
Pregnancy Outcomes and SARS-CoV-2 Infection: The Spanish Obstetric Emergency Group Study


 , , , , ,
, , , , ,  and add
Show full author list
and add
Show full author list
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Main Results
3.1.1. General Data
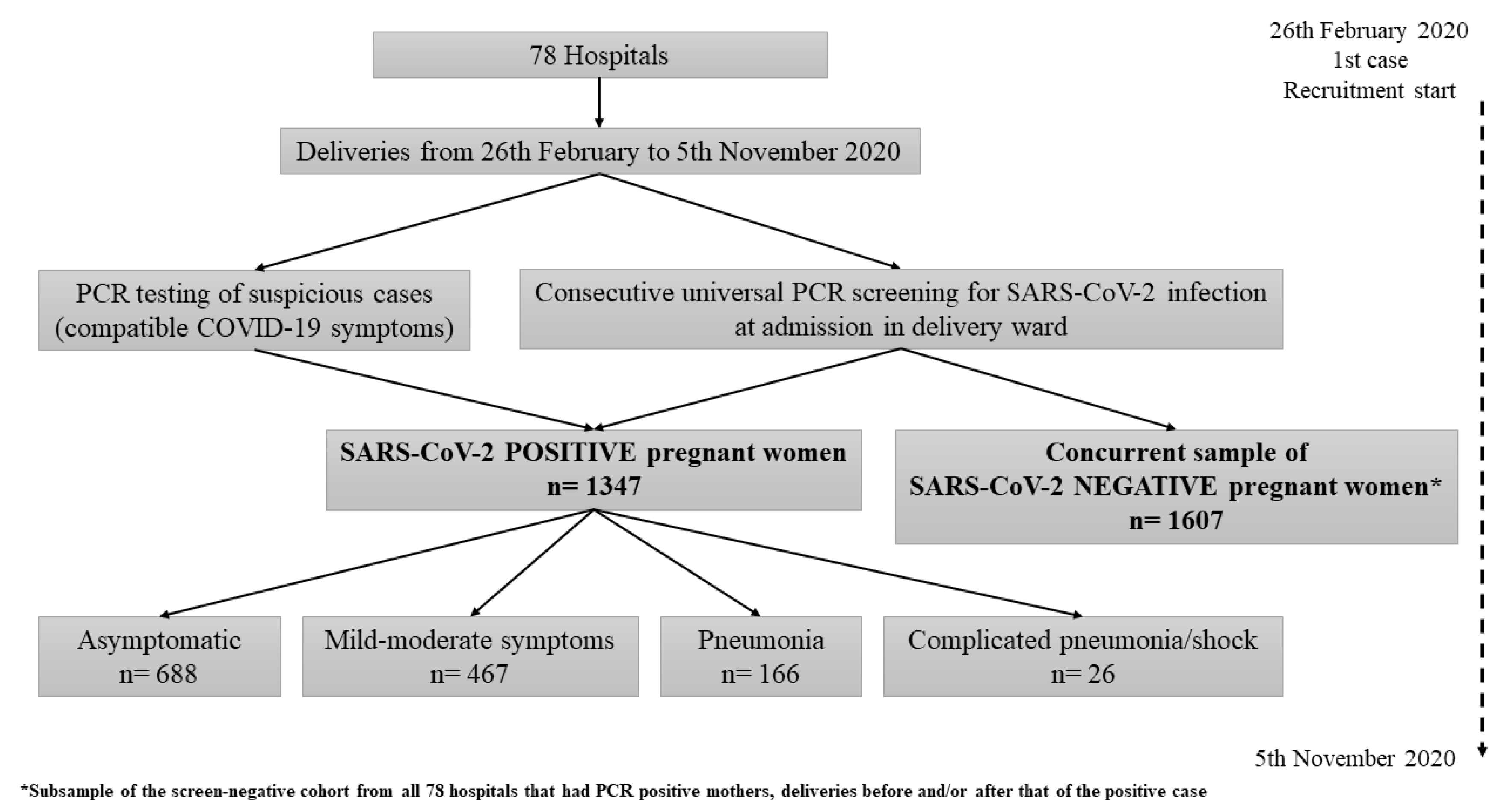
- During the study period, 2954 patients were recorded in the 78 participating hospitals and analyzed: 1347 pregnant women in the infected cohort and 1607 in the non-infected comparison group (Figure 1).
- Of the 1347 positive pregnancies, 51.1% (n = 688) were asymptomatic at delivery while 48.9% (n = 659) showed symptoms.
- Among symptomatic patients, 70.9% (467/659) showed mild–moderate symptoms, 25.2% (166/659) pneumonia and 3.9% (26/659) complicated pneumonia/shock (with ICU admission and/or mechanical ventilation and/or septic shock).
3.1.2. Baseline and Pregnancy Characteristics
- The infected cohort showed a significantly higher proportion of Latin American and Black ethnicities (p < 0.001) compared to the non-infected group (Table 1).
- Maternal age distribution differed between the infected cohort and the non-infected group (p < 0.001), being more skewed to the extremes among infected patients (higher proportion of patients under 24 and above 35 years old).
3.1.3. Maternal and Neonatal Outcomes
- In the SARS-CoV-2-infected cohort, gestational age at delivery was significantly lower (p < 0.001) and the onset of labor was less spontaneous (p < 0.001) compared to non-infected pregnancies (Table 2). In addition, C-section rate was higher in infected patients (27.7% vs. 20.4% non-infected, p < 0.001).
- A higher rate of premature rupture of membranes was observed in the SARS-CoV-2 cohort, both when we analyzed globally (PROM: 15.5% vs. 11.1%, p < 0.001) and in those less than 37 weeks (PPROM: 2.8% vs. 1.4%, p = 0.012).
- More preterm deliveries (<37 weeks of gestational age) were observed in the SARS-CoV-2-infected cohort (11.1% vs. 5.8%; OR 2.00, 95% CI 1.53–2.62; p < 0.001) mainly due to an increase in iatrogenic preterm births, that is, due to medical reasons different from PPROM, as nearly half of preterm births among positive pregnancies were iatrogenic (47.7% vs. 21.3% of preterm births among non-infected; OR 3.37, 95% CI 1.87–6.05; p < 0.001).
- Infected women were more frequently admitted to the ICU before and/or after delivery (2.7% vs. 0.1% non-infected, p < 0.001).
- Women infected with SARS-CoV-2 who developed pre-eclampsia met the criteria for severe pre-eclampsia significantly more than those who were not infected (40.6% vs. 15.6%; OR 3.69, 95% CI 1.62–8.39; p < 0.001), while in the latter, the percentage of moderate pre-eclampsia is higher.
- Higher rates of venous thrombotic events (pulmonary embolism (p = 0.003) and disseminated intravascular coagulation (p = 0.043)) were observed among infected pregnant women.
- No differences were noted between the infected cohort and the non-infected group regarding hemorrhagic events.
- There were two deaths recorded in the SARS-CoV-2-infected cohort versus none in the non-infected group.
- Higher rates of stillbirths as well as of NICU admissions were observed in the SARS-CoV-2-infected cohort; lower birth weight of newborns from infected mothers was also observed (Table 2).
3.1.4. Reasons for Iatrogenic Delivery among SARS-CoV-2-Infected Singleton Preterm Deliveries
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO Coronavirus Disease (COVID-19) Dashboard. Available online: https://covid19.who.int/?gclid=EAIaIQobChMI0bPAdSh6gIVyoKyCh0u9A2mEAAYASAAEgJjsvD_BwE (accessed on 29 March 2021).
- Mehta, N.; Chen, K.; Hardy, E.; Powrie, R. Respiratory disease in pregnancy. Best Pract. Res. Clin. Obstet. Gynaecol. 2015, 29, 598–611. [Google Scholar] [CrossRef] [PubMed]
- Zambrano, L.D.; Ellington, S.; Strid, P.; Galang, R.R.; Oduyebo, T.; Tong, V.T. Update: Characteristics of Symptomatic Women of Reproductive Age with Laboratory-Confirmed SARS-CoV-2 Infection by Pregnancy Status—United States, 22 January–3 October 2020. Morb. Mortal. Wkly Rep. 2020, 69, 1641–1647. [Google Scholar] [CrossRef] [PubMed]
- Allotey, J.; Stallings, E.; Bonet, M.; Yap, M.; Chatterjee, S.; Kew, T.; Debenham, L.; Llavall, A.C.; Dixit, A.; Zhou, D.; et al. Clinical manifestations, risk factors, and maternal and perinatal outcomes of coronavirus disease 2019 in pregnancy: Living systematic review and meta-analysis. BMJ 2020, 370, m3320. [Google Scholar] [CrossRef] [PubMed]
- Martinez Perez, O.; Prats Rodriguez, P.; Hernandez, M.M.; Pardilla, M.B.E.; Perez, N.P.; Hernandez, M.R.V. The association between COVID-19 and preterm delivery: A cohort study with multivariate analysis. medRxiv 2020. [Google Scholar] [CrossRef]
- Martínez-Perez, O.; Vouga, M.; Melguizo, S.C.; Acebal, L.F.; Panchaud, A.; Muñoz-Chápuli, M.; Baud, D. Association Between Mode of Delivery Among Pregnant Women With COVID-19 and Maternal and Neonatal Outcomes in Spain. JAMA 2020, 324, 296–299. [Google Scholar] [CrossRef] [PubMed]
- Centro de Coordinación de Alertas y Emergencias Sanitarias, Ministerio de Sanidad, Gobierno de España. Actualización nº 239. Enfermedad por el coronavirus (COVID-19). 29 October 2020. Available online: https://www.mscbs.gob.es/profesionales/saludPublica/ccayes/alertasActual/nCov/documentos/Actualizacion_239_COVID-19.pdfCDC (accessed on 1 December 2020).
- Encinas Pardilla, M.B.; Caño Aguilar, Á.; Marcos Puig, B.; Sanz Lorenzana, A.; Rodríguez de la Torre, I.; Hernando López de la Manzanara, P.; Fernández Bernardo, A.; Martínez Pérez, Ó. Spanish registry of Covid-19 screening in asymptomatic pregnants. Rev. Esp. Salud Publica 2020, 94, e202009092. [Google Scholar] [PubMed]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gotzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for reporting observational studies. Int. J. Surg. 2014, 12, 1495–1499. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ellington, S.; Strid, P.; Tong Van, T.; Woodworth, K.; Galang, R.G.; Zambrano, L.D.; Nahabedian, J.; Anderson, K.; Gilboa, S.M. Characteristics of Women of Reproductive Age with Laboratory-Confirmed SARS-CoV-2 Infection by Pregnancy Status. Morb. Mortal. Wkly Rep. 2020, 69, 769–775. [Google Scholar] [CrossRef] [PubMed]
- American College of Obstetricians and Gynecologists, Committee on Practice B-O. Prelabor Rupture of Membranes: ACOG Practice Bulletin, Number 217. Obstet. Gynecol. 2020, 135, e80–e97. [Google Scholar] [CrossRef] [PubMed]
- Brown, M.A.; Magee, L.A.; Kenny, L.C.; Karumanchi, S.A.; McCarthy, F.P.; Saito, S.; Hall, D.R.; Warren, C.E.; Adoyi, G.; Ishaku, S.; et al. Hypertensive Disorders of Pregnancy: ISSHP Classification, Diagnosis, and Management Recommendations for International Practice. Hypertension 2018, 72, 24–43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thomson, A.J.; Royal College of Obstetricians and Gynecologists. Care of Women Presenting with Suspected Preterm Prelabour Rupture of Membranes from 24(+0) Weeks of Gestation: Green-top Guideline No. 73. BJOG 2019, 126, e152–e166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bates, D.; Mächler, M.; Bolker, B.; Walker, S. Fitting Linear Mixed-Effects Models Using lme4. J. Stat. Softw. 2015, 67, 48. [Google Scholar] [CrossRef]
- Cruz-Lemini, M.; Ferriols Perez, E.; de la Cruz Conty, M.L.; Caño Aguilar, A.; Encinas Pardilla, M.B.; Prats Rodríguez, P.; Muner Hernando, M.; Forcen Acebal, L.; Pintado Recarte, P.; Medina Mallen, M.D.C.; et al. Obstetric Outcomes of SARS-CoV-2 Infection in Asymptomatic Pregnant Women. Viruses 2021, 13, 112. [Google Scholar] [CrossRef]
- Goldenberg, R.L.; Culhane, J.F.; Iams, J.D.; Romero, R. Epidemiology and causes of preterm birth. Lancet 2008, 371, 75–84. [Google Scholar] [CrossRef]
- Coronado-Arroyo, J.C.; Concepción-Zavaleta, M.J.; Zavaleta-Gutiérrez, F.E.; Concepción-Urteaga, L.A. Is COVID-19 a risk factor for severe preeclampsia? Hospital experience in a developing country. Eur. J. Obstet. Gynecol. Reprod. Biol. 2021, 256, 502–503. [Google Scholar] [CrossRef] [PubMed]
- Mendoza, M.; Garcia-Ruiz, I.; Maiz, N.; Rodo, C.; Garcia-Manau, P.; Serrano, B.; Lopez-Martinez, R.M.; Balcells, J.; Fernandez-Hidalgo, N.; Carreras, E.; et al. Pre-eclampsia-like syndrome induced by severe COVID-19: A prospective observational study. BJOG 2020, 127, 1374–1380. [Google Scholar] [CrossRef] [PubMed]
- Servante, J.; Swallow, G.; Thornton, J.G.; Myers, B.; Munireddy, S.; Malinowski, A.K.; Othman, M.; Li, W.; O’Donoghue, K.; Walker, K.F. Haemostatic and thrombo-embolic complications in pregnant women with COVID-19: A systematic review and critical analysis. BMC Pregnancy Childbirth 2021, 21, 108. [Google Scholar] [CrossRef] [PubMed]
- Juan, J.; Gil, M.M.; Rong, Z.; Zhang, Y.; Yang, H.; Poon, L.C. Effect of coronavirus disease 2019 (COVID-19) on maternal, perinatal and neonatal outcome: Systematic review. Ultrasound Obstet. Gynecol. 2020, 56, 15–27. [Google Scholar] [CrossRef] [PubMed]
- Breslin, N.; Baptiste, C.; Gyamfi-Bannerman, C.; Miller, R.; Martinez, R.; Bernstein, K.; Ring, L.; Landau, R.; Purisch, S.; Friedman, A.M.; et al. Coronavirus disease 2019 infection among asymptomatic and symptomatic pregnant women: Two weeks of confirmed presentations to an affiliated pair of New York City hospitals. Am. J. Obstet. Gynecol. MFM 2020, 2, 100118. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Number | Infected Cohort | Non-Infected Group | p-Value | |
|---|---|---|---|---|
| 1347 | 1607 | |||
| Maternal Characteristics | ||||
| Maternal age (years; median/IQR) | 33 (28–37) | 33 (29–36) | 0.739 | |
| Age Range | 18–24 | 183/1336 (13.7) | 165/1585 (10.4) | 0.001 * |
| 25–34 | 633/1336 (47.4) | 850/1585 (53.6) | ||
| 35–49 | 520/1336 (38.9) | 570/1585 (36.0) | ||
| Ethnicity | White European | 785/1344 (58.4) | 1243/1599 (77.7) | <0.001 * |
| Latino American | 374/1344 (27.8) | 155/1599 (9.7) | ||
| Black non-Hispanic | 35/1344 (2.6) | 21/1599 (1.3) | ||
| Asian non-Hispanic | 40/1344 (3.0) | 41/1599 (2.6) | ||
| Arab | 110/1344 (8.2) | 139/1599 (8.7) | ||
| Nulliparous | 516/1333 (38.7) | 644/1596 (40.4) | 0.366 | |
| Smoking a | 131/1290 (10.2) | 193/1505 (12.8) | 0.028 * | |
| Maternal Comorbidities | ||||
| Obesity (BMI > 30 kg/m2) | 245/1306 (18.8) | 249/1515 (16.4) | 0.105 | |
| Cardiovascular comorbidities | Baseline heart disease b | 15/1316 (1.1) | 11/1528 (0.7) | 0.241 |
| Pre-pregnancy HBP | 19/1304 (1.5) | 17/1514 (1.1) | 0.431 | |
| Pulmonary comorbidities | Chronic pulmonary disease (not asthma) | 3/1316 (0.2) | 2/1532 (0.1) | 0.667 |
| Asthma | 52/1312 (4.0) | 52/1528 (3.4) | 0.428 | |
| Hematologic comorbidities | Chronic hematologic disease | 21/1312 (1.6) | 10/1526 (0.7) | 0.016 * |
| Thrombophilia | 25/1310 (1.9) | 22/1532 (1.4) | 0.325 | |
| Antiphospholipid syndrome | 7/1308 (0.5) | 8/1524 (0.5) | 0.970 | |
| Chronic kidney disease | 5/1313 (0.4) | 5/1528 (0.3) | 1.000 | |
| Chronic liver disease | 11/1319 (0.8) | 8/1536 (0.5) | 0.305 | |
| Rheumatic disease | 11/1314 (0.8) | 16/1524 (1.0%) | 0.560 | |
| Diabetes mellitus | 26 (1.9) | 28 (1.7) | 0.704 | |
| Depressive syndrome | 15/1302 (1.2) | 17/1516 (1.1) | 0.939 | |
| Current Obstetric History | ||||
| Multiple pregnancies | 25 (1.9) | 34 (2.1) | 0.615 | |
| Threatened abortion | 41/1275 (3.2) | 43/1,545 (2.8) | 0.501 | |
| High-risk chromosomal abnormality screening | 31/1288 (2.4) | 37/1544 (2.4) | 0.986 | |
| High-risk pre-eclampsia screening | 69/1149 (6.0) | 68/1438 (4.7) | 0.150 | |
| Positive ultrasound prematurity screening | 16/1132 (1.4) | 30/1411 (2.1) | 0.180 | |
| Gestational diabetes | 97/1309 (7.4) | 136/1584 (8.6) | 0.247 | |
| Intrauterine growth restriction | 48/1290 (3.7) | 44/1566 (2.8) | 0.170 | |
| Pregnancy-induced hypertension c | 50 (3.7) | 55 (3.4) | 0.672 | |
| Number | Infected Cohort | Non-Infected Group | p-Value | |
|---|---|---|---|---|
| 1347 | 1607 | |||
| PERINATAL OUTCOMES | ||||
| Gestational age at delivery (weeks + days; median/IQR) | 39 + 3 (38 + 2–40 + 3) | 39 + 5 (38 + 6–40 + 4) | <0.001 * | |
| Onset of labor | Programmed C-section | 142 (10.5) | 85 (5.3) | <0.001 * |
| Spontaneous | 699 (51.9) | 1000 (62.2) | ||
| Induced | 506 (37.6) | 522 (32.5) | ||
| Type of delivery | Cesarean | 373 (27.7) | 328 (20.4) | <0.001 * |
| Vaginal | 832 (61.8) | 1044 (65.0) | ||
| Operative vaginal | 142 (10.5) | 235 (14.6) | ||
| PROM | 209 (15.5) | 179 (11.1) | <0.001 * | |
| PPROM | 37 (2.8) | 23 (1.4) | 0.012 * | |
| Gestational age at PPROM (weeks + days; median/IQR) | 35 + 0 (33 + 6–35 + 6) | 35 + 1 (34 + 6–36 + 3) | 0.308 | |
| Gestational age range at delivery | <28 weeks | 10 (0.7) | 7 (0.4) | <0.001 * |
| 28 to <32 weeks | 21 (1.6) | 8 (0.5) | ||
| 32 to <37 weeks | 118 (8.8) | 79 (4.9) | ||
| ≥37 weeks | 1198 (88.9) | 1513 (94.2) | ||
| Preterm deliveries (<37 weeks of gestational age) | 149 (11.1) | 94 (5.8) | <0.001 * | |
| Spontaneous delivery (including PPROM) | 58/149 (38.9) | 62/94 (66.0) | ||
| Induced /C-section due to PPROM | 20/149 (13.4) | 12/94 (12.8) | <0.001 * | |
| Iatrogenic delivery (no PPROM) | 71/149 (47.7) | 20/94 (21.3) | ||
| Causes of preterm iatrogenic delivery: | ||||
| COVID-19 mild–moderate symptoms | 15/71 (21.1) | 0/20 (0.0) | ||
| Pneumonia a (alone) | 27/71 (38.0) | 0/20 (0.0) | ||
| Pre-eclampsia b (alone) | 5 c/71 (7.0) | 6/20 (30.0) | ||
| COVID-19 mild-moderate symptoms + pre-eclampsia b | 7/71 (9.9) | 0/20 (0.0) | ||
| Pneumonia a + pre-eclampsia b | 7/71 (9.9) | 0/20 (0.0) | ||
| Other | 10/71 (14.1) | 14/20 (70.0) | ||
| Admitted in ICU d | 36 (2.7) | 2 (0.1) | <0.001 * | |
| Days in ICU (median/IQR) | 12 (8.5–17) | 3 (3–3) | 0.128 | |
| Hemorrhagic events | 70 (5.2) | 89 (5.5) | 0.682 | |
| Abruptio placentae | 12 (0.9) | 7 (0.4) | 0.123 | |
| Postpartum hemorrhage | 61 (4.5) | 86 (5.4) | 0.306 | |
| Pre-eclampsia | 69 (5.1) | 64 (4.0) | 0.137 | |
| Severe pre-eclampsia | 28/69 (40.6) | 10/64 (15.6) | 0.001 * | |
| Admitted in ICU a | 10/28 | 0/10 | ||
| Invasive ventilation | 4/28 | 0/10 | ||
| Moderate pre-eclampsia | 41/69 (59.4) | 54/64 (84.4) | 0.001 * | |
| Thrombotic events | 7 (0.5) | 2 (0.1) | 0.089 | |
| Deep venous thrombosis | 10 (0.7) | 1 (0.1) | 0.003 * | |
| Pulmonary embolism | 4 (0.3) | 0 (0.0) | 0.043 * | |
| Disseminated intravascular coagulation | ||||
| Stillbirth | 10 (0.7) | 3 (0.2) | 0.023 * | |
| MATERNAL MORTALITY | 2 (0.1) | 0 (0.0) | 0.208 | |
| NEONATAL DATA | ||||
| Apgar 5 score <7 | 20/1335 (1.5) | 21/1597 (1.3) | 0.674 | |
| Umbilical artery pH < 7.10 | 40/1081 (3.7) | 46/1248 (3.7) | 0.985 | |
| Birth weight (grams; median/IQR) | 3240 (2890–3550) | 3290 (2970–3600) | 0.001 | |
| Admitted in NICU | 137 (10.2) | 39 (2.4) | <0.001 * | |
| Neonatal mortality | 6 (0.4) | 2 (0.1) | 0.153 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cruz Melguizo, S.; de la Cruz Conty, M.L.; Carmona Payán, P.; Abascal-Saiz, A.; Pintando Recarte, P.; González Rodríguez, L.; Cuenca Marín, C.; Martínez Varea, A.; Oreja Cuesta, A.B.; Rodríguez, P.P.; et al. Pregnancy Outcomes and SARS-CoV-2 Infection: The Spanish Obstetric Emergency Group Study. Viruses 2021, 13, 853. https://doi.org/10.3390/v13050853
Cruz Melguizo S, de la Cruz Conty ML, Carmona Payán P, Abascal-Saiz A, Pintando Recarte P, González Rodríguez L, Cuenca Marín C, Martínez Varea A, Oreja Cuesta AB, Rodríguez PP, et al. Pregnancy Outcomes and SARS-CoV-2 Infection: The Spanish Obstetric Emergency Group Study. Viruses. 2021; 13(5):853. https://doi.org/10.3390/v13050853
Chicago/Turabian StyleCruz Melguizo, Sara, María Luisa de la Cruz Conty, Paola Carmona Payán, Alejandra Abascal-Saiz, Pilar Pintando Recarte, Laura González Rodríguez, Celia Cuenca Marín, Alicia Martínez Varea, Ana Belén Oreja Cuesta, Pilar Prats Rodríguez, and et al. 2021. "Pregnancy Outcomes and SARS-CoV-2 Infection: The Spanish Obstetric Emergency Group Study" Viruses 13, no. 5: 853. https://doi.org/10.3390/v13050853
APA StyleCruz Melguizo, S., de la Cruz Conty, M. L., Carmona Payán, P., Abascal-Saiz, A., Pintando Recarte, P., González Rodríguez, L., Cuenca Marín, C., Martínez Varea, A., Oreja Cuesta, A. B., Rodríguez, P. P., Fernández Buhigas, I., Rodríguez Gallego, M. V., Fernández Alonso, A. M., López Pérez, R., Broullón Molanes, J. R., Encinas Pardilla, M. B., Ramírez Gómez, M., Gimeno Gimeno, M. J., Sánchez Muñoz, A., ... on behalf of the Spanish Obstetric Emergency Group (S.O.E.G.). (2021). Pregnancy Outcomes and SARS-CoV-2 Infection: The Spanish Obstetric Emergency Group Study. Viruses, 13(5), 853. https://doi.org/10.3390/v13050853