2. Materials and Methods
2.1. Subjects
Of the approximately 2000 employees, only 1000 participated in this study, including 171 doctors, 497 nurses, 198 other healthcare professionals, and 134 office workers (male/female ratio: 276/724; age: median 34 years, range 21–69 years).
Nine patients with COVID-19, who had been treated in inpatient settings at the OGMC and had already recovered, were recruited as positive controls, and their blood samples were collected from 5th June to 7th July, approximately 22–89 (median 65) days after symptom onset. Six patients had been treated with respirators, and one of them had extracorporeal membrane oxygenation (ECMO). As negative controls, 186 blood donor samples, frozen for more than 10 years, were used.
2.2. Ethics Approval
This study was approved by the Ethics Committee of OGMC, and written informed consent was obtained from all participants, including the patients with COVID-19.
2.3. Radioligand Assay (RLA)
RLA was used to detect the antibody against the nucleocapsid protein (N) of SARS-CoV-2 (the antigen) [
1,
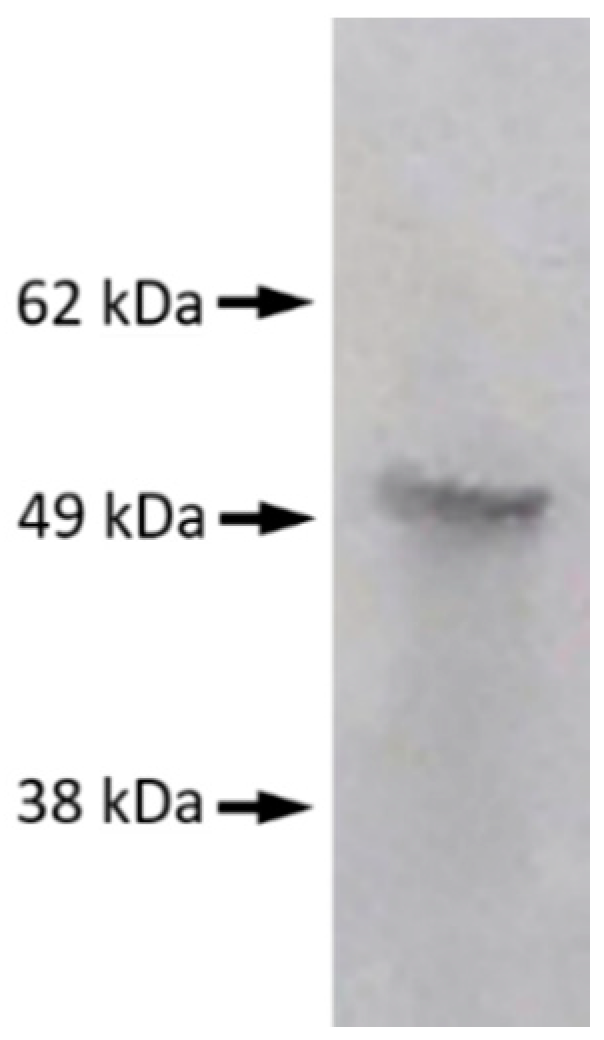
2]. cDNA encoding SARS-CoV-2 N with a His-tag and a T7-tag at the N-terminal was inserted into pET28a. Since N contains 7 methionine residues and T7-tag contains 3, a total of 10 35S-methionine per molecule could play the role of a marker for the protein. In-vitro transcription and translation were conducted using a reticulocyte lysate kit (TNT Quick Coupled Transcription/Translation SystemTM, Promega, Madison, WI, USA) and 35-S-methionine (Perkin Elmer, Waltham, MA, USA) by incubating at 30 °C for 90 min and radiolabeled N protein was separated from that with unincorporated 35S-methionine using a column (Nick ColumnTM, Cytiva, Marlborough, MA, USA). Products were analyzed by SDS-PAGE and autoradiographed to demonstrate the presence of SARS-CoV-2 N (
Figure 1). Tris-buffered saline with 0.1% bovine serum albumin and 0.1% Tween 20 was used for the antigen-antibody reaction. Ninety-six well-containing filter plates (MultiScreenTM, Merk, Darmstadt, Germany) were used as containers of a 50-µL reaction mixture, including 1 µL of serum. Resin adsorbing human IgG (Protein G Sepharose 4 Fast FlowTM, Cytiva, Marlborough, MA, USA) was added to precipitate the antigen-antibody complex. After incubation, the precipitate was washed with Tris-buffered saline containing 1% Tween 20 four times in one hour by aspirating the buffer through the filter at the bottom of the wells. After drying, the scintillation cocktail (Optiphase SuperMixTM, Perkin Elmer Life Science, Boston, MA, USA) was added, and radioactivities were counted.
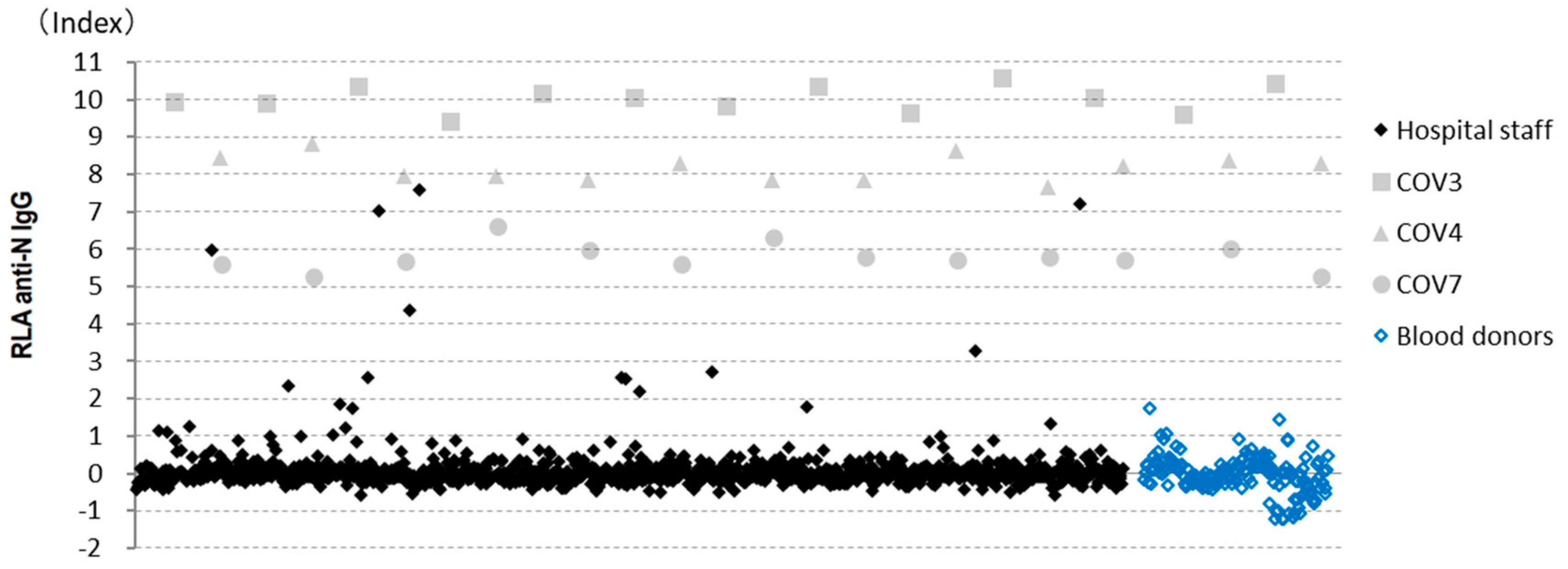
Three samples with different antibody titers from patients with COVID-19 were used as positive controls. To reduce the difference between assays, the index value was used; the average of the negative samples in the plate, excluding those with high or slightly high values, was considered to have an index value of 0, and the average from three positive controls was determined to have an index value of 8. The mean (standard deviation) index value of negative samples within each plate became 0 (0.2–0.3), and the mean (standard deviation) index value of the three positive samples in all 13 plates tested was 10.13 (0.57), 8.33 (0.03), and 5.63 (0.54), respectively.
2.4. Enzyme-Linked Immunosorbent Assays (ELISA)
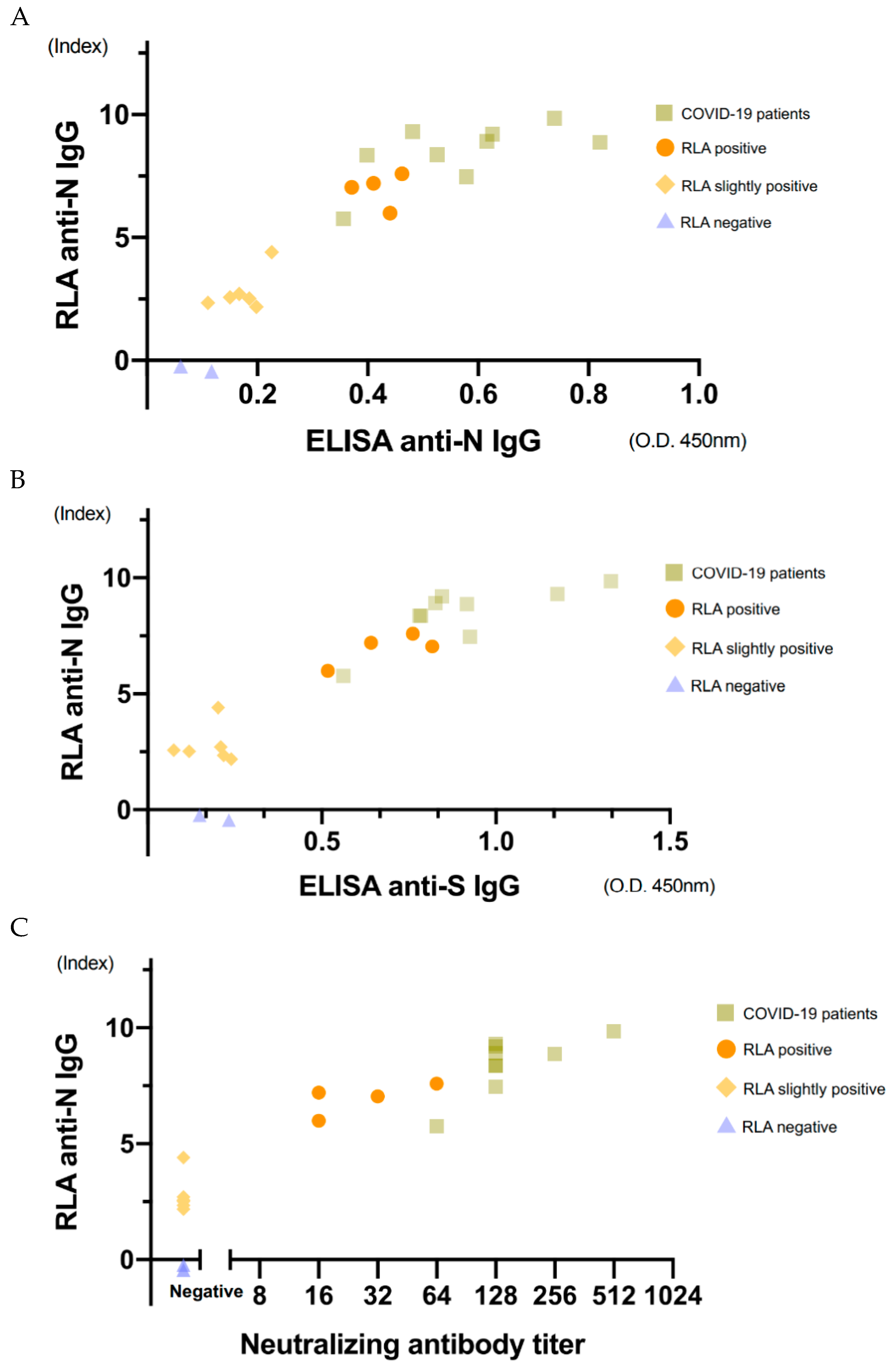
To validate the RLA results, ELISA and neutralizing antibody titration were performed for 21 selected samples, including nine from patients with COVID-19, and four apparently positive, six slightly high, and two negative samples from hospital staff. Anti-SARS-CoV-2 N IgG and anti-SARS-CoV-2 S IgG in the sera were measured using Novel Coronavirus COVID-19 IgG ELISA TM(DRG International, Inc., Springfield, NJ, USA) and COVID-19 Human IgM IgG ELISA kit (Spike protein)TM (CELLSPECT, Morioka, Japan), according to the manufacturer’s protocol.
2.5. Neutralization Assay
One hundred TCID50 of SARS-CoV-2/ Japan/UT-NCGM02 was reacted with 2-fold serial diluted serum at 37 °C for 1 h. The mixture was overlaid onto Vero E6/TMPRSS2 cells for 1 h. After washing, the inoculated cells were cultured in Dulbecco’s Modified Eagle’s Medium (Thermo Fisher Scientific, Waltham, MA, USA) with 2% FCS. Three days post-infection, the neutralizing antibody titer was determined by observation of the cytopathic effect.
2.6. Chemiluminescence Immunoassay (CLIA)
To further validate the RLA results, CLIA measurements using an automatic analyzer were also performed because it had been validated by other researchers [
3,
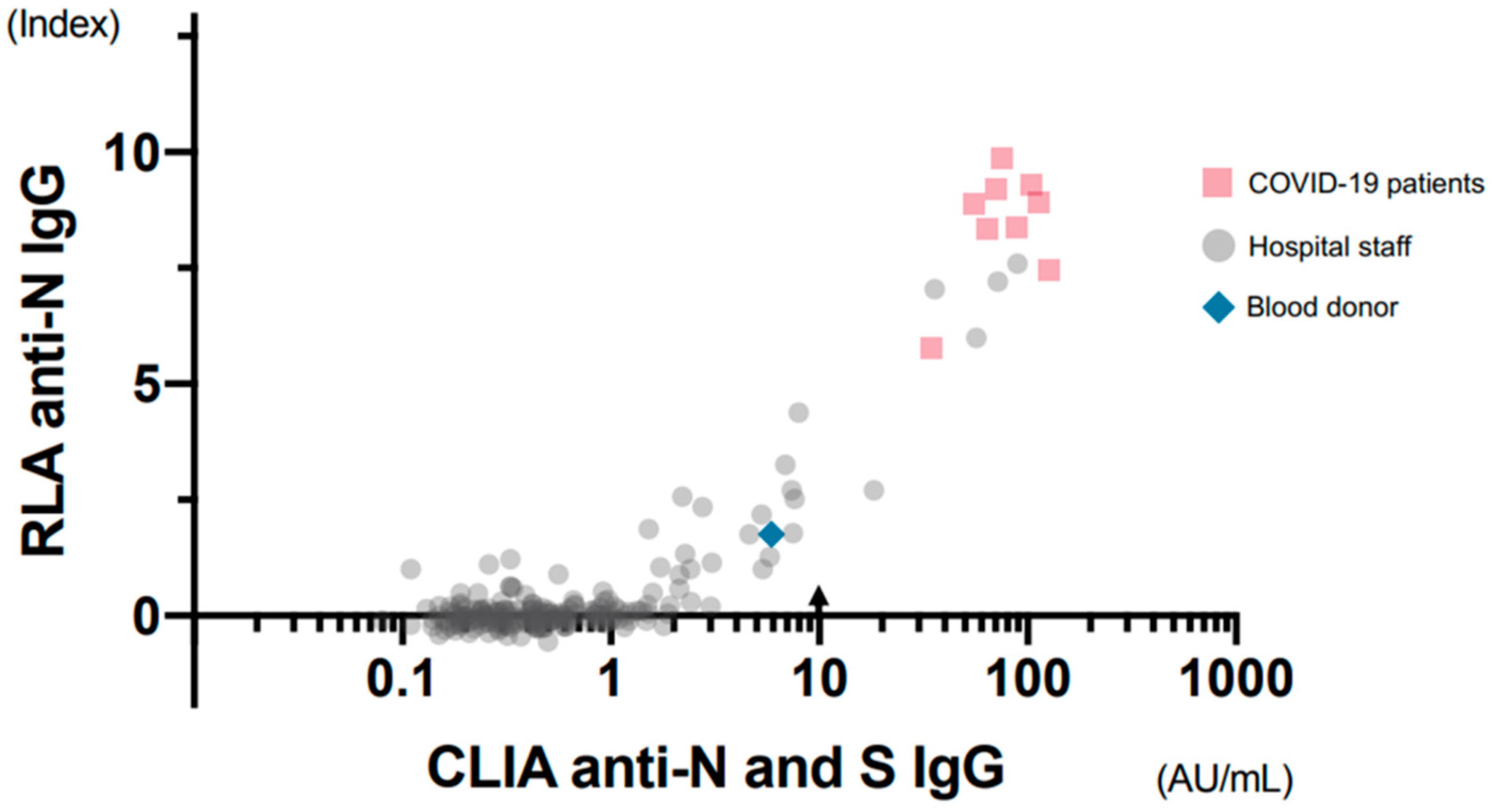
4] and was available for research use. For CLIA, 201 samples were selected, including nine samples from patients with COVID-19, all 22 samples from the hospital staff having 1.0 or more index values by RLA, 169 negative samples having less than 1.0 index values by RIA from the hospital staff, and one blood donor sample with slightly high counts. CLIA was performed using a fully automatic analyzer (iFlashTM, YHLO Biotechnology Company Ltd., Shenzhen, China). In this assay system, magnetic beads coated with SARS-CoV-2 N and S were used as the antigens.
2.7. Statistical Analysis
To compare the correlation between the results of the two methods, Spearman’s rank correlation coefficient was used.
4. Discussion
Various commercialized kits have been developed to date for testing anti-SARS-CoV-2 antibodies; however, we measured the anti-N IgG using RLA. RLA was first introduced in 1997 by Yamamoto et al. [
5] to detect autoantibodies against cytochrome CYP2D6, which causes autoimmune hepatitis, more sensitively than immunoblotting and ELISA. In RLA, the antigen contains 35S-labeled methionine as a marker, and hence, no additional chemical agent is required for luminescence or color development. Radioactivity is a marker of the antigen, and even small amounts of it can be detected accurately. Moreover, the antigen can be mixed with serum in the liquid phase without immobilization. Since the antigen completely preserves the natural conformation, a conformational antibody can be detected. We had previously attempted to detect autoantibodies against neurotransmitter receptors [
6], after which we used the same method to measure antibodies against Borna disease virus [
1,
2]. Since the Borna disease virus infects human nervous cells latently and persistently, the titers of specific antibodies were relatively low. Therefore, it is difficult to obtain consistent results using various antibody detection methods. In our experience, RLA seems to be quite sensitive, quantitative, and reproducible, and can potentially be used as an excellent tool for measuring antibodies precisely.
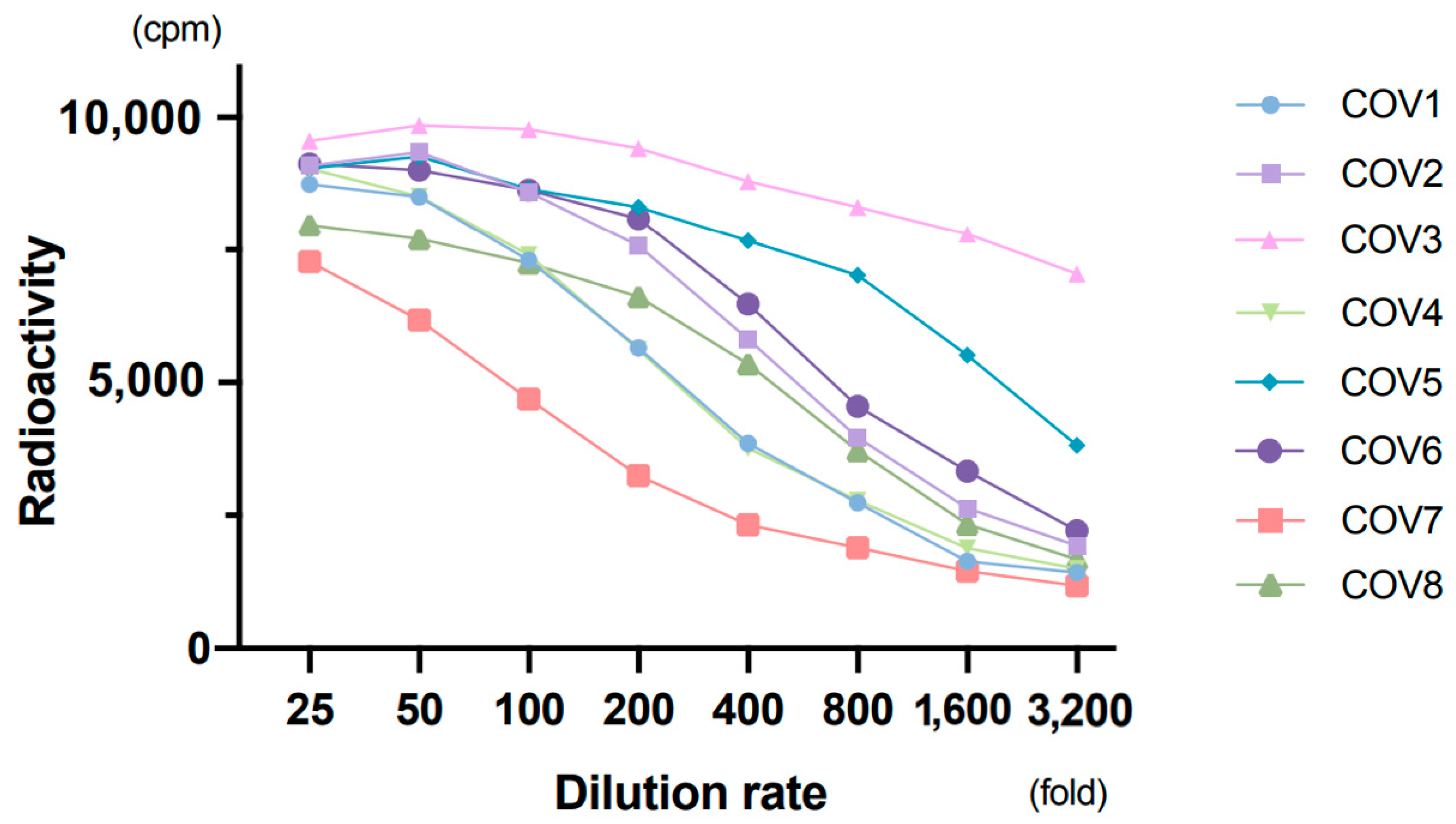
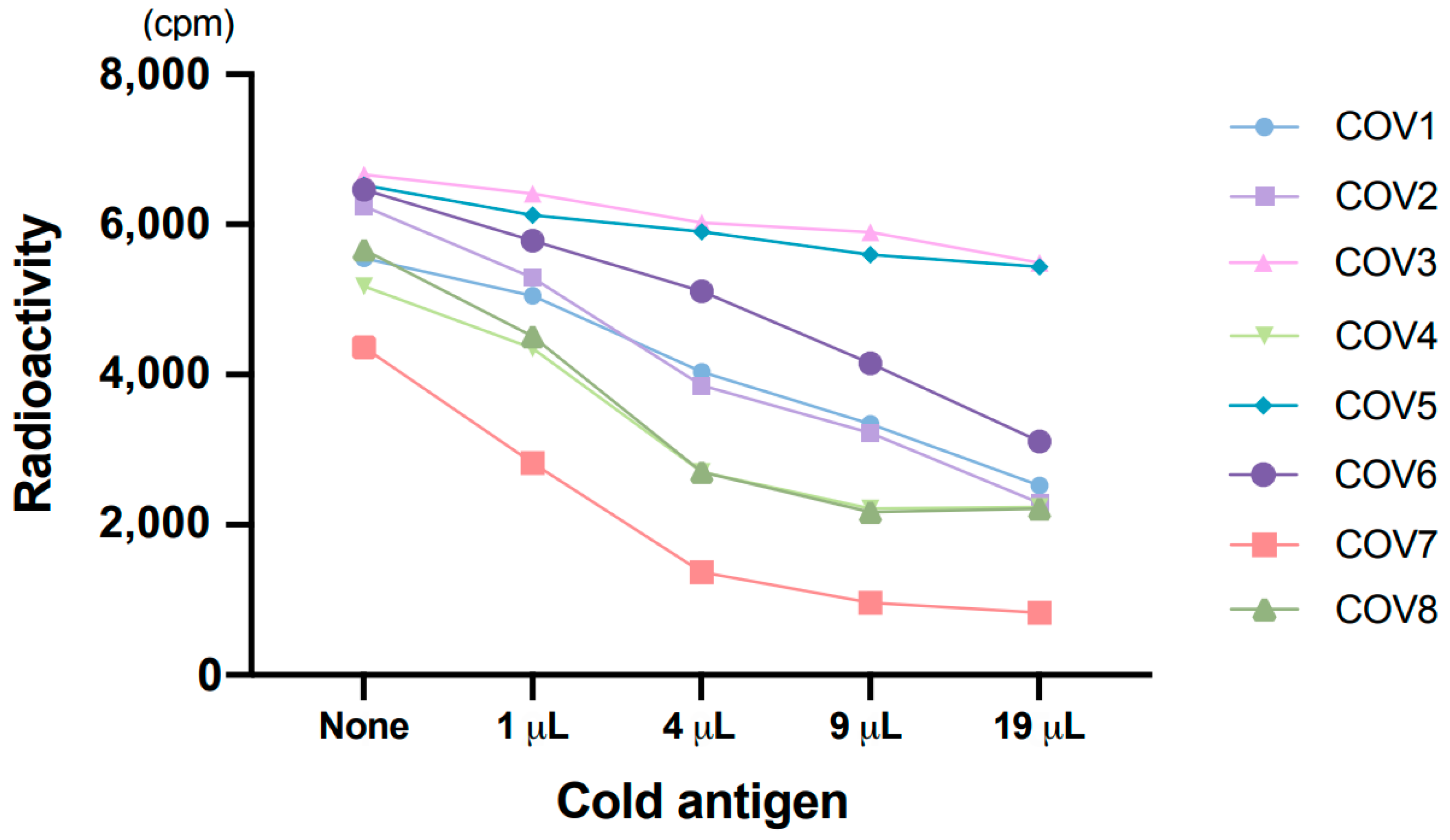
Using RLA, all samples from patients with COVID-19 were found to show high counts. Both the dilution test and the absorption test showed reasonable results. The results of ELISA and neutralizing antibody titration were consistent with those of RLA. Moreover, CLIA, commercialized and validated by other researchers [
3,
4], showed consistency in results with RLA. Therefore, RLA was considered to detect anti-SARS-CoV-2 IgG reliably.
Four out of 1000 samples from hospital staff showed positive counts as high as in patients with COVID-19. Three of them had symptoms and were subsequently diagnosed with COVID-19. The rest had not been diagnosed with COVID-19, although they had experienced a fever for a week. When we planned this study, we expected to find a mildly or symptom-free infected person based on the specific antibodies; however, we did not find such infected individuals. One reason for this might be the very low prevalence of the infection in July 2020 when the blood samples were collected, as no staff with subclinical COVID-19 could be included in this study. Another possibility is that such infected persons had very low titer of antibodies and, were thus included in the group with slightly high counts.
Plebani et al. [
7] surveyed SARS-CoV-2 infection across 8285 health care workers whose blood samples were collected between 22nd February and 29th May; their anti-N and anti-S IgG and IgM levels were measured subsequently. Among them, 378 (4.6%) were seropositive and 286 (3.5%) were positive for viral genomes. Narrowing in on 286 PCR-positive cohorts, 210 (73%) were found seropositive. The seropositivities differed according to the severity of symptoms (severe and hospitalized, mild disease, and asymptomatic were 100%, 83%, and 58%, respectively). In the United States, CDC had examined seroprevalence of anti-SARS-CoV-2 S antibodies in 3248 health professionals, sampled between 3rd April and 19th June [
8]. Among 194 (6.0%) seropositive samples, 56 corresponded to asymptomatic individuals. According to these large-scale studies, some asymptomatic people showed antibodies, whereas others did not. Therefore, sero-surveillance is limited in the detection of infected individuals.
Slightly high counts were observed in 10 or more samples in our study (specifically, 8, 11, or 20 samples excluding four apparently high samples when cut-off points were 2.0, 1.5, or 1.0, respectively). Most of them showed slightly high results with ELISA or CLIA, although many were below the cut-off value of CLIA. When assayed by two or more methods and slightly positive results obtained concordantly, the detected antibodies might be considered as ones attached to SARS-CoV-2 N antigens. Thus, there are two possibilities: cross-reactivity and low titer of the anti-SARS-CoV-2 N antibody.
One blood donor sample showed a slightly high value in both RLA and CLIA. Since the sample had been taken more than 10 years ago, it would not be the real antibody against SARS-CoV-2; rather, it might be a cross-reaction of the antibody with a similar antigen. Hence, the slightly high values in some of the hospital staff samples may have been due to cross-reactions. In that case, those having slightly high anti-N titers and normal anti-S titers would not be incompatible.
SARS-CoV and SARS-CoV-2 have similar amino acid sequences (90% similarity, for example, in the N protein) and can cross-react with each other. Most coronaviruses closest to SARS-CoV-2, which are registered in the GenBank database, are detected from bats. Although MERS, human coronavirus HKU1, and human coronavirus OC43 belong to the same beta coronavirus as SARS-CoV-2, they are less similar in sequence (approximately 50.9%, 35.6%, and 36.6%, respectively). Cross-reactions with similar unknown viruses cannot, therefore, be denied. Hörber et al. [
9] found slightly high values near the cut-off point in one of three patients with influenza A and two of five patients infected with human coronaviruses. Flink et al. [
10] had observed two false positives in two patients infected with human coronavirus OC43; both of them had used S protein as the antigen.
Another possibility for the slightly high results may be the occurrence of very little titer of true antibodies against SARS-CoV-2. In this case, it might be due to either inadequate antibody production and/or lowering of the antibody levels below the cut-off value over time. Long et al. [
11] examined 37 asymptomatic patients with COVID-19 along with 37 mild symptomatic ones and found the antibody titers to be significantly lower in the asymptomatic group than in the symptomatic group; the rates of negative conversion after 8 weeks were 40% and 13% in the asymptomatic and symptomatic groups, respectively. Ibarrondo et al. [
12] estimated the half reduction time of titers in mildly symptomatic patients to be 26–60 days. Together with the Italian and American large-scale sero-surveillances cited above, these findings indicate that asymptomatic or mildly symptomatic infected people should be included in the group with slightly high values around the cut-off point. Infantino et al. [
3] had previously evaluated the iFlashTM CLIA assay system for SARS-CoV-2 antibody employed in this study and reported that the highest sensitivity with a very good specificity performance was reached at a cut-off value of 7.1 rather than 10.0 proposed by the manufacturers. Similarly, Mairesse et al. [
4] suggested a cut-off optimization from 10.0 to 4.86 to obtain maximum sensitivities for the same auto analyzing system.
The Ministry of Health, Labor, and Welfare, Japan had conducted sero-surveillance for general citizens in Tokyo, Osaka, and Miyagi Prefectures in June 2020, and reported five out of 2970 Osaka citizens (0.17%) to be positive (
https://www.mhlw.go.jp/content/10906000/000640184.pdf, accessed on 30 November 2020). In this study, two commercial kits from Roche and Abbott, both using N protein for antigen, were used. Ten citizens were found positive for Roche’s kit, 16 were found positive for Abbott’s kit, and five were found positive for both the kits. A follow-up study based on neutralizing antibody titration was performed, and only five samples with concordantly positive results had neutralizing antibodies (
https://www.mhlw.go.jp/content/000648706.pdf, accessed on 30 November 2020). Since both kits are expected to be highly accurate, samples with high antibody titers cannot possibly be false negatives. Therefore, the discordant samples should have low counts around the cut-off points. Our results regarding neutralizing antibodies being found only in apparently positive samples agreed with the Government’s results.
One of the limitations of our study was the small sample size of COVID-19 patients. More samples from COVID-19 patients could clarify the distribution of the titers of positive samples. Another limitation was that we could not discriminate low-titer true antibodies against SARS-CoV-2 from cross-reactions. This should be clarified in the future. Because RLA is not automated, the lack of accurate procedures might lead to inaccurate quantitation.


 ,
, 






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}