
Clinical and Immunological Predictors of Hemorrhagic Fever with Renal Syndrome Outcome during the Early Phase

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Patients and Methods
2.1. Ethics Statement
2.2. Clinical Classification of Patients with HFRS
2.3. Quantitative Polymerase Chain Reaction (qPCR) and Reverse Transcription (RT)-PCR
2.4. Luminex Assay
2.5. ELISA
2.6. Cell-Free DNA (cfDNA) Extraction and Quantification
2.7. Statistical Analysis
3. Results
3.1. Patient Characteristics and Clinical Findings
3.2. Laboratory Diagnosis of HTNV-Infected HFRS Patients
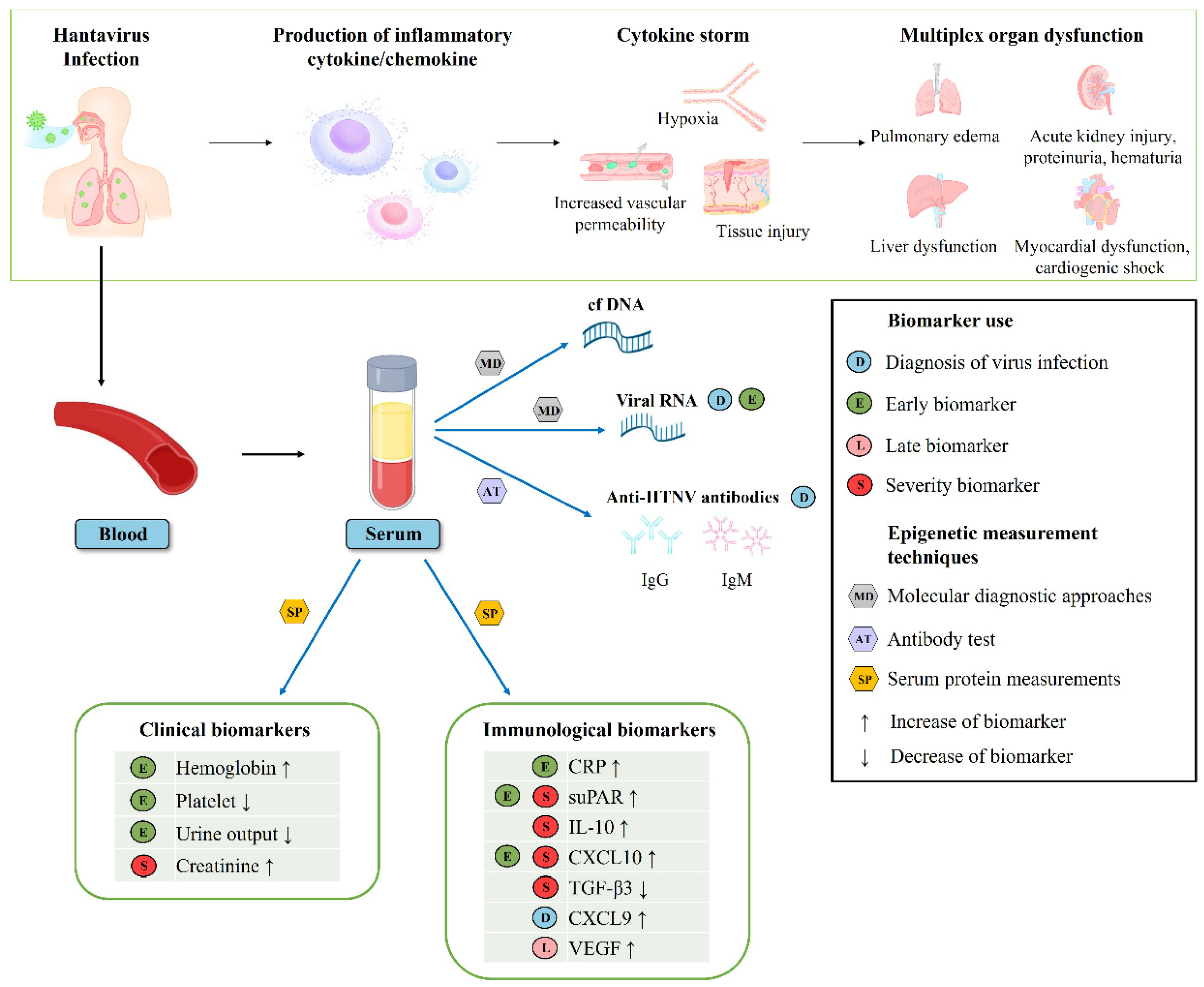
3.3. Clinical and Immunological Biomarkers Associated with Early and Late Phases of HFRS
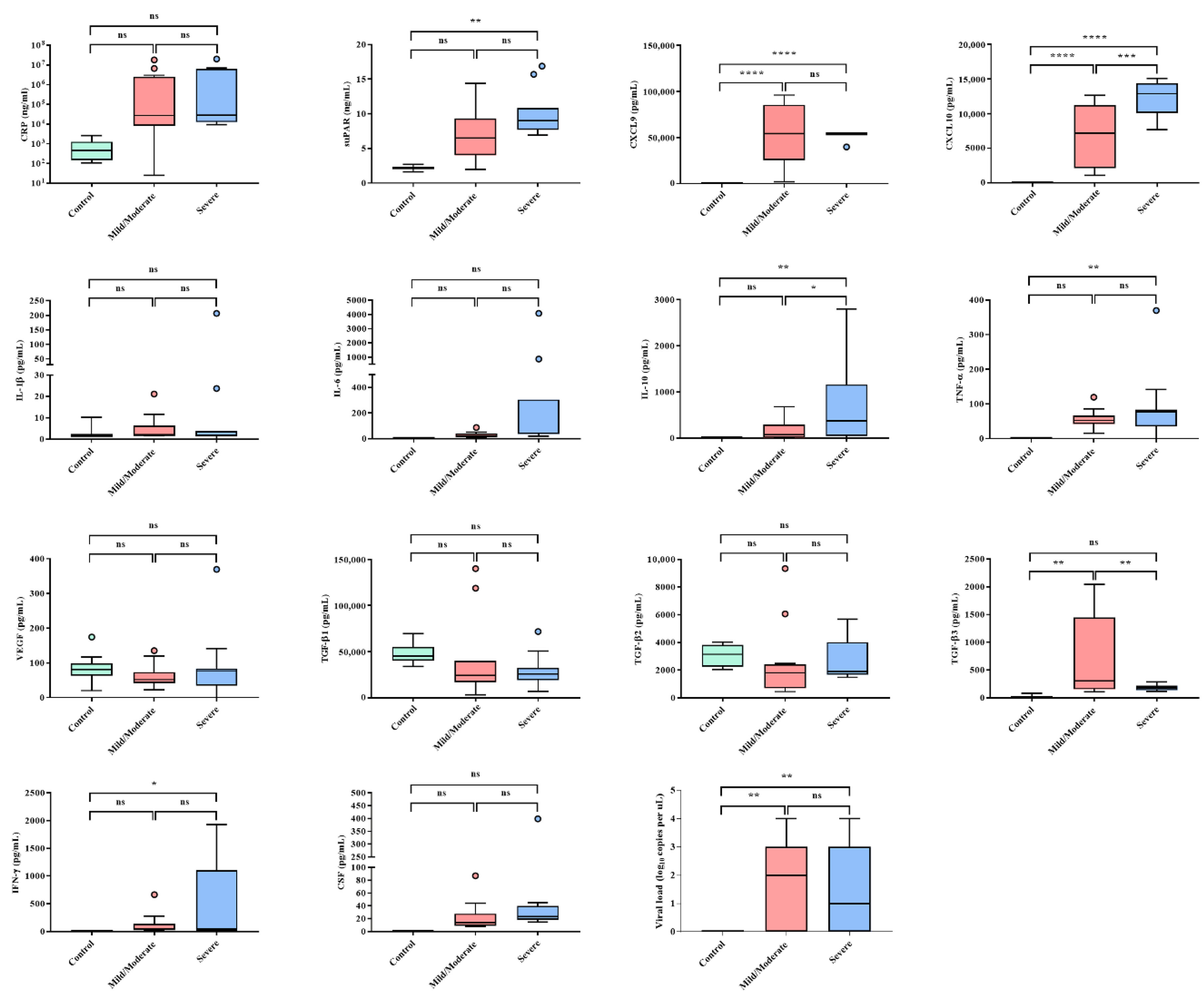
3.4. Clinical and Immunological Biomarkers Associated with HFRS Severity
3.5. Quantitative Analysis of Cell-Free DNA (cfDNA) for Patients with HFRS
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jonsson, C.B.; Figueiredo, L.T.; Vapalahti, O. A global perspective on hantavirus ecology, epidemiology, and disease. Clin. Microbiol. Rev. 2010, 23, 412–441. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Avšič-Županc, T.; Saksida, A.; Korva, M. Hantavirus infections. Clin. Microbiol. Infec. 2019, 21, e6–e16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, H.W.; Baek, L.J.; Johnson, K.M. Isolation of Hantaan Virus, the Etiologic Agent of Korean Hemorrhagic-Fever, from Wild Urban Rats. J. Infect. Dis. 1982, 146, 638–644. [Google Scholar] [CrossRef] [PubMed]
- Brummerkorvenkontio, M.; Vaheri, A.; Hovi, T.; Vonbonsdorff, C.H.; Vuorimies, J.; Manni, T.; Penttinen, K.; Okerblom, N.; Lahdevirta, J. Nephropathia Epidemica: Detection of Antigen in Bank Voles and Serologic Diagnosis of Human Infection. J. Infect. Dis. 1980, 141, 131–134. [Google Scholar] [CrossRef]
- Heyman, P.; Vaheri, A.; Lundkvist, A.; Avsic-Zupanc, T. Hantavirus infections in Europe: From virus carriers to a major public-health problem. Expert Rev. Anti-Infect. Ther. 2009, 7, 205–217. [Google Scholar] [CrossRef]
- Jiang, H.; Du, H.; Wang, L.M.; Wang, P.Z.; Bai, X.F. Corrigendum: Hemorrhagic fever with renal syndrome: Pathogenesis and clinical picture. Front. Cell. Infect. Microbiol. 2016, 6, 178. [Google Scholar] [CrossRef]
- Korva, M.; Rus, K.R.; Pavletic, M.; Saksida, A.; Knap, N.; Jelovsek, M.; Smrdel, K.S.; Jakupi, X.; Humolli, I.; Dedushaj, J.; et al. Characterization of Biomarker Levels in Crimean-Congo Hemorrhagic Fever and Hantavirus Fever with Renal Syndrome. Viruses 2019, 11, 686. [Google Scholar] [CrossRef] [Green Version]
- Isman, F.K.; Zulfikaroglu, B.; Isbilen, B.; Ozalp, N.; Ozmen, M.M.; Bilgic, I.; Koc, M. Copeptin is a predictive biomarker of severity in acute pancreatitis. Am. J. Emerg. Med. 2013, 31, 690–692. [Google Scholar] [CrossRef]
- Donadello, K.; Scolletta, S.; Covajes, C.; Vincent, J.L. suPAR as a prognostic biomarker in sepsis. BMC Med. 2012, 10, 2. [Google Scholar] [CrossRef] [Green Version]
- Baigildina, A.A.; Khaiboullina, S.F.; Martynova, E.V.; Anokhin, V.A.; Lombardi, V.C.; Rizvanov, A.A. Inflammatory cytokines kinetics define the severity and phase of nephropathia epidemica. Biomark. Med. 2015, 9, 99–107. [Google Scholar] [CrossRef]
- Zhang, Y.S.; Liu, B.; Ma, Y.; Yi, J.; Zhang, C.M.; Zhang, Y.; Xu, Z.W.; Wang, J.P.; Yang, K.; Yang, A.G.; et al. Hantaan Virus Infection Induces CXCL10 Expression through TLR3, RIG-I, and MDA-5 Pathways Correlated with the Disease Severity. Mediat. Inflamm. 2014, 2014, 697837. [Google Scholar] [CrossRef] [PubMed]
- Kerget, B.; Kerget, F.; Aksakal, A.; Askin, S.; Ucar, E.Y.; Saglam, L. Evaluation of the relationship between KIM-1 and suPAR levels and clinical severity in COVID-19 patients: A different perspective on suPAR. J. Med. Virol. 2021, 93, 5568–5573. [Google Scholar] [CrossRef] [PubMed]
- Cetinkaya, E.; Senol, K.; Saylam, B.; Tez, M. Red cell distribution width to platelet ratio: New and promising prognostic marker in acute pancreatitis. World J. Gastroenterol. 2014, 20, 14450–14454. [Google Scholar] [CrossRef] [PubMed]
- Mueller, A.A.; Tamura, T.; Crowley, C.P.; DeGrado, J.R.; Haider, H.; Jezmir, J.L.; Keras, G.; Penn, E.H.; Massaro, A.F.; Kim, E.Y. Inflammatory Biomarker Trends Predict Respiratory Decline in COVID-19 Patients. Cell Rep. Med. 2020, 1, 100144. [Google Scholar] [CrossRef]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.-D.; Coopersmith, C.M.J.J. The third international consensus definitions for sepsis and septic shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef]
- Lee, J.C.; Ahn, Y.O.; Kim, D.W.; Heo, D.S. Elevated TGF-b1 secretion and downmodulation of NKG2D underlies impaired NK cytotoxicity in cancer patients. J. Immunother. 2004, 27, S50. [Google Scholar] [CrossRef]
- Wojciechowska-Lacka, A.; Matecka-Nowak, M.; Adamiak, E.; Lacki, J.; Cerkaska-Gluszak, B.J.N. Serum levels of interleukin-10 and interleukin-6 in patients with lung cancer. Neoplasma 1996, 43, 155–158. [Google Scholar]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.J.T.l. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Gong, J.; Dong, H.; Xia, Q.-S.; Huang, Z.-Y.; Wang, D.-K.; Zhao, Y.; Liu, W.-H.; Tu, S.-H.; Zhang, M.-M.; Wang, Q. Correlation analysis between disease severity and inflammation-related parameters in patients with COVID-19: A retrospective study. BMC Infect. Dis. 2020, 20, 1–7. [Google Scholar] [CrossRef]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Denecke, B.; Bigalke, B.; Haap, M.; Overkamp, D.; Lehnert, H.; Haas, C.S. Hantavirus infection: A neglected diagnosis in thrombocytopenia and fever? Mayo Clin. Proc. 2010, 85, 1016–1020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Balmaseda, A.; Hammond, S.N.; Pérez, M.A.; Cuadra, R.; Solano, S.; Rocha, J.; Idiaquez, W.; Harris, E. Assessment of the World Health Organization scheme for classification of dengue severity in Nicaragua. Am. J. Trop. Med. Hyg. 2005, 73, 1059–1062. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hammond, S.N.; Balmaseda, A.; Perez, L.; Tellez, Y.; Saborío, S.I.; Mercado, J.C.; Videa, E.; Rodriguez, Y.; Perez, M.A.; Cuadra, R. Differences in dengue severity in infants, children, and adults in a 3-year hospital-based study in Nicaragua. Am. J. Trop. Med. Hyg. 2005, 73, 1063–1070. [Google Scholar] [CrossRef] [PubMed]
- Tanner, L.; Schreiber, M.; Low, J.G.; Ong, A.; Tolfvenstam, T.; Lai, Y.L.; Ng, L.C.; Leo, Y.S.; Thi Puong, L.; Vasudevan, S.G. Decision tree algorithms predict the diagnosis and outcome of dengue fever in the early phase of illness. PLoS Negl. Trop. Dis. 2008, 2, e196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Du, H.; Li, J.; Yu, H.-T.; Jiang, W.; Zhang, Y.; Wang, J.-N.; Wang, P.-Z.; Bai, X.-F.J.C.C.; Medicine, L. Early indicators of severity and construction of a risk model for prognosis based upon laboratory parameters in patients with hemorrhagic fever with renal syndrome. Clin. Chem. Lab. Med. 2014, 52, 1667–1675. [Google Scholar] [CrossRef]
- Vapalahti, O.; Mustonen, J.; Lundkvist, Å.; Henttonen, H.; Plyusnin, A.; Vaheri, A. Hantavirus infections in Europe. Lancet Infect. Dis. 2003, 3, 653–661. [Google Scholar] [CrossRef]
- Kim, Y.O.; Yoon, S.A.; Ku, Y.M.; Yang, C.W.; Kim, Y.S.; Kim, S.Y.; Choi, E.J.; Chang, Y.S.; Bang, B.K.J.J.o.K.m.s. Serum albumin level correlates with disease severity in patients with hemorrhagic fever with renal syndrome. J. Korean Med. Sci. 2003, 18, 696–700. [Google Scholar] [CrossRef] [Green Version]
- Wang, P.; Li, Z.; Yu, H.; Zhang, Y.; Wang, W.; Jiang, W.; Bai, X. Elevated serum concentrations of inflammatory cytokines and chemokines in patients with haemorrhagic fever with renal syndrome. J. Int. Med. Res. 2012, 40, 648–656. [Google Scholar] [CrossRef] [Green Version]
- Li, M.; Ji, Y.; Dong, Y.; Zhou, Y.; Ren, H.; Xie, M. The detection of vascular endothelial growth factor in serum of patients with hemorrhagic fever with renal syndrome. Inflammation 2013, 36, 962–967. [Google Scholar] [CrossRef]
- Outinen, T.K.; Tervo, L.; Mäkelä, S.; Huttunen, R.; Mäenpää, N.; Huhtala, H.; Vaheri, A.; Mustonen, J.; Aittoniemi, J. Plasma levels of soluble urokinase-type plasminogen activator receptor associate with the clinical severity of acute Puumala hantavirus infection. PLoS ONE 2013, 8, e71335. [Google Scholar] [CrossRef] [Green Version]
- No, J.S.; Kim, W.K.; Kim, J.A.; Lee, S.H.; Lee, S.Y.; Kim, J.H.; Kho, J.H.; Lee, D.; Song, D.H.; Gu, S.H.; et al. Detection of Hantaan virus RNA from anti-Hantaan virus IgG seronegative rodents in an area of high endemicity in Republic of Korea. Microbiol. Immunol. 2016, 60, 268–271. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, G.Y.; Kim, W.K.; Park, K.; Lee, S.H.; Hwang, J.; No, J.S.; Cho, S.; Lee, D.; Song, D.H.; Gu, S.H.; et al. Phylogeographic diversity and hybrid zone of Hantaan orthohantavirus collected in Gangwon Province, Republic of Korea. PLoS Negl. Trop. Dis. 2020, 14, e0008714. [Google Scholar] [CrossRef] [PubMed]
- Alge, J.L.; Arthur, J.M. Biomarkers of AKI: A review of mechanistic relevance and potential therapeutic implications. Clin. J. Am. Soc. Nephrol. 2015, 10, 147–155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jin, K.; Murugan, R.; Sileanu, F.E.; Foldes, E.; Priyanka, P.; Clermont, G.; Kellum, J.A. Intensive Monitoring of Urine Output Is Associated With Increased Detection of Acute Kidney Injury and Improved Outcomes. Chest 2017, 152, 972–979. [Google Scholar] [CrossRef] [Green Version]
- Kellum, J.A.; Sileanu, F.E.; Murugan, R.; Lucko, N.; Shaw, A.D.; Clermont, G. Classifying AKI by Urine Output versus Serum Creatinine Level. J. Am. Soc. Nephrol. 2015, 26, 2231–2238. [Google Scholar] [CrossRef]
- Aghamohammadi, A.; Zafari, M.; Tofighi, M.J.C.j.o.i.m. High maternal hemoglobin concentration in first trimester as risk factor for pregnancy induced hypertension. Casp. J. Intern. Med. 2011, 2, 194. [Google Scholar]
- Koller, O.; Sandvei, R.; Sagen, N. High hemoglobin levels during pregnancy and fetal risk. Int. J. Gynaecol. Obs. 1980, 18, 53–56. [Google Scholar] [CrossRef]
- Sarrel, P.; Lindsay, D.; Poole-Wilson, P.; Collins, P.J.T.L. Hypothesis: Inhibition of endothelium-derived relaxing factor by haemoglobin in the pathogenesis of pre-eclampsia. Lancet 1990, 336, 1030–1032. [Google Scholar] [CrossRef]
- Yu, C.; Xu, C.; Xu, L.; Yu, J.; Miao, M.; Li, Y. Serum proteomic analysis revealed diagnostic value of hemoglobin for nonalcoholic fatty liver disease. J. Hepatol. 2012, 56, 241–247. [Google Scholar] [CrossRef]
- Buttari, B.; Profumo, E.; Petrone, L.; Pietraforte, D.; Siracusano, A.; Margutti, P.; Delunardo, F.; Ortona, E.; Minetti, M.; Salvati, B. Free hemoglobin: A dangerous signal for the immune system in patients with carotid atherosclerosis? Ann. N. Y. Acad. Sci. 2007, 1107, 42–50. [Google Scholar] [CrossRef]
- Cosgriff, T.M. Mechanisms of disease in Hantavirus infection: Pathophysiology of hemorrhagic fever with renal syndrome. Rev. Infect. Dis. 1991, 13, 97–107. [Google Scholar] [CrossRef] [PubMed]
- Reynolds, S.; Galanis, E.; Krajden, M.; Morshed, M.; Bowering, D.; Abelson, W.; Kollmann, T.R. Imported fatal hantavirus pulmonary syndrome. Emerg. Infect. Dis. 2007, 13, 1424–1425. [Google Scholar] [CrossRef] [PubMed]
- Thunø, M.; Macho, B.; Eugen-Olsen, J. suPAR: The molecular crystal ball. Dis. Markers 2009, 27, 157–172. [Google Scholar] [CrossRef] [PubMed]
- Yilmaz, G.; Mentese, A.; Kaya, S.; Uzun, A.; Karahan, S.C.; Koksal, I. The diagnostic and prognostic significance of soluble urokinase plasminogen activator receptor in Crimean-Congo hemorrhagic fever. J. Clin. Virol. 2011, 50, 209–211. [Google Scholar] [CrossRef] [PubMed]
- Green, S.; Vaughn, D.W.; Kalayanarooj, S.; Nimmannitya, S.; Suntayakorn, S.; Nisalak, A.; Rothman, A.L.; Ennis, F.A. Elevated plasma interleukin-10 levels in acute dengue correlate with disease severity. J. Med. Virol. 1999, 59, 329–334. [Google Scholar] [CrossRef]
- Marta, R.; Montero, V.; Hack, C.; Sturk, A.; Maiztegui, J.; Molinas, F. Proinflammatory cytokines and elastase-alpha-1-antitrypsin in Argentine hemorrhagic fever. Am. J. Trop. Med. Hyg. 1999, 60, 85–89. [Google Scholar] [CrossRef] [Green Version]
- Laing, A.G.; Lorenc, A.; del Barrio, I.D.; Das, A.; Fish, M.; Monin, L.; Munoz-Ruiz, M.; McKenzie, D.R.; Hayday, T.S.; Francos-Quijorna, I.; et al. A dynamic COVID-19 immune signature includes associations with poor prognosis. Nat. Med. 2020, 26, 1623–1635. [Google Scholar] [CrossRef]
- Saksida, A.; Wraber, B.; Avšič-Županc, T. Serum levels of inflammatory and regulatory cytokines in patients with hemorrhagic fever with renal syndrome. BMC Infect. Dis. 2011, 11, 142. [Google Scholar] [CrossRef] [Green Version]
- Linderholm, M.; Ahlm, C.; Settergren, B.; Waage, A.; Tärnvik, A. Elevated plasma levels of tumor necrosis factor (TNF)-α, soluble TNF receptors, interleukin (IL)-6, and IL-IO in patients with hemorrhagic fever with renal syndrome. J. Infect. Dis. 1996, 173, 38–43. [Google Scholar] [CrossRef]
- Campbell, D.J.; Kim, C.H.; Butcher, E.C. Chemokines in the systemic organization of immunity. Immunol. Rev. 2003, 195, 58–71. [Google Scholar] [CrossRef]
- Hsieh, M.F.; Lai, S.L.; Chen, J.P.; Sung, J.M.; Lin, Y.L.; Wu-Hsieh, B.A.; Gerard, C.; Luster, A.; Liao, F. Both CXCR3 and CXCL10/IFN-inducible protein 10 are required for resistance to primary infection by dengue virus. J. Immunol. 2006, 177, 1855–1863. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khaiboullina, S.F.; Levis, S.; Morzunov, S.P.; Martynova, E.V.; Anokhin, V.A.; Gusev, O.A.; St Jeor, S.C.; Lombardi, V.C.; Rizvanov, A.A. Serum cytokine profiles differentiating hemorrhagic fever with renal syndrome and hantavirus pulmonary syndrome. Front. Immunol. 2017, 8, 567. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, J.Y.; Liang, W.W.; Chen, S.Y.; Zhu, Y.; Chen, H.M.; Mok, C.K.P.; Zhou, Y.C. Serum Cytokine Profiles in Patients with Dengue Fever at the Acute Infection Phase. Dis. Markers 2018, 2018, 8403937. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dalrymple, N.A.; Mackow, E.R. Endothelial Cells Elicit Immune-Enhancing Responses to Dengue Virus Infection. J. Virol. 2012, 86, 6408–6415. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wrzesinski, S.H.; Wan, Y.S.Y.; Flavell, R.A. Transforming growth factor-beta and the immune response: Implications for anticancer therapy. Clin. Cancer Res. 2007, 13, 5262–5270. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dong, M.; Blobe, G.C.J.B. Role of transforming growth factor-β in hematologic malignancies. Blood 2006, 107, 4589–4596. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sadeghi, M.; Lahdou, I.; Ettinger, J.; Navid, M.H.; Daniel, V.; Zeier, M.; Hofmann, J.; Opelz, G.; Schnitzler, P. Association of low serum TGF-β level in hantavirus infected patients with severe disease. BMC Immunol. 2015, 16, 19. [Google Scholar] [CrossRef] [Green Version]
- Sadeghi, M.; Eckerle, I.; Daniel, V.; Burkhardt, U.; Opelz, G.; Schnitzler, P. Cytokine expression during early and late phase of acute Puumala hantavirus infection. BMC Immunol. 2011, 12, 65. [Google Scholar] [CrossRef] [Green Version]
- Yi, J.; Zhang, Y.; Zhang, Y.; Ma, Y.; Zhang, C.; Li, Q.; Liu, B.; Liu, Z.; Liu, J.; Zhang, X. Increased plasma cell-free DNA level during HTNV infection: Correlation with disease severity and virus load. Viruses 2014, 6, 2723–2734. [Google Scholar] [CrossRef] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| n (%) | |
|---|---|
| Symptoms | |
| Fever | 25/26 (96) |
| Nausea | 8/26 (31) |
| Headache | 5/26 (19) |
| Diarrhea | 3/26 (12) |
| Myalgia | 1/26 (4) |
| Flank pain | 1/26 (4) |
| Chest pain | 1/26 (4) |
| Sore throat | 1/26 (4) |
| Dizziness | 1/26 (4) |
| Dyspnea | 1/26 (4) |
| Weakness | 1/26 (4) |
| Comorbidities | |
| Acute kidney injury | 25/26 (96) |
| Pulmonary edema | 9/26 (35) |
| Hypotension | 8/26 (31) |
| Treatments and outcomes | |
| ICU admission | 20/26 (77) |
| Transfusion | 3/26 (12) |
| Mechanical ventilation | 1/26 (4) |
| Hemodialysis | 1/26 (4) |
| Mortality | 1/26 (4) |
| Mild (n = 1 a) | Moderate (n = 14) | Severe (n = 11) | |
|---|---|---|---|
| Demographics | |||
| Age, years a | 23 | 21–23 | 21–23 |
| Hospital stay, days a | 5 | 9–11 | 11–15 |
| Actual treatment, days a | 4 | 10–12 | 13–17 |
| ICU treatment, days a | 2 | 2–4 | 3–5 |
| Laboratory tests | |||
| Anti-HTNV IgM positivity | 0 | 4 (29%) | 1 (9%) |
| Anti-HTNV IgG positivity, titers b | 0 | 12 (86%), 1:3904 ± 1598 | 9 (82%), 1:1844 ± 1458 |
| HTNV RT-PCR positivity | 0 | 11 (79%) | 10 (91%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, G.-Y.; Kim, W.-K.; No, J.S.; Yi, Y.; Park, H.C.; Jung, J.; Cho, S.; Lee, J.; Lee, S.-H.; Park, K.; et al. Clinical and Immunological Predictors of Hemorrhagic Fever with Renal Syndrome Outcome during the Early Phase. Viruses 2022, 14, 595. https://doi.org/10.3390/v14030595
Lee G-Y, Kim W-K, No JS, Yi Y, Park HC, Jung J, Cho S, Lee J, Lee S-H, Park K, et al. Clinical and Immunological Predictors of Hemorrhagic Fever with Renal Syndrome Outcome during the Early Phase. Viruses. 2022; 14(3):595. https://doi.org/10.3390/v14030595
Chicago/Turabian StyleLee, Geum-Young, Won-Keun Kim, Jin Sun No, Yongjin Yi, Hayne Cho Park, Jaehun Jung, Seungchan Cho, Jingyeong Lee, Seung-Ho Lee, Kyungmin Park, and et al. 2022. "Clinical and Immunological Predictors of Hemorrhagic Fever with Renal Syndrome Outcome during the Early Phase" Viruses 14, no. 3: 595. https://doi.org/10.3390/v14030595
APA StyleLee, G. -Y., Kim, W. -K., No, J. S., Yi, Y., Park, H. C., Jung, J., Cho, S., Lee, J., Lee, S. -H., Park, K., Kim, J., & Song, J. -W. (2022). Clinical and Immunological Predictors of Hemorrhagic Fever with Renal Syndrome Outcome during the Early Phase. Viruses, 14(3), 595. https://doi.org/10.3390/v14030595