0.29 |
| Sensitivity Analyses | |||
| Unadjusted analysis | |||
| HCQ ≥ 3 months | 0.74 | 0.43–1.25 | 0.26 |
| HCQ ≥ 6 months | 0.78 | 0.45–1.35 | 0.37 |
| PS-matching cohort | |||
| HCQ ≥ 3 months | 0.69 | 0.39–1.22 | 0.20 |
| HCQ ≥ 6 months | 0.59 | 0.32–1.07 | 0.08 |
| Odds Ratio | 95% CI | P | |
|---|---|---|---|
| Primary Analysis (HCQ ≥ 1 Month) | |||
| Unadjusted analysis | 0.93 | 0.53–1.63 | 0.79 |
| PS matching cohort | |||
| unadjusted | 0.85 | 0.48–1.53 | 0.59 |
| Adjusted for region a | 1.07 | 0.55–2.07 | 0.85 |
| Adjusted for immunosuppressant use b | 0.84 | 0.45–1.54 | 0.57 |
| Sensitivity Analyses | |||
| HCQ ≥ 3 months | 0.85 | 0.46–1.54 | 0.58 |
| HCQ ≥ 6 months | 0.88 | 0.47–1.64 | 0.68 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bae, S.; Ghang, B.; Kim, Y.-J.; Lim, J.S.; Yun, S.-C.; Kim, Y.-G.; Lee, S.-O.; Kim, S.-H. Recent Hydroxychloroquine Use Is Not Significantly Associated with Positive PCR Results for SARS-CoV-2: A Nationwide Observational Study in South Korea. Viruses 2021, 13, 329. https://doi.org/10.3390/v13020329
Bae S, Ghang B, Kim Y-J, Lim JS, Yun S-C, Kim Y-G, Lee S-O, Kim S-H. Recent Hydroxychloroquine Use Is Not Significantly Associated with Positive PCR Results for SARS-CoV-2: A Nationwide Observational Study in South Korea. Viruses. 2021; 13(2):329. https://doi.org/10.3390/v13020329
Chicago/Turabian StyleBae, Seongman, Byeongzu Ghang, Ye-Jee Kim, Joon Seo Lim, Sung-Cheol Yun, Yong-Gil Kim, Sang-Oh Lee, and Sung-Han Kim. 2021. "Recent Hydroxychloroquine Use Is Not Significantly Associated with Positive PCR Results for SARS-CoV-2: A Nationwide Observational Study in South Korea" Viruses 13, no. 2: 329. https://doi.org/10.3390/v13020329
APA StyleBae, S., Ghang, B., Kim, Y. -J., Lim, J. S., Yun, S. -C., Kim, Y. -G., Lee, S. -O., & Kim, S. -H. (2021). Recent Hydroxychloroquine Use Is Not Significantly Associated with Positive PCR Results for SARS-CoV-2: A Nationwide Observational Study in South Korea. Viruses, 13(2), 329. https://doi.org/10.3390/v13020329