
Risk Factors for Norovirus Infections and Their Association with Childhood Growth: Findings from a Multi-Country Birth Cohort Study

 , , , ,
, , , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
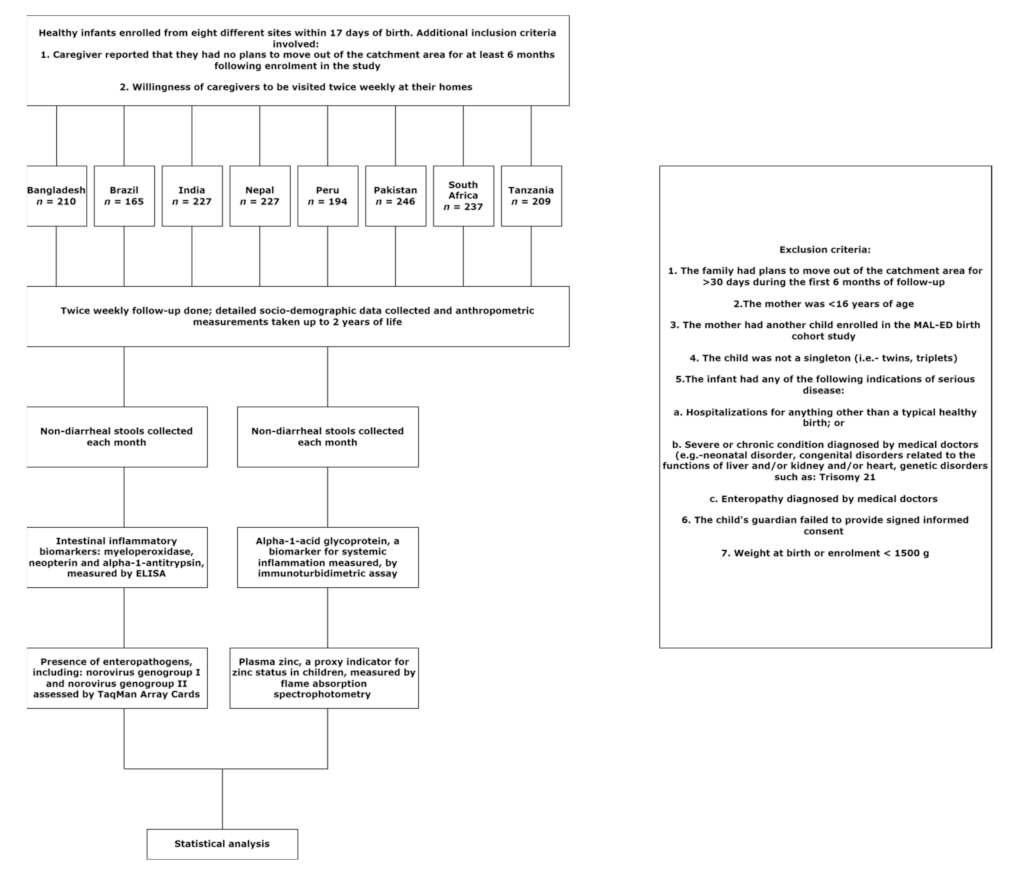
2.1. Study Settings and Ethical Statement
2.2. Collection of Anthropometric, Socio-Demographic and Morbidity Data
2.3. Collection of Biological Specimens and Biochemical Analyses
2.4. Detection of Enteropathogens
2.5. Statistical Analysis
3. Results
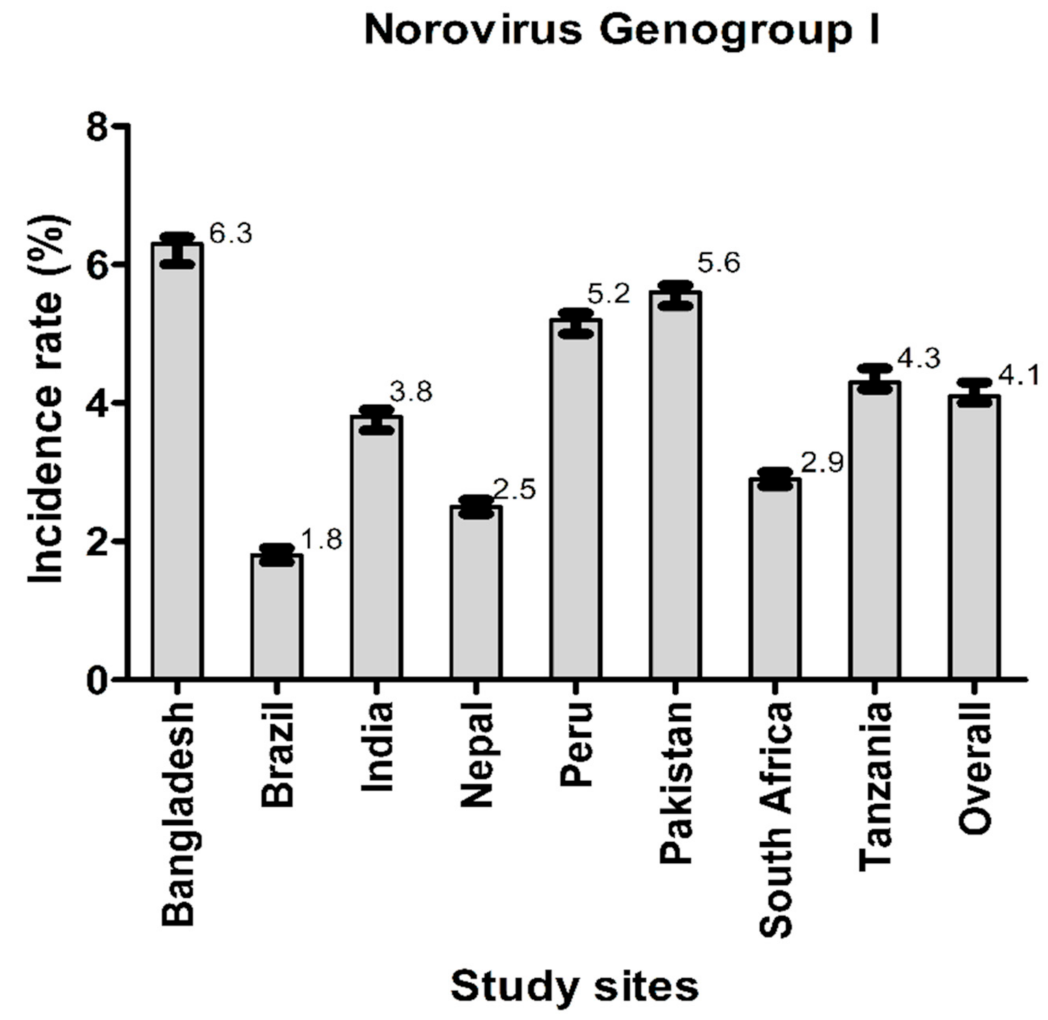
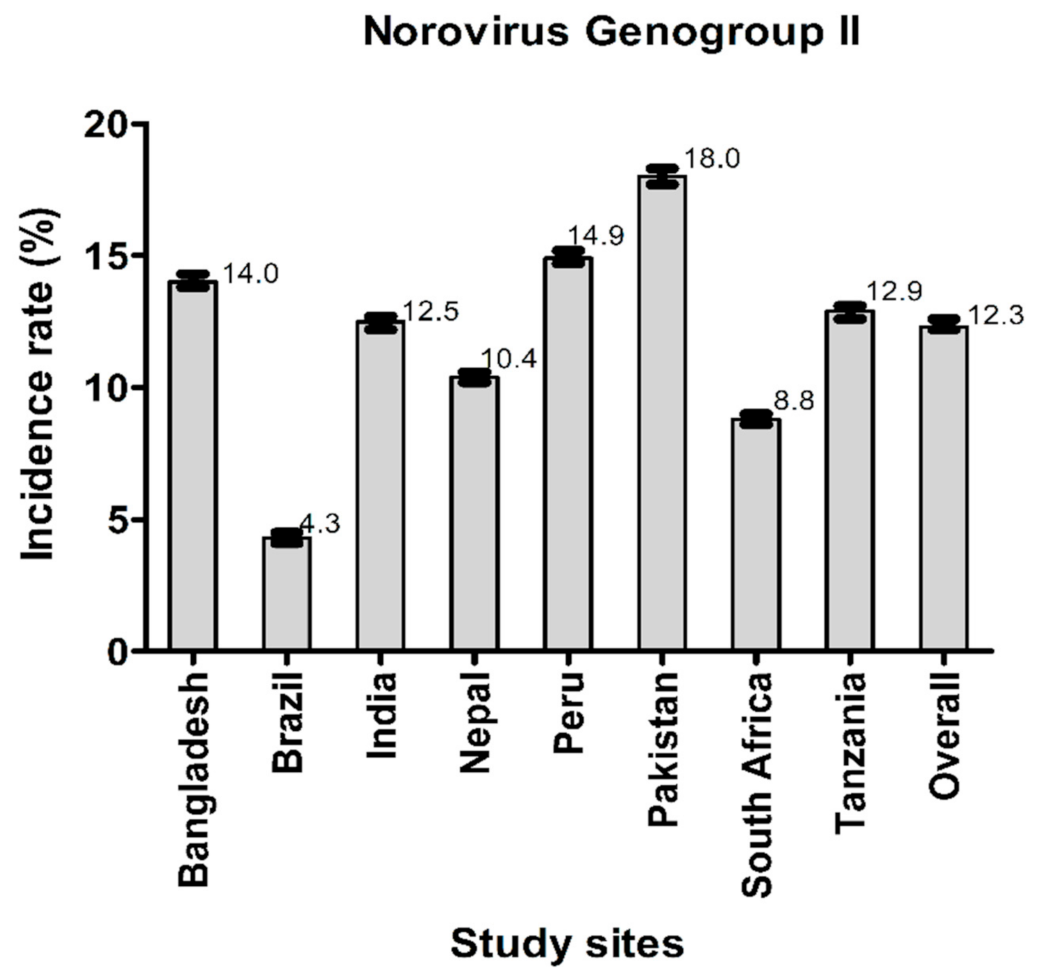
3.1. General Characteristics of the Study Participants and Incidence Rate of Norovirus GI and Norovirus GII
3.2. Factors Associated with Infections by Norovirus GI and Norovirus GII
3.3. Association of Infections by Norovirus GI and Norovirus GII with Linear and Ponderal Growth
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Olofin, I.; McDonald, C.M.; Ezzati, M.; Flaxman, S.; Black, R.E.; Fawzi, W.W.; Caulfield, L.E.; Danaei, G.; for the Nutrition Impact Model Study (Anthropometry Cohort Pooling). Associations of Suboptimal Growth with All-Cause and Cause-Specific Mortality in Children under Five Years: A Pooled Analysis of Ten Prospective Studies. PLoS ONE 2013, 8, e64636. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Black, R.E.; Victora, C.G.; Walker, S.P.; Bhutta, Z.A.; Christian, P.; de Onis, M.; Ezzati, M.; Grantham-McGregor, S.; Katz, J.; Martorell, R.; et al. Maternal and child undernutrition and overweight in low-income and middle-income countries. Lancet 2013, 382, 427–451. [Google Scholar] [CrossRef]
- World Health Organization. WHO Child Growth Standards: Length/Height-for-Age, Weight-for-Age, Weight-for-Length, Weight-for-Height and Body Mass Index-for-Age: Methods and Development; World Health Organization: Geneva, Switzerland, 2006. [Google Scholar]
- Ssentongo, P.; Ssentongo, A.E.; Ba, D.M.; Ericson, J.E.; Na, M.; Gao, X.; Fronterre, C.; Chinchilli, V.M.; Schiff, S.J. Global, regional and national epidemiology and prevalence of child stunting, wasting and underweight in low- and middle-income countries, 2006–2018. Sci. Rep. 2021, 11, 5204. [Google Scholar] [CrossRef] [PubMed]
- Richard, S.A.; Black, R.E.; Gilman, R.H.; Guerrant, R.L.; Kang, G.; Lanata, C.F.; Mølbak, K.; Rasmussen, Z.A.; Sack, R.B.; Valentiner-Branth, P.; et al. Diarrhea in Early Childhood: Short-term Association With Weight and Long-term Association with Length. Am. J. Epidemiol. 2013, 178, 1129–1138. [Google Scholar] [CrossRef] [PubMed]
- Checkley, W.; Epstein, L.D.; Gilman, R.H.; Cabrera, L.; Black, R.E. Effects of acute diarrhea on linear growth in Peruvian children. Am. J. Epidemiol. 2003, 157, 166–175. [Google Scholar] [CrossRef] [Green Version]
- Lee, G.; Olortegui, M.P.; Yori, P.P.; Black, R.E.; Caulfield, L.; Chavez, C.B.; Hall, E.; Pan, W.K.; Meza, R.; Kosek, M. Effects of Shigella-, Campylobacter-and ETEC-associated diarrhea on childhood growth. Pediatric Infect. Dis. J. 2014, 33, 1004–1009. [Google Scholar] [CrossRef] [Green Version]
- Platts-Mills, J.A.; Babji, S.; Bodhidatta, L.; Gratz, J.; Haque, R.; Havt, A.; McCormick, B.J.; McGrath, M.; Olortegui, M.P.; Samie, A.; et al. Pathogen-specific burdens of community diarrhoea in developing countries: A multisite birth cohort study (MAL-ED). Lancet Glob. Health 2015, 3, e564–e575. [Google Scholar] [CrossRef] [Green Version]
- Liu, L.; Oza, S.; Hogan, D.; Perin, J.; Rudan, I.; Lawn, J.E.; Cousens, S.; Mathers, C.; Black, R.E. Global, regional, and national causes of child mortality in 2000–13, with projections to inform post-2015 priorities: An updated systematic analysis. Lancet 2015, 385, 430–440. [Google Scholar] [CrossRef]
- Chhabra, P.; De Graaf, M.; Parra, G.I.; Chan, M.C.-W.; Green, K.; Martella, V.; Wang, Q.; White, P.A.; Katayama, K.; Vennema, H.; et al. Updated classification of norovirus genogroups and genotypes. J. Gen. Virol. 2019, 100, 1393. [Google Scholar] [CrossRef]
- Glass, R.I.; Parashar, U.D.; Estes, M.K. Norovirus gastroenteritis. N. Engl. J. Med. 2009, 361, 1776–1785. [Google Scholar] [CrossRef] [Green Version]
- Gondim, R.D.; Pankov, R.C.; Prata, M.M.; Medeiros, P.H.; Veras, H.N.; Santos, A.K.; Magalhães, L.M.; Havt, A.; Fumian, T.M.; Miagostovich, M.P.; et al. Genetic Diversity of Norovirus Infections, Coinfections, and Undernutrition in Children From Brazilian Semiarid Region. J. Pediatr. Gastroenterol. Nutr. 2018, 67, e117–e122. [Google Scholar] [CrossRef] [PubMed]
- Karst, S.M. Pathogenesis of Noroviruses, Emerging RNA Viruses. Viruses 2010, 2, 748–781. [Google Scholar] [CrossRef] [PubMed]
- Rogawski, E.T.; Liu, J.; Platts-Mills, J.A.; Kabir, F.; Lertsethtakarn, P.; Siguas, M.; Khan, S.S.; Praharaj, I.; Murei, A.; Nshama, R.; et al. Use of quantitative molecular diagnostic methods to investigate the effect of enteropathogen infections on linear growth in children in low-resource settings: Longitudinal analysis of results from the MAL-ED cohort study. Lancet Glob. Health 2018, 6, e1319–e1328. [Google Scholar] [CrossRef] [Green Version]
- The MAL-ED Network Investigators. The MAL-ED study: A multinational and multidisciplinary approach to understand the relationship between enteric pathogens, malnutrition, gut physiology, physical growth, cognitive development, and immune responses in infants and children up to 2 years of age in resource-poor environments. Clin. Infect. Dis. 2014, 59 (Suppl. 4), S193–S206. [Google Scholar]
- De Onis, M.; Onyango, A.W.; Borghi, E.; Siyam, A.; Nishida, C.; Siekmann, J. Development of a WHO growth reference for school-aged children and adolescents. Bull. World Health Organ. 2007, 85, 660–667. [Google Scholar] [CrossRef]
- Kosek, M.; Haque, R.; Lima, A.; Babji, S.; Shrestha, S.; Qureshi, S.; Amidou, S.; Mduma, E.; Lee, G.; Yori, P.P.; et al. Fecal Markers of Intestinal Inflammation and Permeability Associated with the Subsequent Acquisition of Linear Growth Deficits in Infants. Am. J. Trop. Med. Hyg. 2013, 88, 390–396. [Google Scholar] [CrossRef] [Green Version]
- Liu, J.; Kabir, F.; Manneh, J.; Lertsethtakarn, P.; Begum, S.; Gratz, J.; Becker, S.M.; Operario, D.J.; Taniuchi, M.; Janaki, L.; et al. Development and assessment of molecular diagnostic tests for 15 enteropathogens causing childhood diarrhoea: A multicentre study. Lancet Infect. Dis. 2014, 14, 716–724. [Google Scholar] [CrossRef]
- Houpt, E.; Gratz, J.; Kosek, M.; Zaidi, A.K.M.; Qureshi, S.; Kang, G.; Babji, S.; Mason, C.; Bodhidatta, L.; Samie, A.; et al. Microbiologic Methods Utilized in the MAL-ED Cohort Study. Clin. Infect. Dis. 2014, 59 (Suppl. 4), S225–S232. [Google Scholar] [CrossRef] [Green Version]
- Sanchez, J.J.; Alam, A.; Stride, C.B.; Haque, A.; Das, S.; Mahfuz, M.; Roth, D.E.; Sly, P.D.; Long, K.Z.; Ahmed, T. Campylobacter infection and household factors are associated with childhood growth in urban Bangladesh: An analysis of the MAL-ED study. PLoS Neglected Trop. Dis. 2020, 14, e0008328. [Google Scholar] [CrossRef]
- Haque, M.A.; Platts-Mills, J.A.; Mduma, E.; Bodhidatta, L.; Bessong, P.; Shakoor, S.; Kang, G.; Kosek, M.N.; Lima, A.A.; Shrestha, S.K.; et al. Determinants of Campylobacter infection and association with growth and enteric inflammation in children under 2 years of age in low-resource settings. Sci. Rep. 2019, 9, 17124. [Google Scholar] [CrossRef]
- Sanin, K.I.; Islam, M.M.; Mahfuz, M.; Ahmed, A.M.S.; Mondal, D.; Haque, R.; Ahmed, T. Micronutrient adequacy is poor, but not associated with stunting between 12-24 months of age: A cohort study findings from a slum area of Bangladesh. PLoS ONE 2018, 13, e0195072. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zambruni, M.; Luna, G.; Silva, M.; Bausch, D.G.; Rivera, F.P.; Velapatino, G.; Campos, M.; Chea-Woo, E.; Baiocchi, N.; Cleary, T.G.; et al. High Prevalence and Increased Severity of Norovirus Mixed Infections Among Children 12–24 Months of Age Living in the Suburban Areas of Lima, Peru. J. Pediatr. Infect. Dis. Soc. 2016, 5, 337–341. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferreira, M.; Victoria, M.; Carvalho-Costa, F.; Vieira, C.; Xavier, M.; Fioretti, J.; Andrade, J.; Volotão, E.; Rocha, M.; Leite, J.; et al. Surveillance of norovirus infections in the state of Rio De Janeiro, Brazil 2005–2008. J. Med. Virol. 2010, 82, 1442–1448. [Google Scholar] [CrossRef] [PubMed]
- Watkins, W. The ABO blood group system: Historical background. Transfus. Med. 2001, 11, 243–265. [Google Scholar] [CrossRef] [PubMed]
- Tonini, M.A.L.; Barreira, D.M.P.G.; Santolin, L.B.D.F.; Volpini, L.P.B.; Leite, J.P.G.; Le Moullac-Vaidye, B.; Le Pendu, J.; Spano, L.C. FUT2, Secretor Status and FUT3 Polymorphisms of Children with Acute Diarrhea Infected with Rotavirus and Norovirus in Brazil. Viruses 2020, 12, 1084. [Google Scholar] [CrossRef]
- My, P.V.T.; Thompson, C.; Le Phuc, H.; Tuyet, P.T.N.; Vinh, H.; Hoang, N.V.M.; Van Minh, P.; Vinh, N.T.; Thuy, C.T.; Nga, T.T.T.; et al. Endemic Norovirus Infections in Children, Ho Chi Minh City, Vietnam, 2009–2010. Emerg. Infect. Dis. 2013, 19, 977. [Google Scholar] [CrossRef] [PubMed]
- Rogawski, E.T.; Guerrant, R.L.; Havt, A.; Lima, I.F.N.; Medeiros, P.H.Q.S.; Seidman, J.C.; McCormick, B.J.J.; Babji, S.; Hariraju, D.; Bodhidatta, L.; et al. Epidemiology of enteroaggregative Escherichia coli infections and associated outcomes in the MAL-ED birth cohort. PLoS Negl. Trop. Dis. 2017, 11, e0005798. [Google Scholar] [CrossRef] [Green Version]
- Pathela, P.; Roy, E.; Alam, K.; Huq, F.; Hasan, K.Z.; Siddique, A.K.; Sack, R.B. EnterotoxigenicBacteroides fragilis–Associated Diarrhea in Children 0–2 Years of Age in Rural Bangladesh. J. Infect. Dis. 2005, 191, 1245–1252. [Google Scholar] [CrossRef] [Green Version]
- Weichert, S.; Koromyslova, A.; Singh, B.K.; Hansman, S.; Jennewein, S.; Schroten, H.; Hansman, G. Structural Basis for Norovirus Inhibition by Human Milk Oligosaccharides. J. Virol. 2016, 90, 4843–4848. [Google Scholar] [CrossRef] [Green Version]
- Shang, J.; Piskarev, V.E.; Xia, M.; Huang, P.; Jiang, X.; Likhosherstov, L.M.; Novikova, O.S.; Newburg, D.S.; Ratner, D.M. Identifying human milk glycans that inhibit norovirus binding using surface plasmon resonance. Glycobiology 2013, 23, 1491–1498. [Google Scholar] [CrossRef] [Green Version]
- Rouhani, S.; Yori, P.P.; Olortegui, M.P.; Salas, M.S.; Trigoso, D.R.; Mondal, D.; Bodhidatta, L.; Platts-Mills, J.; Samie, A.; Kabir, F.; et al. Norovirus Infection and Acquired Immunity in 8 Countries: Results From the MAL-ED Study. Clin. Infect. Dis. 2016, 62, 1210–1217. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Troeger, H.; Loddenkemper, C.; Schneider, T.; Schreier, E.; Epple, H.-J.; Zeitz, M.; Fromm, M.; Schulzke, J.-D.; Troeger, H.; Loddenkemper, C.; et al. Structural and functional changes of the duodenum in human norovirus infection. Gut 2009, 58, 1070–1077. [Google Scholar] [CrossRef] [PubMed]
- Budge, S.; Parker, A.H.; Hutchings, P.; Garbutt, C. Environmental enteric dysfunction and child stunting. Nutr. Rev. 2019, 77, 240–253. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Semba, R.D.; Shardell, M.; Ashour, F.A.S.; Moaddel, R.; Trehan, I.; Maleta, K.; Ordiz, M.I.; Kraemer, K.; Khadeer, M.A.; Ferrucci, L.; et al. Child Stunting is Associated with Low Circulating Essential Amino Acids. eBioMedicine 2016, 6, 246–252. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nuss, E.T.; Tanumihardjo, S.A.; Fretham, S.J.B.; Carlson, E.S.; Georgieff, M.K. Quality Protein Maize for Africa: Closing the Protein Inadequacy Gap in Vulnerable Populations. Adv. Nutr. Int. Rev. J. 2011, 2, 217–224. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gazi, M.A.; Das, S.; Siddique, M.A.; Alam, M.A.; Fahim, S.M.; Hasan, M.M.; Hossaini, F.; Kabir, M.M.; Noor, Z.; Haque, R.; et al. Plasma Kynurenine to Tryptophan Ratio Is Negatively Associated with Linear Growth of Children Living in a Slum of Bangladesh: Results from a Community-Based Intervention Study. Am. J. Trop. Med. Hyg. 2021, 104, 766. [Google Scholar] [CrossRef]
- Semba, R.D.; Trehan, I.; Gonzalez-Freire, M.; Kraemer, K.; Moaddel, R.; Ordiz, M.I.; Ferrucci, L.; Manary, M. Perspective: The Potential Role of Essential Amino Acids and the Mechanistic Target of Rapamycin Complex 1 (mTORC1) Pathway in the Pathogenesis of Child Stunting. Adv. Nutr. Int. Rev. J. 2016, 7, 853–865. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Bangladesh | Brazil | India | Nepal | Peru | Pakistan | South Africa | Tanzania | Overall |
|---|---|---|---|---|---|---|---|---|---|
| Male Sex (n, %) | 108 (51.4) | 89 (53.9) | 105 (46.3) | 122 (53.7) | 105 (54.1) | 120 (48.8) | 120 (50.6) | 105 (50.2) | 874 (51.0) |
| Days of exclusive breastfeeding | 143.2 ± 42.7 | 93.7 ±57.8 | 105.4 ± 42.9 | 92.5 ± 54.5 | 89.5 ± 61.3 | 19.9 ± 22.7 | 38.6 ± 26.3 | 62.2 ± 35 | 78.6 ± 57.7 |
| Birth weight in kilograms | 2.8 ± 0.4 | 3.4 ± 0.5 | 2.9 ± 0.4 | 3.0 ± 0.4 | 3.1 ± 0.4 | 2.7 ± 0.4 | 3.2 ± 0.5 | 3.2 ± 0.5 | 3.0 ± 0.5 |
| Weight for age z score at enrollment | −1.3 ± 0.9 | −0.2 ± 1.0 | −1.3 ± 1.0 | −0.9 ± 1.0 | −0.6 ±0.9 | −1.4 ± 1.0 | −0.4 ± 1.0 | −0.1 ± 1.1 | −0.8 ± 1.1 |
| Length for age z score at enrollment | −1.0 ± 1.0 | −0.8 ± 1.1 | −1.0 ± 1.1 | −0.7 ± 1.0 | −0.9 ± 1.0 | −1.3 ± 1.1 | −0.7 ± 1.0 | −1.0 ± 1.1 | −0.9 ± 1.1 |
| Length for age z score at 24 months | −2.0 ± 0.9 | 0.0 ± 1.1 | −1.9 ± 1.0 | −1.3 ± 0.9 | −1.9 ± 0.9 | - | −1.7 ± 1.1 | −2.7 ± 1.0 | −1.7 ± 1.2 |
| Weight for age z score at 24 months | −0.8 ± 0.9 | 0.5 ± 1.4 | −0.9 ± 0.9 | −0.3 ± 0.9 | 0.3 ± 0.9 | - | 0.5 ± 1.0 | 0.1 ± 1.0 | −0.1 ± 1.1 |
| Maternal age at enrolment (in years) | 25 ± 5 | 25.4 ± 5.6 | 23.9 ± 4.2 | 26.6 ± 3.7 | 24.8 ± 6.3 | 28.1 ± 5.9 | 27 ± 7.2 | 29.1 ± 6.5 | 26.3 ± 5.9 |
| Maternal BMI at enrolment | 22.3 ± 3.4 | 25.7 ± 4.4 | 22.0 ± 4.0 | 25.1 ± 3.2 | 24.9 ± 3.7 | 21.5 ± 3.8 | 27 ± 5.5 | 22.9 ± 3.2 | 23.9 ± 4.4 |
| Maternal education level (>6 years of schooling) | 77(36.7) | 143 (86.7) | 147 (64.8) | 168(74) | 150 (77.3) | 44 (17.9) | 232(97.9) | 134 (64.1) | 1095 (63.8) |
| Mother has more than 3 living children | 50 (23.8) | 52 (31.5) | 70 (30.2) | 28 (12.3) | 73 (42.8) | 141 (57.3) | 96 (40.5) | 151 (72.2) | 671 (39) |
| Ownership of chicken or cattle (n, %) | 3 (1.4) | 1 (0.6) | 14 (6.2) | 73 (32.2) | 75 (38.7) | 144 (62.3) | 87 (37.2) | 204 (97.6) | 601 (35.4) |
| Routine treatment of drinking water (n, %) | 130 (61.9) | 10 (6.1) | 7 (3.1) | 98 (43.2) | 32 (16.5) | 0 | 12 (5.1) | 12 (5.7) | 301 (17.6) |
| Improved drinking water source (n, %) | 210 (100) | 165 (100) | 227 (100) | 227 (100) | 184 (94.9) | 246 (100) | 196 (82.7) | 89 (42.6) | 1544 (90.0) |
| Improved floor (n, %) | 204 (97.1) | 165 (100) | 222 (97.8) | 109 (48) | 69 (35.6) | 81 (32.9) | 231 (97.5) | 13 (6.2) | 1094 (63.8) |
| Improved sanitary latrine (n, %) | 210 (100) | 165 (100) | 121 (53.3) | 227 (100) | 66 (34) | 197 (80.1) | 232 (97.9) | 19 (9.1) | 1237 (72.1) |
| Monthly income less than 150 USD (n, %) | 69 (32.9) | 161 (97.6) | 19 (8.4) | 106 (46.7) | 58 (29.9) | 115 (46.8) | 179 (75.5) | 0 | 707 (41.2) |
| Greater than 2 people living per room (n, %) | 202 (96.2) | 24 (14.5) | 181 (79.7) | 101 (44.5) | 72 (31.1) | 219 (89.1) | 26 (15.2) | 114 (54.5) | 949 (55.3) |
| Average serum zinc level (mmol/l) ** | 11.3 (10.6, 12.1) | 14 (13, 14.9) | 9.1 (8.6, 9.6) | 11.2 (10.4, 12.2) | 14.8 (13.1, 17.9) | 8.9 (7.7, 10) | 22.9 (14.3, 32.9) | 11.1 (9.9, 12.3) | 11.3 (9.6, 13.7) |
| Average AGP (mg/dL) a ** | 84.3 (71.5, 105) | 95.7 (81, 117) | 97 (83, 110) | 117.7 (102.7, 139) | 115 (98, 130) | 93 (77.5, 112) | 126 (107, 154) | 114.3 (97.7, 139) | 106.3 (87, 127) |
| Risk Factors | Norovirus GI | Norovirus GII | ||
|---|---|---|---|---|
| IRR (95% CI) | p-Value | IRR (95% CI) | p-Value | |
| Male sex | 0.95 (0.93, 0.97) | <0.001 | 1.13 (1.11, 1.14) | <0.001 |
| Duration of exclusive breastfeeding | 0.95 (0.93, 0.96) | 0.030 | 0.96 (0.96, 0.97) | <0.001 |
| Household ownership of chicken or cattle | 0.99 (0.99, 1.01) | 0.385 | 1.00 (0.98, 1.02) | 0.832 |
| LAZ at enrolment | 0.94 (0.91, 0.95) | 0.028 | 0.99 (0.98, 1.00) | 0.197 |
| WAZ at enrolment | 0.97 (0.96, 1.01) | 0.007 | 0.98 (0.97, 1.00) | 0.005 |
| Maternal age in years | 1.00 (0.99, 1.02) | 0.008 | 1.00 (0.99, 1.00) | 0.004 |
| Improved drinking water source | 0.89 (0.83, 0.95) | <0.001 | 0.98 (0.95, 1.00) | 0.150 |
| Improved floor in households | 0.97 (0.95, 0.99) | 0.224 | 0.96 (0.95, 0.99) | 0.001 |
| Maternal BMI | 1.00 (0.99, 1.03) | <0.001 | 1.00 (1.00, 1.02) | 0.003 |
| Use of water treatment methods | 0.85 (0.82, 0.88) | <0.001 | 0.96 (0.95, 0.97) | 0.029 |
| Maternal education more than 6 years of schooling | 0.95 (0.92, 0.98) | 0.001 | 0.98 (0.98, 1.01) | 0.295 |
| Access to improved sanitation | 0.81 (0.79, 0.84) | <0.001 | 0.96 (0.94, 0.98) | <0.001 |
| Mother has more than 3 living children | 1.09 (1.06, 1.13) | <0.001 | 1.11 (1.08, 1.13) | <0.001 |
| More than 2 people live in per room | 1.05 (1.02, 1.08) | <0.001 | 1.03 (0.99, 1.05) | 0.003 |
| Monthly income more than 150 USD | 0.92 (0.89, 0.94) | <0.001 | 0.91 (0.90, 0.94) | <0.001 |
| Site | Length-for-Age Z Score | Weight-for-Age Z Score | ||||||
|---|---|---|---|---|---|---|---|---|
| Norovirus Genogroup I | Norovirus Genogroup II | Norovirus Genogroup I | Norovirus Genogroup II | |||||
| β-Coefficient (95% CI) | p-Value | β-Coefficient (95% CI) | p-Value | β-Coefficient (95% CI) | p-Value | β-Coefficient (95% CI) | p-Value | |
| Bangladesh | −0.36 (−0.38, −0.34) | <0.001 | −0.06 (−0.23, 0.05) | 0.302 | −0.22 (−0.35, −0.15) | <0.001 | −0.073 (−0.10, −0.05) | <0.001 |
| Brazil | −0.49 (−0.57, −0.43) | 0.01 | 0.09 (0.07, 0.11) | 0.608 | −0.30 (−0.433, −0.303) | <0.001 | 0.086 (−0.11, 0.07) | 0.123 |
| India | 0.19 (0.09, −0.24) | 0.128 | −0.12 (−0.24, −0.08) | <0.001 | −0.38 (−0.53, −0.33) | <0.001 | −0.038 (−0.053, −0.023) | <0.001 |
| Nepal | −0.16 (0.12, 0.23) | <0.001 | −0.36 (−0.39, −0.24) | 0.223 | −0.25 (−0.42, −0.009) | 0.003 | −0.025 (−0.09, 0.04) | 0.03 |
| Peru | −0.18 (−0.32, −0.04) | 0.012 | −0.15 (−0.32, −0.05) | 0.008 | −0.36 (−0.52, −0.20) | <0.001 | −0.36 (−0.44, −0.25) | <0.001 |
| South Africa | −0.21 (−0.29, −0.10) | 0.026 | −0.21 (−0.39, −0.17) | 0.025 | 0.02 (−0.02, 0.25) | 0.268 | 0.03 (−0.02, 0.25) | 0.835 |
| Tanzania | −0.29 (−0.39, −0.24) | 0.003 | −0.30 (−0.49, −0.20) | 0.003 | 0.11 (−0.12, 0.35) | 0.346 | 0.11 (−0.12, 0.17) | 0.354 |
| Overall | −0.53 (−0.73, −0.50) | <0.001 | −0.18 (−0.23, 0.07) | 0.671 | −0.39 (−0.49, 0.28) | <0.001 | −0.04 (−0.12, 0.35) | 0.281 |
| Explanatory Variable | Outcome Variables | |||
|---|---|---|---|---|
| Length-for-Age Z Score at 2 Years of Age | Weight-for-Age Z Score at 2 Years of Age | |||
| β-Coefficient (95% CI) | p-Value | β-Coefficient (95% CI) | p-Value | |
| Burden of asymptomatic norovirus GI infection | −0.46 (−0.67, −0.41) | 0.003 | −0.66 (−0.86, −0.53) | <0.001 |
| Male sex | −0.23 (−0.25, −0.20) | <0.001 | −0.10 (−0.12, −0.07) | <0.001 |
| Exclusive breast feeding | 0.057 (0.05, 0.07) | <0.001 | 0.07 (0.06, 0.09) | <0.001 |
| Birth weight | 0.10 (0.06, 0.14) | <0.001 | 0.17 (0.13, 0.28) | <0.001 |
| WAMI score | 0.98 (0.87, 1.10) | <0.001 | 0.96 (0.86, 1.07) | <0.001 |
| Maternal BMI | 0.30 (0.28, 0.33) | <0.001 | 0.14 (0.11, 0.16) | <0.001 |
| Concentration of zinc in plasma | 0.12 (0.04, 0.15) | <0.001 | 0.05 (0.01, 0.09) | 0.017 |
| Concentration of AGP in plasma | −0.08 (−0.17, −0.04) | <0.001 | −0.10 (−0.14, −0.07) | 0.005 |
| Burden of asymptomatic Shigella infection | −0.57 (−0.71, −0.43) | <0.001 | −0.62 (−0.77, −0.43) | <0.001 |
| Burden of asymptomatic Campylobacter infection | −0.30 (−0.38, −0.21) | <0.001 | −0.63 (−0.79, −0.43) | <0.001 |
| Burden of asymptomatic Cryptosporidium infection | −0.45 (−0.64, −0.36) | <0.001 | −0.31 (−0.41, −0.28) | <0.001 |
| Burden of asymptomatic Giardia infection | −0.48 (−0.55, −0.43) | <0.001 | −0.35 (−0.41, −0.28) | <0.001 |
| Burden of asymptomatic ETEC infection | −0.21 (−0.24, 0.10) | <0.001 | −0.65 (−0.78, −0.42) | 0.02 |
| Burden of asymptomatic typical EPEC infection | −0.15 (−.019, −0.08) | <0.001 | −0.11 (−0.14, −0.07) | <0.001 |
| EED score at 24 months | −0.12 (−0.16, 0.06) | <0.001 | −0.21 (−0.27, −0.17) | <0.001 |
| Explanatory Variable | Outcome Variables | |||
|---|---|---|---|---|
| Length-for-Age Z Score at 2 Years of Age | Weight-for-Age Z Score at 2 Years of Age | |||
| β-Coefficient (95% CI) | p-Value | β-Coefficient (95% CI) | p-Value | |
| Burden of asymptomatic norovirus GII infection | −0.13 (−0.30, −0.04) | 0.135 | −0.27 (−0.45, −0.25) | 0.002 |
| Male sex | −0.24 (−0.29, −0.21) | <0.001 | −0.10 (−0.13, −0.08) | <0.001 |
| Exclusive breast feeding | 0.06 (0.04, 0.07) | <0.001 | −0.07 (−0.08, −0.05) | <0.001 |
| Birth weight | 0.27 (0.25, 0.31) | <0.001 | 0.16 (0.18, 0.15) | <0.001 |
| WAMI score | 0.93 (0.84, 1.01) | 0.039 | 0.99 (0.87, 1.03) | <0.001 |
| Maternal BMI | 0.06 (0.05, 0.08) | <0.001 | 0.13 (0.10, 0.16) | 0.017 |
| Concentration of zinc in plasma | 0.12 (0.09, 0.17) | <0.001 | 0.05 (0.03, 0.09) | <0.001 |
| Concentration of AGP in plasma | −0.15 (−0.19. −0.07) | 0.008 | −0.10 (−0.13, −0.09) | 0.037 |
| Burden of asymptomatic Shigella infection | −0.53 (−0.61, −0.44) | <0.001 | −0.64 (−0.77, −0.50) | <0.001 |
| Burden of asymptomatic Campylobacter infection | −0.21 (−0.39, −0.18) | <0.001 | −0.15 (−0.15, −0.14) | <0.001 |
| Burden of asymptomatic Cryptosporidium infection | −0.46 (−0.63, −0.33) | <0.001 | −0.33 (−0.51, −0.24) | <0.001 |
| Burden of asymptomatic Giardia infection | −0.39 (−0.55, −0.42) | <0.001 | −0.34 (−0.40, −0.28) | <0.001 |
| Burden of asymptomatic ETEC infection | −0.14 (−0.18, −0.11) | 0.034 | −0.18 (−0.26, −0.08) | 0.021 |
| Burden of asymptomatic typical EPEC infection | −0.18 (−0.22, −0.15) | <0.001 | −0.21 (−0.26, −0.16) | <0.001 |
| EED score at 24 months | −0.13 (−0.17, −0.10) | <0.001 | −0.17 (−0.19, −0.11) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Palit, P.; Das, R.; Haque, M.A.; Hasan, M.M.; Noor, Z.; Mahfuz, M.; Faruque, A.S.G.; Ahmed, T. Risk Factors for Norovirus Infections and Their Association with Childhood Growth: Findings from a Multi-Country Birth Cohort Study. Viruses 2022, 14, 647. https://doi.org/10.3390/v14030647
Palit P, Das R, Haque MA, Hasan MM, Noor Z, Mahfuz M, Faruque ASG, Ahmed T. Risk Factors for Norovirus Infections and Their Association with Childhood Growth: Findings from a Multi-Country Birth Cohort Study. Viruses. 2022; 14(3):647. https://doi.org/10.3390/v14030647
Chicago/Turabian StylePalit, Parag, Rina Das, Md. Ahshanul Haque, Md. Mehedi Hasan, Zannatun Noor, Mustafa Mahfuz, Abu Syed Golam Faruque, and Tahmeed Ahmed. 2022. "Risk Factors for Norovirus Infections and Their Association with Childhood Growth: Findings from a Multi-Country Birth Cohort Study" Viruses 14, no. 3: 647. https://doi.org/10.3390/v14030647
APA StylePalit, P., Das, R., Haque, M. A., Hasan, M. M., Noor, Z., Mahfuz, M., Faruque, A. S. G., & Ahmed, T. (2022). Risk Factors for Norovirus Infections and Their Association with Childhood Growth: Findings from a Multi-Country Birth Cohort Study. Viruses, 14(3), 647. https://doi.org/10.3390/v14030647