
Viral Infection and Respiratory Exacerbation in Children: Results from a Local German Pediatric Exacerbation Cohort

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subject Description and Sample Collection
2.2. FilmArray Respiratory Panel Testing
2.3. Statistical Analyses
3. Results
3.1. Patient Characteristics
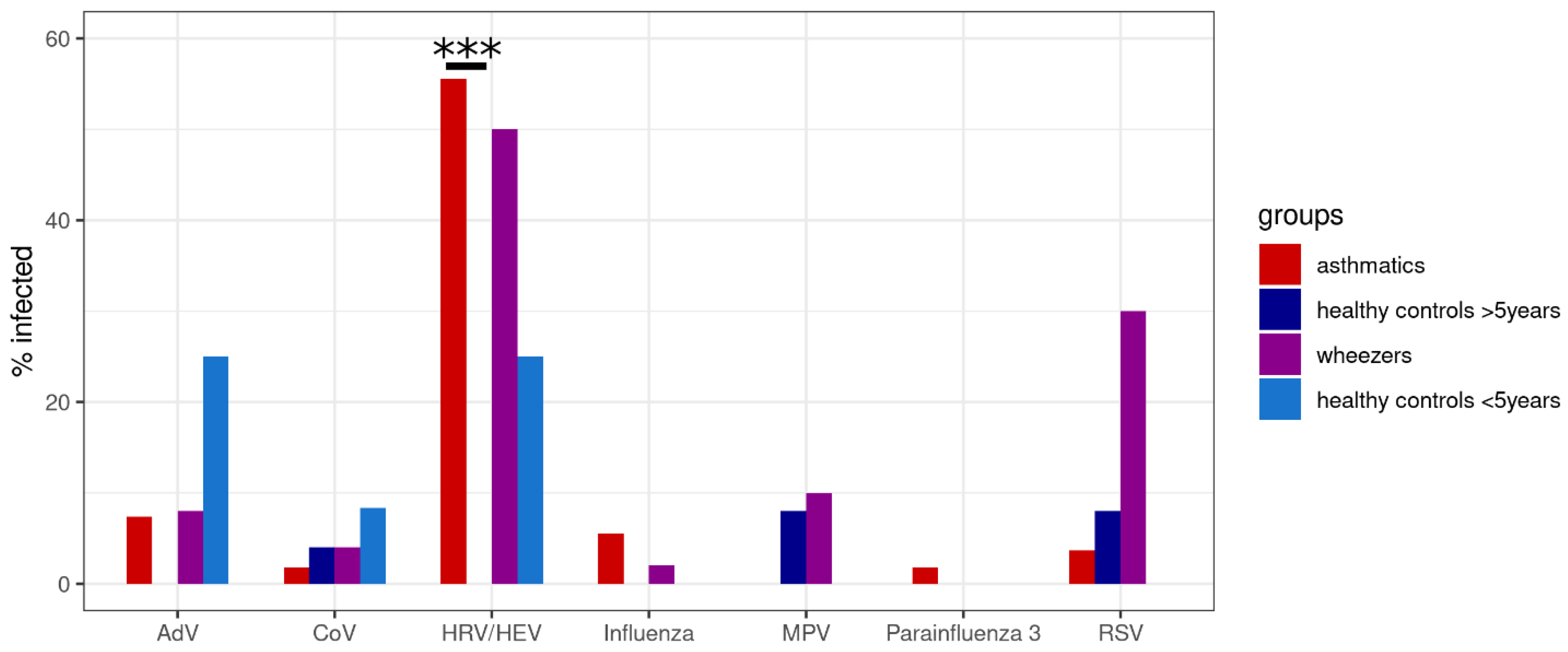
3.2. Rhinovirus and Respiratory Syncytial Virus Are Frequently Associated with Pediatric Exacerbation
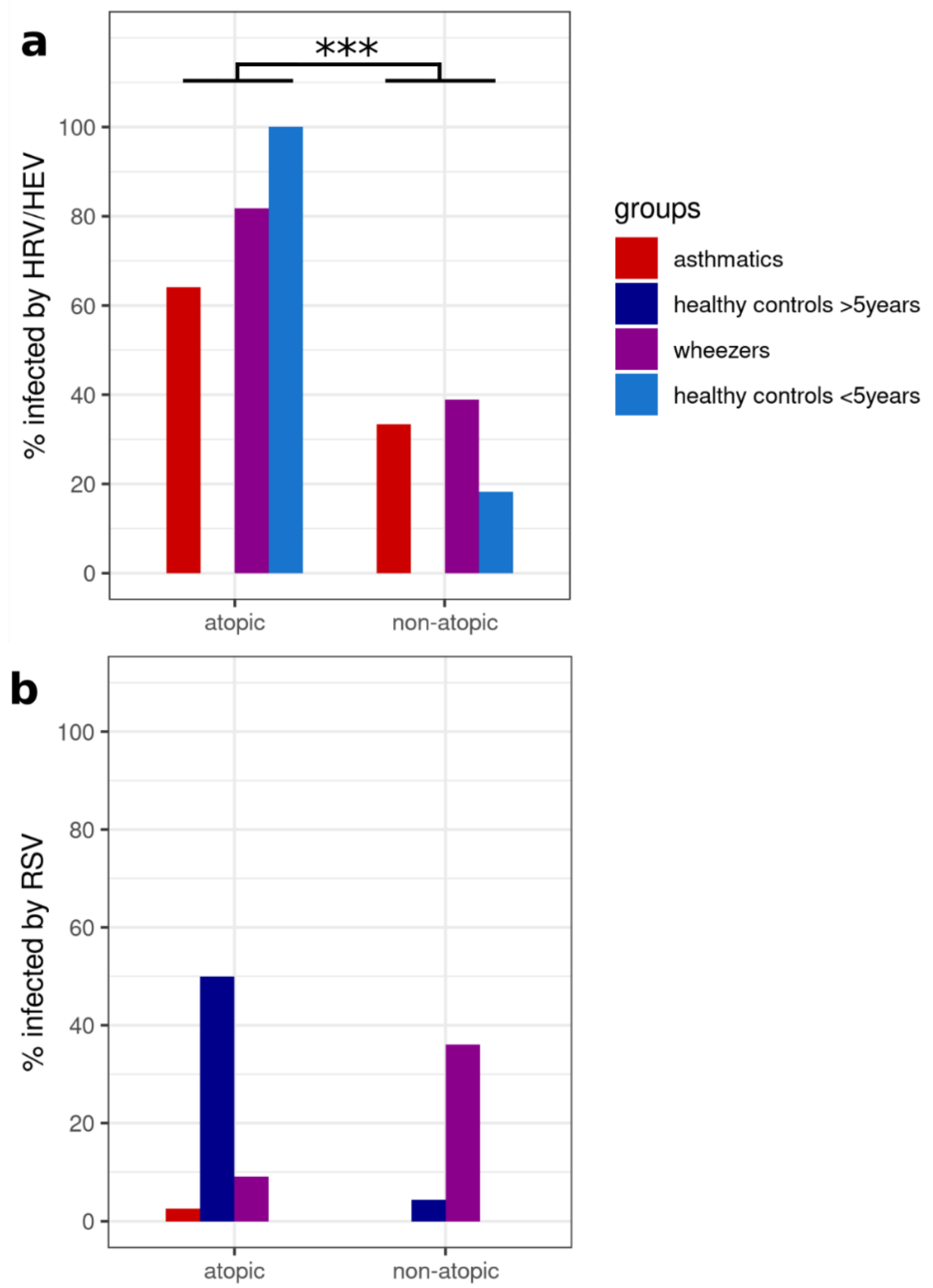
3.3. The Atopy Level Influences the Susceptibility of HRV Infection
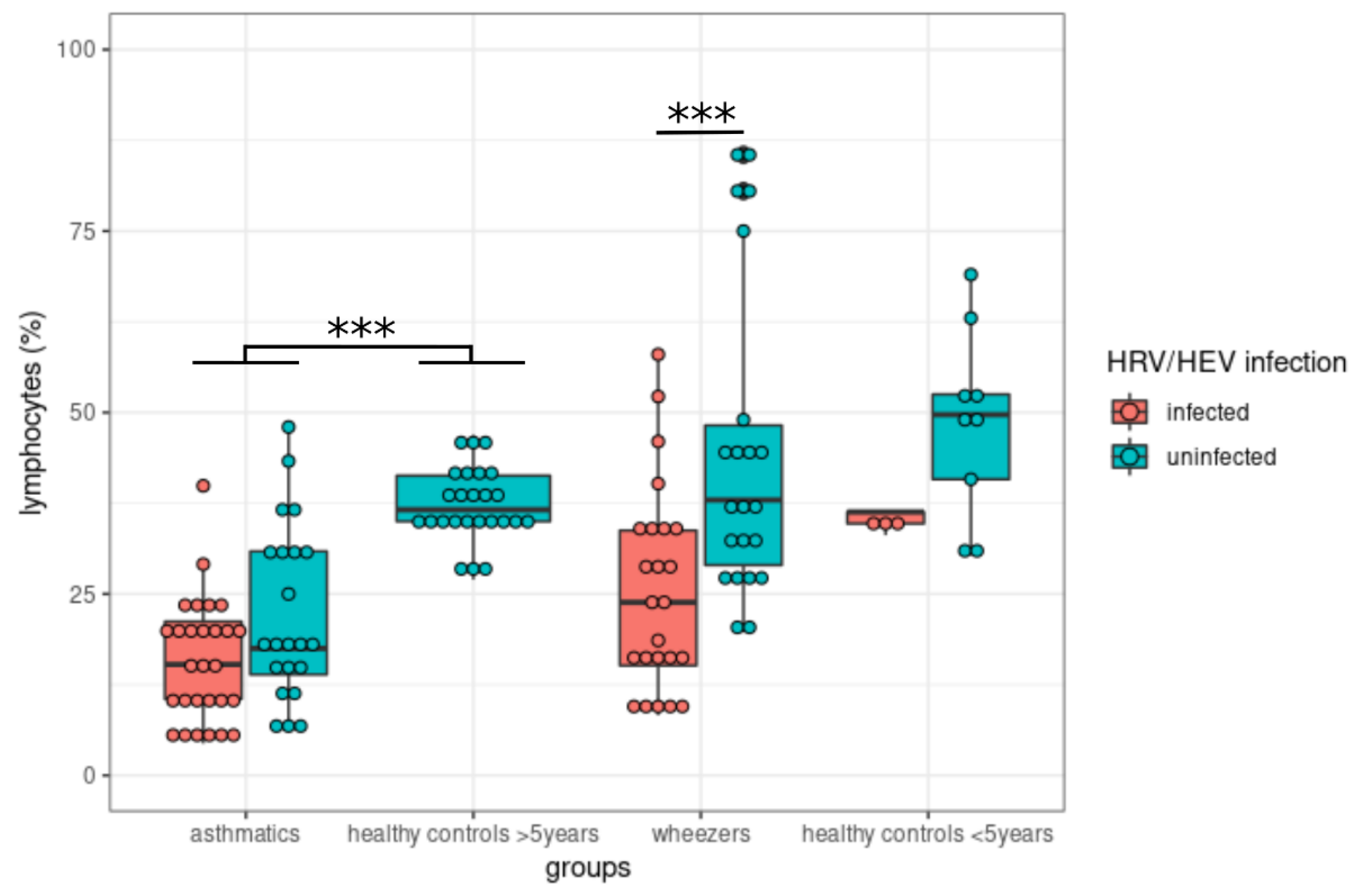
3.4. Rhinovirus Infection Influences Blood Lymphocyte Levels
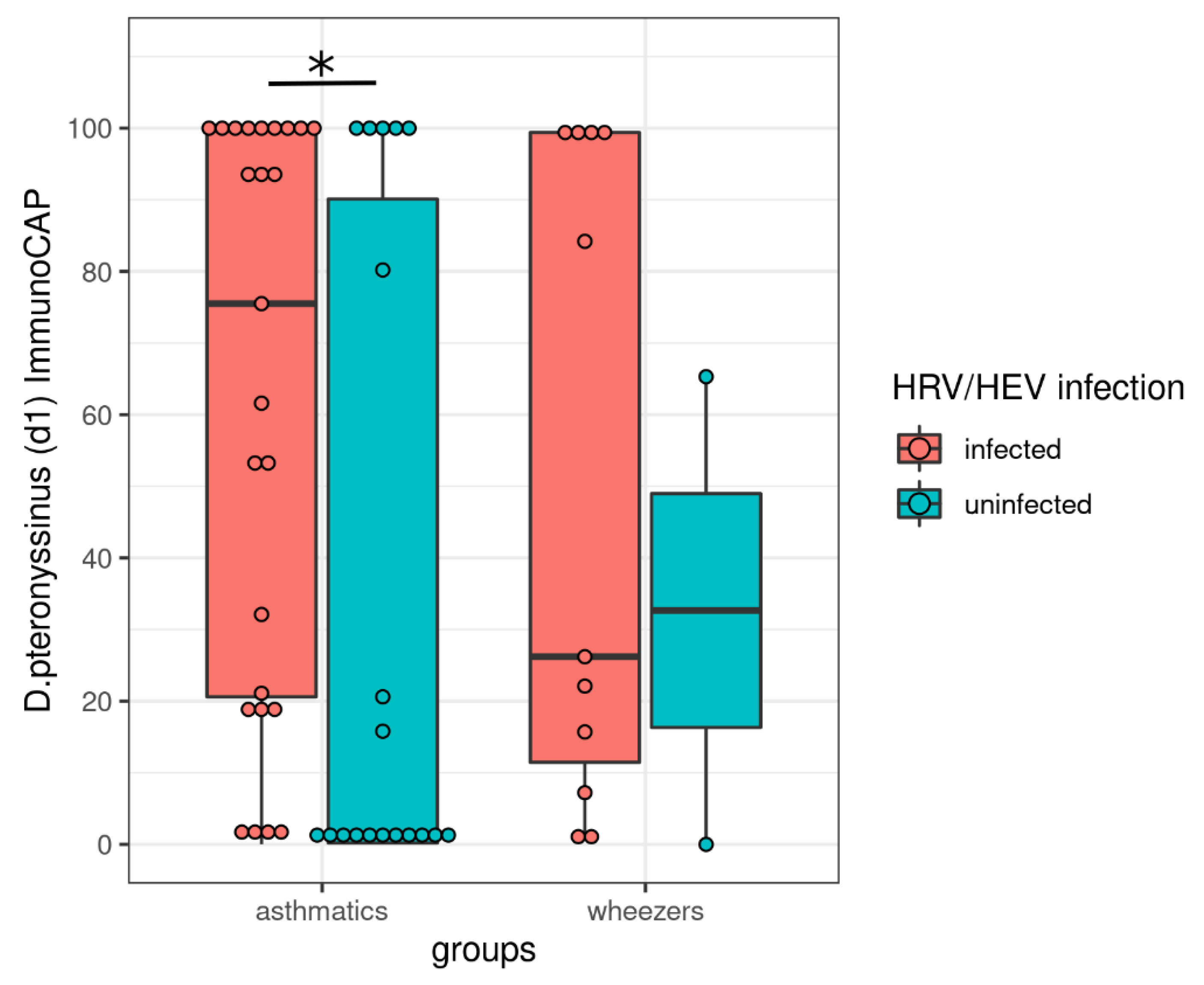
3.5. House Dust Mite Allergy Increases the Susceptibility to Rhinovirus Infection
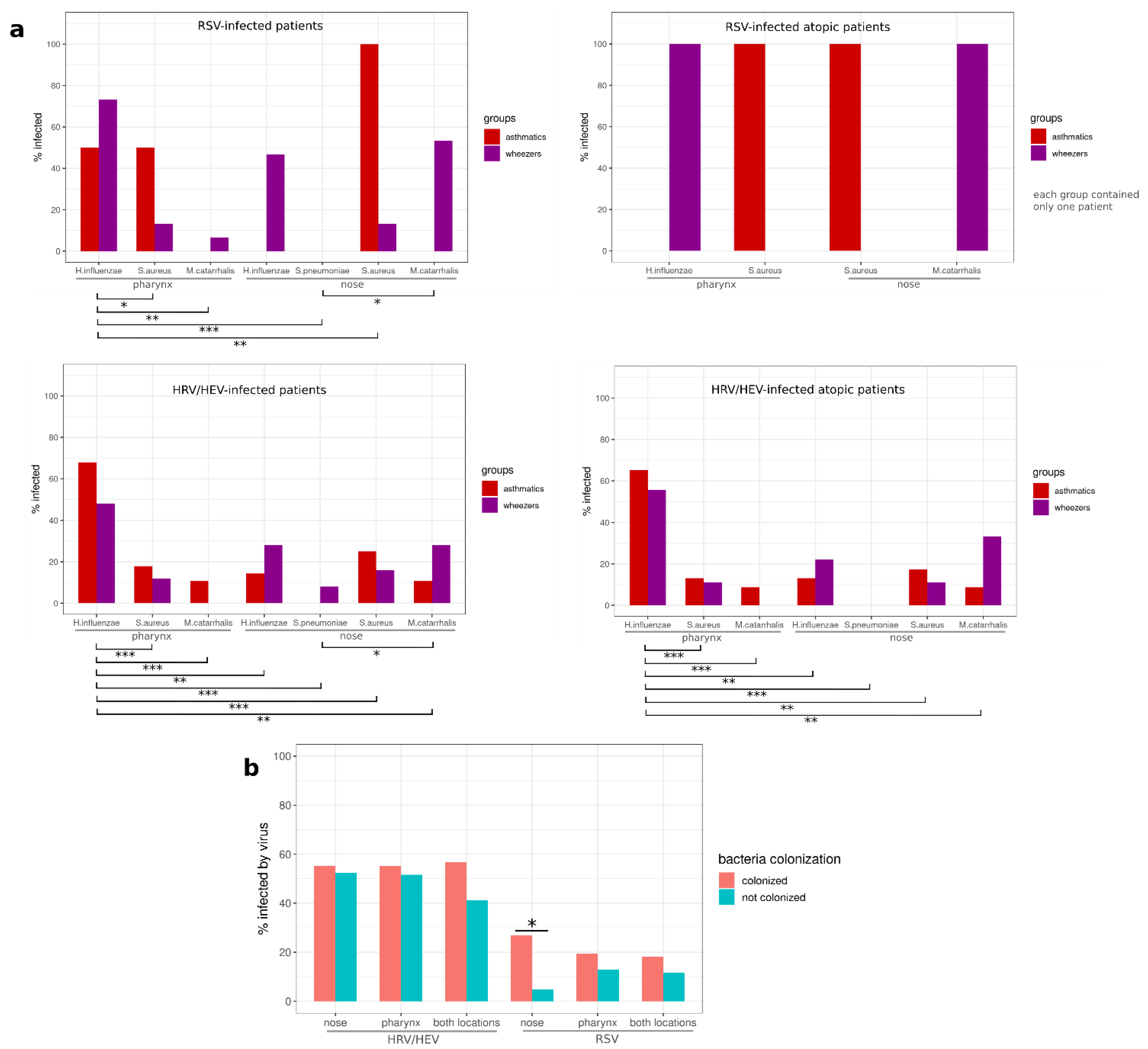
3.6. The Bacterial Colonization in the Nose or Pharynx Was Not Influenced by Asthma Phenotype among Virus-Infected Subjects
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ntontsi, P.; Photiades, A.; Zervas, E.; Xanthou, G.; Samitas, K. Genetics and Epigenetics in Asthma. Int. J. Mol. Sci. 2021, 22, 2412. [Google Scholar] [CrossRef] [PubMed]
- Vos, T.; Flaxman, A.D.; Naghavi, M.; Lozano, R.; Michaud, C.; Ezzati, M.; Shibuya, K.; Salomon, J.A.; Abdalla, S.; Aboyans, V.; et al. Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990-2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2163–2196. [Google Scholar] [CrossRef]
- Mallol, J.; Crane, J.; von Mutius, E.; Odhiambo, J.; Keil, U.; Stewart, A.; Group, I.P.T.S. The International Study of Asthma and Allergies in Childhood (ISAAC) Phase Three: A global synthesis. Allergol. Immunopathol. 2013, 41, 73–85. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pearce, N.; Ait-Khaled, N.; Beasley, R.; Mallol, J.; Keil, U.; Mitchell, E.; Robertson, C.; Group, I.P.T.S. Worldwide trends in the prevalence of asthma symptoms: Phase III of the International Study of Asthma and Allergies in Childhood (ISAAC). Thorax 2007, 62, 758–766. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dharmage, S.C.; Perret, J.L.; Custovic, A. Epidemiology of Asthma in Children and Adults. Front. Pediatr. 2019, 7, 246. [Google Scholar] [CrossRef]
- Diseases, G.B.D.; Injuries, C. Global burden of 369 diseases and injuries in 204 countries and territories, 1990-2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1204–1222. [Google Scholar] [CrossRef]
- The Global Asthma Report 2018; Global Asthma Network: Auckland, New Zealand, 2018.
- Akmatov, M.K.; Holstiege, J.; Steffen, A.; Batzing, J. Trends and regional distribution of outpatient claims for asthma, 2009-2016, Germany. Bull. World Health Organ. 2020, 98, 40–51. [Google Scholar] [CrossRef]
- Backer, V.; Harmsen, L.; Lund, T.; Pedersen, L.; Porsbjerg, C.; Rasmussen, L.; Thomsen, S.F.; Nolte, H. A 3-year longitudinal study of asthma quality of life in undiagnosed and diagnosed asthma patients. Int. J. Tuberc. Lung Dis. 2007, 11, 463–469. [Google Scholar]
- De Marco, R.; Cerveri, I.; Bugiani, M.; Ferrari, M.; Verlato, G. An undetected burden of asthma in Italy: The relationship between clinical and epidemiological diagnosis of asthma. Eur. Respir. J. 1998, 11, 599–605. [Google Scholar]
- Van Gent, R.; van Essen, L.E.; Rovers, M.M.; Kimpen, J.L.; van der Ent, C.K.; de Meer, G. Quality of life in children with undiagnosed and diagnosed asthma. Eur. J. Pediatr. 2007, 166, 843–848. [Google Scholar] [CrossRef] [Green Version]
- Wu, A.C.; Greenberger, P.A. Asthma: Overdiagnosed, Underdiagnosed, and Ineffectively Treated. J. Allergy Clin. Immunol. Pract. 2018, 6, 801–802. [Google Scholar] [CrossRef] [PubMed]
- Bundesärztekammer (BÄK); Kassenärztliche Bundesvereinigung (KBV). Arbeitsgemein-schaft der Wissenschaftlichen Medizinischen Fachgesellschaften (AWMF). Nationale VersorgungsLeitlinie Asthma—Langfassung. Auflage 2020, 4. [Google Scholar] [CrossRef]
- Burbank, A.J.; Sood, A.K.; Kesic, M.J.; Peden, D.B.; Hernandez, M.L. Environmental determinants of allergy and asthma in early life. J. Allergy Clin. Immunol. 2017, 140, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perez, L.; Declercq, C.; Iniguez, C.; Aguilera, I.; Badaloni, C.; Ballester, F.; Bouland, C.; Chanel, O.; Cirarda, F.B.; Forastiere, F.; et al. Chronic burden of near-roadway traffic pollution in 10 European cities (APHEKOM network). Eur. Respir. J. 2013, 42, 594–605. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Busse, W.W.; Lemanske, R.F., Jr.; Gern, J.E. Role of viral respiratory infections in asthma and asthma exacerbations. Lancet 2010, 376, 826–834. [Google Scholar] [CrossRef]
- Jartti, T.; Gern, J.E. Role of viral infections in the development and exacerbation of asthma in children. J. Allergy Clin. Immunol. 2017, 140, 895–906. [Google Scholar] [CrossRef] [Green Version]
- Ko, F.W.; Chan, P.K.; Chan, R.W.Y.; Chan, K.P.; Ip, A.; Kwok, A.; Ngai, J.C.; Ng, S.S.; On, C.T.; Hui, D.S. Molecular detection of respiratory pathogens and typing of human rhinovirus of adults hospitalized for exacerbation of asthma and chronic obstructive pulmonary disease. Respir. Res. 2019, 20, 210. [Google Scholar] [CrossRef]
- Merckx, J.; Ducharme, F.M.; Martineau, C.; Zemek, R.; Gravel, J.; Chalut, D.; Poonai, N.; Quach, C.; Pediatric Emergency Research Canada, D.T. Respiratory Viruses and Treatment Failure in Children with Asthma Exacerbation. Pediatrics 2018, 142. [Google Scholar] [CrossRef] [Green Version]
- Zheng, S.Y.; Wang, L.L.; Ren, L.; Luo, J.; Liao, W.; Liu, E.M. Epidemiological analysis and follow-up of human rhinovirus infection in children with asthma exacerbation. J. Med. Virol. 2018, 90, 219–228. [Google Scholar] [CrossRef]
- Borchers, A.T.; Chang, C.; Gershwin, M.E.; Gershwin, L.J. Respiratory syncytial virus—A comprehensive review. Clin. Rev. Allergy Immunol. 2013, 45, 331–379. [Google Scholar] [CrossRef]
- Chatziparasidis, G.; Kantar, A. COVID-19 in Children with Asthma. Lung 2021, 199, 7–12. [Google Scholar] [CrossRef] [PubMed]
- Chow, E.J.; Doyle, J.D.; Uyeki, T.M. Influenza virus-related critical illness: Prevention, diagnosis, treatment. Crit. Care 2019, 23, 214. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kumar, K.; Singanayagam, A.; Johnston, S.L. Respiratory Virus Infections in Asthma: Research Developments and Therapeutic Advances. Acta. Med. Acad. 2020, 49, 130–143. [Google Scholar] [CrossRef] [PubMed]
- Obuchi, M.; Adachi, Y.; Takizawa, T.; Sata, T. Influenza A(H1N1)pdm09 virus and asthma. Front. Microbiol. 2013, 4, 307. [Google Scholar] [CrossRef] [Green Version]
- Radzikowska, U.; Ding, M.; Tan, G.; Zhakparov, D.; Peng, Y.; Wawrzyniak, P.; Wang, M.; Li, S.; Morita, H.; Altunbulakli, C.; et al. Distribution of ACE2, CD147, CD26, and other SARS-CoV-2 associated molecules in tissues and immune cells in health and in asthma, COPD, obesity, hypertension, and COVID-19 risk factors. Allergy 2020, 75, 2829–2845. [Google Scholar] [CrossRef]
- Sienko, J.; Kotowski, M.; Bogacz, A.; Lechowicz, K.; Drozdzal, S.; Rosik, J.; Sietnicki, M.; Sienko, M.; Kotfis, K. COVID-19: The Influence of ACE Genotype and ACE-I and ARBs on the Course of SARS-CoV-2 Infection in Elderly Patients. Clin. Interv. Aging 2020, 15, 1231–1240. [Google Scholar] [CrossRef]
- Tay, H.; Wark, P.A.; Bartlett, N.W. Advances in the treatment of virus-induced asthma. Expert Rev. Respir. Med. 2016, 10, 629–641. [Google Scholar] [CrossRef]
- Cipriani, F.; Calamelli, E.; Ricci, G. Allergen Avoidance in Allergic Asthma. Front. Pediatr 2017, 5, 103. [Google Scholar] [CrossRef] [Green Version]
- Guibas, G.V.; Mathioudakis, A.G.; Tsoumani, M.; Tsabouri, S. Relationship of Allergy with Asthma: There Are More Than the Allergy "Eggs" in the Asthma ”Basket”. Front. Pediatr. 2017, 5, 92. [Google Scholar] [CrossRef] [Green Version]
- Hashmi, M.F.; Tariq, M.; Cataletto, M.E. Asthma. In StatPearls; StatPearls: Treasure Island, FL, USA, 2022. [Google Scholar]
- Locksley, R.M. Asthma and allergic inflammation. Cell 2010, 140, 777–783. [Google Scholar] [CrossRef] [Green Version]
- Quirt, J.; Hildebrand, K.J.; Mazza, J.; Noya, F.; Kim, H. Asthma. Allergy Asthma Clin. Immunol. 2018, 14, 50. [Google Scholar] [CrossRef] [PubMed]
- Finotto, S. Resolution of allergic asthma. Semin Immunopathol. 2019, 41, 665–674. [Google Scholar] [CrossRef] [PubMed]
- Tesch, F.; Sydendal Grand, T.; Wuestenberg, E.; Elliott, L.; Schmitt, J.; Kuster, D. Healthcare costs associated with allergic rhinitis, asthma allergy immunotherapy. Eur Ann. Allergy Clin. Immunol. 2020, 52, 164–174. [Google Scholar] [CrossRef] [PubMed]
- Hsu, J.; Qin, X.; Beavers, S.F.; Mirabelli, M.C. Asthma-Related School Absenteeism, Morbidity, and Modifiable Factors. Am. J. Prev. Med. 2016, 51, 23–32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bergroth, E.; Aakula, M.; Elenius, V.; Remes, S.; Piippo-Savolainen, E.; Korppi, M.; Piedra, P.A.; Bochkov, Y.A.; Gern, J.E.; Camargo, C.A., Jr.; et al. Rhinovirus Type in Severe Bronchiolitis and the Development of Asthma. J. Allergy Clin. Immunol. Pract. 2020, 8, 588–595.e584. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.; Pan, Y.; Zhu, Y.; Song, Y.; Su, X.; Yang, L.; Li, M. Association between rhinovirus wheezing illness and the development of childhood asthma: A meta-analysis. BMJ Open 2017, 7, e013034. [Google Scholar] [CrossRef] [Green Version]
- Muehling, L.M.; Heymann, P.W.; Wright, P.W.; Eccles, J.D.; Agrawal, R.; Carper, H.T.; Murphy, D.D.; Workman, L.J.; Word, C.R.; Ratcliffe, S.J.; et al. Human TH1 and TH2 cells targeting rhinovirus and allergen coordinately promote allergic asthma. J. Allergy Clin. Immunol. 2020, 146, 555–570. [Google Scholar] [CrossRef]
- Williams, T.C.; Jackson, D.J.; Maltby, S.; Walton, R.P.; Ching, Y.M.; Glanville, N.; Singanayagam, A.; Brewins, J.J.; Clarke, D.; Hirsman, A.G.; et al. Rhinovirus-induced CCL17 and CCL22 in Asthma Exacerbations and Differential Regulation by STAT6. Am. J. Respir Cell Mol. Biol. 2021, 64, 344–356. [Google Scholar] [CrossRef]
- Coutts, J.; Fullarton, J.; Morris, C.; Grubb, E.; Buchan, S.; Rodgers-Gray, B.; Thwaites, R. Association between respiratory syncytial virus hospitalization in infancy and childhood asthma. Pediatr. Pulmonol. 2020, 55, 1104–1110. [Google Scholar] [CrossRef] [Green Version]
- Ruotsalainen, M.; Hyvarinen, M.K.; Piippo-Savolainen, E.; Korppi, M. Adolescent asthma after rhinovirus and respiratory syncytial virus bronchiolitis. Pediatr. Pulmonol. 2013, 48, 633–639. [Google Scholar] [CrossRef]
- Coverstone, A.M.; Wang, L.; Sumino, K. Beyond Respiratory Syncytial Virus and Rhinovirus in the Pathogenesis and Exacerbation of Asthma: The Role of Metapneumovirus, Bocavirus and Influenza Virus. Immunol. Allergy Clin. N. Am. 2019, 39, 391–401. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Garcia, M.L.; Calvo Rey, C.; Del Rosal Rabes, T. Pediatric Asthma and Viral Infection. Arch. Bronconeumol. 2016, 52, 269–273. [Google Scholar] [CrossRef]
- Jartti, T.; Bonnelykke, K.; Elenius, V.; Feleszko, W. Role of viruses in asthma. Semin. Immunopathol. 2020, 42, 61–74. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guilbert, T.W.; Singh, A.M.; Danov, Z.; Evans, M.D.; Jackson, D.J.; Burton, R.; Roberg, K.A.; Anderson, E.L.; Pappas, T.E.; Gangnon, R.; et al. Decreased lung function after preschool wheezing rhinovirus illnesses in children at risk to develop asthma. J. Allergy Clin. Immunol. 2011, 128, 532–538.e10. [Google Scholar] [CrossRef]
- Jackson, D.J.; Gangnon, R.E.; Evans, M.D.; Roberg, K.A.; Anderson, E.L.; Pappas, T.E.; Printz, M.C.; Lee, W.M.; Shult, P.A.; Reisdorf, E.; et al. Wheezing rhinovirus illnesses in early life predict asthma development in high-risk children. Am. J. Respir. Crit. Care Med. 2008, 178, 667–672. [Google Scholar] [CrossRef] [PubMed]
- Rubner, F.J.; Jackson, D.J.; Evans, M.D.; Gangnon, R.E.; Tisler, C.J.; Pappas, T.E.; Gern, J.E.; Lemanske, R.F., Jr. Early life rhinovirus wheezing, allergic sensitization, and asthma risk at adolescence. J. Allergy Clin. Immunol. 2017, 139, 501–507. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sigurs, N.; Bjarnason, R.; Sigurbergsson, F.; Kjellman, B. Respiratory syncytial virus bronchiolitis in infancy is an important risk factor for asthma and allergy at age 7. Am. J. Respir. Crit. Care Med. 2000, 161, 1501–1507. [Google Scholar] [CrossRef]
- Sigurs, N.; Bjarnason, R.; Sigurbergsson, F.; Kjellman, B.; Bjorksten, B. Asthma and immunoglobulin E antibodies after respiratory syncytial virus bronchiolitis: A prospective cohort study with matched controls. Pediatrics 1995, 95, 500–505. [Google Scholar] [CrossRef]
- Sigurs, N.; Gustafsson, P.M.; Bjarnason, R.; Lundberg, F.; Schmidt, S.; Sigurbergsson, F.; Kjellman, B. Severe respiratory syncytial virus bronchiolitis in infancy and asthma and allergy at age 13. Am. J. Respir. Crit. Care Med. 2005, 171, 137–141. [Google Scholar] [CrossRef]
- Aydin, M.; Naumova, E.A.; Lutz, S.; Meyer-Bahlburg, A.; Arnold, W.H.; Kreppel, F.; Ehrhardt, A.; Postberg, J.; Wirth, S. Do Current Asthma-Preventive Measures Appropriately Face the World Health Organization’s Concerns: A Study Presentation of a New Clinical, Prospective, Multicentric Pediatric Asthma Exacerbation Cohort in Germany. Front. Pediatr. 2020, 8, 574462. [Google Scholar] [CrossRef]
- Engelkes, M.; Baan, E.J.; de Ridder, M.A.J.; Svensson, E.; Prieto-Alhambra, D.; Lapi, F.; Giaquinto, C.; Picelli, G.; Boudiaf, N.; Albers, F.; et al. Incidence, risk factors and re-exacerbation rate of severe asthma exacerbations in a multinational, multidatabase pediatric cohort study. Pediatr. Allergy Immunol. 2020, 31, 496–505. [Google Scholar] [CrossRef] [PubMed]
- Nasreen, S.; Wilk, P.; Mullowney, T.; Karp, I. Asthma exacerbation trajectories and their predictors in children with incident asthma. Ann. Allergy Asthma Immunol. 2019, 123, 293–300.e292. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Global Initiative for Asthma. Global Strategy for Asthma Management and Prevention. 2021. Available online: www.ginasthma.org (accessed on 10 December 2021).
- Thomas, M.; Kay, S.; Pike, J.; Williams, A.; Rosenzweig, J.R.; Hillyer, E.V.; Price, D. The Asthma Control Test (ACT) as a predictor of GINA guideline-defined asthma control: Analysis of a multinational cross-sectional survey. Prim. Care Respir. J. 2009, 18, 41–49. [Google Scholar] [CrossRef] [Green Version]
- Aydin, M.; Weisser, C.; Rué, O.; Mariadassou, M.; Maaß, S.; Behrendt, A.-K.; Jaszczyszyn, Y.; Heilker, T.; Spaeth, M.; Vogel, S.; et al. The Rhinobiome of Exacerbated Wheezers and Asthmatics: Insights From a German Pediatric Exacerbation Network. Front. Allergy 2021, 2, 667562. [Google Scholar] [CrossRef]
- Leber, A.L.; Everhart, K.; Daly, J.A.; Hopper, A.; Harrington, A.; Schreckenberger, P.; McKinley, K.; Jones, M.; Holmberg, K.; Kensinger, B. Multicenter Evaluation of BioFire FilmArray Respiratory Panel 2 for Detection of Viruses and Bacteria in Nasopharyngeal Swab Samples. J. Clin. Microbiol 2018, 56, e01945-17. [Google Scholar] [CrossRef] [Green Version]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2020. [Google Scholar]
- Hadley, W.; François, R.; Henry, L.; Müller, K. dplyr: A Grammar of Data Manipulation. R Package Version 1.0.7; 2021. [Google Scholar]
- David Meyer, A.Z.; Hornik, K. vcd: Visualizing Categorical Data. R Package Version 1.4–9; 2021. [Google Scholar]
- Wickham, H. ggplot2: Elegant Graphics for Data Analysis; Springer: New York, NY, USA, 2016. [Google Scholar]
- Komlosi, Z.I.; van de Veen, W.; Kovacs, N.; Szucs, G.; Sokolowska, M.; O’Mahony, L.; Akdis, M.; Akdis, C.A. Cellular and molecular mechanisms of allergic asthma. Mol. Aspects Med. 2021, 100995. [Google Scholar] [CrossRef]
- Mims, J.W. Asthma: Definitions and pathophysiology. Int. Forum Allergy Rhinol. 2015, 5, S2–S6. [Google Scholar] [CrossRef]
- Holt, P.G. Developmental factors as determinants of risk for infections and atopy in childhood. Eur. Respir. Rev. 2005, 14, 69–73. [Google Scholar] [CrossRef] [Green Version]
- Martinez, F.D. Heterogeneity of the association between lower respiratory illness in infancy and subsequent asthma. Proc. Am. Thorac Soc. 2005, 2, 157–161. [Google Scholar] [CrossRef]
- Nicholas, B.; Dudley, S.; Tariq, K.; Howarth, P.; Lunn, K.; Pink, S.; Sterk, P.J.; Adcock, I.M.; Monk, P.; Djukanovic, R.; et al. Susceptibility to influenza virus infection of bronchial biopsies in asthma. J. Allergy Clin. Immunol. 2017, 140, 309–312.e304. [Google Scholar] [CrossRef] [Green Version]
- Van Kerkhove, M.D.; Vandemaele, K.A.; Shinde, V.; Jaramillo-Gutierrez, G.; Koukounari, A.; Donnelly, C.A.; Carlino, L.O.; Owen, R.; Paterson, B.; Pelletier, L.; et al. Risk factors for severe outcomes following 2009 influenza A (H1N1) infection: A global pooled analysis. PLoS Med. 2011, 8, e1001053. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, J.M.; Koh, H.Y.; Moon, S.Y.; Yoo, I.K.; Ha, E.K.; You, S.; Kim, S.Y.; Yon, D.K.; Lee, S.W. Allergic disorders and susceptibility to and severity of COVID-19: A nationwide cohort study. J. Allergy Clin. Immunol. 2020, 146, 790–798. [Google Scholar] [CrossRef] [PubMed]
- Kuruvilla, M.E.; Lee, F.E.; Lee, G.B. Understanding Asthma Phenotypes, Endotypes, and Mechanisms of Disease. Clin. Rev. Allergy Immunol. 2019, 56, 219–233. [Google Scholar] [CrossRef]
- Cabana, M.D.; McKean, M.; Caughey, A.B.; Fong, L.; Lynch, S.; Wong, A.; Leong, R.; Boushey, H.A.; Hilton, J.F. Early Probiotic Supplementation for Eczema and Asthma Prevention: A Randomized Controlled Trial. Pediatrics 2017, 140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Forno, E.; Bacharier, L.B.; Phipatanakul, W.; Guilbert, T.W.; Cabana, M.D.; Ross, K.; Covar, R.; Gern, J.E.; Rosser, F.J.; Blatter, J.; et al. Effect of Vitamin D3 Supplementation on Severe Asthma Exacerbations in Children with Asthma and Low Vitamin D Levels: The VDKA Randomized Clinical Trial. JAMA 2020, 324, 752–760. [Google Scholar] [CrossRef]
- Greer, F.R.; Sicherer, S.H.; Burks, A.W.; Committee on Nutrition; Section on Allergy and Immunology. The Effects of Early Nutritional Interventions on the Development of Atopic Disease in Infants and Children: The Role of Maternal Dietary Restriction, Breastfeeding, Hydrolyzed Formulas, and Timing of Introduction of Allergenic Complementary Foods. Pediatrics 2019, 143, e20190281. [Google Scholar] [CrossRef] [Green Version]
- Guilbert, T.W.; Morgan, W.J.; Krawiec, M.; Lemanske, R.F., Jr.; Sorkness, C.; Szefler, S.J.; Larsen, G.; Spahn, J.D.; Zeiger, R.S.; Heldt, G.; et al. The Prevention of Early Asthma in Kids study: Design, rationale and methods for the Childhood Asthma Research and Education network. Control Clin. Trials 2004, 25, 286–310. [Google Scholar] [CrossRef]
- Mastrorilli, C.; Caffarelli, C.; Hoffmann-Sommergruber, K. Food allergy and atopic dermatitis: Prediction, progression, and prevention. Pediatr. Allergy Immunol. 2017, 28, 831–840. [Google Scholar] [CrossRef]
- Menzies-Gow, A.; Busse, W.W.; Castro, M.; Jackson, D.J. Prevention and Treatment of Asthma Exacerbations in Adults. J. Allergy Clin. Immunol. Pract. 2021, 9, 2578–2586. [Google Scholar] [CrossRef]
- Murray, C.S.; Foden, P.; Sumner, H.; Shepley, E.; Custovic, A.; Simpson, A. Preventing Severe Asthma Exacerbations in Children. A Randomized Trial of Mite-Impermeable Bedcovers. Am. J. Respir. Crit. Care Med. 2017, 196, 150–158. [Google Scholar] [CrossRef]
- Nicholson, P.J.; Cullinan, P.; Burge, S.; British Occupational Health Research, F. Concise guidance: Diagnosis, management and prevention of occupational asthma. Clin. Med. 2012, 12, 156–159. [Google Scholar] [CrossRef] [PubMed]
- Tachimoto, H.; Imanari, E.; Mezawa, H.; Okuyama, M.; Urashima, T.; Hirano, D.; Gocho, N.; Urashima, M. Effect of Avoiding Cow’s Milk Formula at Birth on Prevention of Asthma or Recurrent Wheeze Among Young Children: Extended Follow-up from the ABC Randomized Clinical Trial. JAMA Netw Open 2020, 3, e2018534. [Google Scholar] [CrossRef] [PubMed]
- Agache, I.; Beltran, J.; Akdis, C.; Akdis, M.; Canelo-Aybar, C.; Canonica, G.W.; Casale, T.; Chivato, T.; Corren, J.; Del Giacco, S.; et al. Efficacy and safety of treatment with biologicals (benralizumab, dupilumab, mepolizumab, omalizumab and reslizumab) for severe eosinophilic asthma. A systematic review for the EAACI Guidelines—Recommendations on the use of biologicals in severe asthma. Allergy 2020, 75, 1023–1042. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chapman, K.R.; Albers, F.C.; Chipps, B.; Munoz, X.; Devouassoux, G.; Bergna, M.; Galkin, D.; Azmi, J.; Mouneimne, D.; Price, R.G.; et al. The clinical benefit of mepolizumab replacing omalizumab in uncontrolled severe eosinophilic asthma. Allergy 2019, 74, 1716–1726. [Google Scholar] [CrossRef] [Green Version]
- Ortega, H.G.; Liu, M.C.; Pavord, I.D.; Brusselle, G.G.; FitzGerald, J.M.; Chetta, A.; Humbert, M.; Katz, L.E.; Keene, O.N.; Yancey, S.W.; et al. Mepolizumab treatment in patients with severe eosinophilic asthma. N. Engl. J. Med. 2014, 371, 1198–1207. [Google Scholar] [CrossRef] [Green Version]
- Soong, W.; Yoo, B.; Pazwash, H.; Holweg, C.T.J.; Casale, T.B. Omalizumab response in patients with asthma by number and type of allergen. Ann. Allergy Asthma Immunol. 2021, 127, 223–231. [Google Scholar] [CrossRef]
- Chau-Etchepare, F.; Hoerger, J.L.; Kuhn, B.T.; Zeki, A.A.; Haczku, A.; Louie, S.; Kenyon, N.J.; Davis, C.E.; Schivo, M. Viruses and non-allergen environmental triggers in asthma. J. Investig. Med. 2019, 67, 1029–1041. [Google Scholar] [CrossRef] [Green Version]
- Costa, L.D.; Costa, P.S.; Camargos, P.A. Exacerbation of asthma and airway infection: Is the virus the villain? J. Pediatr. 2014, 90, 542–555. [Google Scholar] [CrossRef] [Green Version]
- Deschildre, A.; Pichavant, M.; Engelmann, I.; Langlois, C.; Drumez, E.; Pouessel, G.; Boileau, S.; Romero-Cubero, D.; Decleyre-Badiu, I.; Dewilde, A.; et al. Virus-triggered exacerbation in allergic asthmatic children: Neutrophilic airway inflammation and alteration of virus sensors characterize a subgroup of patients. Respir. Res. 2017, 18, 191. [Google Scholar] [CrossRef] [Green Version]
- Zhu, J.; Message, S.D.; Mallia, P.; Kebadze, T.; Contoli, M.; Ward, C.K.; Barnathan, E.S.; Mascelli, M.A.; Kon, O.M.; Papi, A.; et al. Bronchial mucosal IFN-alpha/beta and pattern recognition receptor expression in patients with experimental rhinovirus-induced asthma exacerbations. J. Allergy Clin. Immunol. 2019, 143, 114–125.e114. [Google Scholar] [CrossRef] [Green Version]
- Biagi, C.; Rocca, A.; Poletti, G.; Fabi, M.; Lanari, M. Rhinovirus Infection in Children with Acute Bronchiolitis and Its Impact on Recurrent Wheezing and Asthma Development. Microorganisms 2020, 8, 1620. [Google Scholar] [CrossRef] [PubMed]
- Ferolla, F.M.; Hijano, D.R.; Acosta, P.L.; Rodriguez, A.; Duenas, K.; Sancilio, A.; Barboza, E.; Caria, A.; Gago, G.F.; Almeida, R.E.; et al. Macronutrients during pregnancy and life-threatening respiratory syncytial virus infections in children. Am. J. Respir. Crit. Care Med. 2013, 187, 983–990. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, J.L.; Pham, S.; Borish, L. Rhinovirus and Asthma Exacerbations. Immunol. Allergy Clin. N. Am. 2019, 39, 335–344. [Google Scholar] [CrossRef] [PubMed]
- Niespodziana, K.; Stenberg-Hammar, K.; Megremis, S.; Cabauatan, C.R.; Napora-Wijata, K.; Vacal, P.C.; Gallerano, D.; Lupinek, C.; Ebner, D.; Schlederer, T.; et al. PreDicta chip-based high resolution diagnosis of rhinovirus-induced wheeze. Nat. Commun. 2018, 9, 2382. [Google Scholar] [CrossRef]
- Real-Hohn, A.; Blaas, D. Rhinovirus Inhibitors: Including a New Target, the Viral RNA. Viruses 2021, 13, 1784. [Google Scholar] [CrossRef]
- Tang, J.W.; Loh, T.P. Correlations between climate factors and incidence--a contributor to RSV seasonality. Rev. Med. Virol. 2014, 24, 15–34. [Google Scholar] [CrossRef]
- Teeratakulpisarn, J.; Pientong, C.; Ekalaksananan, T.; Ruangsiripiyakul, H.; Uppala, R. Rhinovirus infection in children hospitalized with acute bronchiolitis and its impact on subsequent wheezing or asthma: A comparison of etiologies. Asian Pac. J. Allergy Immunol. 2014, 32, 226–234. [Google Scholar] [CrossRef]
- Zhou, Y.; Tong, L.; Li, M.; Wang, Y.; Li, L.; Yang, D.; Zhang, Y.; Chen, Z. Recurrent Wheezing and Asthma After Respiratory Syncytial Virus Bronchiolitis. Front. Pediatr. 2021, 9, 649003. [Google Scholar] [CrossRef]
- Elnifro, E.M.; Ashshi, A.M.; Cooper, R.J.; Klapper, P.E. Multiplex PCR: Optimization and application in diagnostic virology. Clin. Microbiol. Rev. 2000, 13, 559–570. [Google Scholar] [CrossRef]
- Vila, J.; Gomez, M.D.; Salavert, M.; Bosch, J. [Methods of rapid diagnosis in clinical microbiology: Clinical needs]. Enferm. Infecc. Microbiol. Clin. 2017, 35, 41–46. [Google Scholar] [CrossRef]
- De Kluijver, J.; Evertse, C.E.; Sont, J.K.; Schrumpf, J.A.; van Zeijl-van der Ham, C.J.; Dick, C.R.; Rabe, K.F.; Hiemstra, P.S.; Sterk, P.J. Are rhinovirus-induced airway responses in asthma aggravated by chronic allergen exposure? Am. J. Respir. Crit. Care Med. 2003, 168, 1174–1180. [Google Scholar] [CrossRef] [Green Version]
- Yang, Z.; Mitlander, H.; Vuorinen, T.; Finotto, S. Mechanism of Rhinovirus Immunity and Asthma. Front. Immunol. 2021, 12, 731846. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, S.E.; Lamson, D.M.; St George, K.; Walsh, T.J. Human rhinoviruses. Clin. Microbiol. Rev. 2013, 26, 135–162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kerr, S.L.; Mathew, C.; Ghildyal, R. Rhinovirus and Cell Death. Viruses 2021, 13, 629. [Google Scholar] [CrossRef] [PubMed]
- Rossmann, M.G.; Arnold, E.; Erickson, J.W.; Frankenberger, E.A.; Griffith, J.P.; Hecht, H.J.; Johnson, J.E.; Kamer, G.; Luo, M.; Mosser, A.G.; et al. Structure of a human common cold virus and functional relationship to other picornaviruses. Nature 1985, 317, 145–153. [Google Scholar] [CrossRef]
- Basnet, S.; Palmenberg, A.C.; Gern, J.E. Rhinoviruses and Their Receptors. Chest 2019, 155, 1018–1025. [Google Scholar] [CrossRef]
- Schober, D.; Kronenberger, P.; Prchla, E.; Blaas, D.; Fuchs, R. Major and minor receptor group human rhinoviruses penetrate from endosomes by different mechanisms. J. Virol. 1998, 72, 1354–1364. [Google Scholar] [CrossRef] [Green Version]
- Hewson, C.A.; Jardine, A.; Edwards, M.R.; Laza-Stanca, V.; Johnston, S.L. Toll-like receptor 3 is induced by and mediates antiviral activity against rhinovirus infection of human bronchial epithelial cells. J. Virol. 2005, 79, 12273–12279. [Google Scholar] [CrossRef] [Green Version]
- Triantafilou, K.; Vakakis, E.; Richer, E.A.; Evans, G.L.; Villiers, J.P.; Triantafilou, M. Human rhinovirus recognition in non-immune cells is mediated by Toll-like receptors and MDA-5, which trigger a synergetic pro-inflammatory immune response. Virulence 2011, 2, 22–29. [Google Scholar] [CrossRef] [Green Version]
- Hasegawa, K.; Mansbach, J.M.; Camargo, C.A., Jr. Infectious pathogens and bronchiolitis outcomes. Expert Rev. Anti-Infect. Ther. 2014, 12, 817–828. [Google Scholar] [CrossRef]
- Bakaletz, L.O. Viral-bacterial co-infections in the respiratory tract. Curr. Opin. Microbiol. 2017, 35, 30–35. [Google Scholar] [CrossRef] [PubMed]
- Lednicky, J.A.; Rayner, J.O. Uncommon respiratory pathogens. Curr. Opin. Pulm. Med. 2006, 12, 235–239. [Google Scholar] [CrossRef] [PubMed]
- Man, W.H.; de Steenhuijsen Piters, W.A.; Bogaert, D. The microbiota of the respiratory tract: Gatekeeper to respiratory health. Nat. Rev. Microbiol. 2017, 15, 259–270. [Google Scholar] [CrossRef]
- Pendleton, K.M.; Huffnagle, G.B.; Dickson, R.P. The significance of Candida in the human respiratory tract: Our evolving understanding. Pathog. Dis. 2017, 75, ftx029. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reckziegel, M.; Weber-Osel, C.; Egerer, R.; Gruhn, B.; Kubek, F.; Walther, M.; Wilhelm, S.; Zell, R.; Krumbholz, A. Viruses and atypical bacteria in the respiratory tract of immunocompromised and immunocompetent patients with airway infection. Eur J. Clin. Microbiol. Infect. Dis. 2020, 39, 1581–1592. [Google Scholar] [CrossRef] [PubMed]
- Dinwiddie, D.L.; Denson, J.L.; Kennedy, J.L. Role of the Airway Microbiome in Respiratory Infections and Asthma in Children. Pediatr. Allergy Immunol. Pulmonol. 2018, 31, 236–240. [Google Scholar] [CrossRef] [PubMed]
- Berg, G.; Rybakova, D.; Fischer, D.; Cernava, T.; Verges, M.C.; Charles, T.; Chen, X.; Cocolin, L.; Eversole, K.; Corral, G.H.; et al. Microbiome definition re-visited: Old concepts and new challenges. Microbiome 2020, 8, 103. [Google Scholar] [CrossRef]
- David, L.A.; Maurice, C.F.; Carmody, R.N.; Gootenberg, D.B.; Button, J.E.; Wolfe, B.E.; Ling, A.V.; Devlin, A.S.; Varma, Y.; Fischbach, M.A.; et al. Diet rapidly and reproducibly alters the human gut microbiome. Nature 2014, 505, 559–563. [Google Scholar] [CrossRef] [Green Version]
- Depner, M.; Taft, D.H.; Kirjavainen, P.V.; Kalanetra, K.M.; Karvonen, A.M.; Peschel, S.; Schmausser-Hechfellner, E.; Roduit, C.; Frei, R.; Lauener, R.; et al. Maturation of the gut microbiome during the first year of life contributes to the protective farm effect on childhood asthma. Nat. Med. 2020, 26, 1766–1775. [Google Scholar] [CrossRef]
- Giles, E.M.; Couper, J. Microbiome in health and disease. J. Paediatr. Child. Health 2020, 56, 1735–1738. [Google Scholar] [CrossRef]
- Lynch, S.V.; Pedersen, O. The Human Intestinal Microbiome in Health and Disease. N. Engl. J. Med. 2016, 375, 2369–2379. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, Y.; Jackson, D.; Bacharier, L.B.; Mauger, D.; Boushey, H.; Castro, M.; Durack, J.; Huang, Y.; Lemanske, R.F., Jr.; Storch, G.A.; et al. The upper-airway microbiota and loss of asthma control among asthmatic children. Nat. Commun. 2019, 10, 5714. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Durack, J.; Christian, L.S.; Nariya, S.; Gonzalez, J.; Bhakta, N.R.; Ansel, K.M.; Beigelman, A.; Castro, M.; Dyer, A.M.; Israel, E.; et al. Distinct associations of sputum and oral microbiota with atopic, immunologic, and clinical features in mild asthma. J. Allergy Clin. Immunol. 2020, 146, 1016–1026. [Google Scholar] [CrossRef] [PubMed]
- Lai, P.S.; Kolde, R.; Franzosa, E.A.; Gaffin, J.M.; Baxi, S.N.; Sheehan, W.J.; Gold, D.R.; Gevers, D.; Xavier, R.J.; Phipatanakul, W. The classroom microbiome and asthma morbidity in children attending 3 inner-city schools. J. Allergy Clin. Immunol. 2018, 141, 2311–2313. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Phipatanakul, W.; Bailey, A.; Hoffman, E.B.; Sheehan, W.J.; Lane, J.P.; Baxi, S.; Rao, D.; Permaul, P.; Gaffin, J.M.; Rogers, C.A.; et al. The school inner-city asthma study: Design, methods, and lessons learned. J. Asthma 2011, 48, 1007–1014. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, A.; Hunt, E.; MacSharry, J.; Murphy, D.M. The Microbiome and the Pathophysiology of Asthma. Respir. Res. 2016, 17, 163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bosch, A.; Levin, E.; van Houten, M.A.; Hasrat, R.; Kalkman, G.; Biesbroek, G.; de Steenhuijsen Piters, W.A.A.; de Groot, P.C.M.; Pernet, P.; Keijser, B.J.F.; et al. Development of Upper Respiratory Tract Microbiota in Infancy is Affected by Mode of Delivery. EBioMedicine 2016, 9, 336–345. [Google Scholar] [CrossRef] [Green Version]
- Mohajeri, M.H.; Brummer, R.J.M.; Rastall, R.A.; Weersma, R.K.; Harmsen, H.J.M.; Faas, M.; Eggersdorfer, M. The role of the microbiome for human health: From basic science to clinical applications. Eur. J. Nutr. 2018, 57, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Kloepfer, K.M.; Lee, W.M.; Pappas, T.E.; Kang, T.J.; Vrtis, R.F.; Evans, M.D.; Gangnon, R.E.; Bochkov, Y.A.; Jackson, D.J.; Lemanske, R.F., Jr.; et al. Detection of pathogenic bacteria during rhinovirus infection is associated with increased respiratory symptoms and asthma exacerbations. J. Allergy Clin. Immunol. 2014, 133, 1301–1307. [Google Scholar] [CrossRef] [Green Version]
- Teo, S.M.; Mok, D.; Pham, K.; Kusel, M.; Serralha, M.; Troy, N.; Holt, B.J.; Hales, B.J.; Walker, M.L.; Hollams, E.; et al. The infant nasopharyngeal microbiome impacts severity of lower respiratory infection and risk of asthma development. Cell Host Microbe. 2015, 17, 704–715. [Google Scholar] [CrossRef] [Green Version]
- Mansbach, J.M.; Hasegawa, K.; Henke, D.M.; Ajami, N.J.; Petrosino, J.F.; Shaw, C.A.; Piedra, P.A.; Sullivan, A.F.; Espinola, J.A.; Camargo, C.A., Jr. Respiratory syncytial virus and rhinovirus severe bronchiolitis are associated with distinct nasopharyngeal microbiota. J. Allergy Clin. Immunol. 2016, 137, 1909–1913.e1904. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amat, F.; Plantard, C.; Mulliez, A.; Petit, I.; Rochette, E.; Verdan, M.; Henquell, C.; Labbe, G.; Heraud, M.C.; Evrard, B.; et al. RSV-hRV co-infection is a risk factor for recurrent bronchial obstruction and early sensitization 3 years after bronchiolitis. J. Med. Virol. 2018, 90, 867–872. [Google Scholar] [CrossRef] [PubMed]
- Rosas-Salazar, C.; Shilts, M.H.; Tovchigrechko, A.; Schobel, S.; Chappell, J.D.; Larkin, E.K.; Shankar, J.; Yooseph, S.; Nelson, K.E.; Halpin, R.A.; et al. Differences in the Nasopharyngeal Microbiome During Acute Respiratory Tract Infection with Human Rhinovirus and Respiratory Syncytial Virus in Infancy. J. Infect. Dis. 2016, 214, 1924–1928. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| AdV 2 AdV 3 AdV 6 AdV 7.1 AdV 8 | CV 229E CV HKU1 CV NL63 CV OC43 | MERS-CoV SARS-CoV2 | HMPV | HRV/HEV | Influenza A Influenza B | PIV 1 PIV 2 PIV 3 PIV 4 | RSV |
| B. p. B. pp. | C. pneumoniae | M. pneumoniae |
| Asthmatics | Wheezers | Healthy Controls | |
|---|---|---|---|
| Population (n) | 54 | 50 | 37 |
| Age (years) average (minimum-maximum) | 9.8 (5.29–17.27) | 2.1 (0.43–4.48) | 8.2 (1.39–16.30) |
| Female (%) | 33.3 | 32.0 | 45.9 |
| Positive atopic status (%) | 76.5 (n = 51) | 23.4 (n = 47) | 8.1 |
| Negative steroid status (%) | 57.1 (n = 49) | 73.5 (n = 49) | 0 |
| Breast feeding (%) | 76.7 (n = 43) | 72.9 (n = 48) | 91.2 (n = 34) |
| Maternal alcohol/tobacco abuse (%) | 20.5 (n = 44) | 22.9 (n = 48) | 5.9 (n = 34) |
| Pet owner (%) | 23.3 (n = 43) | 21.3 (n = 47) | 29.4 (n = 34) |
| Mold exposition (%) | 50.0 (n = 42) | 28.3 (n = 46) | 17.7 (n = 34) |
| Traffic exposition (%) | 39.5 (n = 43) | 34.0 (n = 47) | 14.7 (n = 34) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sallard, E.; Schult, F.; Baehren, C.; Buedding, E.; Mboma, O.; Ahmad-Nejad, P.; Ghebremedhin, B.; Ehrhardt, A.; Wirth, S.; Aydin, M. Viral Infection and Respiratory Exacerbation in Children: Results from a Local German Pediatric Exacerbation Cohort. Viruses 2022, 14, 491. https://doi.org/10.3390/v14030491
Sallard E, Schult F, Baehren C, Buedding E, Mboma O, Ahmad-Nejad P, Ghebremedhin B, Ehrhardt A, Wirth S, Aydin M. Viral Infection and Respiratory Exacerbation in Children: Results from a Local German Pediatric Exacerbation Cohort. Viruses. 2022; 14(3):491. https://doi.org/10.3390/v14030491
Chicago/Turabian StyleSallard, Erwan, Frank Schult, Carolin Baehren, Eleni Buedding, Olivier Mboma, Parviz Ahmad-Nejad, Beniam Ghebremedhin, Anja Ehrhardt, Stefan Wirth, and Malik Aydin. 2022. "Viral Infection and Respiratory Exacerbation in Children: Results from a Local German Pediatric Exacerbation Cohort" Viruses 14, no. 3: 491. https://doi.org/10.3390/v14030491
APA StyleSallard, E., Schult, F., Baehren, C., Buedding, E., Mboma, O., Ahmad-Nejad, P., Ghebremedhin, B., Ehrhardt, A., Wirth, S., & Aydin, M. (2022). Viral Infection and Respiratory Exacerbation in Children: Results from a Local German Pediatric Exacerbation Cohort. Viruses, 14(3), 491. https://doi.org/10.3390/v14030491