
Increased Serum Mir-150-3p Expression Is Associated with Radiological Lung Injury Improvement in Patients with COVID-19

 , , ,
, , ,  , ,
, , 

Abstract
:1. Introduction
2. Materials and Methods
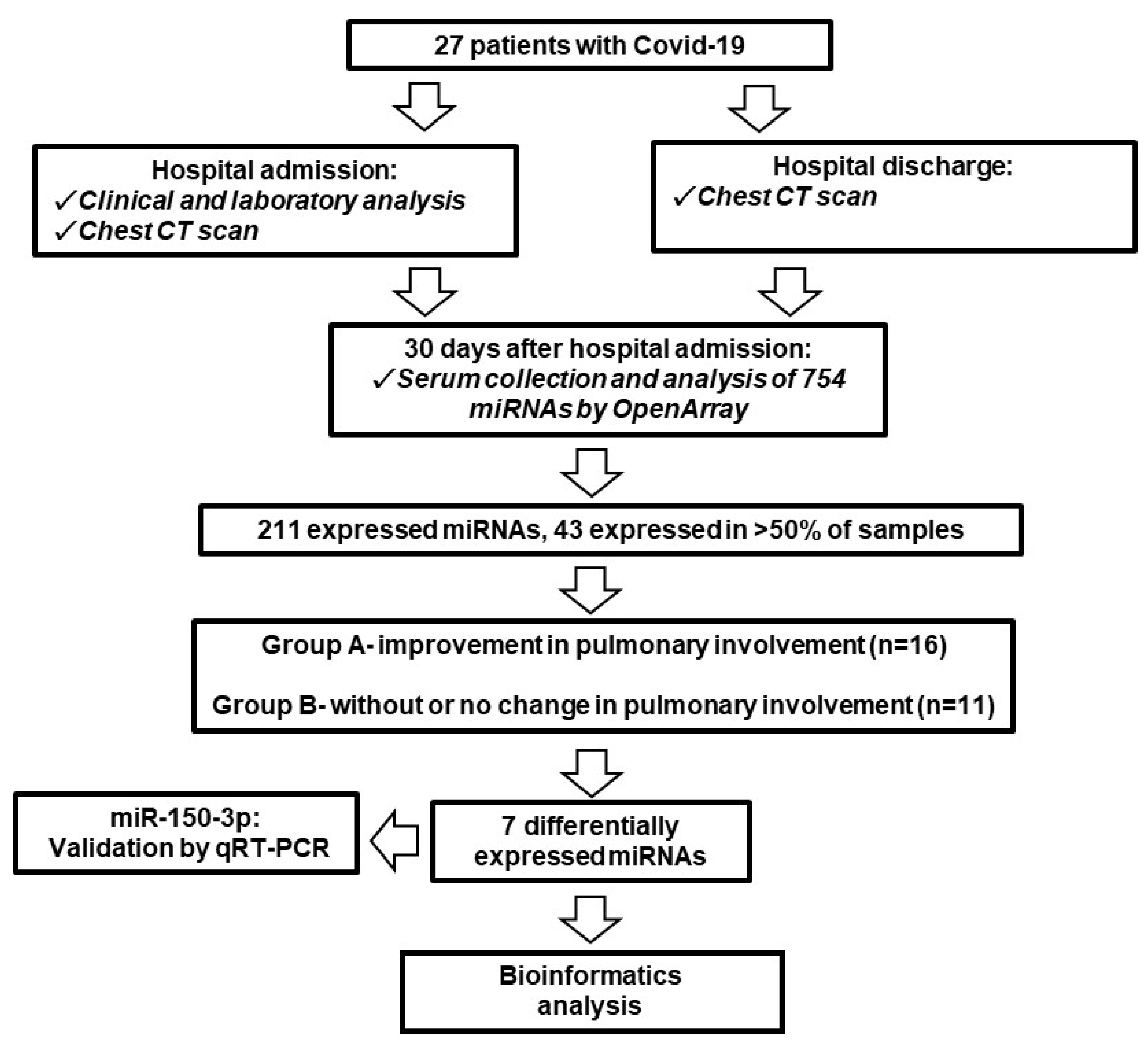
2.1. Patient Recruitment, Characteristics, and Sample Acquisition
2.2. Extraction and Analysis of Serum miRNA Expression
2.3. Target Prediction in SARS-CoV-2 Genome and Receptors
2.4. Statistical Analysis
3. Results
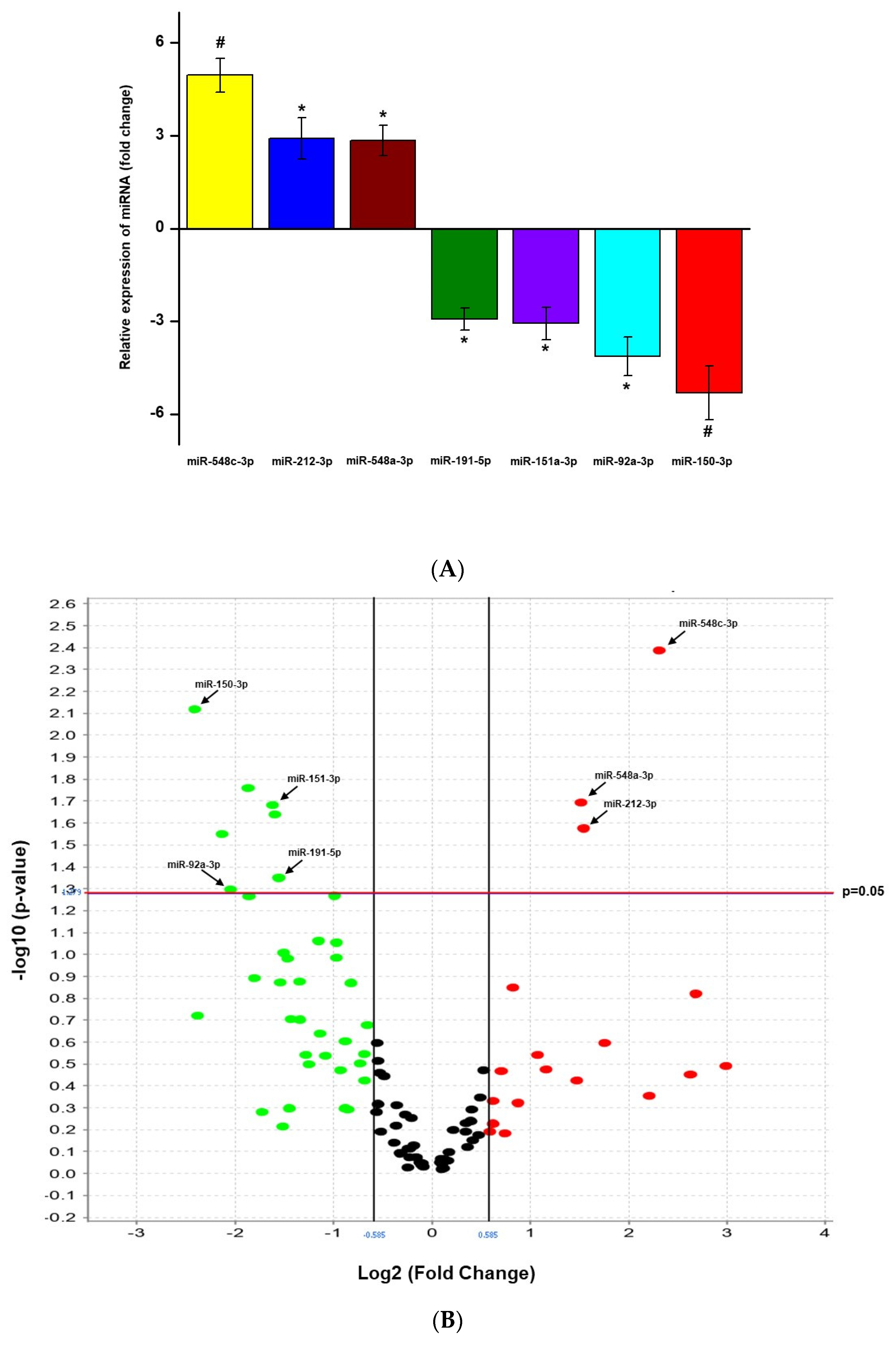
3.1. Clinical Characteristics of Participants and miRNA Expression Levels
3.2. Target Prediction in SARS-CoV-2 Receptors
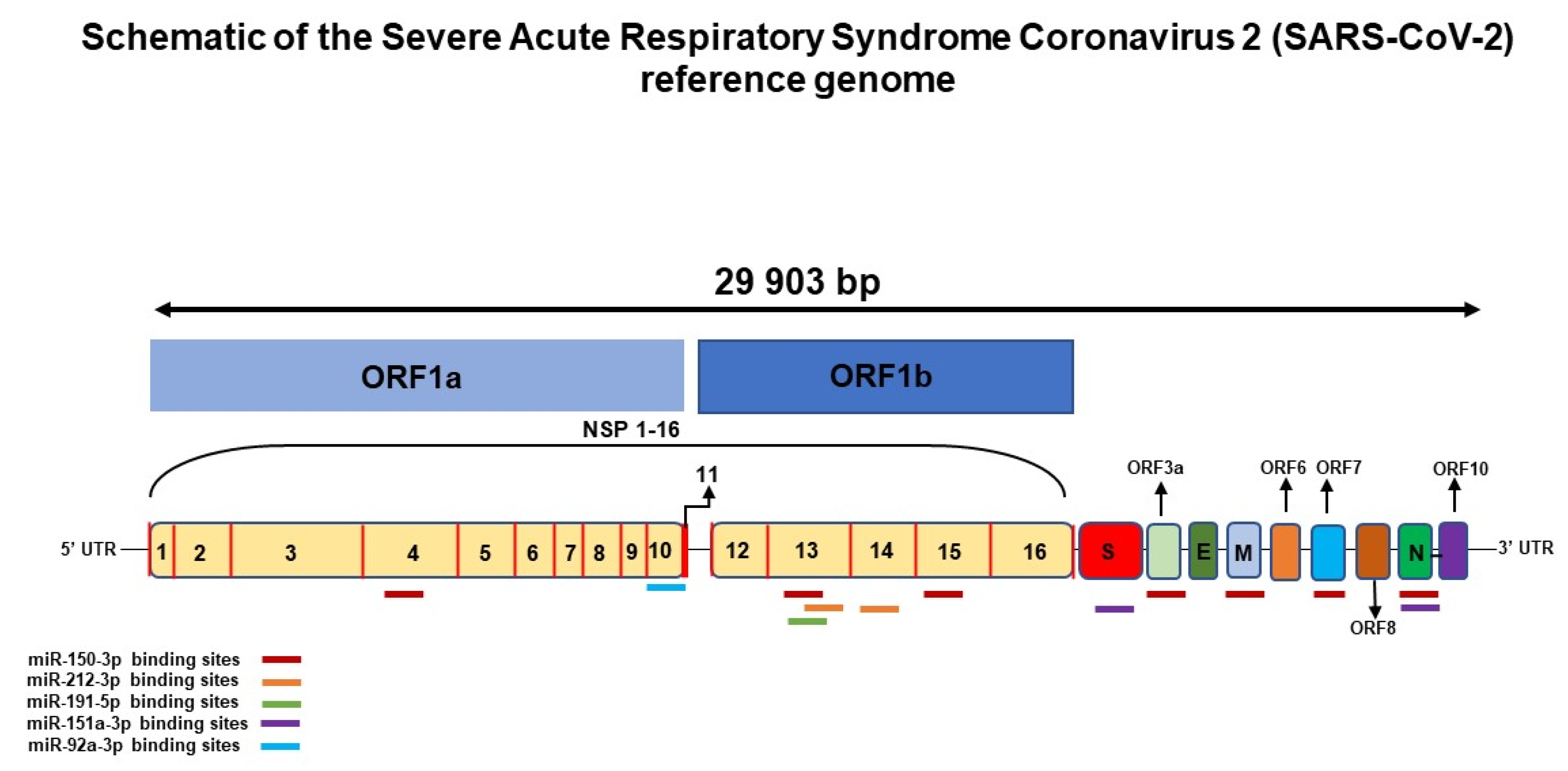
3.3. Target Prediction in SARS-CoV-2
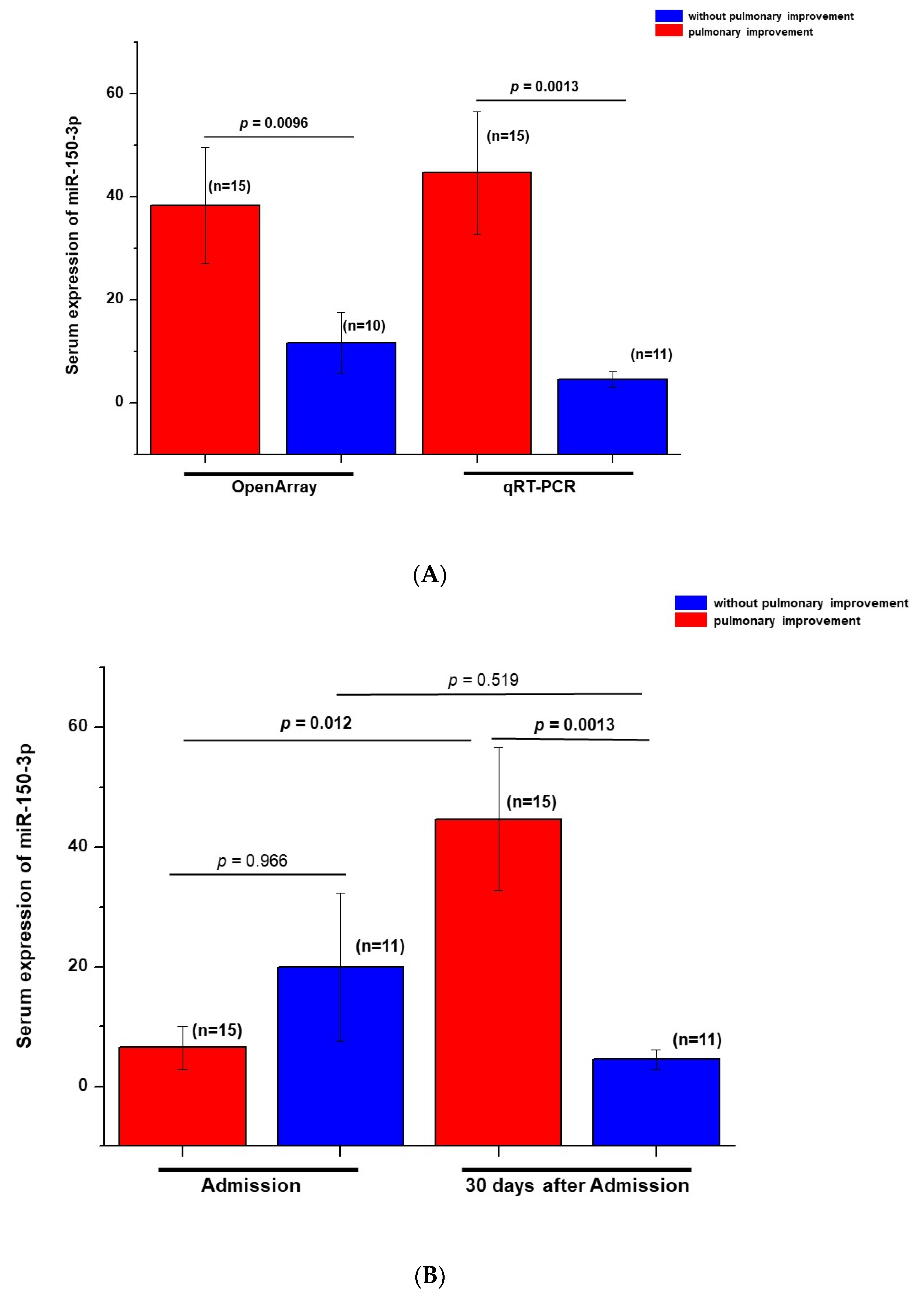
3.4. Validation of miR-150-3p Expression Levels
3.5. Correlation Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. China Novel Coronavirus Investigating and Research Team. A Novel Coronavirus from Patients with Pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef] [PubMed]
- Jin, D.; An, X.; Zhang, Y.; Zhao, S.; Duan, L.; Duan, Y.; Lian, F.; Tong, X. Potential Mechanism Prediction of Herbal Medicine for Pulmonary Fibrosis Associated with SARS-CoV-2 Infection Based on Network Analysis and Molecular Docking. Front. Pharmacol. 2021, 12, 602218. [Google Scholar] [CrossRef] [PubMed]
- Cheng, Z.; Qin, L.; Cao, Q.; Dai, J.; Pan, A.; Yang, W.; Gao, Y.; Chen, L.; Yan, F. Quantitative computed tomography of the coronavirus disease 2019 (COVID-19) pneumonia. Radiol. Infect. Dis. 2020, 7, 55–61. [Google Scholar] [CrossRef] [PubMed]
- Katopodis, P.; Randeva, H.S.; Spandidos, D.A.; Saravi, S.; Kyrou, I.; Karteris, E. Host cell entry mediators implicated in the cellular tropism of SARS-CoV-2, the pathophysiology of COVID-19 and the identification of microRNAs that can modulate the expression of these mediators. Int. J. Mol. Med. 2021, 49, 20. [Google Scholar] [CrossRef]
- Yoshikawa, F.S.Y.; Teixeira, F.M.E.; Sato, M.N.; Oliveira, L.M.S. Delivery of microRNAs by Extracellular Vesicles in Viral Infections: Could the News be Packaged? Cells 2019, 8, 611. [Google Scholar] [CrossRef] [Green Version]
- Ferruelo, A.; Peñuelas, O.; Lorente, J.A. MicroRNAs as biomarkers of acute lung injury. Ann. Transl. Med. 2018, 6, 34. [Google Scholar] [CrossRef]
- Guiot, J.; Struman, I.; Louis, E.; Louis, R.; Malaise, M.; Njock, M.-K. Exosomal miRNAs in lung diseases: From Biologic Function to Therapeutic Targets. J. Clin. Med. 2019, 8, 1345. [Google Scholar] [CrossRef] [Green Version]
- Bargieł, W.; Cierpiszewska, K.; Maruszczak, K.; Pakuła, A.; Szwankowska, D.; Wrzesińska, A.; Gutowski, L.; Formanowicz, D. Recognized and Potentially New Biomarkers-Their Role in Diagnosis and Prognosis of Cardiovascular Disease. Medicina 2021, 57, 701. [Google Scholar] [CrossRef]
- Rajasegaran, Y.; Azlan, A.; Rosli, A.A.; Yik, M.Y.; Zi, K.K.; Yusoff, N.M.; Moses, E.J. Footprints of microRNAs in Cancer Biology. Biomedicines 2021, 9, 1494. [Google Scholar] [CrossRef]
- Paul, S.; Vázquez, L.A.B.; Reyes-Pérez, P.R.; Estrada-Meza, C.; Alburquerque, R.A.A.; Pathak, S.; Banerjee, A.; Bandyopadhyay, A.; Chakraborty, S.; Srivastava, A. The role of microRNAs in solving COVID-19 puzzle from infection to therapeutics: A mini-review. Virus Res. 2022, 308, 198631. [Google Scholar] [CrossRef]
- Mansour, E.; Palma, A.C.; Ulaf, R.G.; Ribeiro, L.C.; Bernardes, A.F.; Nunes, T.A.; Agrela, M.V.; Bombassaro, B.; Monfort-Pires, M.; Camargo, R.L.; et al. Safety and Outcomes Associated with the Pharmacological Inhibition of the Kinin-Kallikrein System in Severe COVID-19. Viruses 2021, 13, 309. [Google Scholar] [CrossRef] [PubMed]
- Corman, V.M.; Landt, O.; Kaiser, M.; Molenkamp, R.; Meijer, A.; Chu, D.K.; Bleicker, B.; Brünink, S.; Schneider, J.; Schmidt, M.L.; et al. Detection of 2019 novel coronavirus (2019-nCoV) by real-time RT-PCR. Eurosurveillance 2020, 25, 2000045. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pan, F.; Ye, T.; Sun, P.; Gui, S.; Liang, B.; Li, L.; Zheng, D.; Wang, J.; Hesketh, R.L.; Yang, L.; et al. Time Course of Lung Changes at Chest CT during Recovery from Coronavirus Disease 2019 (COVID-19). Radiology 2020, 295, 715–721. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paim, L.R.; Schreiber, R.; Rossi, G.; Matos-Souza, J.R.; Silva, A.A.C.; Calegari, D.R.; Cheng, S.; Marques, F.Z.; Sposito, A.C.; Gorla, J.I.; et al. Circulating microRNAs, Vascular Risk, and Physical Activity in Spinal Cord-Injured Subjects. J. Neurotrauma 2019, 36, 845–852. [Google Scholar] [CrossRef] [PubMed]
- Livak, K.J.; Schmittgen, T.D. Analysis of relative gene expression data using real-time quantitative PCR and the 2(-Delta Delta C(T)) Method. Methods 2001, 25, 402–408. [Google Scholar] [CrossRef]
- Miranda, K.C.; Huynh, T.; Tay, Y.; Ang, Y.-S.; Tam, W.-L.; Thomson, A.M.; Lim, B.; Rigoutsos, I. A Pattern-Based Method for the Identification of MicroRNA Binding Sites and Their Corresponding Heteroduplexes. Cell 2006, 126, 1203–1217. [Google Scholar] [CrossRef] [Green Version]
- Akula, S.M.; Bolin, P.; Cook, P.P. Cellular miR-150-5p may have a crucial role to play in the biology of SARS-CoV-2 infection by regulating nsp10 gene. RNA Biol. 2021, 19, 1–11. [Google Scholar] [CrossRef]
- Xu, J.; Xu, D.; Yu, Z.; Fu, Z.; Lv, Z.; Meng, L.; Zhao, X. Exosomal miR-150 partially attenuated acute lung injury by mediating microvascular endothelial cells and MAPK pathway. Biosci. Rep. 2021, 42, BSR20203363. [Google Scholar] [CrossRef]
- Chow, J.T.; Salmena, L. Prediction and Analysis of SARS-CoV-2-Targeting MicroRNA in Human Lung Epithelium. Genes 2020, 11, 1002. [Google Scholar] [CrossRef]
- Elemam, N.M.; Hasswan, H.; Aljaibeji, H.; Sharif-Askari, N.S.; Halwani, R.; Taneera, J.; Sulaiman, N. Profiling Levels of Serum microRNAs and Soluble ACE2 in COVID-19 Patients. Life 2022, 12, 575. [Google Scholar] [CrossRef]
- Elemam, N.M.; Hasswan, H.; Aljaibeji, H.; Sulaiman, N. Circulating Soluble ACE2 and Upstream microRNA Expressions in Serum of Type 2 Diabetes Mellitus Patients. Int. J. Mol. Sci. 2021, 22, 5263. [Google Scholar] [CrossRef] [PubMed]
- Tu-Allah Khan, A.; Khalid, Z.; Zahid, H.; Yousaf, M.A.; Abdul Rauf Shakoori, A.R. A computational and bioinformatic analysis of ACE2: An elucidation of its dual role in COVID-19 pathology and finding its associated partners as potential therapeutic targets. J. Biomol. Struct. Dyn. 2020, 40, 1813–1829. [Google Scholar] [CrossRef] [PubMed]
- Fayyad-Kazan, M.; Makki, R.; Skafi, N.; Homsi, M.E.; Hamade, A.; Majzoub, R.E.; Hamade, E.; Fayyad-Kazan, H.; Badran, B. Circulating miRNAs: Potential diagnostic role for coronavirus disease 2019 (COVID-19). Infect. Genet. Evol. 2021, 94, 105020. [Google Scholar] [CrossRef] [PubMed]
- Park, J.H.; Choi, Y.; Lim, C.; Park, J.; Yu, S.; Kim, Y.; Han, H.J.; Kim, C.; Song, Y.; Kim, C.; et al. Potential Therapeutic Effect of Micrornas in Extracellular Vesicles from Mesenchymal Stem Cells against SARS-CoV-2. Cells 2021, 10, 2393. [Google Scholar] [CrossRef] [PubMed]
- Martucci, G.; Arcadipane, A.; Tuzzolino, F.; Occhipinti, G.; Panarello, G.; Carcione, C.; Bonicolini, E.; Vitiello, C.; Lorusso, R.; Conaldi, P.G.; et al. Identification of a Circulating miRNA Signature to Stratify Acute Respiratory Distress Syndrome Patients. J. Pers. Med. 2020, 11, 15. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | With Improvement (n = 16) | Without Improvement (n = 11) | p |
|---|---|---|---|
| Clinical characteristics | |||
| Female/male | 9/7 | 3/8 | 0.273 |
| Age (years) | 49.1 ± 13.4 | 53.6 ± 8.0 | 0.322 |
| Body Mass Index (kg/m2) | 32.5 ± 4.6 | 30.0 ± 4.5 | 0.187 |
| Hypertension, n (%) | 6 (37.5) | 5 (45.5) | 0.988 |
| Diabetes mellitus, n (%) | 6 (37.5) | 4 (36.4) | 0.952 |
| Obesity, n (%) | 12 (75.0) | 7 (63.6) | 0.836 |
| Former smoker, n (%) | 0 (0) | 2 (18.2) | 0.355 |
| Systolic blood pressure (mmHg) | 139.0 ± 17.6 | 134.7 ± 16.7 | 0.532 |
| Diastolic blood pressure (mmHg) | 67.9 ± 34.9 | 76.2 ± 34.5 | 0.550 |
| Oxygen saturation (%) | 97.8 ± 1.1 | 97.6 ± 0.9 | 0.669 |
| PaO2/FiO2 ratio | 314 [272–335] | 335 [310–371] | 0.095 |
| Respiratory rate, per minute | 20.8 ± 3.8 | 19.0 ± 2.4 | 0.176 |
| Laboratory data | |||
| White cell count (×109/L) | 7.1 [6.2–8.8] | 6.0 [5.5–6.6] | 0.054 |
| Lymphocyte count (×109/L) | 4.8 [1.9–30.7] | 1.60 [1.2–5.1] | 0.020 |
| Platelet count (×109/L) | 334.3 ± 84.0 | 290.1 ± 143.5 | 0.322 |
| Plasma glucose (mg/dL) | 134.5 ± 47.8 | 128.7 ± 47.7 | 0.771 |
| Serum creatinine (mg/dL) | 0.64 [0.50–0.83] | 0.86 [0.77–1.04] | 0.009 |
| AST (U/L) | 30 [17–42] | 28 [21–60] | 0.477 |
| C-reactive protein (mg/L) | 15.8 [3.7–34.0] | 23.1 [9.8–39.7] | 0.278 |
| High-sensitivity troponin I, ng/L | 8.5 [4.9–24.8] | 7.6 [4.2–13.7] | 0.712 |
| Brain natriuretic peptide, ng/mL | 50 [50–83] | 50 [50–499] | 0.765 |
| D-dimer, μg/mL | 1254 [643–2029] | 780 [672–999] | 0.256 |
| Urea (mg/dL) | 26 [21–31] | 28 [26–47] | 0.217 |
| Global lung CT scoring | |||
| Score | 11.2 ± 4.3 | 12.1 ± 3.4 | 0.569 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bueno, L.C.M.; Paim, L.R.; Minin, E.O.Z.; da Silva, L.M.; Mendes, P.R.; Kiyota, T.A.; Schreiber, A.Z.; Bombassaro, B.; Mansour, E.; Moretti, M.L.; et al. Increased Serum Mir-150-3p Expression Is Associated with Radiological Lung Injury Improvement in Patients with COVID-19. Viruses 2022, 14, 1363. https://doi.org/10.3390/v14071363
Bueno LCM, Paim LR, Minin EOZ, da Silva LM, Mendes PR, Kiyota TA, Schreiber AZ, Bombassaro B, Mansour E, Moretti ML, et al. Increased Serum Mir-150-3p Expression Is Associated with Radiological Lung Injury Improvement in Patients with COVID-19. Viruses. 2022; 14(7):1363. https://doi.org/10.3390/v14071363
Chicago/Turabian StyleBueno, Larissa C. M., Layde R. Paim, Eduarda O. Z. Minin, Luís Miguel da Silva, Paulo R. Mendes, Tatiana A. Kiyota, Angelica Z. Schreiber, Bruna Bombassaro, Eli Mansour, Maria Luiza Moretti, and et al. 2022. "Increased Serum Mir-150-3p Expression Is Associated with Radiological Lung Injury Improvement in Patients with COVID-19" Viruses 14, no. 7: 1363. https://doi.org/10.3390/v14071363
APA StyleBueno, L. C. M., Paim, L. R., Minin, E. O. Z., da Silva, L. M., Mendes, P. R., Kiyota, T. A., Schreiber, A. Z., Bombassaro, B., Mansour, E., Moretti, M. L., Chow, J. T.-S., Salmena, L., Coelho-Filho, O. R., Velloso, L. A., Nadruz, W., & Schreiber, R. (2022). Increased Serum Mir-150-3p Expression Is Associated with Radiological Lung Injury Improvement in Patients with COVID-19. Viruses, 14(7), 1363. https://doi.org/10.3390/v14071363