
SARS-CoV-2 Vaccine Willingness among Pregnant and Breastfeeding Women during the First Pandemic Wave: A Cross-Sectional Study in Switzerland

 ,
,  , , , ,
, , , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
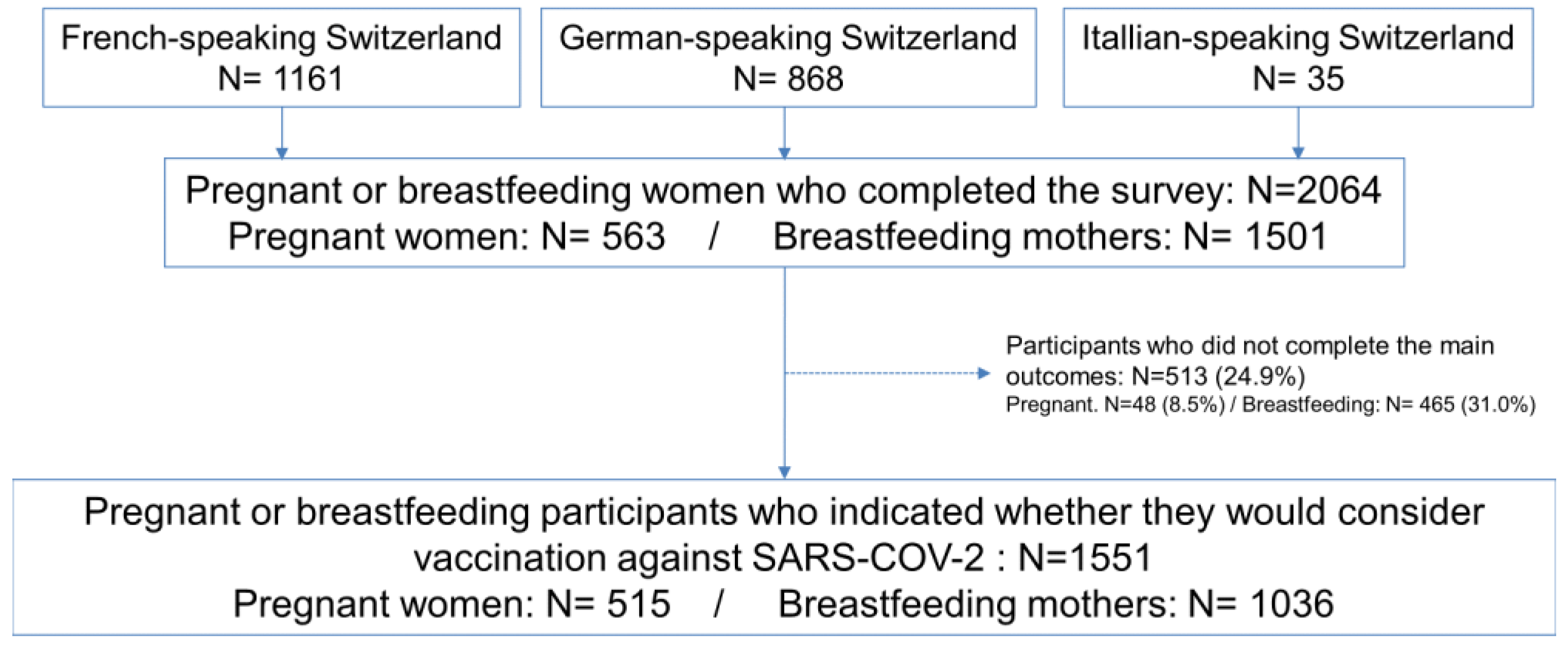
2.1. Study Population and Data Collection
2.2. Study Population
2.3. Variables
2.4. Main Outcomes
2.5. Statistical Analysis
2.6. Missing Values
3. Results
3.1. Baseline Characteristics
3.2. SARS-CoV-2 Exposure, Fears, and Beliefs
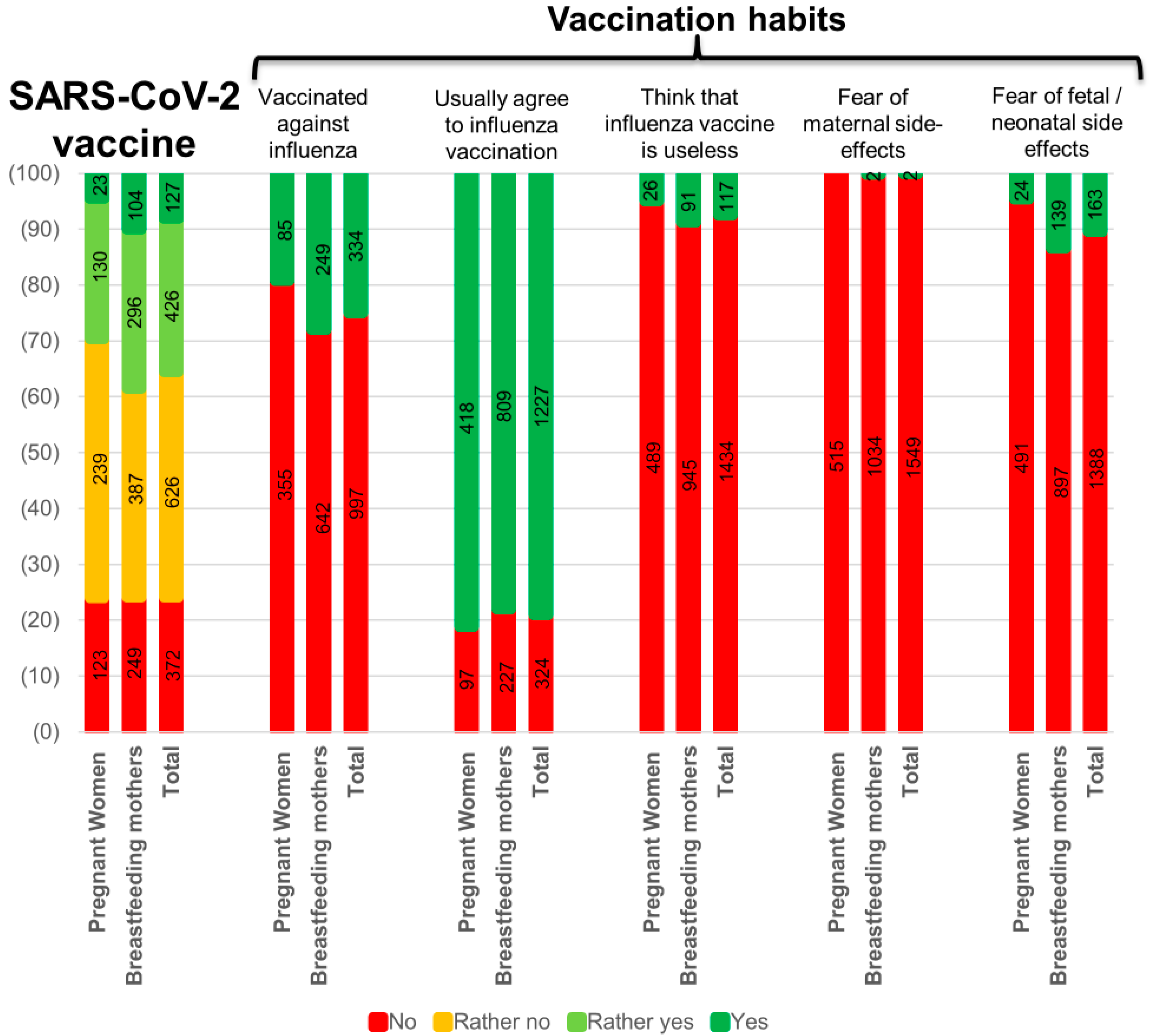
3.3. Vaccination Practices and Beliefs
3.4. Willingness to Get the SARS-CoV-2 Vaccine
3.5. Factors Associated with SARS-CoV-2 Vaccine Willingness
4. Discussion
4.1. Interpretation
4.2. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- FOPH. Status Report, Switzerland and Liechtenstein. Available online: https://www.covid19.admin.ch/ (accessed on 1 May 2021).
- Favre, G.; Pomar, L.; Baud, D. Coronavirus Disease 2019 during Pregnancy: Do not Underestimate the Risk of Maternal Adverse Outcomes. Am. J. Obstet. Gynecol. MFM 2020, 2, 100160. [Google Scholar] [CrossRef]
- Jering, K.S.; Claggett, B.L.; Cunningham, J.W.; Rosenthal, N.; Vardeny, O.; Greene, M.F.; Solomon, S.D. Clinical Characteristics and Outcomes of Hospitalized Women Giving Birth With and Without COVID-19. JAMA Intern. Med. 2021, 181, 714. [Google Scholar] [CrossRef]
- Lokken, E.M.; Taylor, G.G.; Huebner, E.M.; Vanderhoeven, J.; Hendrikson, S.; Coler, B.; Sheng, J.S.; Walker, C.L.; McCartney, S.A.; Kretzer, N.M.; et al. Higher SARS-CoV-2 Infection Rate in Pregnant Patients. Am. J. Obstet. Gynecol. 2021. [Google Scholar] [CrossRef] [PubMed]
- Zambrano, L.D.; Ellington, S.; Strid, P.; Galang, R.R.; Oduyebo, T.; Tong, V.T.; Woodworth, K.R.; Nahabedian, J.F., III; Azziz-Baumgartner, E.; Gilboa, S.M.; et al. Update: Characteristics of Symptomatic Women of Reproductive Age with Laboratory-Confirmed SARS-CoV-2 Infection by Pregnancy Status-United States, January 22–October 3, 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 1641–1647. [Google Scholar] [CrossRef]
- Allotey, J.; Stallings, E.; Bonet, M.; Yap, M.; Chatterjee, S.; Kew, T.; Debenham, L.; Llavall, A.C.; Dixit, A.; Zhou, D.; et al. Clinical Manifestations, Risk Factors, and Maternal and Perinatal Outcomes of Coronavirus Disease 2019 in Pregnancy: Living Systematic Review and Meta-Analysis. BMJ 2020, 370, m3320. [Google Scholar] [CrossRef] [PubMed]
- Khalil, A.; Kalafat, E.; Benlioglu, C.; O’Brien, P.; Morris, E.; Draycott, T.; Thangaratinam, S.; Doare, K.L.; Heath, P.; Ladhani, S.; et al. SARS-CoV-2 Infection in Pregnancy: A Systematic Review and Meta-Analysis of Clinical Features and Pregnancy Outcomes. EClinicalMedicine 2020, 25, 100446. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Perez, O.; Vouga, M.; Melguizo, S.C.; Acebal, L.F.; Panchaud, A.; Muñoz-Chápuli, M.; Baud, D. Association Between Mode of Delivery Among Pregnant Women With COVID-19 and Maternal and Neonatal Outcomes in Spain. JAMA 2020, 324, 296–299. [Google Scholar] [CrossRef] [PubMed]
- Khalil, A.; Von Dadelszen, P.; Draycott, T.; Ugwumadu, A.; O’Brien, P.; Magee, L. Change in the Incidence of Stillbirth and Preterm Delivery During the COVID-19 Pandemic. JAMA 2020, 324, 705. [Google Scholar] [CrossRef] [PubMed]
- Hcini, N.; Maamri, F.; Picone, O.; Carod, J.F.; Lambert, V.; Mathieu, M.; Carles, G.; Pomar, L. Maternal, Fetal and Neonatal Outcomes of Large Series of SARS-CoV-2 Positive Pregnancies in Peripartum Period: A Single-Center Prospective Comparative Study. Eur. J. Obstet. Gynecol. Reprod. Biol. 2021, 257, 11–18. [Google Scholar] [CrossRef]
- Baud, D.; Greub, G.; Favre, G.; Gengler, C.; Jaton, K.; Dubruc, E.; Pomar, L. Second-Trimester Miscarriage in a Pregnant Woman With SARS-CoV-2 Infection. JAMA 2020, 323, 2198–2200. [Google Scholar] [CrossRef]
- Swissmedic. Available online: https://www.swissmedic.ch/swissmedic/fr/home/news/coronavirus-covid-19/dritten-impfstoff-gegen-covid-19-erkrankung.html (accessed on 1 May 2021).
- WHO. Ten Threats. Available online: https://www.who.int/news-room/spotlight/ten-threats-to-global-health-in-2019 (accessed on 1 May 2021).
- Blanchard-Rohner, G.; Siegrist, C.-A. Vaccination during Pregnancy to Protect Infants Against Influenza: Why and Why Not? Vaccine 2011, 29, 7542–7550. [Google Scholar] [CrossRef] [PubMed]
- Reuman, P.D.; Ayoub, E.M.; Small, P.A. Effect of Passive Maternal Antibody on Influenza Illness in Children: A Prospective Study of Influenza A in Mother-Infant Pairs. Pediatr. Infect. Dis. J. 1987, 6, 398–403. [Google Scholar] [CrossRef] [PubMed]
- Blanchard-Rohner, G.; Eberhardt, C. Review of Maternal Immunisation during Pregnancy: Focus on Pertussis and Influenza. Swiss Med. Wkly. 2017, 147, w14526. [Google Scholar] [PubMed]
- Erb, M.L.; Erlanger, T.E.; Heininger, U. Child-Parent Immunization Survey: How Well are National Immunization Recommendations Accepted by the Target Groups? Vaccine X 2019, 1, 100013. [Google Scholar] [CrossRef]
- Healy, C.M.; Rench, M.A.; Montesinos, D.P.; Ng, N.; Swaim, L.S. Knowledge and Attitiudes of Pregnant Women and their Providers Towards Recommendations for Immunization during Pregnancy. Vaccine 2015, 33, 5445–5451. [Google Scholar] [CrossRef] [PubMed]
- Abu-Raya, B.; Maertens, K.; Edwards, K.M.; Omer, S.B.; Englund, J.A.; Flanagan, K.L.; Snape, M.D.; Amirthalingam, G.; Leuridan, E.; Van Damme, P.; et al. Global Perspectives on Immunization During Pregnancy and Priorities for Future Research and Development: An International Consensus Statement. Front. Immunol. 2020, 11, 1282. [Google Scholar] [CrossRef]
- MacDougall, D.M.; Halperin, S.A. Improving Rates of Maternal Immunization: Challenges and Opportunities. Hum. Vaccines Immunother. 2016, 12, 857–865. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilson, R.J.; Paterson, P.; Jarrett, C.; Larson, H.J. Understanding Factors Influencing Vaccination Acceptance during Pregnancy Globally: A Literature Review. Vaccine 2015, 33, 6420–6429. [Google Scholar] [CrossRef] [Green Version]
- Lutz, C.S.; Carr, W.; Cohn, A.; Rodriguez, L. Understanding Barriers and Predictors of Maternal Immunization: Identifying gaps through an Exploratory Literature Review. Vaccine 2018, 36, 7445–7455. [Google Scholar] [CrossRef]
- Mohammed, H.; Roberts, C.T.; Grzeskowiak, L.E.; Giles, L.; Leemaqz, S.; Dalton, J.; Dekker, G.; Marshall, H.S. Psychosocial Determinants of Pertussis and Influenza Vaccine Uptake in Pregnant Women: A Prospective Study. Vaccine 2020, 38, 3358–3368. [Google Scholar] [CrossRef]
- Ceulemans, M.; Foulon, V.; Ngo, E.; Panchaud, A.; Winterfeld, U.; Pomar, L.; Lambelet, V.; Cleary, B.; O’Shaughnessy, F.; Passier, A.; et al. Mental Health Status of Pregnant and Breastfeeding Women during the COVID-19 Pandemic-A Multinational Cross-Sectional Study. Acta Obstet. Gynecol. Scand. 2021. [Google Scholar] [CrossRef] [PubMed]
- Ceulemans, M.; Foulon, V.; Panchaud, A.; Winterfeld, U.; Pomar, L.; Lambelet, V.; Cleary, B.; O’Shaughnessy, F.; Passier, A.; Richardson, J.; et al. Vaccine Willingness and Impact of the COVID-19 Pandemic on Women’s Perinatal Experiences and Practices—A Multinational, Cross-Sectional Study Covering the First Wave of the Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 3367. [Google Scholar] [CrossRef] [PubMed]
- Cox, J.L.; Holden, J.M.; Sagovsky, R. Detection of Postnatal Depression. Development of the 10-Item Edinburgh Post-Natal Depression Scale. Br. J. Psychiatry 1987, 150, 782–786. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bergink, V.; Kooistra, L.; Berg, M.P.L.-V.D.; Wijnen, H.; Bunevicius, R.; van Baar, A.; Pop, V. Validation of the Edinburgh Depression Scale during Pregnancy. J. Psychosom. Res. 2011, 70, 385–389. [Google Scholar] [CrossRef]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.; Löwe, B. A Brief Measure for Assessing Generalized Anxiety Disorder: The GAD-7. Arch. Intern. Med. 2006, 166, 1092–1097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A Global Measure of Perceived Stress. J. Health Soc. Behav. 1983, 24, 385–396. [Google Scholar] [CrossRef]
- Taylor, J.M. Psychometric Analysis of the Ten-Item Perceived Stress Scale. Psychol. Assess. 2015, 27, 90–101. [Google Scholar] [CrossRef] [Green Version]
- Skjefte, M.; Ngirbabul, M.; Akeju, O.; Escudero, D.; Hernandez-Diaz, S.; Wyszynski, D.F.; Wu, J.W. COVID-19 Vaccine Acceptance among Pregnant Women and Mothers of Young Children: Results of a Survey in 16 Countries. Eur. J. Epidemiol. 2021, 36, 197–211. [Google Scholar] [CrossRef]
- Ashley, N.; Battarbee, M.S.S.; Varner, M.; Newes-Adeyi, G.; Daugherty, M.; Gyamfi-Bannerman, C.; Tita, A.; Vorwaller, K.; Vargas, C.; Subramaniam, A.; et al. Attitudes Toward COVID-19 Illness and COVID-19 Vaccination among Pregnant Women: A Cross-Sectional Multicenter Study during August–December 2020. Pre-print.2021. Available online: https://www.medrxiv.org/content/10.1101/2021.03.26.21254402v1 (accessed on 1 May 2021).
- Lang, P.; Zimmermann, H.; Piller, U.; Steffen, R.; Hatz, C. The Swiss National Vaccination Coverage Survey, 2005–2007. Public Health Rep. 2011, 126, 97–108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Les Suisses Sceptiques à L'égard des Vaccins. Available online: https://www.pharmapro.ch/news/les-suisses-sceptiques-a-l-egard-des-vaccins-0222.htm (accessed on 1 May 2021).
- Niveau de Formation de la Population-Données de L’indicateur. Available online: https://www.bfs.admin.ch/bfs/fr/home/statistiques/situation-economique-sociale-population/egalite-femmes-hommes/formation/niveau-formation.assetdetail.12527179.html (accessed on 1 May 2021).
- Situation Professionnelle Selon le Sexe et la Situation Familiale. Available online: https://www.bfs.admin.ch/bfs/fr/home/statistiques/catalogues-banques-donnees/tableaux.assetdetail.13108456.html (accessed on 1 May 2021).
- Pfizer-BioNTech. Study to Evaluate the Safety, Tolerability, and Immunogenicity of SARS CoV-2 RNA Vaccine Candidate (BNT162b2) Against COVID-19 in Healthy Pregnant Women 18 Years of Age and Older. U.S in National Library of Medicine. 2021. Available online: https://clinicaltrials.gov/ct2/show/NCT04754594 (accessed on 1 May 2021).
- SGGG. Available online: https://www.sggg.ch/fr/nouvelles/detail/1/infection-a-coronavirus-covid-19-et-grossesse/ (accessed on 1 May 2021).
- Harvard Gazette. Available online: https://news.harvard.edu/gazette/story/2021/03/study-shows-covid-19-vaccinated-mothers-pass-antibodies-to-newborns/ (accessed on 1 May 2021).
- Gilbert, P.D.; Rudnick, C.A. Newborn Antibodies to SARS-CoV-2 Detected in Cord Blood after Maternal Vaccination. medRxiv 2021. [Google Scholar] [CrossRef]
- Atyeo, C.; Pullen, K.M.; Bordt, E.A.; Fischinger, S.; Burke, J.; Michell, A.; Slein, M.D.; Loos, C.; Shook, L.L.; Boatin, A.A.; et al. Compromised SARS-CoV-2-Specific Placental Antibody Transfer. Cell 2021, 184, 628–642.e10. [Google Scholar] [CrossRef]
- Shimabukuro, T.T.; Kim, S.Y.; Myers, T.R.; Moro, P.L.; Oduyebo, T.; Panagiotakopoulos, L.; Marquez, P.L.; Olson, C.K.; Liu, R.; Chang, K.T.; et al. Preliminary Findings of mRNA Covid-19 Vaccine Safety in Pregnant Persons. N. Engl. J. Med. 2021. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Pregnant Women | Breastfeeding Mothers | Total | |||||
|---|---|---|---|---|---|---|---|
| n = 515 | (%) | n = 1036 | (%) | n = 1551 | (%) | ||
| Baseline characteristics | |||||||
| Maternal age (years)—median (IQR) | 33 | (31–35) | 33 | (31–35) | 33 | (31–35) | |
| >40 years | 19 | (3.7) | 63 | (6.1) | 82 | (5.3) | |
| Marital status | |||||||
| Married/cohabiting | 422 | (81.9) | 815 | (78.7) | 1237 | (79.8) | |
| Single/divorced/others | 4 | (0.8) | 9 | (0.9) | 13 | (0.8) | |
| Unknown | 89 | (17.3) | 212 | (20.5) | 301 | (19.4) | |
| Working status | |||||||
| Health care provider | 122 | (23.7) | 195 | (18.8) | 317 | (20.4) | |
| Employed other than HCP | 257 | (49.9) | 465 | (44.9) | 722 | (46.6) | |
| Student | 3 | (0.6) | 7 | (0.7) | 10 | (0.6) | |
| Housewife | 21 | (4.1) | 118 | (11.4) | 139 | (9.0) | |
| Job seeker | 12 | (2.3) | 23 | (2.2) | 35 | (2.3) | |
| Unknown | 100 | (19.4) | 228 | (22.0) | 328 | (21.1) | |
| Educational level | |||||||
| Less than high school | 9 | (1.8) | 20 | (1.9) | 29 | (1.9) | |
| High school | 75 | (14.6) | 212 | (20.5) | 287 | (18.5) | |
| More than high school | 257 | (49.9) | 464 | (44.8) | 721 | (46.5) | |
| Unknown | 174 | (33.8) | 340 | (32.8) | 514 | (33.0) | |
| Primary language | |||||||
| French | 217 | (42.1) | 418 | (40.4) | 635 | (40.9) | |
| German | 183 | (35.5) | 322 | (31.1) | 505 | (32.6) | |
| Italian | 8 | (1.6) | 23 | (2.2) | 31 | (2.0) | |
| Other | 18 | (3.5) | 61 | (5.8) | 79 | (5.1) | |
| Unknown | 89 | (17.3) | 212 | (20.5) | 301 | (19.4) | |
| Maternal co-morbidities | |||||||
| Any comorbidity | 51 | (9.9) | 100 | (9.7) | 151 | (9.7) | |
| Pulmonary | 14 | (2.7) | 28 | (2.7) | 42 | (2.7) | |
| Cardio-vascular | 6 | (1.2) | 11 | (1.1) | 17 | (1.1) | |
| Pregestational diabetes | 5 | (1.0) | 9 | (0.9) | 14 | (0.9) | |
| Thyroid dysfunction | 12 | (2.3) | 27 | (2.6) | 39 | (2.5) | |
| Oncologic | 1 | (0.2) | 2 | (0.2) | 3 | (0.2) | |
| Hematologic | 2 | (0.4) | 0 | (0.0) | 2 | (0.1) | |
| Auto-immune | 2 | (0.4) | 4 | (0.4) | 6 | (0.4) | |
| Neurologic | 3 | (0.6) | 4 | (0.4) | 7 | (0.5) | |
| Psychic | 3 | (0.6) | 6 | (0.6) | 9 | (0.6) | |
| Digestive | 3 | (0.6) | 7 | (0.7) | 10 | (0.7) | |
| Uro-genital tract | 6 | (1.2) | 15 | (1.4) | 21 | (1.4) | |
| Cutaneous | 2 | (0.4) | 4 | (0.4) | 6 | (0.4) | |
| ENT | 0 | (0.0) | 1 | (0.1) | 1 | (0.1) | |
| Smoking | 69 | (13.4) | 149 | (14.4) | 218 | (14.1) | |
| Actual pregnancy or breastfeeding | |||||||
| Practitioner: | Obstetrician | 468 | 90.9 | / | |||
| Midwife | 13 | 8.3 | |||||
| Family physician | 4 | 0.8 | |||||
| Gestation | 1 | 240 | 46.6 | / | |||
| >1 | 275 | 53.4 | |||||
| Parity | 0 | 20/274 | 7.3 | / | |||
| 1 | 204/274 | 74.4 | |||||
| >1 | 50/274 | 18.2 | |||||
| Planned pregnancy | 483 | 93.8 | / | ||||
| Gestational age—median (IQR) | 28 | (18-34) | / | ||||
| 1st Trimester | 79 | (15.0) | |||||
| 2nd Trimester | 194 | (40.7) | |||||
| 3rd Trimester | 241 | (44.3) | |||||
| Neonate hospitalized in NICU | / | 29 | (2.8) | ||||
| Pregnant Women | Breastfeeding Mothers | Total | ||||||
|---|---|---|---|---|---|---|---|---|
| n = 515 | (%) | n = 1036 | (%) | n = 1551 | (%) | |||
| SARS-COV-2 exposure | ||||||||
| Symptoms during the 3 last months | 296 | (57.5) | 554 | (53.5) | 850 | (54.8) | ||
| Hospitalized for COVID-19 | 2 | (0.4) | 7 | (0.7) | 9 | (0.6) | ||
| Tested for SARS-CoV-2 infection | 48 | (9.3) | 122 | (11.8) | 170 | (10.9) | ||
| PCR on nasopharyngeal swab | 39 | (7.6) | 112 | (108.0) | 151 | (9.7) | ||
| positive | 5/39 | (12.8) | 6/112 | (5.3) | 11/151 | (7.3) | ||
| negative | 33/39 | (84.6) | 103/112 | (92.0) | 136/151 | (90.1) | ||
| unknown | 1/39 | (2.6) | 3/112 | (2.7) | 4/151 | (2.7) | ||
| Serology | 7 | (1.4) | 21 | (2.0) | 28 | (1.8) | ||
| positive | 3/7 | (42.9) | 2/21 | (9.5) | 5/28 | (17.9) | ||
| negative | 3/7 | (42.9) | 16/21 | (76.2) | 19/28 | (67.9) | ||
| unknown | 1/7 | (14.2) | 3/21 | (14.3) | 4/28 | (14.3) | ||
| Scanner | 2 | (0.4) | 2 | (0.2) | 4 | (2.6) | ||
| positive | 2/2 | (100.0) | 0/2 | (0.0) | 2/4 | (50.0) | ||
| negative | 0/2 | (0.0) | 2/2 | (100.0) | 2/4 | (50.0) | ||
| Living with someone with symptoms | 82 | (15.9) | 220 | (21.2) | 302 | (19.5) | ||
| Living with someone tested positive | 4 | (0.8) | 10 | (1.0) | 14 | (0.9) | ||
| Living with someone > 65 years old | 6 | (1.2) | 12 | (1.2) | 18 | (1.2) | ||
| Negative impact of the COVID-19 pandemic on: | ||||||||
| Pregnancy or breastfeeding experience | 97 | (18.8) | 41 | (4.0) | 138 | (8.9) | ||
| unknown | 240 | (46.6) | 524 | (50.6) | 764 | (49.3) | ||
| Life habits | 350 | (68.2) | 700 | (67.6) | 1050 | (67.7) | ||
| unknown | 8 | (1.6) | 25 | (2.4) | 33 | (2.1) | ||
| Work | 295 | (57.3) | 394 | (38.0) | 689 | (44.4) | ||
| unknown | 100 | (19.4) | 320 | (30.9) | 420 | (27.1) | ||
| Fear of an adverse fetal outcome | 275 | (53.4) | / | |||||
| Symptoms of severe depression, anxiety or high stress perceived during the 1st wave | 53 | (10.3) | 117 | (11.3) | 170 | (11.0) | ||
| Participants Willing to Get Vaccinated against COVID-19 | Participants Not Willing to Get Vaccinated against COVID-19 | OR | (95% CI) | p | aOR | (95% CI) | p | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| N | (%) | N | (%) | ||||||||
| 553 | (35.7) | 998 | (64.3) | ||||||||
| Baseline characteristics | |||||||||||
| Maternal age >40 years | 42 | (7.6) | 40 | (4.0) | 2.0 | (1.3–3.0) | 0.003 | 1.8 | (1.1–3.2) | 0.028 | |
| Educational level > highschool | 300 * | (75.9) | 421 * | (65.6) | 1.7 | (1.3–2.2) | <0.001 | 1.5 | (1.1–2.0) | 0.017 | |
| Professionally active | 387 * | (87.4) | 652 * | (83.6) | 1.4 | (1.0–1.9) | 0.007 | 1.0 | (0.7–1.5) | 0.919 | |
| Primary language | |||||||||||
| French | 238 | (52.8) | 397 | (49.7) | 1.1 | (0.9–1.4) | 0.295 | ||||
| German | 159 * | (35.3) | 346 * | (43.3) | 0.7 | (0.6–0.9) | 0.005 | 0.7 | (0.5–0.9) | 0.015 | |
| Italian | 19 * | (4.2) | 12 * | (1.5) | 2.9 | (1.4–6.0) | 0.005 | 3.3 | (1.4–8.0) | 0.007 | |
| Any maternal co-morbidity | 58 | (10.5) | 93 | (9.3) | 1.1 | (0.8–1.6) | 0.457 | ||||
| Impact of the SARS-COV-2 pandemic | |||||||||||
| Tested positive for SARS-COV-2 (RT-PCR, serology and/or CT) | 9 | (1.6) | 3 | (0.3) | 5.5 | (1.5–20.4) | 0.011 | 3.3 | (0.8–13.7) | 0.095 | |
| Living with someone >65 years old | 10 | (1.8) | 8 | (0.8) | 2.3 | (0.8–6.7) | 0.076 | 2.0 | (0.7–6.1) | 0.094 | |
| Negative impact of the pandemic on | |||||||||||
| Pregnancy | 52 | (19.9) | 86 | (16.3) | 1.1 | (1.0–1.2) | 0.215 | ||||
| Life habits | 398 * | (72.8) | 652 * | (67.2) | 1.3 | (1.0–1.7) | 0.023 | 1.0 | (0.8–1.4) | 0.822 | |
| Work | 244 | (60.1) | 445 | (61.4) | 1.0 | (0.7–1.2) | 0.672 | ||||
| Symptoms of severe depression, anxiety or high stress | 68 | (12.3) | 102 | (10.2) | 1.2 | (0.9–1.7) | 0.211 | ||||
| Vaccination habits and beliefs | |||||||||||
| Vaccinated against Influenza last year | 197 * | (41.1) | 137 * | (16.1) | 3.6 | (2.8–4.7) | <0.001 | 2.1 | (1.5–2.8) | <0.001 | |
| Usually decline vaccination | 30 | (5.4) | 294 | (29.5) | 0.1 | (0.1–0.2) | <0.001 | 0.2 | (0.1–0.3) | <0.001 | |
| Fear of side effects related to vaccines | 51 | (9.2) | 114 | (11.4) | 0.8 | (0.6–1.1) | 0.179 | ||||
| Supplementary model including pregnancy-related variables (tested only in pregnant women, N = 515) | N | (%) | N | (%) | OR | (95%CI) | p | aOR | (95%CI) | p | |
| 153 | (29.7) | 362 | (60.3) | ||||||||
| Follow-up by an obstetrician | 144 | (94.1) | 324 | (89.5) | 1.9 | (0.9–4.0) | 0.101 | 3.6 | (1.2–11.2) | 0.027 | |
| Gestational age | |||||||||||
| T1 | 25 | (16.3) | 54 | (15.0) | 1.1 | (0.7–1.9) | 0.691 | ||||
| T2 | 47 | (30.7) | 147 | (40.7) | 0.6 | (0.4–1.0) | 0.033 | 0.6 | (0.4–0.9) | 0.015 | |
| T3 | 81 | (52.9) | 160 | (44.3) | 1.4 | (1.0–2.0) | 0.074 | 1.8 | (1.1–2.7) | 0.018 | |
| Fear of an adverse fetal outcome in case of infection | 75 | (49.0) | 200 | (55.3) | 0.9 | (0.8–1.0) | 0.196 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stuckelberger, S.; Favre, G.; Ceulemans, M.; Nordeng, H.; Gerbier, E.; Lambelet, V.; Stojanov, M.; Winterfeld, U.; Baud, D.; Panchaud, A.; et al. SARS-CoV-2 Vaccine Willingness among Pregnant and Breastfeeding Women during the First Pandemic Wave: A Cross-Sectional Study in Switzerland. Viruses 2021, 13, 1199. https://doi.org/10.3390/v13071199
Stuckelberger S, Favre G, Ceulemans M, Nordeng H, Gerbier E, Lambelet V, Stojanov M, Winterfeld U, Baud D, Panchaud A, et al. SARS-CoV-2 Vaccine Willingness among Pregnant and Breastfeeding Women during the First Pandemic Wave: A Cross-Sectional Study in Switzerland. Viruses. 2021; 13(7):1199. https://doi.org/10.3390/v13071199
Chicago/Turabian StyleStuckelberger, Sarah, Guillaume Favre, Michael Ceulemans, Hedvig Nordeng, Eva Gerbier, Valentine Lambelet, Milos Stojanov, Ursula Winterfeld, David Baud, Alice Panchaud, and et al. 2021. "SARS-CoV-2 Vaccine Willingness among Pregnant and Breastfeeding Women during the First Pandemic Wave: A Cross-Sectional Study in Switzerland" Viruses 13, no. 7: 1199. https://doi.org/10.3390/v13071199
APA StyleStuckelberger, S., Favre, G., Ceulemans, M., Nordeng, H., Gerbier, E., Lambelet, V., Stojanov, M., Winterfeld, U., Baud, D., Panchaud, A., & Pomar, L. (2021). SARS-CoV-2 Vaccine Willingness among Pregnant and Breastfeeding Women during the First Pandemic Wave: A Cross-Sectional Study in Switzerland. Viruses, 13(7), 1199. https://doi.org/10.3390/v13071199